
Neo-Fs Index: A Novel Immunohistochemical Biomarker Panel Predicts Survival and Response to Anti-Angiogenetic Agents in Clear Cell Renal Cell Carcinoma


Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics of the Study Population
2.2. Immunohistochemical Marker Expression
2.3. Prognostic Impact of Immunohistochemical Markers
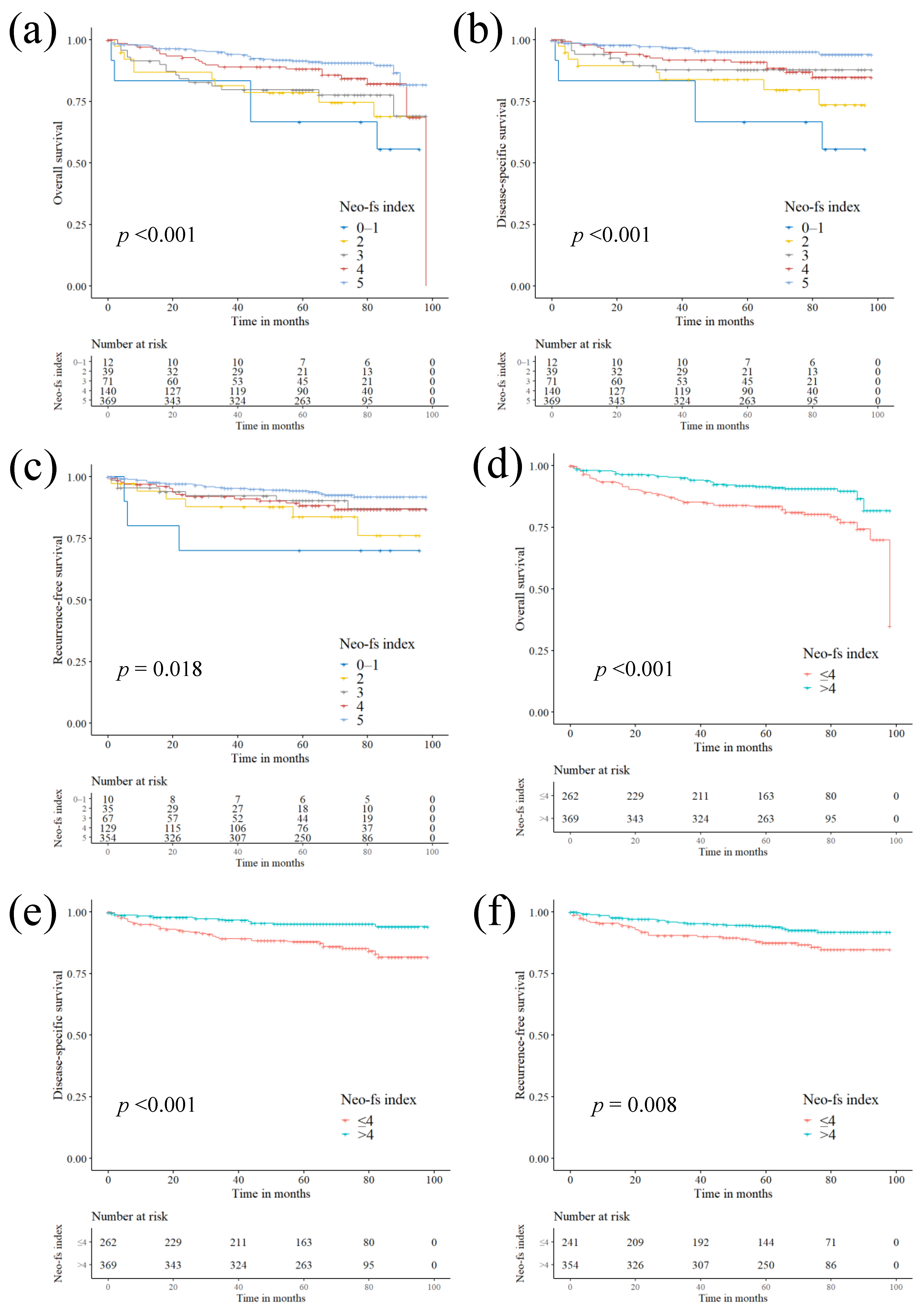
2.4. Prognostic Impact of Neo-Fs Index and its Association with Clinicopathological Characteristics
2.5. Impact of Immunohistochemical Markers and Neo-fs Index on the Treatment Response
2.6. The Cancer Genome Atlas (TCGA) Gene Expression
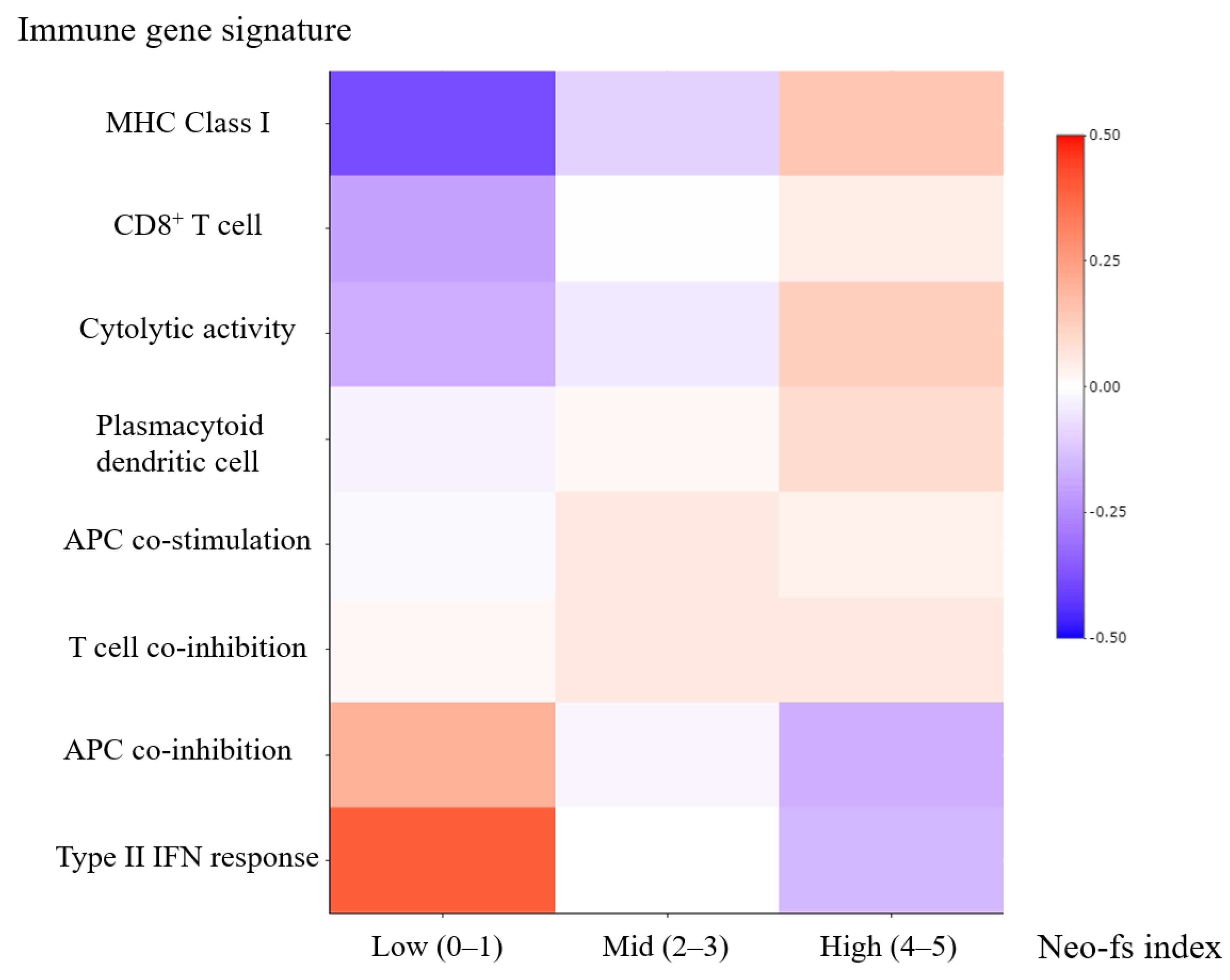
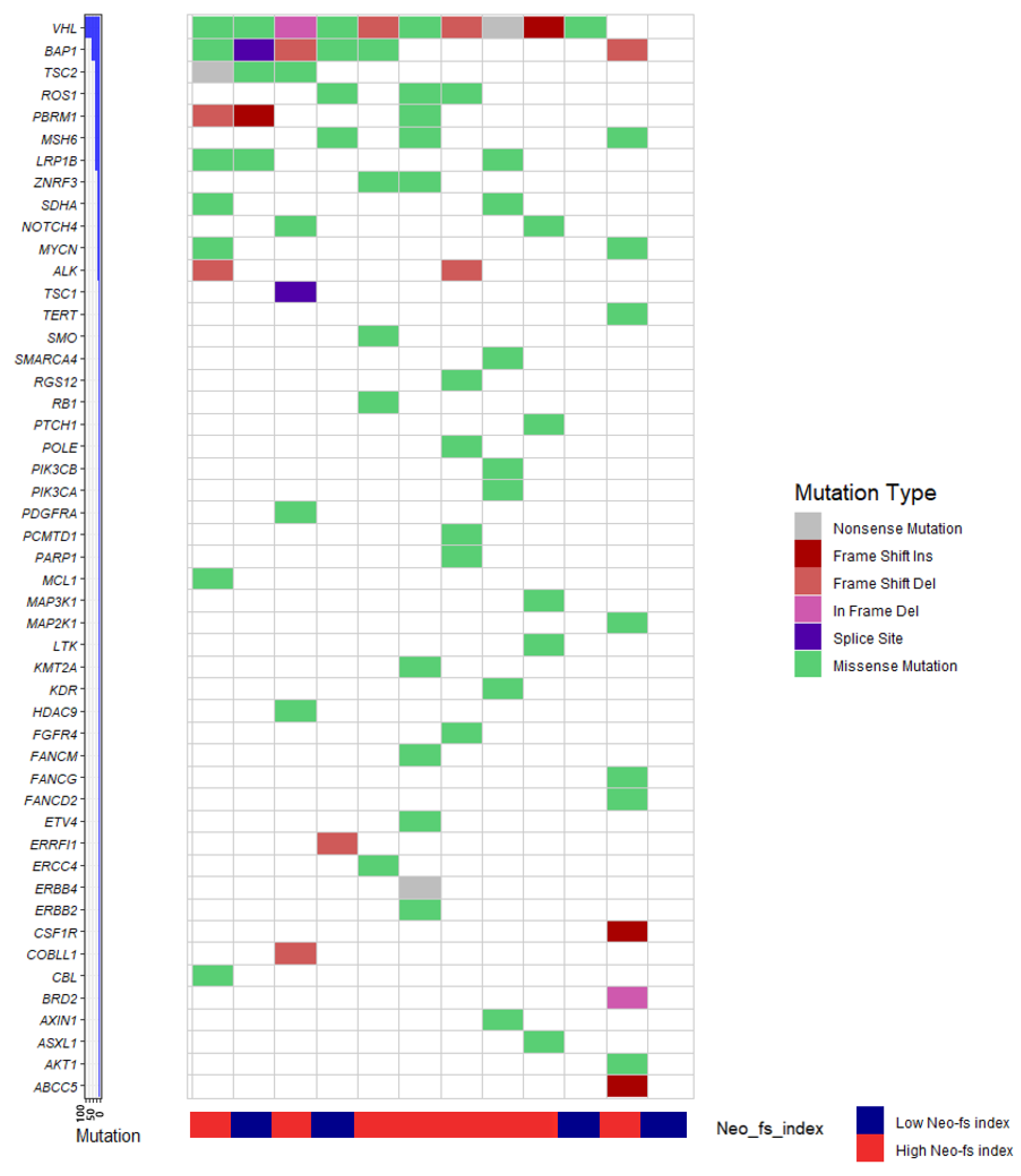
