
EBUS-TBNA Cytological Samples for Comprehensive Molecular Testing in Non–Small Cell Lung Cancer


 , , , ,
, , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. EBUS-TBNA
2.3. Flexible Bronchoscopy
2.4. Genetic Testing
2.5. Statistical Analysis
3. Results
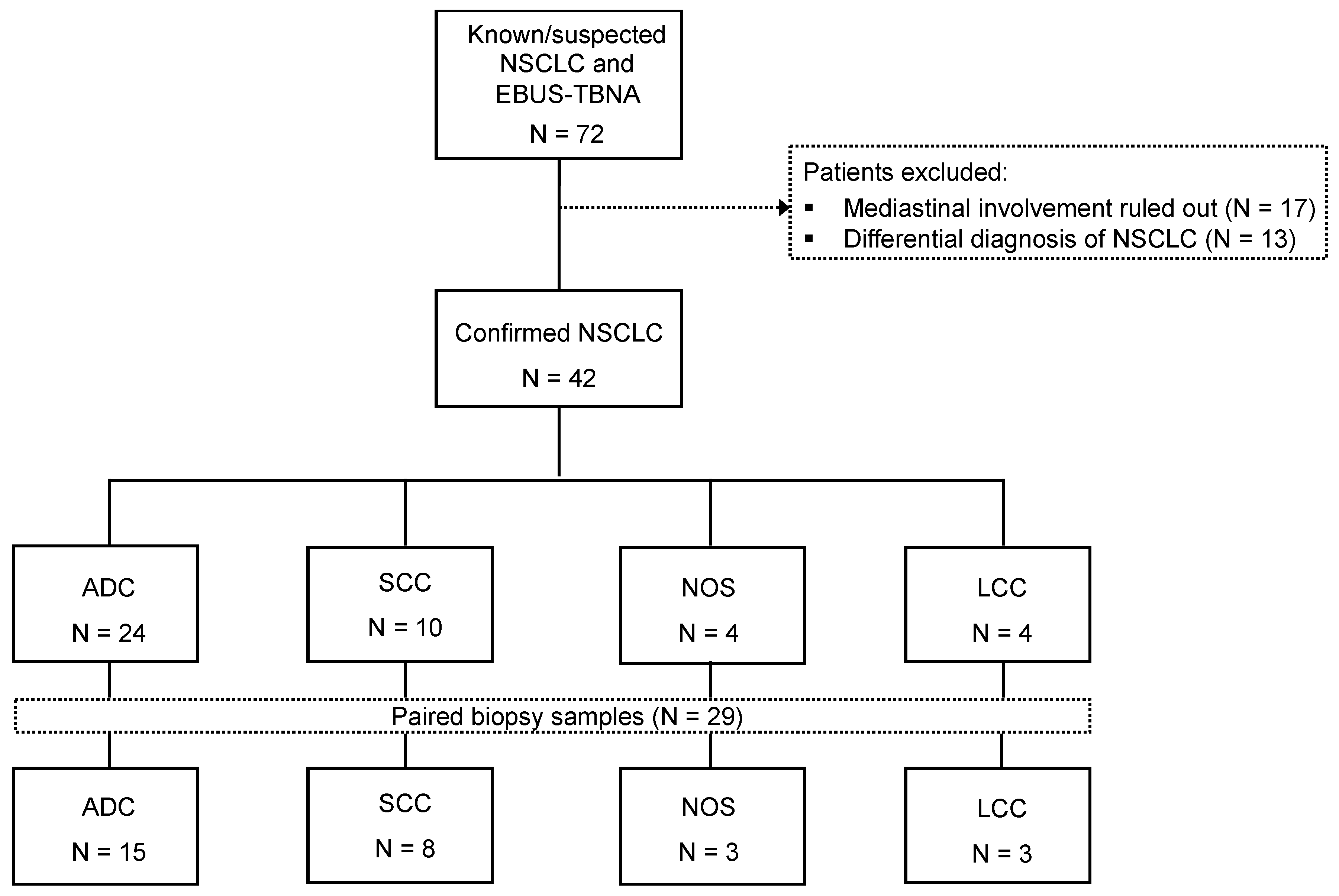
3.1. Patients
3.2. Flexible Bronchoscopy and EBUS-TBNA Representativeness
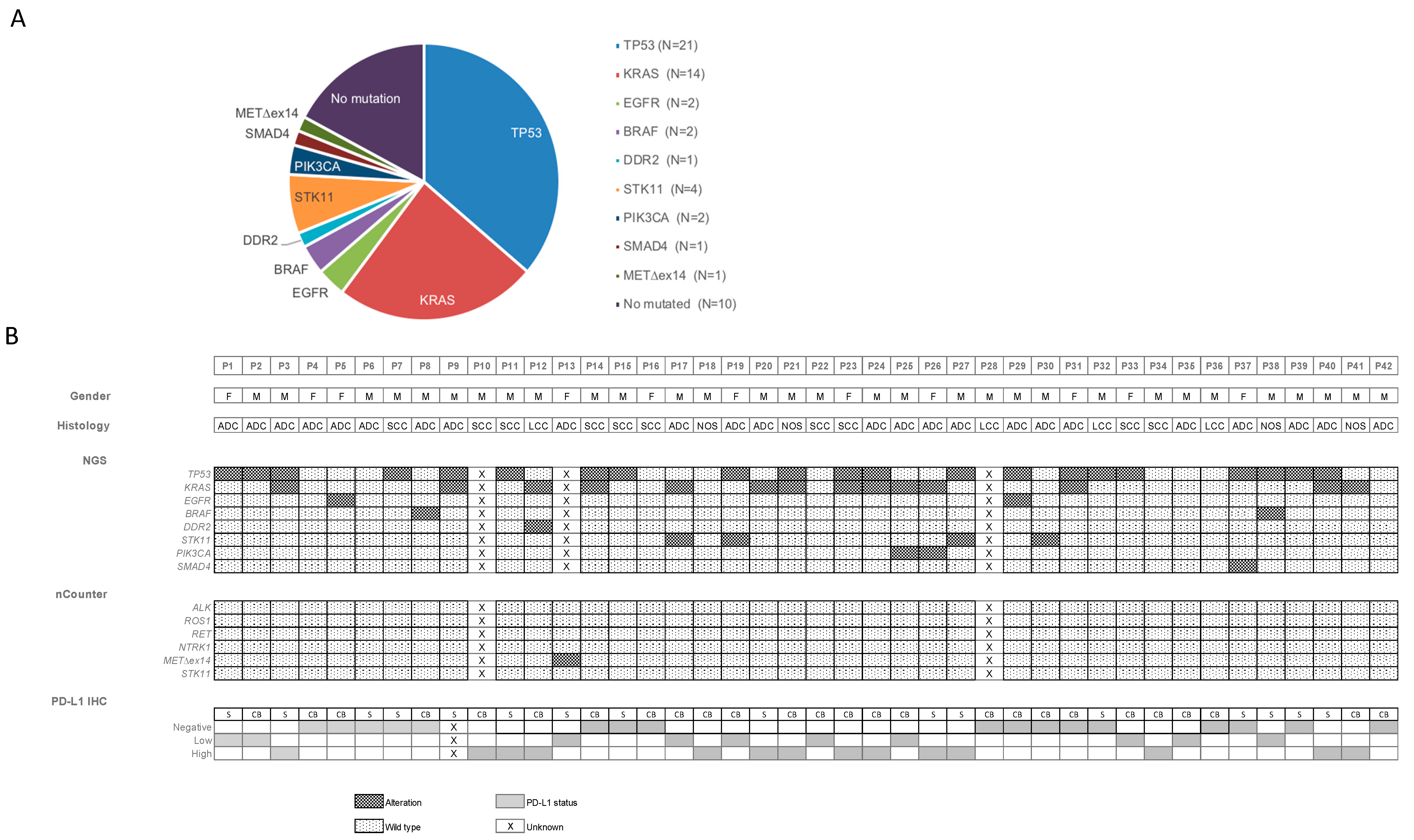
3.3. Molecular Analysis of Cytological Material Obtained by EBUS-TBNA
3.4. Comparison of Paired EBUS-TBNA Cytology and Biopsy Samples by Targeted NGS and NCounter
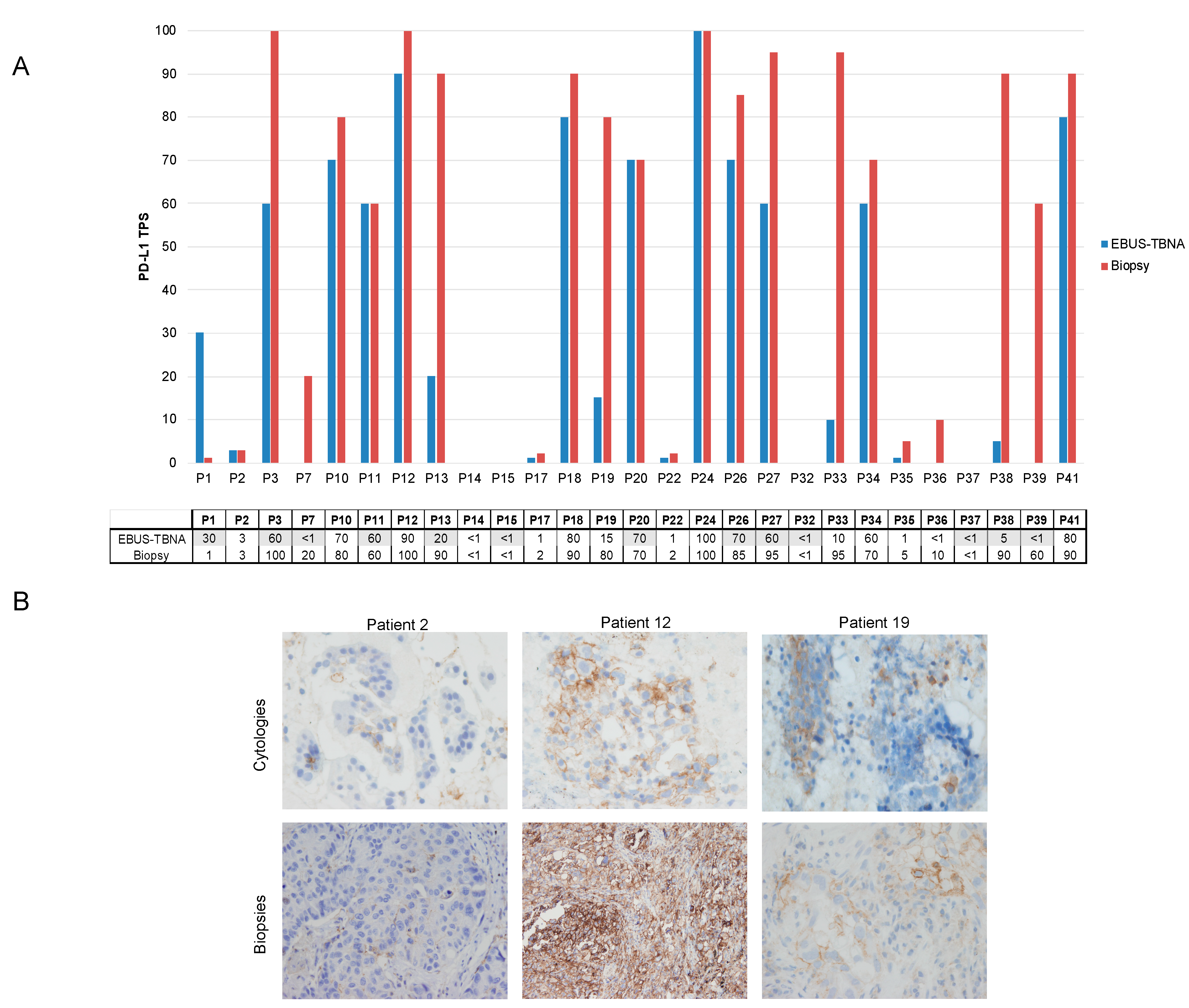
3.5. PD-L1 Expression in Paired Cytology and Biopsy Samples from Patients with Advanced NSCLC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- Reck, M.; Rabe, K.F. Precision Diagnosis and Treatment for Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 849–861. [Google Scholar] [CrossRef] [Green Version]
- Majem, M.; Juan, O.; Insa, A.; Reguart, N.; Trigo, J.M.; Carcereny, E.; García-Campelo, R.; García, Y.; Guirado, M.; Provencio, M. SEOM clinical guidelines for the treatment of non-small cell lung cancer (2018). Clin. Transl. Oncol. 2019, 21, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef] [Green Version]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B.; Biermann, W.A.; Donington, J.; Leighl, N.B.; Lew, M.; Pantelas, J.; Ramalingam, S.S.; Reck, M.; et al. Molecular Testing Guideline for the Selection of Patients With Lung Cancer for Treatment With Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 911–919. [Google Scholar] [CrossRef]
- Garrido, P.; Conde, E.; De Castro, J.; Gómez-Román, J.J.; Felip, E.; Pijuan, L.; Isla, D.; Sanz, J.; Paz-Ares, L.; López-Ríos, F. Updated guidelines for predictive biomarker testing in advanced non-small-cell lung cancer: A National Consensus of the Spanish Society of Pathology and the Spanish Society of Medical Oncology. Clin. Transl. Oncol. 2020, 22, 989–1003. [Google Scholar] [CrossRef] [Green Version]
