
Early Detection of Local Tumor Progression after Irreversible Electroporation (IRE) of Hepatocellular Carcinoma Using Gd-EOB-DTPA-Based MR Imaging at 3T

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
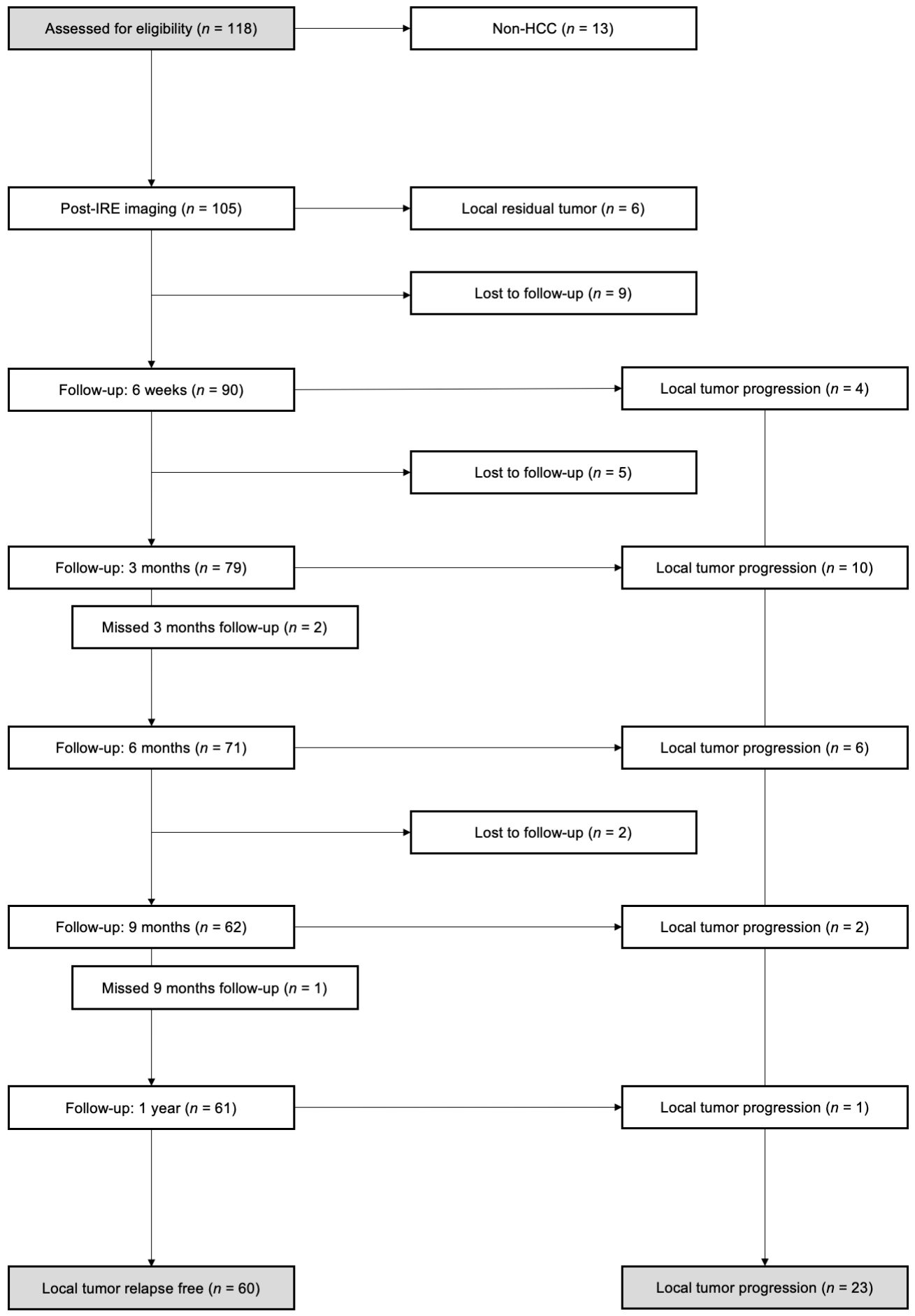
2.1. Study Design, Patient Selection and Patient Characteristics
2.2. Irreversible Electroporation (IRE)
2.3. Image Acquisition
2.4. Statistical Analysis
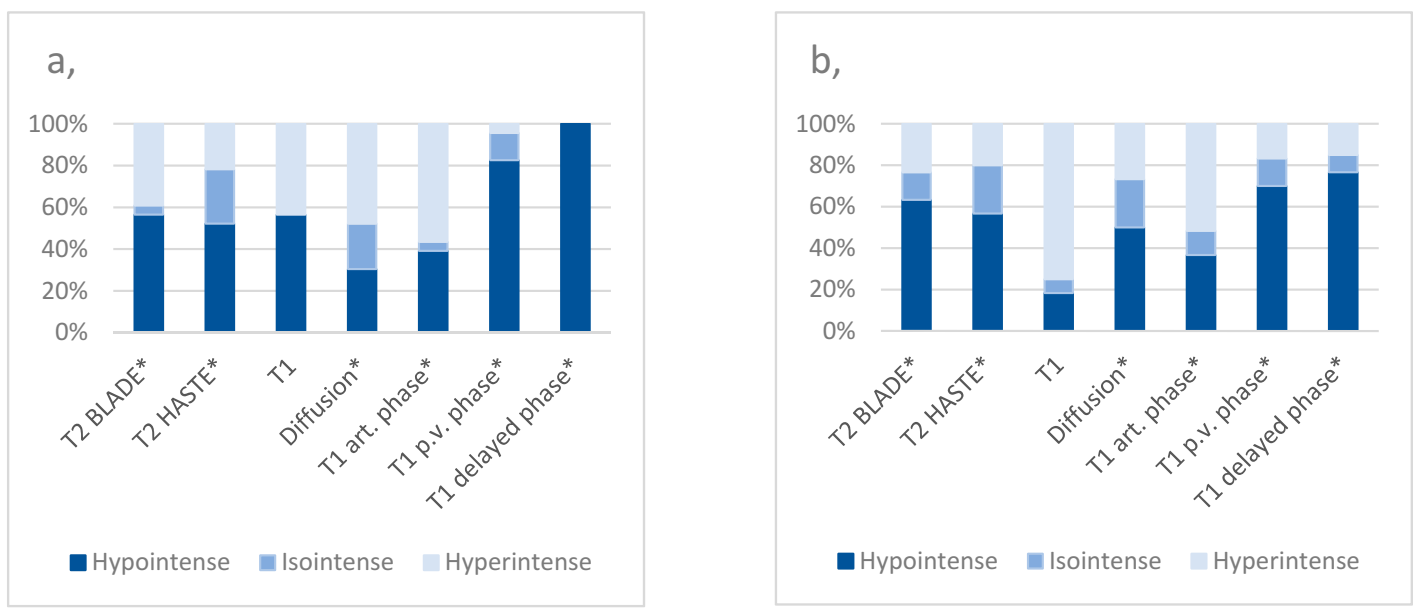
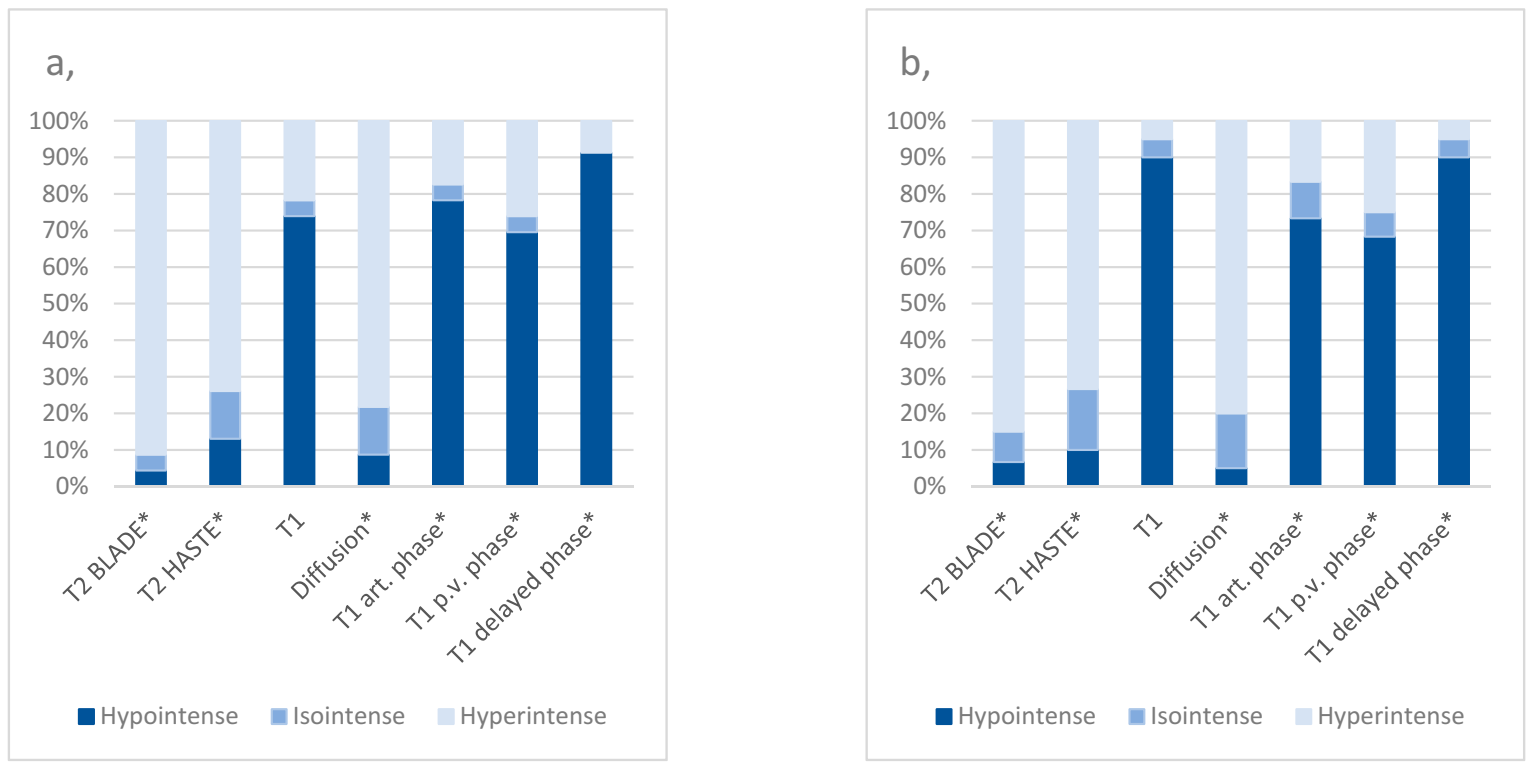
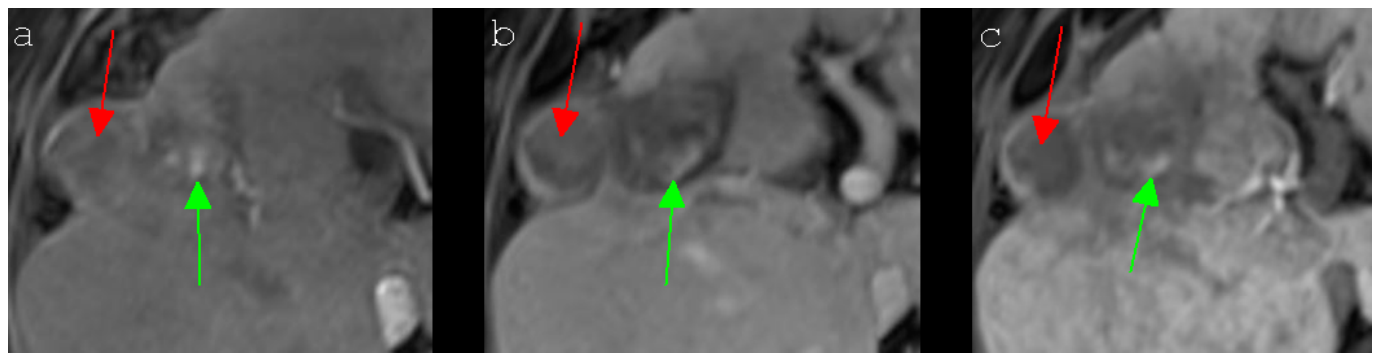
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BLADE | Proprietary name for periodically overlapping parallel lines with enhanced reconstruction (PROPELLER) from Siemens Healthcare |
| CI | Confidence interval |
| CIRSE | Cardiovascular and Interventional Radiological Society of Europe |
| DOR DWI | Diagnostic odds ratio Diffusion weighted imaging |
| FN | False negative |
| FNR | False negative rate |
| FP | False positive |
| FPR | False positive rate |
| Gd-EOB-DTPA | Gadoxetate-Disodium-Ethoxybenzyl-Diethylenetriamine-pentaacetic-acid (C23H28GdN3Na2O11; Eovist®/Primovist®) |
| HASTE | Half-Fourier acquisition single-shot turbo-spin echo |
| HCC | Hepatocellular carcinoma |
| IRE | Irreversible electroporation |
| LR– | Negative likelihood ratio |
| LR+ | Positive likelihood ratio |
| LTP | Local tumor progression |
| MRI | Magnetic resonance imaging |
| MWA | Microwave ablation |
| N | Negative |
| NPV | Negative prediction value |