2.7. Molecular Phenotype of Clear Cell Renal Cell Carcinoma and Neo-fs Index
3. Discussion
4. Materials and Methods
4.1. Case Selection
4.2. Pathological Evaluation
4.3. Immunohistochemistry
4.4. Outcome Measures
4.5. TCGA Gene Expression Data
4.6. Targeted Next-Generation Sequencing
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turajlic, S.; Litchfield, K.; Xu, H.; Rosenthal, R.; McGranahan, N.; Reading, J.L.; Wong, Y.N.S.; Rowan, A.; Kanu, N.; Al Bakir, M.; et al. Insertion-and-deletion-derived tumour-specific neoantigens and the immunogenic phenotype: A pan-cancer analysis. Lancet Oncol. 2017, 18, 1009–1021. [Google Scholar] [CrossRef] [Green Version]
- Moch, H.; Humphrey, P.A.; Ulbright, T.M. WHO Classification of Tumours of the Urinary System and Male Genital Organs; International Agency for Research on Cancer: Lyon, France, 2016. [Google Scholar]
- Bedke, J.; Gauler, T.; Grünwald, V.; Hegele, A.; Herrmann, E.; Hinz, S.; Janssen, J.; Schmitz, S.; Schostak, M.; Tesch, H.; et al. Systemic therapy in metastatic renal cell carcinoma. World J. Urol. 2017, 35, 179–188. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Motzer, R.J. Systemic Therapy for Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2017, 376, 354–366. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Kidney Cancer (Version 2.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf (accessed on 22 June 2020).