- Teixidó, C.; Giménez-Capitán, A.; Molina-Vila, M. Ángel; Peg, V.; Karachaliou, N.; Rodríguez-Capote, A.; Castellví, J.; Rosell, R. RNA Analysis as a Tool to Determine Clinically Relevant Gene Fusions and Splice Variants. Arch. Pathol. Lab. Med. 2018, 142, 474–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navani, N.; Nankivell, M.; Lawrence, D.R.; Lock, S.; Makker, H.; Baldwin, D.R.; Stephens, R.J.; Parmar, M.K.; Spiro, S.G.; Morris, S.; et al. Lung cancer diagnosis and staging with endobronchial ultrasound-guided transbronchial needle aspiration compared with conventional approaches: An open-label, pragmatic, randomised controlled trial. Lancet Respir. Med. 2015, 3, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Jurado, J.; Saqi, A.; Maxfield, R.; Newmark, A.; Lavelle, M.; Bacchetta, M.; Gorenstein, L.; Dovidio, F.; Ginsburg, M.E.; Sonett, J.; et al. The Efficacy of EBUS-Guided Transbronchial Needle Aspiration for Molecular Testing in Lung Adenocarcinoma. Ann. Thorac. Surg. 2013, 96, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Casadio, C.; Guarize, J.; Donghi, S.; Di Tonno, C.; Fumagalli, C.; Vacirca, D.; Dell’Orto, P.; De Marinis, F.; Spaggiari, L.; Viale, G.; et al. Molecular Testing for Targeted Therapy in Advanced Non–Small Cell Lung Cancer: Suitability of Endobronchial Ultrasound Transbronchial Needle Aspiration. Am. J. Clin. Pathol. 2015, 144, 629–634. [Google Scholar] [CrossRef]
- Righi, L.; Franzi, F.; Montarolo, F.; Gatti, G.; Bongiovanni, M.; Sessa, F.; La Rosa, S. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA)—from morphology to molecular testing. J. Thorac. Dis. 2017, 9, S395–S404. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Bussy, S.; Labarca, G.; Pires, Y.; Caviedes, I.; Burotto, M. Molecular Testing of EGFR, EGFR Resistance Mutation, ALK and ROS1 Achieved by EBUS-TBNA in Chile. Arch. Bronconeumol. (Engl. Ed.) 2017, 53, 172–174. [Google Scholar] [CrossRef]
- Roy-Chowdhuri, S.; Dacic, S.; Ghofrani, M.; Illei, P.B.; Layfield, L.J.; Lee, C.; Michael, C.W.; Miller, R.A.; Mitchell, J.W.; Nikolic, B.; et al. Collection and Handling of Thoracic Small Biopsy and Cytology Specimens for Ancillary Studies: Guideline From the College of American Pathologists in Collaboration With the American College of Chest Physicians, Association for Molecular Pathology, American Society of Cytopathology, American Thoracic Society, Pulmonary Pathology Society, Papanicolaou Society of Cytopathology, Society of Interventional Radiology, and Society of Thoracic Radiology. Arch. Pathol. Lab. Med. 2020, 144, 933–958. [Google Scholar] [CrossRef]
