
Genetic Predictors of Chemotherapy-Induced Peripheral Neuropathy from Paclitaxel, Carboplatin and Oxaliplatin: NCCTG/Alliance N08C1, N08CA and N08CB Study

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
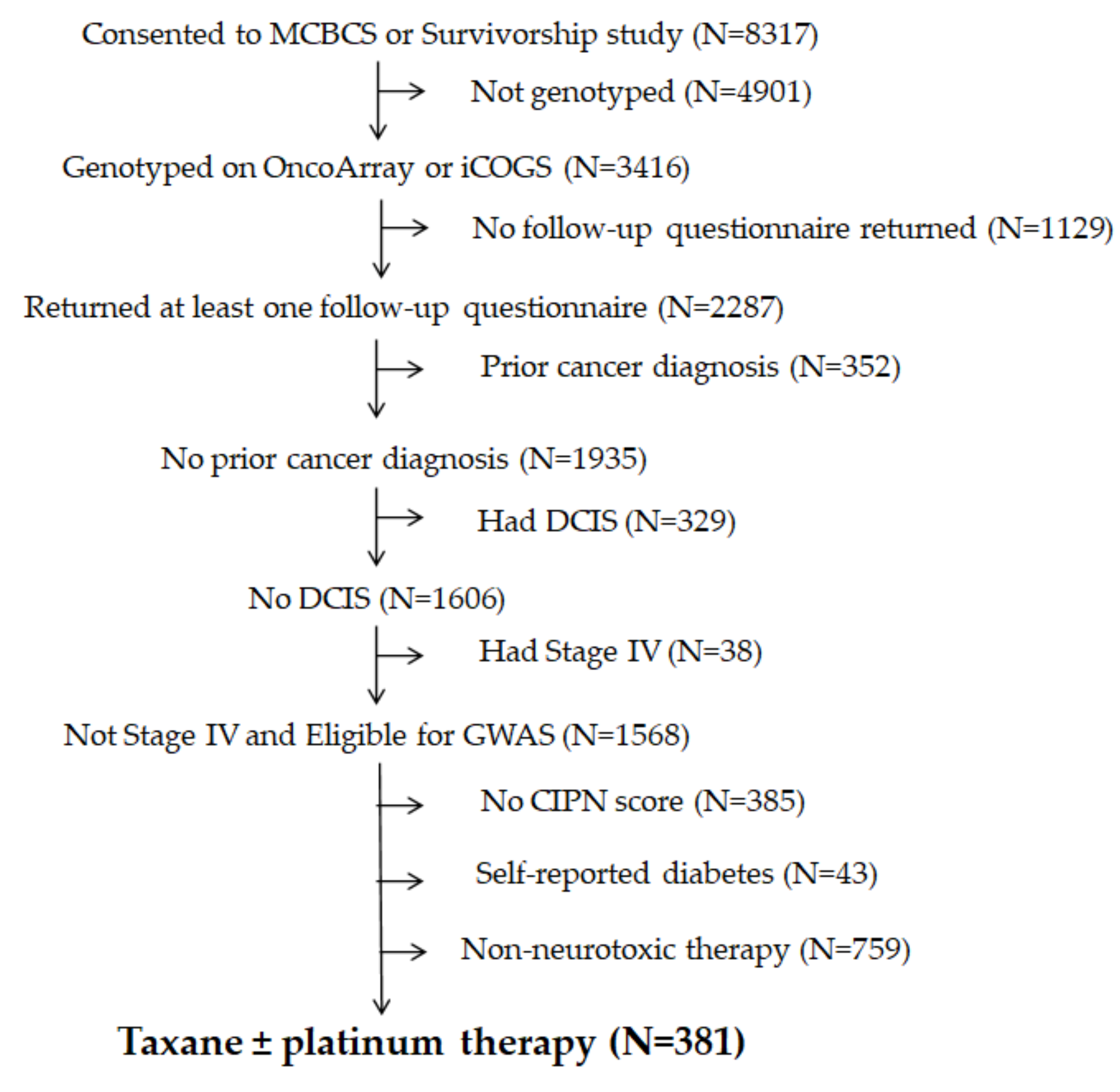
2.1. Patient Population
2.2. Measurement of Chemotherapy-Induced Peripheral Neuropathy (CIPN) Symptoms
2.3. DNA Extraction, Genotyping and Quality Control
2.4. Candidate Gene SNPs
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
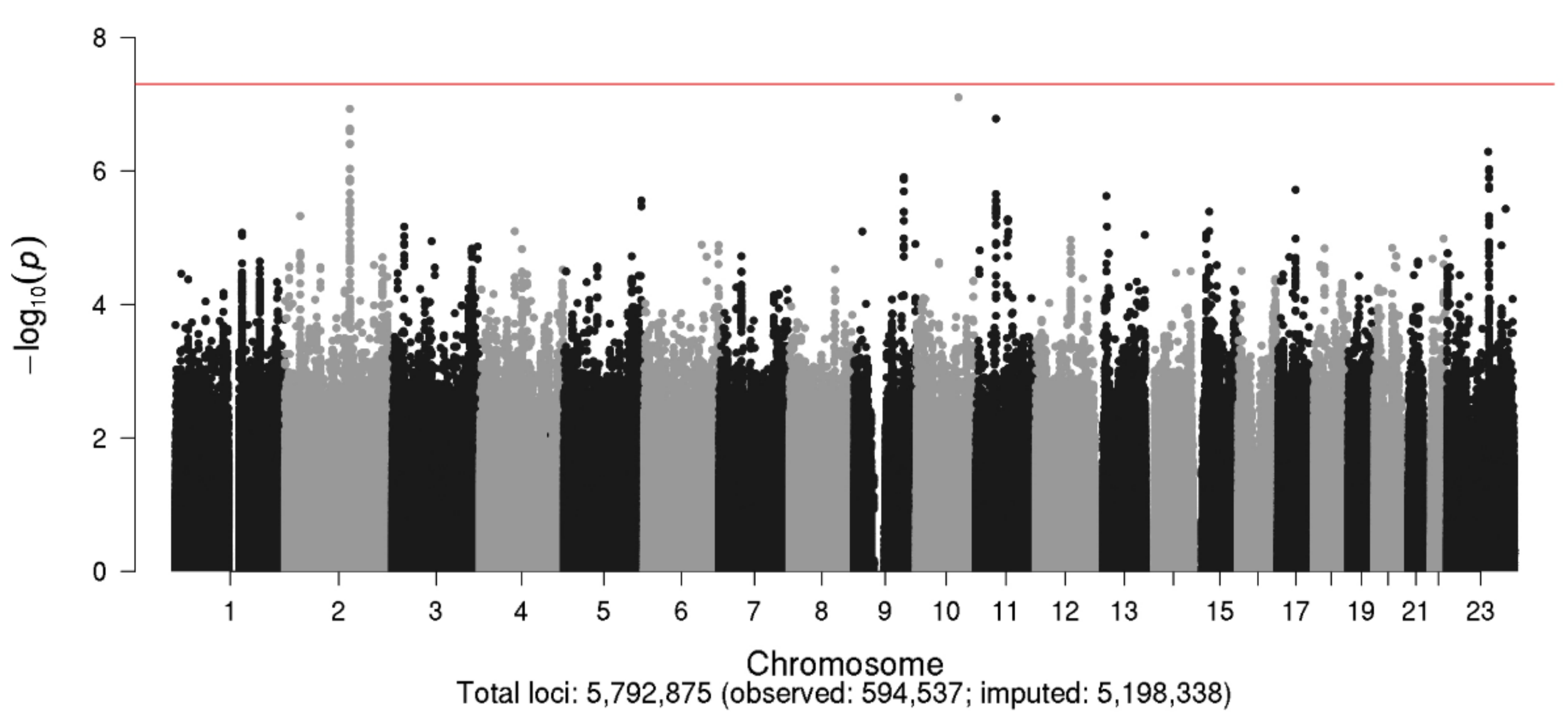
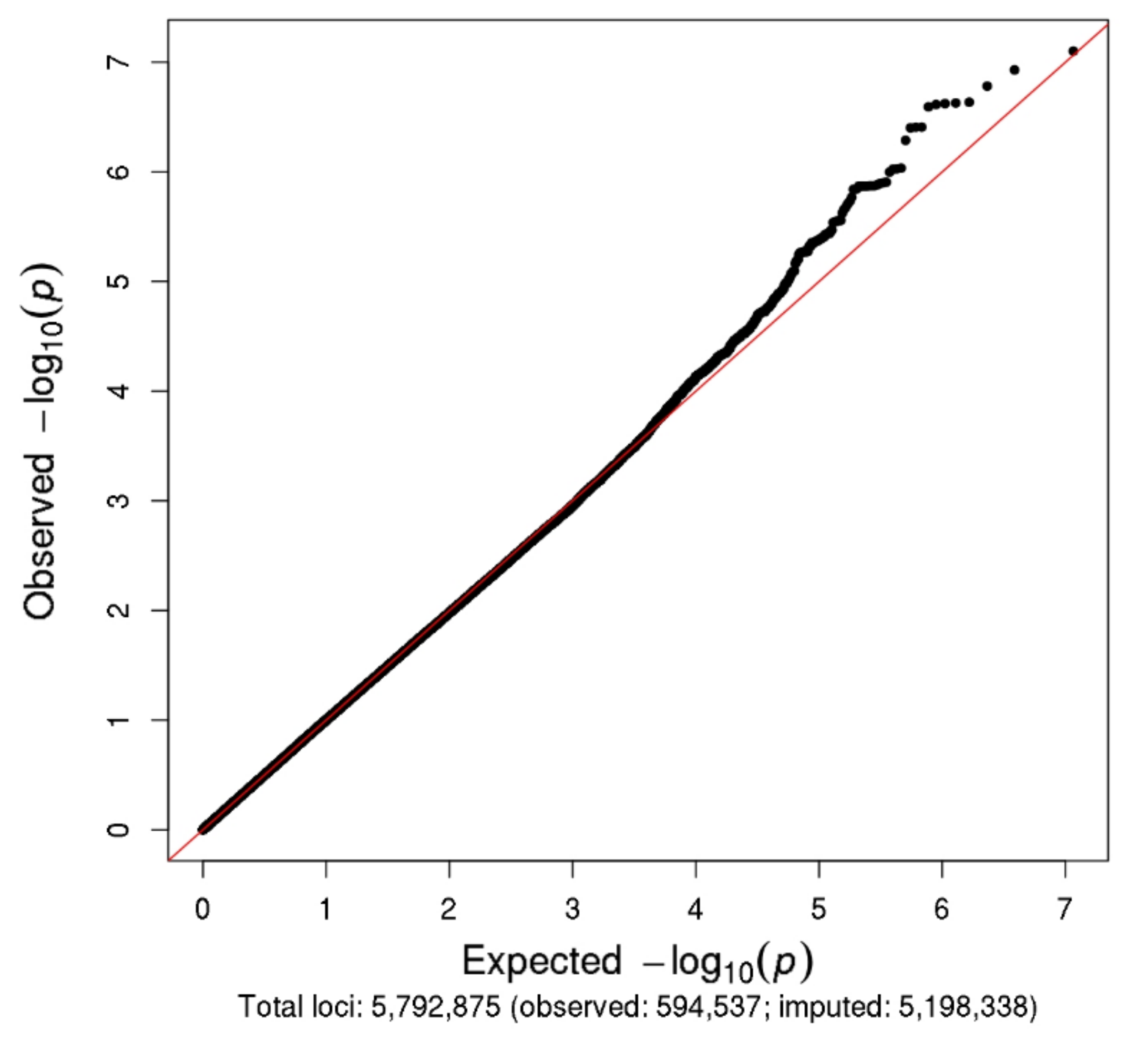
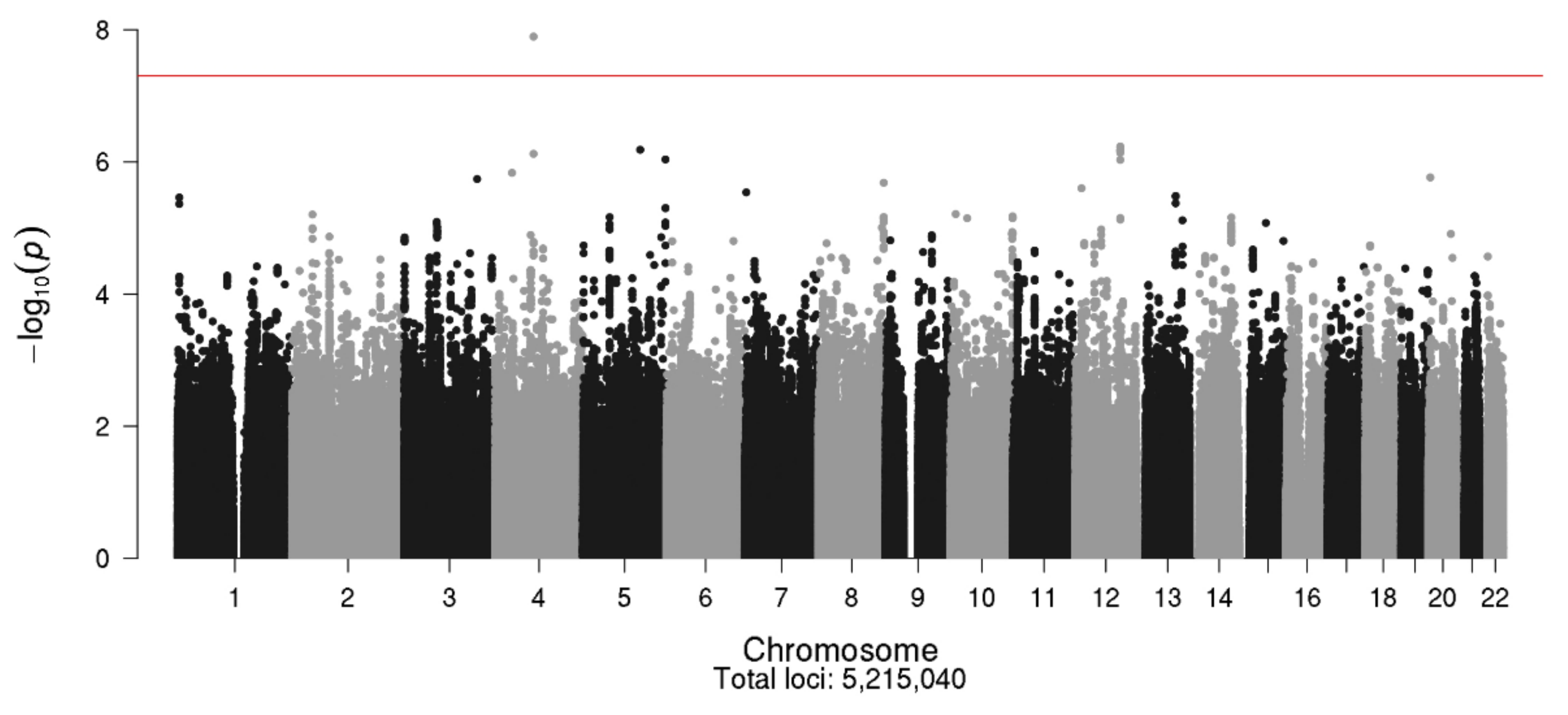
3.2. Genome-Wide Association Study (GWAS) Results
3.3. Candidate SNP Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, A.; Hertz, D.L.; Morales, M.; Adams, E.J.; Gordon, S.; Tan, C.J.; Staff, N.P.; Kamath, J.; Oh, J.; Shinde, S.; et al. Biological predictors of chemotherapy-induced peripheral neuropathy (CIPN): MASCC neurological complications working group overview. Support Care Cancer 2019, 27, 3729–3737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colvin, L.A. Chemotherapy-induced peripheral neuropathy: Where are we now? Pain 2019, 160, S1–S10. [Google Scholar] [CrossRef] [PubMed]
- Staff, N.P.; Grisold, A.; Grisold, W.; Windebank, A.J. Chemotherapy-induced peripheral neuropathy: A current review. Ann. Neurol. 2017, 81, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Travis, L.B.; Fossa, S.D.; Sesso, H.D.; Frisina, R.D.; Herrmann, D.N.; Beard, C.J.; Feldman, D.R.; Pagliaro, L.C.; Miller, R.C.; Vaughn, D.J.; et al. Chemotherapy-induced peripheral neurotoxicity and ototoxicity: New paradigms for translational genomics. J. Natl. Cancer Inst. 2014. [CrossRef] [PubMed] [Green Version]