| P | Positive |
| PPV | Positive prediction value |
| RF | Relapse-free/control |
| SD | Standard deviation |
| SIR | Society of Interventional Radiology |
| TN | True negative |
| TNR | True negative rate |
| TP | True positive |
| TPR | True positive rate |
| T1 d.p. | T1 delayed phase |
| T1 p.v. | T1 portal venous |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MRI Sequence | Signal Intensity | ||
|---|---|---|---|
| Hypointense | Isointense | Hyperintense | |
| T2 BLADE * | 0 | 2 | 4 |
| T2 HASTE * | 0 | 1 | 5 |
| T1 | 1 | 3 | 2 |
| Diffusion | 0 | 3 | 3 |
| T1 arterial phase * | 0 | 1 | 5 |
| T1 portal venous phase * | 2 | 4 | 0 |
| T1 delayed phase * | 5 | 1 | 0 |
References
- Sasson, A.R.; Sigurdson, E.R. Surgical treatment of liver metastases. Semin Oncol. 2002, 29, 107–118. [Google Scholar] [CrossRef]
- Ahmed, M. Technology Assessment Committee of the Society of Interventional Radiology. Image-guided tumor ablation: Standardization of terminology and reporting criteria-a 10-year update: Supplement to the consensus document. J. Vasc. Interv. Radiol. 2014, 25, 1706–1708. [Google Scholar] [CrossRef]
- Meloni, M.F.; Andreano, A.; Bovo, G.; Chiarpotto, B.; Amabile, C.; Gelsomino, S.; Lazzaroni, S.; Sironi, S. Acute portal venous injury after microwave ablation in an in vivo porcine model: A rare possible complication. J. Vasc. Interv. Radiol. 2011, 22, 947–951. [Google Scholar] [CrossRef]