- Dietel, M.; Bubendorf, L.; Dingemans, A.-M.C.; Dooms, C.; Elmberger, G.; García, R.C.; Kerr, K.M.; Lim, E.; López-Ríos, F.; Thunnissen, E.; et al. Diagnostic procedures for non-small-cell lung cancer (NSCLC): Recommendations of the European Expert Group. Thorax 2016, 71, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy-Chowdhuri, S.; Aisner, D.L.; Allen, T.C.; Beasley, M.B.; Borczuk, A.; Cagle, P.T.; Capelozzi, V.; Dacic, S.; Santos, G.D.C.; Hariri, L.P.; et al. Biomarker Testing in Lung Carcinoma Cytology Specimens: A Perspective from Members of the Pulmonary Pathology Society. Arch. Pathol. Lab. Med. 2016, 140, 1267–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thunnissen, E.; Kerr, K.M.; Herth, F.J.; Lantuejoul, S.; Papotti, M.; Rintoul, R.C.; Rossi, G.; Skov, B.G.; Weynand, B.; Bubendorf, L.; et al. The challenge of NSCLC diagnosis and predictive analysis on small samples. Practical approach of a working group. Lung Cancer 2012, 76, 1–18. [Google Scholar] [CrossRef]
- Marin, E.; Teixido, C.; Carmona-Rocha, E.; Reyes, R.; Arcocha, A.; Viñolas, N.; Rodríguez-Mues, M.; Cabrera, C.; Sánchez, M.; Vollmer, I.; et al. Usefulness of Two Independent DNA and RNA Tissue-Based Multiplex Assays for the Routine Care of Advanced NSCLC Patients. Cancers 2020, 12, 1124. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Castillo, P.; Marginet, M.; Jares, P.; García, M.; Gonzalvo, E.; Arance, A.; García, A.; Alos, L.; Teixidó, C. Implementation of an NGS panel for clinical practice in paraffin-embedded tissue samples from locally advanced and metastatic melanoma patients. Explor. Target Antitumor Ther. 2020, 1, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Reguart, N.; Teixidó, C.; Giménez-Capitán, A.; Paré, L.; Galván, P.; Viteri, S.; Rodríguez, S.; Peg, V.; Aldeguer, E.; Viñolas, N.; et al. Prat A. Identification of