- Flatters, S.J.L.; Dougherty, P.M.; Colvin, L.A. Clinical and preclinical perspectives on Chemotherapy-Induced Peripheral Neuropathy (CIPN): A narrative review. Br. J. Anaesth. 2017, 119, 737–749. [Google Scholar] [CrossRef] [Green Version]
- Hershman, D.L.; Lacchetti, C.; Dworkin, R.H.; Lavoie Smith, E.M.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Gavin, P.; Lavino, A.; Lustberg, M.B.; et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J. Clin. Oncol. 2014, 32, 1941–1967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, T.M.; Ryan, S.J.; Bennett, A.V.; Stover, A.M.; Saracino, R.M.; Rogak, L.J.; Jewell, S.T.; Matsoukas, K.; Li, Y.; Basch, E. The association between clinician-based common terminology criteria for adverse events (CTCAE) and patient-reported outcomes (PRO): A systematic review. Support Care Cancer 2016, 24, 3669–3676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleeland, C.S.; Sloan, J.A.; Group, A.O. Assessing the Symptoms of Cancer Using Patient-Reported Outcomes (ASCPRO): Searching for standards. J. Pain Symptom Manag. 2010, 39, 1077–1085. [Google Scholar] [CrossRef]
- Niska, J.R.; Thorpe, C.S.; Halyard, M.Y.; Tan, A.D.; Atherton, P.J.; Dueck, A.C.; Patel, S.H.; Sloan, J.A. Patient-reported quality-of-life outcomes in relation to provider-assessed adverse events during head and neck radiotherapy. J. Patient Rep. Outcomes 2020, 4, 60. [Google Scholar] [CrossRef]
- Quinten, C.; Maringwa, J.; Gotay, C.C.; Martinelli, F.; Coens, C.; Reeve, B.B.; Flechtner, H.; Greimel, E.; King, M.; Osoba, D.; et al. Patient self-reports of symptoms and clinician ratings as predictors of overall cancer survival. J. Natl. Cancer Inst. 2011, 103, 1851–1858. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Satele, D.; Pattabasavaiah, S.; Buckner, J.C.; Sloan, J.A. Normative data and clinically significant effect sizes for single-item numerical linear analogue self-assessment (LASA) scales. Health Qual. Life Outcomes 2014, 12, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sloan, J.A.; Berk, L.; Roscoe, J.; Fisch, M.J.; Shaw, E.G.; Wyatt, G.; Morrow, G.R.; Dueck, A.C.; National Cancer, I. Integrating patient-reported outcomes into cancer symptom management clinical trials supported by the National Cancer Institute-sponsored clinical trials networks. J. Clin. Oncol. 2007, 25, 5070–5077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sloan, J.A.; Halyard, M.; El Naqa, I.; Mayo, C. Lessons From Large-Scale Collection of Patient-Reported Outcomes: Implications for Big Data Aggregation and Analytics. Int. J. Radiat Oncol. Biol. Phys. 2016, 95, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Zorina-Lichtenwalter, K.; Parisien, M.; Diatchenko, L. Genetic studies of human neuropathic pain conditions: A review. Pain 2018, 159, 583–594. [Google Scholar] [CrossRef]
- Cavaletti, G.; Cornblath, D.R.; Merkies, I.S.J.; Postma, T.J.; Rossi, E.; Frigeni, B.; Alberti, P.; Bruna, J.; Velasco, R.; Argyriou, A.A.; et al. The chemotherapy-induced peripheral neuropathy outcome measures standardization study: From consensus to the first validity and reliability findings. Ann. Oncol. 2013, 24, 454–462. [Google Scholar] [CrossRef]
- Hertz, D.L. Concerns regarding use of patient-reported outcomes in biomarker studies of chemotherapy-induced peripheral neuropathy. Pharm. J. 2019, 19, 411–416. [Google Scholar] [CrossRef]
- Cliff, J.; Jorgensen, A.L.; Lord, R.; Azam, F.; Cossar, L.; Carr, D.F.; Pirmohamed, M. The molecular genetics of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2017, 120, 127–140. [Google Scholar] [CrossRef]