- Crocetti, L.; de Baere, T.; Lencioni, R. Quality improvement guidelines for radiofrequency ablation of liver tumours. Cardiovasc. Interv. Radiol. 2010, 33, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dollinger, M.; Müller-Wille, R.; Zeman, F.; Haimerl, M.; Niessen, C.; Beyer, L.P.; Lang, S.A.; Teufel, A.; Stroszczynski, C.; Wiggermann, P. Irreversible electroporation of malignant hepatic tumors-Alterations in venous structures at subacute follow-up and evolution at mid-term follow-up. PLoS ONE 2015, 10, e0135773. [Google Scholar] [CrossRef]
- Rubinsky, B.; Onik, G.; Mikus, P. Irreversible electroporation: A new ablation modality-clinical implications. Technol. Cancer Res. Treat. 2007, 6, 37–48. [Google Scholar] [CrossRef]
- Lee, E.W.; Chen, C.; Prieto, V.E.; Dry, S.M.; Loh, C.T.; Kee, S.T. Advanced hepatic ablation technique for creating complete cell death: Irreversible electroporation. Radiology 2010, 255, 426–433. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lu, D.S.; Osuagwu, F.; Lassman, C. Irreversible electroporation in porcine liver: Short- and long-term effect on the hepatic veins and adjacent tissue by CT with pathological correlation. Investig. Radiol. 2012, 47, 671–675. [Google Scholar] [CrossRef]
- Tameez Ud Din, A.; Tameez-Ud-Din, A.; Chaudhary, F.M.D.; Chaudhary, N.A.; Siddiqui, K.H. Irreversible Electroporation for liver tumors: A review of literature. Cureus 2019, 11, e4994. [Google Scholar] [CrossRef] [Green Version]
