
Association between Lipid Profiles and the Incidence of Hepatocellular Carcinoma: A Nationwide Population-Based Study

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Ethics Statement
2.3. Study Population
2.4. Definition of HCC
2.5. Measurement of Cholesterol Levels
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
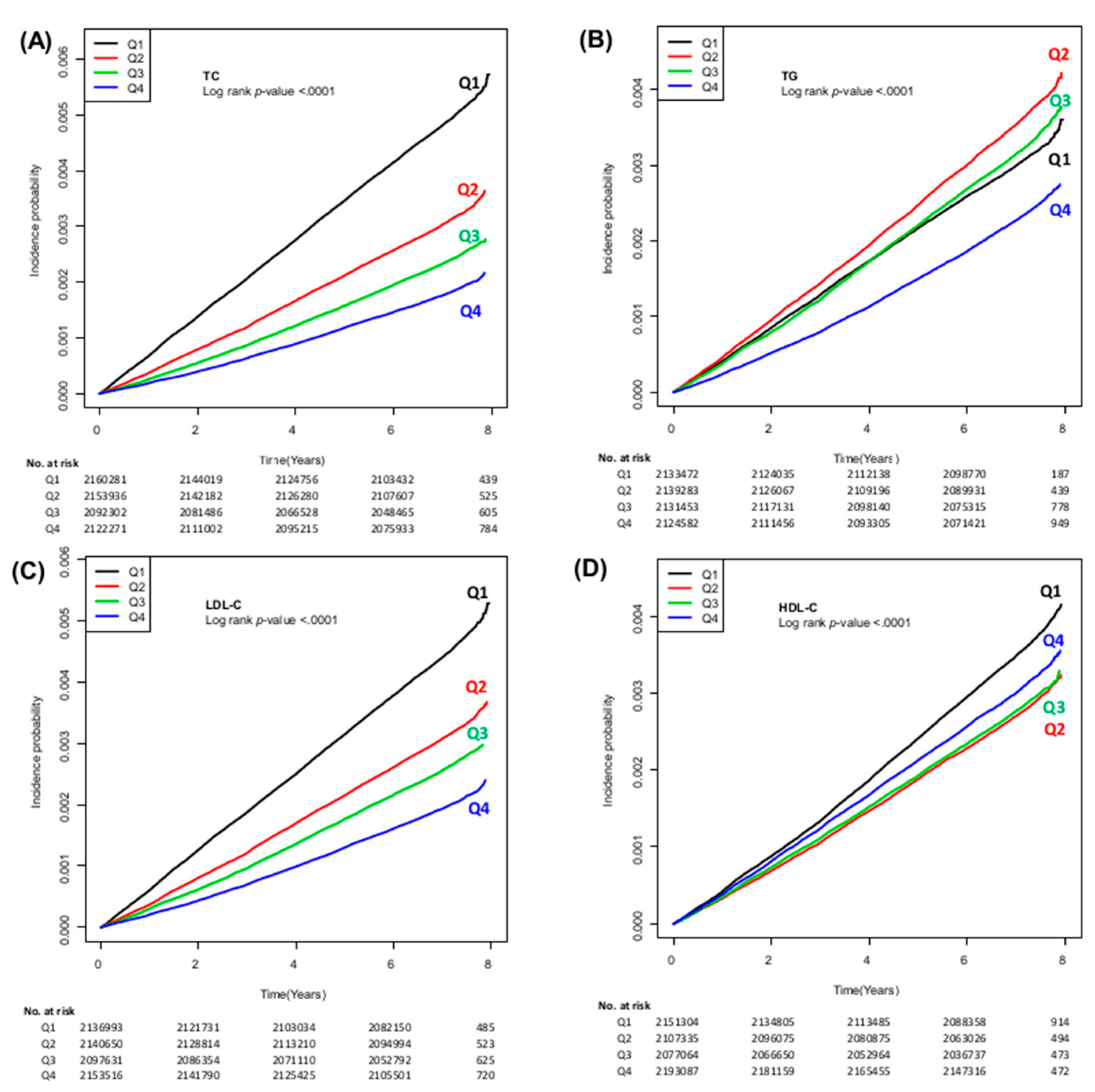
3.2. Incidence of HCC According to Lipid Profiles
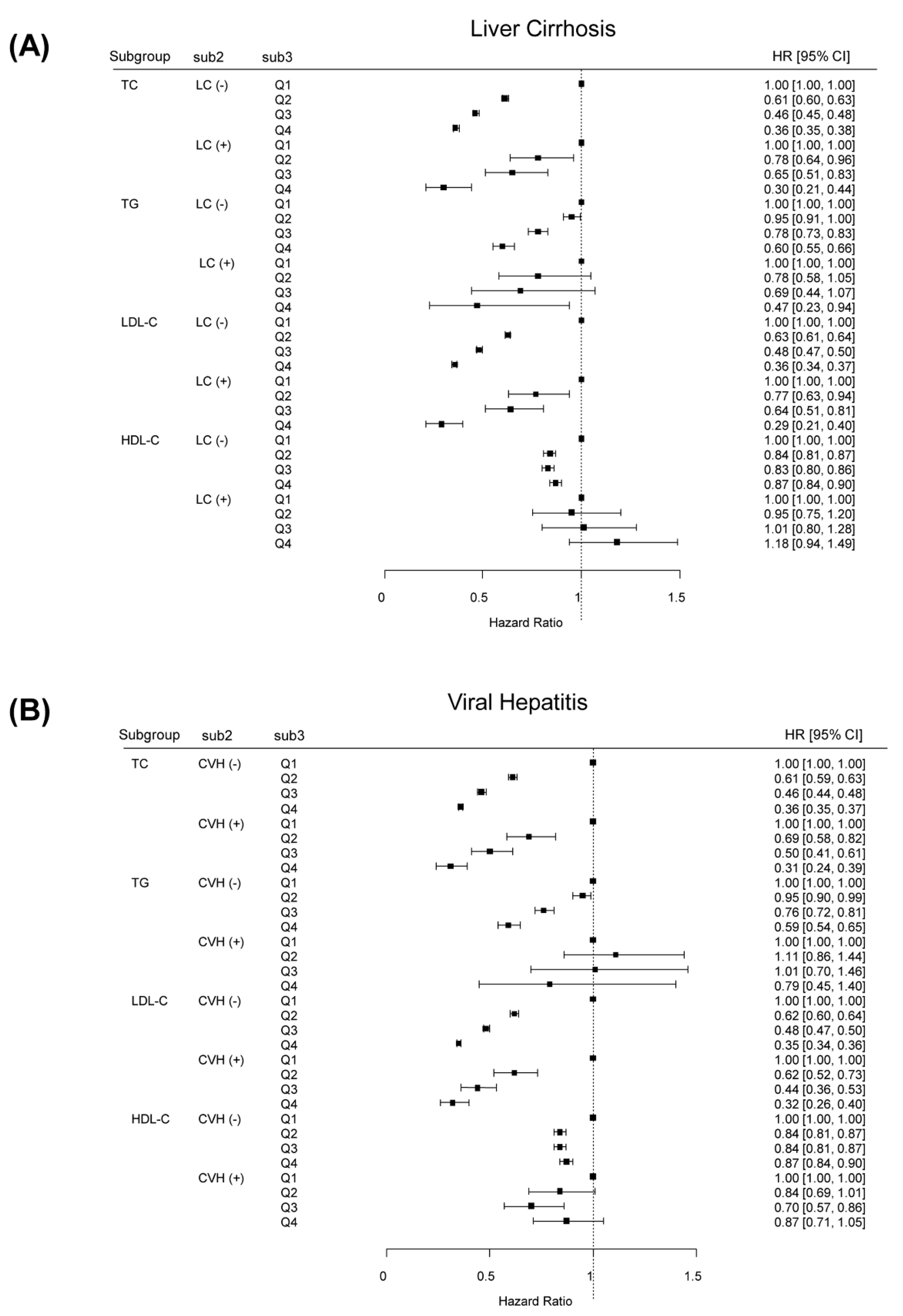
3.3. Stratified Analyses by the Presence of LC, Viral Hepatitis or Gender
3.4. Sensitivity Analysis
3.5. Incidence of HCC According to Lipid Profiles among Subjects Taking Statin
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krause, M.R.; Regen, S.L. The structural role of cholesterol in cell membranes: From condensed bilayers to lipid rafts. Acc. Chem. Res. 2014, 47, 3512–3521. [Google Scholar] [CrossRef]
- Long, J.; Zhang, C.J.; Zhu, N.; Du, K.; Yin, Y.F.; Tan, X.; Liao, D.F.; Qin, L. Lipid metabolism and carcinogenesis, cancer development. Am. J. Cancer Res. 2018, 8, 778–791. [Google Scholar] [PubMed]
- Yang, C.; Tian, G.; Mi, J.; Wei, X.; Li, X.; Li, X.; Wang, W.; Wang, B. Causal relevance of circulating high-density lipoprotein cholesterol with cancer: A Mendelian randomization meta-analysis. Sci. Rep. 2015, 5, 9495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benn, M.; Tybjaerg-Hansen, A.; Stender, S.; Frikke-Schmidt, R.; Nordestgaard, B.G. Low-density lipoprotein cholesterol and the risk of cancer: A mendelian randomization study. J. Natl. Cancer Inst. 2011, 103, 508–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motta, M.; Giugno, I.; Ruello, P.; Pistone, G.; Di Fazio, I.; Malaguarnera, M. Lipoprotein (a) behaviour in patients with hepatocellular carcinoma. Minerva Med. 2001, 92, 301–305. [Google Scholar] [PubMed]