ALK, ROS1, and RET fusions by a multiplexed mRNA-based assay in formalin-fixed, paraffin-embedded samples from advanced non-small-cell lung cancer patients. Clin. Chem. 2017, 63, 751–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixidó, C.; Vilariño, N.; Reyes, R.; Reguart, N. PD-L1 expression testing in non-small cell lung cancer. Ther. Adv. Med. Oncol. 2018, 10, 1758835918763493. [Google Scholar] [CrossRef] [PubMed]
- Reguart, N.; Teixidó, C.; Giménez-Capitán, A.; Vilariño, N.; Arcocha, A.; Jares, P.; Castillo, S.; Bernal, X.; Muñoz, S.; Palmero, R.; et al. Prat A. P1.01-075 Simultaneous Multiplex Profiling of Gene Fusions, METe14 Mutations and Immune Genes in Advanced NSCLC by NCounter Technology. J. Thoracic Oncol. 2017, 12, S1923. [Google Scholar] [CrossRef]
- Raad, S.; Hanna, N.; Jalal, S.; Bendaly, E.; Zhang, C.; Nuguru, S.; Oueini, H.; Diab, K. Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration Use for Subclassification and Genotyping of Lung Non-Small-Cell Carcinoma. South. Med. J. 2018, 111, 484–488. [Google Scholar] [CrossRef]
- Turner, S.R.; Buonocore, D.; Desmeules, P.; Rekhtman, N.; Dogan, S.; Lin, O.; Arcila, M.E.; Jones, D.R.; Huang, J. Feasibility of endobronchial ultrasound transbronchial needle aspiration for massively parallel next-generation sequencing in thoracic cancer patients. Lung Cancer 2018, 119, 85–90. [Google Scholar] [CrossRef]
- Stoy, S.P.; Segal, J.P.; Mueller, J.; Furtado, L.V.; Vokes, E.E.; Patel, J.D.; Murgu, S. Feasibility of Endobronchial Ultrasound-guided Transbronchial Needle Aspiration Cytology Specimens for Next Generation Sequencing in Non–small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, 230–238.e2. [Google Scholar] [CrossRef]
- Biswas, A.; Leon, M.E.; Drew, P.; Fernandez-Bussy, S.; Furtado, L.V.; Jantz, M.A.; Mehta, H.J. Clinical performance of endobronchial ultrasound-guided transbronchial needle aspiration for assessing programmed death ligand-1 expression in nonsmall cell lung cancer. Diagn. Cytopathol. 2018, 46, 378–383. [Google Scholar] [CrossRef]