- Saini, A.; Breen, I.; Alzubaidi, S.; Pershad, Y.; Sheth, R.; Naidu, S.; Knuttinen, M.G.; Albadawi, H.; Oklu, R. Irreversible Electroporation in liver lancers and whole organ engineering. J. Clin. Med. 2018, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Mathy, R.M.; Tinoush, P.; da Florencia, R.D.; Braun, A.; Ghamarnejad, O.; Radeleff, B.; Kauczor, H.U.; Chang, D.H. Impact of needle positioning on ablation success of irreversible electroporation: A unicentric retrospective analysis. Sci. Rep. 2020, 10, 21902. [Google Scholar] [CrossRef]
- Gazelle, G.S.; Goldberg, S.N.; Solbiati, L.; Livraghi, T. Tumor ablation with radio-frequency energy. Radiology 2000, 217, 633–646. [Google Scholar] [CrossRef]
- Lewin, J.S.; Connell, C.F.; Duerk, J.L.; Chung, Y.C.; Clampitt, M.E.; Spisak, J.; Gazelle, G.S.; Haaga, J.R. Interactive MRI-guided radiofrequency interstitial thermal ablation of abdominal tumors: Clinical trial for evaluation of safety and feasibility. J. Magn. Reson. Imaging 1998, 8, 40–47. [Google Scholar] [CrossRef]
- Roberts, L.R.; Sirlin, C.B.; Zaiem, F.; Almasri, J.; Prokop, L.J.; Heimbach, J.K.; Murad, M.H.; Mohammed, K. Imaging for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. Hepatology 2018, 67, 401–421. [Google Scholar] [CrossRef] [Green Version]
- Haimerl, M.; Wächtler, M.; Zeman, F.; Verloh, N.; Platzek, I.; Schreyer, A.G.; Stroszczynski, C.; Wiggermann, P. Quantitative evaluation of enhancement patterns in focal solid liver lesions with Gd-EOB-DTPA-enhanced MRI. PLoS ONE 2014, 9, e100315. [Google Scholar] [CrossRef]