- Abraham, J.E.; Guo, Q.; Dorling, L.; Tyrer, J.; Ingle, S.; Hardy, R.; Vallier, A.L.; Hiller, L.; Burns, R.; Jones, L.; et al. Replication of genetic polymorphisms reported to be associated with taxane-related sensory neuropathy in patients with early breast cancer treated with Paclitaxel. Clin. Cancer Res. 2014, 20, 2466–2475. [Google Scholar] [CrossRef] [Green Version]
- Argyriou, A.A.; Bruna, J.; Genazzani, A.A.; Cavaletti, G. Chemotherapy-induced peripheral neurotoxicity: Management informed by pharmacogenetics. Nat. Rev. Neurol. 2017, 13, 492–504. [Google Scholar] [CrossRef]
- Baldwin, R.M.; Owzar, K.; Zembutsu, H.; Chhibber, A.; Kubo, M.; Jiang, C.; Watson, D.; Eclov, R.J.; Mefford, J.; McLeod, H.L.; et al. A genome-wide association study identifies novel loci for paclitaxel-induced sensory peripheral neuropathy in CALGB 40101. Clin. Cancer Res. 2012, 18, 5099–5109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Custodio, A.; Moreno-Rubio, J.; Aparicio, J.; Gallego-Plazas, J.; Yaya, R.; Maurel, J.; Higuera, O.; Burgos, E.; Ramos, D.; Calatrava, A.; et al. Pharmacogenetic predictors of severe peripheral neuropathy in colon cancer patients treated with oxaliplatin-based adjuvant chemotherapy: A GEMCAD group study. Ann. Oncol. 2014, 25, 398–403. [Google Scholar] [CrossRef]
- Green, H.; Soderkvist, P.; Rosenberg, P.; Horvath, G.; Peterson, C. mdr-1 single nucleotide polymorphisms in ovarian cancer tissue: G2677T/A correlates with response to paclitaxel chemotherapy. Clin. Cancer Res. 2006, 12, 854–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasmats, J.; Kupershmidt, I.; Rodriguez-Antona, C.; Su, Q.J.; Khan, M.S.; Jara, C.; Mielgo, X.; Lundeberg, J.; Green, H. Identification of candidate SNPs for drug induced toxicity from differentially expressed genes in associated tissues. Gene 2012, 506, 62–68. [Google Scholar] [CrossRef]