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; Grünwald, V.; Gillessen, S.; Horwich, A. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooney, M.S.; Shukla, S.A.; Wu, C.J.; Getz, G.; Hacohen, N. Molecular and genetic properties of tumors associated with local immune cytolytic activity. Cell 2015, 160, 48–61. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Man, X.; Zhan, X.; Gao, J.; Gong, Y.; Li, Z. Differential expressions of APC protein in pancreatic cancer and its precursor lesions. Chin. J. Gastroenterol. 2012, 17, 266–270. [Google Scholar] [CrossRef]
- Chu, D.; Zhang, Z.; Zhou, Y.; Wang, W.; Li, Y.; Zhang, H.; Dong, G.; Zhao, Q.; Ji, G. Notch1 and Notch2 have opposite prognostic effects on patients with colorectal cancer. Ann. Oncol. 2011, 22, 2440–2447. [Google Scholar] [CrossRef]
- Zhuang, Z.; Lin, J.; Huang, Y.; Lin, T.; Zheng, Z.; Ma, X. Notch 1 is a valuable therapeutic target against cell survival and proliferation in clear cell renal cell carcinoma. Oncol. Lett. 2017, 14, 3437–3444. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Ju, Z.; Zhao, W.; Wang, L.; Peng, Y.; Ge, Z.; Nagel, Z.D.; Zou, J.; Wang, C.; Kapoor, P.; et al. ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade. Nat. Med. 2018, 24, 556–562. [Google Scholar] [CrossRef]
- Lowenthal, B.M.; Nason, K.S.; Pennathur, A.; Luketich, J.D.; Pai, R.K.; Davison, J.M.; Ma, C. Loss of ARID1A expression is associated with DNA mismatch repair protein deficiency and favorable prognosis in advanced stage surgically resected esophageal adenocarcinoma. Hum. Pathol. 2019, 94, 1–10. [Google Scholar] [CrossRef]
- Donadon, M.; Di Tommaso, L.; Soldani, C.; Franceschini, B.; Terrone, A.; Mimmo, A.; Vitali, E.; Roncalli, M.; Lania, A.; Torzilli, G. Filamin A expression predicts early recurrence of hepatocellular carcinoma after hepatectomy. Liver Int. 2018, 38, 303–311. [Google Scholar] [CrossRef]
- Gachechiladze, M.; Skarda, J.; Janikova, M.; Mgebrishvili, G.; Kharaishvili, G.; Kolek, V.; Grygarkova, I.; Klein, J.; Poprachova, A.; Arabuli, M.; et al. Overexpression of filamin-A protein is associated with aggressive phenotype and poor survival outcomes in NSCLC patients treated with platinum-based combination chemotherapy. Neoplasma 2016, 63, 274–281. [Google Scholar] [CrossRef] [Green Version]
- McGranahan, N.; Furness, A.J.; Rosenthal, R.; Ramskov, S.; Lyngaa, R.; Saini, S.K.; Jamal-Hanjani, M.; Wilson, G.A.; Birkbak, N.J.; Hiley, C.T.; et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 2016, 351, 1463–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miao, D.; Margolis, C.A.; Gao, W.; Voss, M.H.; Li, W.; Martini, D.J.; Norton, C.; Bossé, D.; Wankowicz, S.M.; Cullen, D.; et al. Genomic correlates of response to immune checkpoint therapies in clear cell renal cell carcinoma. Science 2018, 359, 801–806. [Google Scholar] [CrossRef] [Green Version]
- Voss, M.H.; Buros Novik, J.; Hellmann, M.D.; Ball, M.; Hakimi, A.A.; Miao, D.; Margolis, C.; Horak, C.; Wind-Rotolo, M.; De Velasco, G.; et al. Correlation of degree of tumor immune infiltration and insertion-and-deletion (indel) burden with outcome on programmed death 1 (PD1) therapy in advanced renal cell cancer (RCC). J. Clin. Oncol. 2018, 36 (Suppl. 15), 4518. [Google Scholar] [CrossRef]
- Yang, J.; Yan, J.; Liu, B. Targeting VEGF/VEGFR to Modulate Antitumor Immunity. Front. Immunol. 2018, 9, 978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aparicio, L.M.A.; Fernandez, I.P.; Cassinello, J. Tyrosine kinase inhibitors reprogramming immunity in renal cell carcinoma: Rethinking cancer immunotherapy. Clin. Transl. Oncol. 2017, 19, 1175–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greifenberg, V.; Ribechini, E.; Rössner, S.; Lutz, M.B. Myeloid-derived suppressor cell activation by combined LPS and IFN-gamma treatment impairs DC development. Eur. J. Immunol. 2009, 39, 2865–2876. [Google Scholar] [CrossRef] [PubMed]