- Balogh, J.; Victor, D., III; Asham., E.H.; Burroughs, S.G.; Boktour, M.; Saharia, A.; Li, X.; Ghobrial, R.M.; Monsour, H.P., Jr. Hepatocellular carcinoma: A review. J. Hepatocell. Carcinoma 2016, 3, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Ozer Etik, D.; Suna, N.; Boyacioglu, A.S. Management of Hepatocellular Carcinoma: Prevention, Surveillance, Diagnosis, and Staging. Exp. Clin. Transplant. 2017, 15, 31–35. [Google Scholar]
- Niessen, C.; Igl, J.; Pregler, B.; Beyer, L.; Noeva, E.; Dollinger, M.; Schreyer, A.G.; Jung, E.M.; Stroszczynski, C.; Wiggermann, P. Factors associated with short-term local recurrence of liver cancer after percutaneous ablation using irreversible electroporation: A prospective single-center study. J. Vasc. Interv. Radiol. 2015, 26, 694–702. [Google Scholar] [CrossRef]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; Chen, M.H.; Choi, B.I.; de Baère, T.; Dodd, G.D., 3rd; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria-a 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef]
- Choi, J.Y.; Lee, J.M.; Sirlin, C.B. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 2014, 272, 635–654. [Google Scholar] [CrossRef] [Green Version]
- “N-1” Chi-squared Test as Recommended by Campbell (2007) and Richardson (2011). Available online: https://www.medcalc.org/calc/comparison_of_proportions.php (accessed on 15 November 2020).
- IBM SPSS Statistics, Version 25; Software for Technical Computation: Armonk, NY, USA.