- Kanai, M.; Kawaguchi, T.; Kotaka, M.; Shinozaki, K.; Touyama, T.; Manaka, D.; Ishigure, K.; Hasegawa, J.; Munemoto, Y.; Matsui, T.; et al. Large-scale prospective pharmacogenomics study of oxaliplatin-induced neuropathy in colon cancer patients enrolled in the JFMC41-1001-C2 (JOIN Trial). Ann. Oncol. 2016, 27, 1143–1148. [Google Scholar] [CrossRef] [Green Version]
- Leandro-Garcia, L.J.; Inglada-Perez, L.; Pita, G.; Hjerpe, E.; Leskela, S.; Jara, C.; Mielgo, X.; Gonzalez-Neira, A.; Robledo, M.; Avall-Lundqvist, E.; et al. Genome-wide association study identifies ephrin type A receptors implicated in paclitaxel induced peripheral sensory neuropathy. J. Med. Genet. 2013, 50, 599–605. [Google Scholar] [CrossRef]
- Leandro-Garcia, L.J.; Leskela, S.; Jara, C.; Green, H.; Avall-Lundqvist, E.; Wheeler, H.E.; Dolan, M.E.; Inglada-Perez, L.; Maliszewska, A.; de Cubas, A.A.; et al. Regulatory polymorphisms in beta-tubulin IIa are associated with paclitaxel-induced peripheral neuropathy. Clin. Cancer Res. 2012, 18, 4441–4448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leskela, S.; Jara, C.; Leandro-Garcia, L.J.; Martinez, A.; Garcia-Donas, J.; Hernando, S.; Hurtado, A.; Vicario, J.C.; Montero-Conde, C.; Landa, I.; et al. Polymorphisms in cytochromes P450 2C8 and 3A5 are associated with paclitaxel neurotoxicity. Pharm. J. 2011, 11, 121–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoudpour, S.H.; Bandapalli, O.R.; da Silva Filho, M.I.; Campo, C.; Hemminki, K.; Goldschmidt, H.; Merz, M.; Forsti, A. Chemotherapy-induced peripheral neuropathy: Evidence from genome-wide association studies and replication within multiple myeloma patients. BMC Cancer 2018, 18, 820. [Google Scholar] [CrossRef] [Green Version]
- Oguri, T.; Mitsuma, A.; Inada-Inoue, M.; Morita, S.; Shibata, T.; Shimokata, T.; Sugishita, M.; Nakayama, G.; Uehara, K.; Hasegawa, Y.; et al. Genetic polymorphisms associated with oxaliplatin-induced peripheral neurotoxicity in Japanese patients with colorectal cancer. Int. J. Clin. Pharmacol. Ther. 2013, 51, 475–481. [Google Scholar] [CrossRef]