- Ooi, K.; Shiraki, K.; Sakurai, Y.; Morishita, Y.; Nobori, T. Clinical significance of abnormal lipoprotein patterns in liver diseases. Int. J. Mol. Med. 2005, 15, 655–660. [Google Scholar] [CrossRef]
- Kanel, G.C.; Radvan, G.; Peters, R.L. High-density lipoprotein cholesterol and liver disease. Hepatology 1983, 3, 343–348. [Google Scholar] [CrossRef]
- Eisenberg, S.; Levy, R.I. Lipoprotein metabolism. Adv. Lipid Res. 1975, 13, 1–89. [Google Scholar]
- Korean Association for the Study of the Liver. KASL clinical practice guidelines for liver cirrhosis: Varices, hepatic encephalopathy, and related complications. Clin. Mol. Hepatol. 2020, 26, 83–127. [Google Scholar] [CrossRef]
- Jiang, S.S.; Weng, D.S.; Jiang, L.; Zhang, Y.J.; Pan, K.; Pan, Q.Z.; Chen, C.L.; Zhao, J.J.; Zhang, X.F.; Zhang, H.X.; et al. The clinical significance of preoperative serum cholesterol and high-density lipoprotein-cholesterol levels in hepatocellular carcinoma. J. Cancer 2016, 7, 626–632. [Google Scholar] [CrossRef] [Green Version]
- Kitahara, C.M.; De González, A.B.; Freedman, N.D.; Huxley, R.; Mok, Y.; Jee, S.H.; Samet, J.M. Total cholesterol and cancer risk in a large prospective study in Korea. J. Clin. Oncol. 2011, 29, 1592–1598. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.M.; Jang, W.; Shin, D.W. Association of statin use with Parkinson’s disease: Dose-response relationship. Mov. Disord. 2019, 34, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Soh, H.; Im, J.P.; Han, K.; Park, S.; Hong, S.W.; Moon, J.M.; Kang, E.A.; Chun, J.; Lee, H.J.; Kim, J.S. Crohn’s disease and ulcerative colitis are associated with different lipid profile disorders: A nationwide population-based study. Aliment. Pharmacol. Ther. 2020, 51, 446–456. [Google Scholar] [CrossRef]