- Cannon, R.; Ellis, S.; Hayes, D.; Narayanan, G.; Martin, R.C. 2nd. Safety and early efficacy of irreversible electroporation for hepatic tumors in proximity to vital structures. J. Surg. Oncol. 2013, 107, 544–549. [Google Scholar] [CrossRef]
- Philips, P.; Hays, D.; Martin, R.C.G. Irreversible electroporation ablation (IRE) of unresectable soft tissue tumors: Learning curve evaluation in the first 150 patients treated. PLoS ONE 2013, 8, e76260. [Google Scholar]
- Thomson, K.R.; Cheung, W.; Ellis, S.J.; Federman, D.; Kavnoudias, H.; Loader-Oliver, D.; Roberts, S.; Evans, P.; Ball, C.; Haydon, A. Investigation of the safety of irreversible electroporation in humans. J. Vasc. Interv. Radiol. 2011, 22, 611–621. [Google Scholar] [CrossRef]
- Kingham, T.P.; Karkar, A.M.; D’Angelica, M.I.; Allen, P.J.; Dematteo, R.P.; Getrajdman, G.I.; Sofocleous, C.T.; Solomon, S.B.; Jarnagin, W.R.; Fong, Y. Ablation of perivascular hepatic malignant tumors with irreversible electroporation. J. Am. Coll. Surg. 2012, 215, 379–387. [Google Scholar] [CrossRef]
- Rimola, J.; Forner, A.; Sapena, V.; Llarch, N.; Darnell, A.; Díaz, A.; García-Criado, A.; Bianchi, L.; Vilana, R.; Díaz-González, Á.; et al. Performance of gadoxetic acid MRI and diffusion-weighted imaging for the diagnosis of early recurrence of hepatocellular carcinoma. Eur. Radiol. 2020, 30, 186–194. [Google Scholar] [CrossRef]
- Padia, S.A.; Johnson, G.E.; Yeung, R.S.; Park, J.O.; Hippe, D.S.; Kogut, M.J. Irreversible electroporation in patients with hepatocellular carcinoma: Immediate versus delayed findings at MR imaging. Radiology 2016, 278, 285–294. [Google Scholar] [CrossRef] [Green Version]
- Kalra, N.; Gupta, P.; Gorsi, U.; Bhujade, H.; Chaluvashetty, S.B.; Duseja, A.; Singh, V.; Dhiman, R.K.; Chawla, Y.K.; Khandelwal, N. Irreversible Electroporation for unresectable hepatocellular carcinoma: Initial experience. Cardiovasc. Interv. Radiol. 2019, 42, 584–590. [Google Scholar] [CrossRef]
- Sutter, O.; Calvo, J.; N’Kontchou, G.; Nault, J.C.; Ourabia, R.; Nahon, P.; Ganne-Carrié, N.; Bourcier, V.; Zentar, N.; Bouhafs, F.; et al. Safety and efficacy of irreversible electroporation for the treatment of hepatocellular carcinoma not amenable to thermal ablation techniques: A retrospective single-center case series. Radiology 2017, 284, 877–886. [Google Scholar] [CrossRef]
- Langan, R.C.; Goldman, D.A.; D’Angelica, M.I.; DeMatteo, R.P.; Allen, P.J.; Balachandran, V.P.; Jarnagin, W.R.; Kingham, T.P. Recurrence patterns following irreversible electroporation for hepatic malignancies. J. Surg. Oncol. 2017, 115, 704–710. [Google Scholar] [CrossRef] [Green Version]
- Cheung, W.; Kavnoudias, H.; Roberts, S.; Szkandera, B.; Kemp, W.; Thomson, K.R. Irreversible electroporation for unresectable hepatocellular carcinoma: Initial experience and review of safety and outcomes. Technol. Cancer Res. Treat. 2013, 12, 233–241. [Google Scholar] [CrossRef]
- Eisele, R.M.; Chopra, S.S.; Glanemann, M.; Gebauer, B. Risk of local failure after ultrasound guided irreversible electroporation of malignant liver tumors. Interv. Med. Appl. Sci. 2014, 6, 147–153. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Choi, D.; Mitchell, D.G.; Verma, S.K.; Bergin, D.; Navarro, V.J.; Malliah, A.B.; McGowan, C.; Hann, H.W.; Herrine, S.K. Hepatocellular carcinoma with indeterminate or false-negative findings at initial MR imaging: Effect on eligibility for curative treatment initial observations. Radiology 2007, 244, 776–783. [Google Scholar] [CrossRef]