- Sissung, T.M.; Mross, K.; Steinberg, S.M.; Behringer, D.; Figg, W.D.; Sparreboom, A.; Mielke, S. Association of ABCB1 genotypes with paclitaxel-mediated peripheral neuropathy and neutropenia. Eur. J. Cancer 2006, 42, 2893–2896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sucheston-Campbell, L.E.; Clay-Gilmour, A.I.; Barlow, W.E.; Budd, G.T.; Stram, D.O.; Haiman, C.A.; Sheng, X.; Yan, L.; Zirpoli, G.; Yao, S.; et al. Genome-wide meta-analyses identifies novel taxane-induced peripheral neuropathy-associated loci. Pharm. Genom. 2018, 28, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Won, H.H.; Lee, J.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; Kim, J.W.; Lee, S.Y.; Park, S.H. Polymorphic markers associated with severe oxaliplatin-induced, chronic peripheral neuropathy in colon cancer patients. Cancer 2012, 118, 2828–2836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertz, D.L.; Roy, S.; Motsinger-Reif, A.A.; Drobish, A.; Clark, L.S.; McLeod, H.L.; Carey, L.A.; Dees, E.C. CYP2C8*3 increases risk of neuropathy in breast cancer patients treated with paclitaxel. Ann. Oncol. 2013, 24, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Terrazzino, S.; Argyriou, A.A.; Cargnin, S.; Antonacopoulou, A.G.; Briani, C.; Bruna, J.; Velasco, R.; Alberti, P.; Campagnolo, M.; Lonardi, S.; et al. Genetic determinants of chronic oxaliplatin-induced peripheral neurotoxicity: A genome-wide study replication and meta-analysis. J. Peripher. Nerv. Syst. 2015, 20, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Beutler, A.S.; Kulkarni, A.A.; Kanwar, R.; Klein, C.J.; Therneau, T.M.; Qin, R.; Banck, M.S.; Boora, G.K.; Ruddy, K.J.; Wu, Y.; et al. Sequencing of Charcot-Marie-Tooth disease genes in a toxic polyneuropathy. Ann. Neurol. 2014, 76, 727–737. [Google Scholar] [CrossRef] [Green Version]