- Lee, J.; Jang, S.; Jeong, H.; Ryu, O.H. Validation of the Friedewald formula for estimating low density lipoprotein cholesterol: The Korea National Health and Nutrition Examination Survey, 2009 to 2011. Korean J. Intern. Med. 2020, 35, 150–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.K.; Seeger, J.D. Lipid profiles among US elderly with untreated rheumatoid arthritis--the Third National Health and Nutrition Examination Survey. J. Rheumatol. 2005, 32, 2311–2316. [Google Scholar] [PubMed]
- Borba, E.F.; Bonfa, E. Dyslipoproteinemias in systemic lupus erythematosus: Influence of disease, activity, and anticardiolipin antibodies. Lupus 1997, 6, 533–539. [Google Scholar] [CrossRef]
- Michiel, D.F.; Oppenheim, J.J. Cytokines as positive and negative regulators of tumor promotion and progression. Semin. Cancer Biol. 1992, 3, 3–15. [Google Scholar] [PubMed]
- Norata, G.D.; Pirillo, A.; Ammirati, E.; Catapano, A.L. Emerging role of high density lipoproteins as a player in the immune system. Atherosclerosis 2012, 220, 11–21. [Google Scholar] [CrossRef]
- Qin, W.H.; Yang, Z.S.; Li, M.; Chen, Y.; Zhao, X.F.; Qin, Y.Y.; Song, J.Q.; Wang, B.B.; Yuan, B.; Cui, X.L.; et al. High Serum Levels of Cholesterol Increase Antitumor Functions of Nature Killer Cells and Reduce Growth of Liver Tumors in Mice. Gastroenterology 2020, 158, 1713–1727. [Google Scholar] [CrossRef]
- Krisans, S.K. Cell compartmentalization of cholesterol biosynthesis. Ann. N. Y. Acad. Sci. 1996, 804, 142–164. [Google Scholar] [CrossRef]
- Siemianowicz, K.; Gminski, J.; Stajszczyk, M.; Wojakowski, W.; Goss, M.; Machalski, M.; Telega, A.; Brulinski, K.; Magiera-Molendowska, H. Serum total cholesterol and triglycerides levels in patients with lung cancer. Int. J. Mol. Med. 2000, 5, 201–205. [Google Scholar] [CrossRef]
- Cooper, M.E.; Akdeniz, A.; Hardy, K.J. Effects of liver transplantation and resection on lipid parameters: A longitudinal study. Aust. N. Z. J. Surg. 1996, 66, 743–746. [Google Scholar] [CrossRef]