- Tartour, E.; Pere, H.; Maillere, B.; Terme, M.; Merillon, N.; Taieb, J.; Sandoval, F.; Quintin-Colonna, F.; Lacerda, K.; Karadimou, A.; et al. Angiogenesis and immunity: A bidirectional link potentially relevant for the monitoring of antiangiogenic therapy and the development of novel therapeutic combination with immunotherapy. Cancer Metastasis Rev. 2011, 30, 83–95. [Google Scholar] [CrossRef]
- Pal, S.K.; Hossain, D.M.; Zhang, Q.; Frankel, P.H.; Jones, J.O.; Carmichael, C.; Ruel, C.; Lau, C.; Kortylewski, M. Pazopanib as third line therapy for metastatic renal cell carcinoma: Clinical efficacy and temporal analysis of cytokine profile. J. Urol. 2015, 193, 1114–1121. [Google Scholar] [CrossRef]
- Finke, J.; Ko, J.; Rini, B.; Rayman, P.; Ireland, J.; Cohen, P. MDSC as a mechanism of tumor escape from sunitinib mediated anti-angiogenic therapy. Int. Immunopharmacol. 2011, 11, 856–861. [Google Scholar] [CrossRef] [Green Version]
- Snyder, A.; Makarov, V.; Merghoub, T.; Yuan, J.; Zaretsky, J.M.; Desrichard, A.; Walsh, L.A.; Postow, M.A.; Wong, P.; Ho, T.S.; et al. Genetic Basis for Clinical Response to CTLA-4 Blockade in Melanoma. N. Engl. J. Med. 2014, 371, 2189–2199. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Hansen, U.K.; Ramskov, S.; Bjerregaard, A.M.; Borch, A.; Andersen, R.; Draghi, A.; Donia, M.; Bentzen, A.K.; Marquard, A.M.; Szallasi, Z.; et al. Tumor-Infiltrating T Cells From Clear Cell Renal Cell Carcinoma Patients Recognize Neoepitopes Derived From Point and Frameshift Mutations. Front. Immunol. 2020, 11, 373. [Google Scholar] [CrossRef] [PubMed]
- D’Aniello, C.; Berretta, M.; Cavaliere, C.; Rossetti, S.; Facchini, B.A.; Iovane, G.; Mollo, G.; Capasso, M.; Pepa, C.D.; Pesce, L.; et al. Biomarkers of Prognosis and Efficacy of Anti-angiogenic Therapy in Metastatic Clear Cell Renal Cancer. Front. Oncol. 2019, 9, 1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA; American Joint Commission on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Jeon, M.J.; Chun, S.M.; Lee, J.Y.; Choi, K.W.; Kim, D.; Kim, T.Y.; Jang, S.J.; Kim, W.B.; Shong, Y.K.; Song, D.E.; et al. Mutational profile of papillary thyroid microcarcinoma with extensive lymph node metastasis. Endocrine 2019, 64, 130–138. [Google Scholar] [CrossRef]
- Chun, S.M.; Sung, C.O.; Jeon, H.; Kim, T.I.; Lee, J.Y.; Park, H.; Kim, Y.; Kim, D.; Jang, S.J. Next-Generation Sequencing Using S1 Nuclease for Poor-Quality Formalin-Fixed, Paraffin-Embedded Tumor Specimens. J. Mol. Diagn. 2018, 20, 802–811. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M.; et al. The Genome Analysis Toolkit: A MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, Z.; Markovets, A.; Ahdesmaki, M.; Chapman, B.; Hofmann, O.; McEwen, R.; Johnson, J.; Dougherty, B.; Barrett, J.C.; Dry, J.R. VarDict: A novel and versatile variant caller for next-generation sequencing in cancer research. Nucleic Acids Res. 2016, 44, e108. [Google Scholar] [CrossRef]
- Cibulskis, K.; Lawrence, M.S.; Carter, S.L.; Sivachenko, A.; Jaffe, D.; Sougnez, C.; Gabriel, S.; Meyerson, M.; Lander, E.S.; Getz, G. Sensitive detection of somatic point mutations in impure and heterogeneous cancer samples. Nat. Biotechnol. 2013, 31, 213–219. [Google Scholar] [CrossRef]
- Sherry, S.T.; Ward, M.H.; Kholodov, M.; Baker, J.; Phan, L.; Smigielski, E.M.; Sirotkin, K. dbSNP: The NCBI database of genetic variation. Nucleic Acids Res. 2001, 29, 308–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lek, M.; Karczewski, K.J.; Minikel, E.V.; Samocha, K.E.; Banks, E.; Fennell, T.; O’Donnell-Luria, A.H.; Ware, J.S.; Hill, A.J.; Cummings, B.B.; et al. Analysis of protein-coding genetic variation in 60,706 humans. Nature 2016, 536, 285–291. [Google Scholar] [CrossRef] [Green Version]