- Fernandez-Bussy, S.; Biswas, A.; Labarca, G.; Jantz, M.A.; Mehta, H.J. Comparison of Endobronchial Ultrasound–guided Transbronchial Needle Aspiration With Stylet Retracted Partially Versus Completely for Molecular Testing. J. Bronchol. Interv. Pulmonol. 2019, 26, 222–224. [Google Scholar] [CrossRef]
- Herth, F.J.F.; Eberhardt, R.; Krasnik, M.; Ernst, A. Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration of Lymph Nodes in the Radiologically and Positron Emission Tomography-Normal Mediastinum in Patients with Lung Cancer. Chest 2008, 133, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Wahidi, M.M.; Herth, F.; Yasufuku, K.; Shepherd, R.W.; Yarmus, L.; Chawla, M.; Lamb, C.; Casey, K.R.; Patel, S.; Silvestri, G.A.; et al. Technical Aspects of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 816–835. [Google Scholar] [CrossRef] [Green Version]
- Yarmus, L.; Akulian, J.; Gilbert, C.; Feller-Kopman, D.; Lee, H.J.; Zarogoulidis, P.; Lechtzin, N.; Ali, S.Z.; Sathiyamoorthy, V. Optimizing Endobronchial Ultrasound for Molecular Analysis. How Many Passes Are Needed? Ann. Am. Thorac. Soc. 2013, 10, 636–643. [Google Scholar] [CrossRef]
- Midha, A.; Sharpe, A.; Scott, M.; Walker, J.; Shi, K.; Ballas, M.; Garassino, M.C.; Rizvi, N.A. PD-L1 expression in advanced NSCLC: Primary lesions versus metastatic sites and impact of sample age. J. Clin. Oncol. 2016, 34, 3025. [Google Scholar] [CrossRef]
- Fielding, D.; Dalley, A.J.; Bashirzadeh, F.; Singh, M.; Nandakumar, L.; Reed, A.E.M.; Black, D.; Kazakoff, S.; Pearson, J.V.; Nones, K.; et al. Diff-Quik Cytology Smears from Endobronchial Ultrasound Transbronchial Needle Aspiration Lymph Node Specimens as a Source of DNA for Next-Generation Sequencing Instead of Cell Blocks. Respiration 2019, 97, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Mineura, K.; Hamaji, M.; Yoshizawa, A.; Nakajima, N.; Kayawake, H.; Tanaka, S.; Yamada, Y.; Yutaka, Y.; Nakajima, D.; Ohsumi, A.; et al. Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration to assess tumor-programmed cell death ligand-1 expression in mediastinal lymph nodes metastasized from non-small cell lung cancer. Surg Today 2020, 50, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Jug, R.; Giovacchini, C.X.; Liu, B.; Green, C.L.; Clarke, J.M.; Mahmood, K.; Pavlisko, E.N. EBUS-FNA cytologic-histologic correlation of PD-L1 immunohistochemistry in non–small cell lung cancer. J. Am. Soc. Cytopathol. 