- Lewis, G.F.; Rader, D.J. New insights into the regulation of HDL metabolism and reverse cholesterol transport. Circ. Res. 2005, 96, 1221–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.H.; Plank, L.D.; Suk, K.T.; Park, Y.E.; Lee, J.; Choi, J.H.; Heo, N.Y.; Park, J.; Kim, T.O.; Moon, Y.S.; et al. Trends in the prevalence of chronic liver disease in the Korean adult population, 1998–2017. Clin. Mol. Hepatol. 2020, 26, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Cicognani, C.; Malavolti, M.; Morselli-Labate, A.M.; Zamboni, L.; Sama, C.; Barbara, L. Serum lipid and lipoprotein patterns in patients with liver cirrhosis and chronic active hepatitis. Arch. Intern. Med. 1997, 157, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Alsabti, E.A. Serum lipids in hepatoma. Oncology 1979, 36, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Ahaneku, J.E.; Taylor, G.O.; Olubuyide, I.O.; Agbedana, E.O. Abnormal lipid and lipoprotein patterns in liver cirrhosis with and without hepatocellular carcinoma. J. Pak. Med. Assoc. 1992, 42, 260–263. [Google Scholar] [PubMed]
- Eggens, I.; Ekstrom, T.J.; Aberg, F. Studies on the biosynthesis of polyisoprenols, cholesterol and ubiquinone in highly differentiated human hepatomas. J. Exp. Pathol. 1990, 71, 219–232. [Google Scholar]
- Baenke, F.; Peck, B.; Miess, H.; Schulze, A. Hooked on fat: The role of lipid synthesis in cancer metabolism and tumour development. Dis. Models Mech. 2013, 6, 1353–1363. [Google Scholar] [CrossRef] [Green Version]
- Tosi, M.R.; Tugnoli, V. Cholesteryl esters in malignancy. Clin. Chim. Acta 2005, 359, 27–45. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HCC | |||
|---|---|---|---|
| No | Yes | p-Value | |
| n | 8,501,899 | 26,891 | |
| Age, years | 45.4 ± 13.8 | 57.8 ± 11.2 | <0.0001 |
| Male (%) | 4,762,306 (56.1) | 21,023 (78.2) | <0.0001 |
| Lowest income quintile (%) | 2,255,880 (26.5) | 7378 (27.4) | 0.0008 |
| Urban residence (%) | 3,891,641 (45.8) | 12,127 (45.1) | 0.03 |
| Smoking status | <0.0001 | ||
| Never-smoker (%) | 4,976,898 (58.5) | 11,861 (44.1) | |