- McLaren, W.; Pritchard, B.; Rios, D.; Chen, Y.; Flicek, P.; Cunningham, F. Deriving the consequences of genomic variants with the Ensembl API and SNP Effect Predictor. Bioinformatics 2010, 26, 2069–2070. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.T.; Thorvaldsdóttir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative genomics viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | N (%) | Immunohistochemistry | N (%) |
|---|---|---|---|
| Sex | APC (0–1 vs. 2–3) | ||
| Male | 480 (75.2%) | Low expression | 548 (86.7%) |
| Female | 158 (24.8%) | High expression | 84 (13.3%) |
| Age (years) | NOTCH1 (0–1 vs. 2–3) | ||
| <55 years | 316 (49.5%) | Low expression | 436 (69.0%) |
| ≥55 years | 322 (50.5%) | High expression | 196 (31.0%) |
| Procedure | ARID1A (0–2 vs. 3) | ||
| Partial nephrectomy | 340 (53.3%) | Low expression | 627 (99.1%) |
| Radical nephrectomy | 298 (46.7%) | High expression | 6 (0.9%) |
| WHO/ISUP nuclear grade * | FAT1 (0–1 vs. 2–3) | ||
| 1‒2 | 331 (51.9%) | Low expression | 474 (74.9%) |
| 3‒4 | 307 (48.1%) | High expression | 159 (25.1%) |
| Tumor size (cm) | VHL (0 vs. 1–3) | ||
| <4 cm | 388 (60.8%) | Low expression | 177 (28.0%) |
| ≥4 cm | 250 (39.2%) | High expression | 455 (72.0%) |
| pT stage | EYS (0–1 vs. 2–3) | ||
| pT1‒2 | 496 (77.7%) | Low expression | 527 (83.0%) |
| pT3‒4 | 142 (22.3%) | High expression | 108 (17.0%) |
| pN stage | KMT2D (0–1 vs. 2–3) | ||
| pN0/pNx | 623 (97.6%) | Low expression | 296 (46.8%) |
| pN1 | 15 (2.4%) | High expression | 337 (53.2%) |
| Lymphovascular invasion | Filamin A (0–2 vs. 3) | ||
| Absent | 537 (84.2%) | Low expression | 579 (91.5%) |
| Present | 101 (15.8%) | High expression | 54 (8.5%) |
| Resection margin | PTEN (0 vs. 1–3) | ||
| Clear | 624 (97.8%) | Low expression | 112 (17.6%) |
| Involved | 14 (2.2%) | High expression | 526 (82.4%) |
| Necrosis | p53 (0 vs. 1–3) | ||
| Absent | 538 (84.3%) | Low expression | 36 (5.6%) |
| Present | 100 (15.7%) | High expression | 602 (94.4%) |
| Sarcomatoid change | |||
| Absent | 603 (94.5%) | ||
| Present | 35 (5.5%) | ||
| Anti-angiogenetic agent | |||
| Not received | 573 (89.8%) | ||
| Received | 65 (10.2%) | ||
| mTOR inhibitor | |||
| Not received | 600 (94.0%) | ||
| Received | 38 (6.0%) | ||
| Variables | Overall Survival | Disease-Specific Survival | Recurrence-Free Survival | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Clinicopathologic variables | ||||||
| Female (vs. Male) | 0.729 (0.430–1.238) | 0.242 | 0.726 (0.376–1.402) | 0.341 | 0.800 (0.422–1.515) | 0.493 |
| Age ≥ 55 years | 3.328 (2.057–5.387) | <0.001 | 2.702 (1.516–4.817) | 0.001 | 2.316 (1.322–4.059) | 0.003 |
| Radical nephrectomy (vs. partial nephrectomy) | 3.797 (2.345–6.146) | <0.001 | 16.769 (6.069–46.335) | <0.001 | 3.915 (2.167–7.073) | <0.001 |
| ISUP grade 3–4 | 4.052 (2.464–6.663) | <0.001 | 12.064 (4.818–30.210) | <0.001 | 5.385 (2.785–10.414) | <0.001 |
| Tumor size ≥ 4 cm | 5.622 (3.474–9.097) | <0.001 | 19.062 (7.610–47.747) | <0.001 | 4.818 (2.724–8.520) | <0.001 |
| pT3–4 | 6.281 (4.117–9.584) | <0.001 | 16.709 (8.807–31.699) | <0.001 | 8.920 (5.205–15.289) | <0.001 |
| pN1 (vs. pN0/pNx) | 15.837 (8.688–28.868) | <0.001 | 26.214 (13.893–49.463) | <0.001 | 69.925 (25.878–188.944) | <0.001 |
| Lymphovascular invasion | 7.281 (4.777–11.097) | <0.001 | 12.505 (7.250–21.569) | <0.001 | 6.041 (3.522–10.360) | <0.001 |
| Margin involvement | 5.792 (2.793–12.010) | <0.001 | 7.757 (3.511–17.136) | <0.001 | 9.450 (4.038–22.113) | <0.001 |
| Necrosis | 7.462 (4.926–11.304) | <0.001 | 23.111 (12.436–42.951) | <0.001 | 8.777 (5.172–14.893) | <0.001 |