2020, 9, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, F.; Nankivell, M.; Adizie, J.B.; Maqsood, U.; Elshafi, M.; Jafri, S.; Lerner, A.D.; Woolhouse, I.; Munavvar, M.; Evison, M.; et al. Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration for PD-L1 Testing in Non-small Cell Lung Cancer. Chest 2020, 158, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Wang, H.; Zerbo, A.; Beaudoin, S.; Ofiara, L.; Fiset, P.-O.; Benedetti, A.; Gonzalez, A.V. Programmed Death Ligand 1 Testing of Endobronchial Ultrasound–guided Transbronchial Needle Aspiration Samples Acquired for the Diagnosis and Staging of Non–Small Cell Lung Cancer. J. Bronchol. Interv. Pulmonol. 2020, 27, 50–57. [Google Scholar] [CrossRef]
- Xie, F.; Zheng, X.; Mao, X.; Zhao, R.; Ye, J.; Zhang, Y.; Sun, J. Next-Generation Sequencing for Genotyping of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration Samples in Lung Cancer. Ann Thorac. Surg 2019, 108, 219–226. [Google Scholar] [CrossRef]
- Yoshimura, K.; Inoue, Y.; Karayama, M.; Tsuchiya, K.; Mori, K.; Suzuki, Y.; Iwashita, Y.; Kahyo, T.; Kawase, A.; Tanahashi, M.; et al. Heterogeneity analysis of PD-L1 expression and copy number status in EBUS-TBNA biopsy specimens of non-small cell lung cancer: Comparative assessment of primary and metastatic sites. Lung Cancer 2019, 134, 202–209. [Google Scholar] [CrossRef]
- Wang, G.; Ionescu, D.N.; Lee, C.-H.; Hiruki, T.; Myers, R.; Shaipanich, T.; Lam, S.; Melosky, B.; Zhou, C. PD-L1 testing on the EBUS-FNA cytology specimens of non-small cell lung cancer. Lung Cancer 2019, 136, 1–5. [Google Scholar] [CrossRef]
- Sakata, K.K.; Midthun, D.E.; Mullon, J.J.; Kern, R.M.; Nelson, D.R.; Edell, E.S.; Schiavo, D.N.; Jett, J.R.; Aubry, M.C. Comparison of Programmed Death Ligand-1 Immunohistochemical Staining Between Endobronchial Ultrasound Transbronchial Needle Aspiration and Resected Lung Cancer Specimens. Chest 2018, 154, 827–837. [Google Scholar] [CrossRef]