| Ex-smoker (%) | 1,183,381 (13.9) | 5604 (20.8) | |
| Current smoker (%) | 2,341,620 (27.5) | 9426 (35.1) | |
| Alcohol consumption | <0.0001 | ||
| Complete or near abstinence (%) | 4,191,220 (49.3) | 13,054 (48.5) | |
| Moderate consumption (%) | 3,615,635 (42.5) | 10,131 (37.7) | |
| Heavy consumption (%) | 695,044 (8.2) | 3706 (13.8) | |
| Regular physical activity (%) | 1,496,016 (17.6) | 5516 (20.5) | <0.0001 |
| BMI, kg/m2 | 23.5 ± 3.2 | 24.1 ± 3.1 | <0.0001 |
| WC, cm | 79.7 ± 9.0 | 83.8 ± 8.4 | <0.0001 |
| SBP, mmHg | 121.6 ± 14.7 | 127.0 ± 15.7 | <0.0001 |
| DBP, mmHg | 76.0 ± 9.9 | 78.3 ± 10.2 | <0.0001 |
| Comorbidities | |||
| Hypertension (%) | 1,775,635 (20.9) | 10,815 (40.2) | <0.0001 |
| DM (%) | 522,711 (6.2) | 5726 (21.3) | <0.0001 |
| Dyslipidemia (%) | 808,069 (9.5) | 1568 (5.8) | <0.0001 |
| Liver cirrhosis (%) | 5838 (0.1) | 561 (2.1) | <0.0001 |
| Viral hepatitis (%) | 85,562 (1.0) | 806 (3) | <0.0001 |
| Chronic kidney disease (%) | 427,518 (5.0) | 1933 (7.2) | <0.0001 |
| Fenofibrate medication (%) | 31,486 (0.4) | 141 (0.5) | <0.0001 |
| Laboratory results | |||
| Fasting glucose (mg/dL) | 95.5 ± 20.6 | 106.3 ± 33.5 | <0.0001 |
| Total cholesterol (mg/dL) | 193.0 ± 34.0 | 179.4 ± 34.3 | <0.0001 |
| TG (mg/dL) | 129.2 ± 88.2 | 119.9 ± 78.1 | <0.0001 |
| LDL-C (mg/dL) | 111.9 ± 31.5 | 102.0 ± 31.4 | <0.0001 |
| HDL-C (mg/dL) | 55.1 ± 13.9 | 53.1 ± 14.6 | <0.0001 |
| HCC Cases (n) | Incidence of HCC (100,000 Person-(100,000 Person-Years) | Crude HR (95% CI) | Adjusted HR a (95% CI) | p-Value | |
|---|---|---|---|---|---|
| TC (mg/dL) | |||||
| Q1 (0–169) | 10,839 | 69.22 | 1 (reference) | 1 (reference) | |
| Q2 (170–191) | 6891 | 43.98 | 0.64 (0.62–0.66) | 0.61 (0.59–0.63) | <0.0001 |
| Q3 (200–214) | 5170 | 33.94 | 0.49 (0.47–0.51) | 0.46 (0.44–0.47) | <0.0001 |
| Q4 (≥215) | 3991 | 25.84 | 0.37 (0.36–0.39) | 0.36 (0.34–0.37) | <0.0001 |