| Sarcomatoid change | 7.289 (4.416–12.031) | <0.001 | 12.974 (7.516–22.396) | <0.001 | 9.280 (4.792–17.970) | <0.001 |
| AAA recipient | 11.146 (7.334–16.938) | <0.001 | 36.948 (20.155–67.735) | <0.001 | 56.860 (32.589–99.207) | <0.001 |
| mTOR inhibitor recipient | 13.798 (8.881–21.438) | <0.001 | 32.525 (19.109–55.362) | <0.001 | 46.282 (24.568–87.191) | <0.001 |
| Immunohistochemistry | ||||||
| High APC expression | 1.663 (0.979–2.827) | 0.060 | 2.129 (1.143–3.966) | 0.017 | 1.537 (0.774–3.049) | 0.219 |
| High NOTCH1 expression | 1.806 (1.182–2.758) | 0.006 | 2.029 (1.195–3.447) | 0.009 | 1.835 (1.077–3.128) | 0.026 |
| High ARID1A expression | 4.634 (1.675–12.820) | 0.003 | 6.290 (1.954–20.251) | 0.002 | 2.307 (0.319–16.687) | 0.408 |
| High FAT1 expression | 0.659 (0.383–1.134) | 0.132 | 0.415 (0.188–0.916) | 0.029 | 0.627 (0.315–1.245) | 0.182 |
| High VHL expression | 0.573 (0.375–0.877) | 0.010 | 0.482 (0.286–0.814) | 0.006 | 0.527 (0.307–0.904) | 0.020 |
| High EYS expression | 2.416 (1.540–3.789) | <0.001 | 3.294 (1.911–5.676) | <0.001 | 1.710 (0.919–3.180) | 0.090 |
| High KMT2D expression | 0.859 (0.562–1.313) | 0.483 | 0.967 (0.566–1.653) | 0.904 | 0.705 (0.413–1.205) | 0.201 |
| High Filamin A expression | 2.439 (1.417–4.198) | 0.001 | 3.826 (2.080–7.040) | <0.001 | 3.217 (1.659–6.236) | 0.001 |
| High PTEN expression | 0.438 (0.280–0.686) | <0.001 | 0.284 (0.167–0.482) | <0.001 | 0.637 (0.337–1.207) | 0.167 |
| High p53 expression | 0.719 (0.329–1.570) | 0.408 | 0.387 (0.176–0.854) | 0.019 | 0.361 (0.164–0.798) | 0.012 |
| Neo-fs index | ||||||
| 0–1 | 4.497 (1.759–11.498) | 0.002 | 8.655 (3.206–23.369) | <0.001 | 4.715 (1.418–15.679) | 0.011 |
| 2 | 2.811 (1.388–5.694) | 0.004 | 4.553 (1.978–10.478) | <0.001 | 2.797 (1.143–6.843) | 0.024 |
| 3 | 2.424 (1.337–4.395) | 0.004 | 2.496 (1.085–5.741) | 0.031 | 1.647 (0.710–3.822) | 0.246 |
| 4 | 1.673 (0.981–2.853) | 0.059 | 2.392 (1.220–4.691) | 0.011 | 1.804 (0.946–3.439) | 0.073 |
| 5 (reference) | 1 | - | 1 | - | 1 | - |
| p-for trend | 0.690 (0.584–0.815) | <0.001 | 0.608 (0.499–0.741) | <0.001 | 0.711 (0.573–0.883) | 0.002 |
| Neo-fs index | ||||||
| Low (≤4) | 1 | - | 1 | - | 1 | - |
| High (>4) | 0.461 (0.301–0.708) | <0.001 | 0.331 (0.188–0.581) | <0.001 | 0.495 (0.291–0.844) | 0.010 |
| Variables | Overall Survival (OS) | Disease-Specific Survival (DSS) | Recurrence-Free Survival (RFS) | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Clinicopathologic variables | ||||||
| Age ≥ 55 years | 3.005 (1.833–4.925) | <0.001 | 2.501 (1.365–4.585) | 0.003 | 1.671 (0.923–3.027) | 0.090 |
| Radical nephrectomy (vs. partial nephrectomy) | 0.915 (0.484–1.729) | 0.784 | 1.919 (0.593–6.207) | 0.276 | 0.811 (0.394–1.671) | 0.571 |
| ISUP grade 3–4 | 1.271 (0.704–2.296) | 0.426 | 1.799 (0.634–5.105) | 0.269 | 2.396 (1.098–5.227) | 0.028 |
| Tumor size ≥ 4 cm | 2.374 (1.220–4.620) | 0.011 | 3.516 (1.160–10.653) | 0.026 | 2.348 (1.056–5.220) | 0.036 |
| pT3–4 | 0.874 (0.442–1.729) | 0.699 | 0.824 (0.321–2.116) | 0.687 | 1.545 (0.707–3.379) | 0.276 |
| pN1 (vs. pN0/pNx) | 1.270 (0.585–2.757) | 0.546 | 1.112 (0.503–2.458) | 0.792 | 3.916 (1.075–14.266) | 0.038 |
| Lymphovascular invasion | 1.537 (0.657–3.593) | 0.322 | 1.409 (0.561–3.537) | 0.465 | 2.162 (1.101–4.245) | 0.025 |
| Margin involvement | 2.552 (1.441–4.519) | 0.001 | 2.527 (1.222–5.225) | 0.012 | 3.193 (1.033–9.870) | 0.044 |
| Necrosis | 1.633 (0.885–3.012) | 0.116 | 2.186 (0.948–5.038) | 0.066 | 1.386 (0.642–2.994) | 0.406 |
| Sarcomatoid change | 1.311 (0.710–2.420) | 0.387 | 1.396 (0.739–2.636) | 0.304 | 0.912 (0.392–2.122) | 0.830 |
| AAA recipient | 2.796 (1.342–5.825) | 0.006 | 6.642 (2.642–16.699) | <0.001 | 29.152 (13.253–64.125) | <0.001 |