- Ghigna, M.R.; Crutu, A.; Florea, V.; Feuillet-Soummer, S.; Baldeyrou, P.; Adam, J.; Lacroix, L.; Besse, B.; Mercier, O.; Fadel, E.; et al. Endobronchial ultrasound-guided fine-needle aspiration for pulmonary carcinomas genotyping: Experience with 398 cases including rapid. J. Thorac. Dis. 2018, 10, 4653–4658. [Google Scholar] [CrossRef]
- Sakakibara, R.; Inamura, K.; Tambo, Y.; Ninomiya, H.; Kitazono, S.; Yanagitani, N.; Horiike, A.; Ohyanagi, F.; Matsuura, Y.; Nakao, M.; et al. EBUS-TBNA as a Promising Method for the Evaluation of Tumor PD-L1 Expression in Lung Cancer. Clin. Lung Cancer 2017, 18, 527–534.e1. [Google Scholar] [CrossRef]
- Skov, B.G.; Skov, T. Paired Comparison of PD-L1 Expression on Cytologic and Histologic Specimens from Malignancies in the Lung Assessed With PD-L1 IHC 28-8pharmDx and PD-L1 IHC 22C3pharmDx. Appl. Immunohistochem. Mol. Morphol. 2017, 25, 453–459. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.K.; Han, G.; Schalper, K.A.; Carvajal-Hausdorf, D.; Pelekanou, V.; Rehman, J.; Velcheti, V.; Herbst, R.S.; Lorusso, P.M.; Rimm, D.L. Quantitative Assessment of the Heterogeneity of PD-L1 Expression in Non–Small-Cell Lung Cancer. JAMA Oncol. 2016, 2, 46–54. [Google Scholar] [CrossRef]
- Casadevall, D.; Clavé, S.; Taus, Á.; Hardy-Werbin, M.; Rocha, P.; Lorenzo, M.; Menéndez, S.; Salido, M.; Albanell, J.; Pijuan, L.; et al. Heterogeneity of Tumor and Immune Cell PD-L1 Expression and Lymphocyte Counts in Surgical NSCLC Samples. Clin. Lung Cancer 2017, 18, 682–691.e5. [Google Scholar] [CrossRef] [PubMed]
- Ben Dori, S.; Aizic, A.; Sabo, E.; Hershkovitz, D. Spatial heterogeneity of PD-L1 expression and the risk for misclassification of PD-L1 immunohistochemistry in non-small cell lung cancer. Lung Cancer 2020, 147, 91–98. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. (%) or Mean (Range) | |
|---|---|
| Age (years) | 67.1 (52–83) |
| Sex | |
| Male | 31 (73.8) |
| Female | 11 (26.2) |
| Smoking status | |
| Current | 20 (47.6) |
| Former | 17 (40.5) |
| Never | 5 (11.9) |
| Staging by CT or PET | |
| IIIA | 4 (9.5) |
| IIIB | 12 (28.5) |
| IIIC | 2 (4.8) |
| IVA | 6 (14.3) |
| IVB | 18 (42.9) |
| Histological type | |