- Takada, Y.; Otsuka, M.; Todoroki, T.; Fukao, K. Accompanying liver cirrhosis as a risk factor for recurrence after resection of solitary hepatocellular carcinoma. Hepatogastroenterology 2003, 50, 1991–1995. [Google Scholar]
- Bruix, J.; Sherman, M. American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]





| Characteristics | Patients with a Local Tumor Progression | Reference Group | p-Value |
|---|---|---|---|
| Number of patients | 23 | 60 | |
| Age (y) | |||
| Mean ± SD | 67.8 ± 11.3 | 67.6 ± 11.2 | 0.460 2 |
| Median (IQR) | 68.0 (16.0) | 68.0 (17.0) | |
| Range | 48–85 | 36–84 | |
| Sex, n (%) | |||
| Male | 17 (73.9) | 47 (78.3) | 0.671 1 |
| Female | 6 (26.1) | 13 (21.7) | |
| Patients with liver cirrhosis, n (%) | 9 (39.1) | 40 (66.7) | 0.023 *1 |
| Tumor localization, n (%) | |||
| Segment I | 0 (0.0) | 3 (5.0) | 0.278 1 |
| Segment II | 3 (13.0) | 6 (10.0) | 0.696 1 |
| Segment III | 4 (17.4) | 5 (8.4) | 0.242 1 |
| Segment IVa | 2 (8.7) | 5 (8.4) | 0.965 1 |
| Segment IVb | 3 (13.0) | 7 (11.6) | 0.861 1 |
| Segment V | 4 (17.4) | 8 (13.3) | 0.636 1 |
| Segment VI | 2 (8.7) | 7 (11.6) | 0.705 1 |
| Segment VII | 0 (0.0) | 5 (8.4) | 0.154 1 |
| Segment VIII | 5 (21.8) | 14 (23.3) | 0.885 1 |
| Tumor diameter (cm), mean ± SD | 2.1 ± 1.1 | 2.3 ± 1.1 | 0.263 2 |
| Tumor diameter (cm), median (IQR) | 19.0 (10.0) | 20.0 (9.0) | |
| Subcapsular localization of the tumor, n (%) | 14 (60.9) | 32 (53.3) | 0.535 1 |
| Distance between tumor and skin (cm), mean ± SD | 66.4 ± 23.1 | 73.1 ± 23.8 | 0.228 2 |
| Distance between tumor and skin (cm), median (IQR) | 65.0 (39.0) | 70.0 (31.0) | |
| Tumors associated with vascular structures, n (%) | 13 (56.5) | 43 (71.7) | 0.189 1 |
| Number of IRE electrodes, mean ± SD | 4.7 ± 1.2 | 4.7 ± 1.0 | 0.94 2 |
| Number of IRE electrodes, median (IQR) | 5.0 (2.0) | 5.0 (2.0) |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Liver cirrhosis: no vs. yes | 0.34 (0.12–0.94) | 0.039 * |
| Localization of the HCC: Segment I–IV vs. V–VIII | 0.77 (0.26–2.28) | 0.641 |
| Distance between tumor and skin: ≤60 cm vs. >60 cm | 0.70 (0.24–2.01) | 0.503 |
| Number of IRE electrodes: ≤3 vs. >3 | 0.99 (0.25–3.90) | 0.991 |
| Localization of the HCC: subcapsular vs. not subcapsular | 1.45 (0.50–4.21) | 0.496 |
| Localization of Local Tumor Progression | Number of Patients, n (%) |
|---|---|
| Central ablation area | 0 (0.0) |
| Central and peripheral ablation area | 4 (17.4) |
| Peripheral ablation area | 19 (82.6) |
| Time of First Observation of Local Tumor Progression | |
| Six weeks after IRE | 4 (17.4) |
| Three months after IRE | 10 (43.5) |
| Six months after IRE | 6 (26.1) |
| Nine months after IRE | 2 (8.7) |
| One year after IRE | 1 (4.3) |
| MRI Sequence | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | DOR |
|---|---|---|---|---|---|
| T2 BLADE | 40.91 (20.71–63.65) | 73.08 (58.98–84.43) | 39.13 (19.71–61.46) | 74.51 (60.37–85.67) | 1.877 |