| TG (mg/dL) | |||||
| Q1 (0–72) | 6711 | 43.17 | 1 (reference) | 1 (reference) | |
| Q2 (73–105) | 7969 | 51.24 | 1.19 (1.15–1.23) | 0.95 (0.91–0.99) | <0.0001 |
| Q3 (106–157) | 7078 | 45.72 | 1.06 (1.02–1.09) | 0.77 (0.72–0.82) | <0.0001 |
| Q4 (≥158) | 5133 | 33.26 | 0.77 (0.74–0.80) | 0.59 (0.54–0.65) | <0.0001 |
| LDL-C (mg/dL) | |||||
| Q1 (0–90) | 9846 | 63.58 | 1 (reference) | 1 (reference) | |
| Q2 (91–110) | 6923 | 44.46 | 0.70 (0.68–0.72) | 0.62 (0.60–0.64) | <0.0001 |
| Q3 (111–131) | 5678 | 37.18 | 0.58 (0.57–0.60) | 0.48 (0.46–0.50) | <0.0001 |
| Q4 (≥132) | 4444 | 28.34 | 0.45 (0.43–0.46) | 0.35 (0.34–0.36) | <0.0001 |
| HDL-C (mg/dL) | |||||
| Q1 (0–48) | 7891 | 50.51 | 1 (reference) | 1 (reference) | |
| Q2 (49–57) | 6022 | 39.24 | 0.78 (0.75–0.80) | 0.84 (0.81–0.86) | <0.0001 |
| Q3 (58–66) | 6046 | 40.0 | 0.79 (0.77–0.82) | 0.83 (0.80–0.86) | <0.0001 |
| Q4 (≥67) | 6932 | 43.53 | 0.86 (0.84–0.89) | 0.87 (0.84–0.90) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, Y.; Cho, E.J.; Yoo, J.-J.; Chang, Y.; Chung, G.E.; Jeong, S.-M.; Park, S.-H.; Han, K.; Shin, D.W.; Yu, S.J. Association between Lipid Profiles and the Incidence of Hepatocellular Carcinoma: A Nationwide Population-Based Study. Cancers 2021, 13, 1599. https://doi.org/10.3390/cancers13071599
Cho Y, Cho EJ, Yoo J-J, Chang Y, Chung GE, Jeong S-M, Park S-H, Han K, Shin DW, Yu SJ. Association between Lipid Profiles and the Incidence of Hepatocellular Carcinoma: A Nationwide Population-Based Study. Cancers. 2021; 13(7):1599. https://doi.org/10.3390/cancers13071599
Chicago/Turabian StyleCho, Yuri, Eun Ju Cho, Jeong-Ju Yoo, Young Chang, Goh Eun Chung, Su-Min Jeong, Sang-Hyun Park, Kyungdo Han, Dong Wook Shin, and Su Jong Yu. 2021. "Association between Lipid Profiles and the Incidence of Hepatocellular Carcinoma: A Nationwide Population-Based Study" Cancers 13, no. 7: 1599. https://doi.org/10.3390/cancers13071599