| Adenocarcinoma | 24 (57.2) |
| Squamous cell carcinoma | 10 (23.8) |
| Non-otherwise specified | 4 (9.5) |
| Large cell carcinoma | 4 (9.5) |
| EBUS Findings | No. (%) or Mean (Range) |
|---|---|
| Regions sampled | 78 |
| Nodes | 63 (80.8%) |
| Mediastinal | |
| Subcarinal | 22 (28.2) |
| Right lower paratracheal | 19 (24.3) |
| Left lower paratracheal | 7 (9.0) |
| Right higher paratracheal | 2 (2.6) |
| Lobar | |
| Right interlobar | 7 (9.0) |
| Left interlobar | 3 (3.8) |
| Right hilar | 2 (2.6) |
| Left hilar | 1 (1.3) |
| Peribronchial primary tumor mass | 15 (19.2) |
| Number passes per each node station/site | 6 (1–13) |
| Lymph node characteristics | |
| Size by EBUS (mm) | 13.7 (5.9–32.7) |
| SUV by PET | 16.9 (0.0–48.5) |
| Biopsy | ||||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| EBUS-TBNA | Positive | 18 Φ | 0 | 18 |
| Negative | 0 | 5 | 5 | |
| Total | 18 | 5 | 23 | |
| Biopsy | |||||
|---|---|---|---|---|---|
| Negative | Low-Positive | High-Positive | Total | ||
| EBUS-TBNA | Negative | 4 | 2 | 1 | 7 |
| Low-positive | 0 | 5 | 4 | 9 | |
| High-positive | 0 | 0 | 11 | 11 | |
| Total | 4 | 7 | 16 | 27 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin-Deleon, R.; Teixido, C.; Lucena, C.M.; Martinez, D.; Fontana, A.; Reyes, R.; García, M.; Viñolas, N.; Vollmer, I.; Sanchez, M.; et al. EBUS-TBNA Cytological Samples for Comprehensive Molecular Testing in Non–Small Cell Lung Cancer. Cancers 2021, 13, 2084. https://doi.org/10.3390/cancers13092084
Martin-Deleon R, Teixido C, Lucena CM, Martinez D, Fontana A, Reyes R, García M, Viñolas N, Vollmer I, Sanchez M, et al. EBUS-TBNA Cytological Samples for Comprehensive Molecular Testing in Non–Small Cell Lung Cancer. Cancers. 2021; 13(9):2084. https://doi.org/10.3390/cancers13092084
Chicago/Turabian StyleMartin-Deleon, Roberto, Cristina Teixido, Carmen Mª Lucena, Daniel Martinez, Ainhoa Fontana, Roxana Reyes, Mireia García, Nuria Viñolas, Ivan Vollmer, Marcelo Sanchez, and et al. 2021. "EBUS-TBNA Cytological Samples for Comprehensive Molecular Testing in Non–Small Cell Lung Cancer" Cancers 13, no. 9: 2084. https://doi.org/10.3390/cancers13092084