| mTOR inhibitor recipient | 1.429 (0.696–2.934) | 0.330 | 1.219 (0.586–2.537) | 0.596 | 1.176 (0.540–2.562) | 0.683 |
| Immunohistochemistry | ||||||
| High APC expression | NA | NA | 2.717 (1.333–5.539) | 0.006 | NA | NA |
| High NOTCH1 expression | 1.694 (1.057–2.714) | 0.028 | 1.782 (0.963–3.298) | 0.066 | 2.021 (1.116–3.659) | 0.020 |
| High ARID1A expression | 4.558 (1.568–13.252) | 0.005 | 6.303 (1.726–23.016) | 0.005 | NA | NA |
| High FAT1 expression | 1.231 (0.690–2.197) | 0.483 | 1.287 (0.542–3.053) | 0.567 | NA | NA |
| High VHL expression | 1.131 (0.712–1.797) | 0.601 | 1.273 (0.712–2.276) | 0.415 | 1.003 (0.558–1.801) | 0.992 |
| High EYS expression | 1.806 (1.108–2.945) | 0.018 | 2.212 (1.188–4.119) | 0.012 | NA | NA |
| High Filamin A expression | 1.524 (0.795–2.920) | 0.204 | 2.108 (1.007–4.415) | 0.048 | 1.243 (0.497–3.112) | 0.642 |
| High PTEN expression | 0.977 (0.602–1.585) | 0.924 | 0.999 (0.562–1.775) | 0.998 | NA | NA |
| High p53 expression | NA | NA | 0.745 (0.325–1.707) | 0.486 | 0.930 (0.364–2.377) | 0.880 |
| Neo-fs index | ||||||
| 0–1 | 2.099 (0.775–5.688) | 0.145 | 3.135 (1.029–9.556) | 0.044 | 1.840 (0.454–7.457) | 0.393 |
| 2 | 2.285 (1.011–5.162) | 0.047 | 4.494 (1.578–12.800) | 0.005 | 2.935 (1.038–8.296) | 0.042 |
| 3 | 2.774 (1.486–5.177) | 0.001 | 3.007 (1.238–7.300) | 0.015 | 1.475 (0.564–3.86) | 0.428 |
| 4 | 1.128 (0.628–2.025) | 0.688 | 1.665 (0.749–3.699) | 0.211 | 2.265 (1.105–4.642) | 0.026 |
| 5 (reference) | 1 | - | 1 | - | 1 | - |
| p-for trend | 0.757 (0.632–0.907) | 0.003 | 0.690 (0.552–0.863) | 0.001 | 0.787 (0.615–1.007) | 0.057 |
| Neo-fs index | ||||||
| Low (≤4) | 1 | - | 1 | - | 1 | - |
| High (>4) | 0.595 (0.372–0.951) | 0.030 | 0.430 (0.225–0.825) | 0.011 | 0.480 (0.259–0.890) | 0.020 |
| Variables | Anti-Angiogenic Agent | mTOR Inhibitor | ||||
|---|---|---|---|---|---|---|
| PR/SD,PD | ORR | p | SD/PD | DCR | p | |
| Low APC | 17/36 | 32.1% | 0.092 | 7/18 | 28.0% | 0.999 |
| High APC | 0/8 | 0% | 1/2 | 33.3% | ||
| Low NOTCH1 | 12/26 | 31.6% | 0.406 | 5/14 | 26.3% | 0.573 |
| High NOTCH1 | 5/18 | 21.7% | 3/6 | 33.3% | ||
| Low ARID1A | 17/44 | 27.9% | 0.999 | 8/19 | 29.6% | 0.999 |
| High ARID1A | 0/1 | 0% | 0/1 | 0.0% | ||
| Low EYS | 15/29 | 34.1% | 0.114 | 8/13 | 38.1% | 0.075 |
| High EYS | 2/15 | 11.8% | 0/7 | 0% | ||
| Low Filamin A | 16/32 | 33.3% | 0.088 | 6/16 | 27.3% | 0.999 |
| High Filamin A | 1/12 | 7.7% | 2/4 | 33.3% | ||
| Indel signatures (positive number) | ||||||
| 0–1 | 0/3 | 0% | 0.027 | 0/2 | 0% | 0.742 |
| 2 | 1/4 | 20.0% | 0/1 | 0% | ||
| 3 | 1/8 | 11.1% | 2/1 | 66.7% | ||
| 4 | 3/14 | 17.6% | 2/6 | 25.0% | ||
| 5 | 12/15 | 44.4% | 4/10 | 28.6% | ||
| Indel signatures (positive number) | ||||||
| Neo-fs index ≤ 4 | 5/29 | 14.7% | 0.010 | 4/10 | 28.6% | 0.999 |
| Neo-fs index > 4 | 12/15 | 44.4% | 4/10 | 28.6% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Park, J.-Y.; Shin, S.-J.; Lim, B.J.; Go, H. Neo-Fs Index: A Novel Immunohistochemical Biomarker Panel Predicts Survival and Response to Anti-Angiogenetic Agents in Clear Cell Renal Cell Carcinoma. Cancers 2021, 13, 1199. https://doi.org/10.3390/cancers13061199
Kim J, Park J-Y, Shin S-J, Lim BJ, Go H. Neo-Fs Index: A Novel Immunohistochemical Biomarker Panel Predicts Survival and Response to Anti-Angiogenetic Agents in Clear Cell Renal Cell Carcinoma. Cancers. 2021; 13(6):1199. https://doi.org/10.3390/cancers13061199
Chicago/Turabian StyleKim, Jisup, Jee-Young Park, Su-Jin Shin, Beom Jin Lim, and Heounjeong Go. 2021. "Neo-Fs Index: A Novel Immunohistochemical Biomarker Panel Predicts Survival and Response to Anti-Angiogenetic Agents in Clear Cell Renal Cell Carcinoma" Cancers 13, no. 6: 1199. https://doi.org/10.3390/cancers13061199