| T2 HASTE * | 29.41 (10.31–55.96) | 53.85 (33.37–73.41) | 29.41 (10.31–55.96) | 53.85 (33.37–73.41) | 0.486 |
| T1 | 43.48 (23.19–65.51) | 19.64 (10.23–32.43) | 18.18 (9.08–30.9) | 45.83 (25.55–67.18) | 0.188 |
| Diffusion * | 61.11 (35.75–82.7) | 65.22 (49.75–78.65) | 40.74 (22.39–61.2) | 81.08 (64.84–92.04) | 2.948 |
| T1 art. * | 59.09 (36.35–79.29) | 41.51 (28.14–55.87) | 29.55 (16.76–45.2) | 70.79 (51.96–85.78) | 1.024 |
| T1 p.v. * | 95.00 (75.13–99.87) | 17.65 (8.4–30.87) | 31.15 (19.9–44.29) | 90.00 (55.5–99.75) | 4.078 |
| T1 d.p. * | 100.00 (85.18–100.0) | 16.36 (7.77–28.8) | 33.33 (22.44–45.71) | 100.00 (66.37–100.0) | -/- 1 |
| MRI Sequence | Sensitivity | Specificity | PPV | NPV | DOR |
|---|---|---|---|---|---|
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | ||
| T2 BLADE | 95.45 | 7.27 | 29.17 | 80.00 | 1.646 |
| (77.16–99.88) | (2.02–17.59) | (19.05–41.07) | (28.36–99.49) | ||
| T2 HASTE * | 85.00 | 12.00 | aat27.87 | 66.67 | 0.773 |
| (62.11–96.79) | (4.53–24.31) | (17.15–40.83) | (29.93–92.51) | ||
| T1 | 22.73 | 94.74 | 62.50 | 76.06 | 5.292 |
| (7.82–45.37) | (85.38–98.9) | (24.49–91.48) | (64.46–85.39) | ||
| Diffusion * | 90 | 5.88 | 27.27 | 60 | 0.562 |
| (68.3–98.77) | (1.23–16.24) | (17.03–39.64) | (14.66–94.73) | ||
| T1 art. * | 18.18 | 81.48 | 28.57 | 70.97 | 0.978 |
| (5.19–40.28) | (68.57–90.75) | (8.39–58.1) | (58.05–81.8) | ||
| T1 p.v. * | 72.73 | 26.79 | 28.07 | 71.43 | 0.975 |
| (49.78–89.27) | (15.83–40.3) | (16.97–41.54) | (47.82–88.72) | ||
| T1 d.p. * | 91.3 | 5.26 | 28 | 60 | 0.583 |
| (71.96–98.93) | (1.1–14.62) | (18.24–39.56) | (14.66–94.73) |
| Point of Time | Patients with a Local Tumor Progression | Reference Group | ||
|---|---|---|---|---|
| Diameter of the Ablation Area (cm) | Diameter of the Ablation Area (cm) | |||
| Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | |
| Six weeks after IRE | 5.6 ± 1.3 | 5.6 (1.2) | 5.5 ± 1.5 | 5.3 (1.1) |
| Three months after IRE | 4.5 ± 1.3 | 4.2 (1.1) | 4.3 ± 1.5 | 4.1 (1.2) |
| Six months after IRE | 4.3 ± 1.1 | 4.2 (1.1) | 3.6 ± 1.6 | 3.6 (1.0) |
| Nine months after IRE | 3.8 ± 1.2 | 3.9 (1.0) | 3.5 ± 1.7 | 3.4 (1.0) |
| One year after IRE | 3.5 ± 1.1 | 3.5 (1.0) | 3.4 ± 1.8 | 3.2 (1.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bäumler, W.; Wiggermann, P.; Lürken, L.; Dollinger, M.; Stroszczynski, C.; Beyer, L.P.; Schicho, A. Early Detection of Local Tumor Progression after Irreversible Electroporation (IRE) of Hepatocellular Carcinoma Using Gd-EOB-DTPA-Based MR Imaging at 3T. Cancers 2021, 13, 1595. https://doi.org/10.3390/cancers13071595
Bäumler W, Wiggermann P, Lürken L, Dollinger M, Stroszczynski C, Beyer LP, Schicho A. Early Detection of Local Tumor Progression after Irreversible Electroporation (IRE) of Hepatocellular Carcinoma Using Gd-EOB-DTPA-Based MR Imaging at 3T. Cancers. 2021; 13(7):1595. https://doi.org/10.3390/cancers13071595
Chicago/Turabian StyleBäumler, Wolf, Philipp Wiggermann, Lukas Lürken, Marco Dollinger, Christian Stroszczynski, Lukas P. Beyer, and Andreas Schicho. 2021. "Early Detection of Local Tumor Progression after Irreversible Electroporation (IRE) of Hepatocellular Carcinoma Using Gd-EOB-DTPA-Based MR Imaging at 3T" Cancers 13, no. 7: 1595. https://doi.org/10.3390/cancers13071595