- Boora, G.K.; Kulkarni, A.A.; Kanwar, R.; Beyerlein, P.; Qin, R.; Banck, M.S.; Ruddy, K.J.; Pleticha, J.; Lynch, C.A.; Behrens, R.J.; et al. Association of the Charcot-Marie-Tooth disease gene ARHGEF10 with paclitaxel induced peripheral neuropathy in NCCTG N08CA (Alliance). J. Neurol. Sci. 2015, 357, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Le-Rademacher, J.G.; Lopez, C.L.; Kanwar, R.; Major-Elechi, B.; Abyzov, A.; Banck, M.S.; Therneau, T.M.; Sloan, J.A.; Loprinzi, C.L.; Beutler, A.S. Neurological safety of oxaliplatin in patients with uncommon variants in Charcot-Marie-tooth disease genes. J. Neurol. Sci. 2020, 411, 116687. [Google Scholar] [CrossRef] [Green Version]
- Leal, A.D.; Qin, R.; Atherton, P.J.; Haluska, P.; Behrens, R.J.; Tiber, C.H.; Watanaboonyakhet, P.; Weiss, M.; Adams, P.T.; Dockter, T.J.; et al. North Central Cancer Treatment Group/Alliance trial N08CA-the use of glutathione for prevention of paclitaxel/carboplatin-induced peripheral neuropathy: A phase 3 randomized, double-blind, placebo-controlled study. Cancer 2014, 120, 1890–1897. [Google Scholar] [CrossRef] [Green Version]
- Loprinzi, C.L.; Qin, R.; Dakhil, S.R.; Fehrenbacher, L.; Flynn, K.A.; Atherton, P.; Seisler, D.; Qamar, R.; Lewis, G.C.; Grothey, A. Phase III randomized, placebo-controlled, double-blind study of intravenous calcium and magnesium to prevent oxaliplatin-induced sensory neurotoxicity (N08CB/Alliance). J. Clin. Oncol. 2014, 32, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Loprinzi, C.L.; Reeves, B.N.; Dakhil, S.R.; Sloan, J.A.; Wolf, S.L.; Burger, K.N.; Kamal, A.; Le-Lindqwister, N.A.; Soori, G.S.; Jaslowski, A.J.; et al. Natural history of paclitaxel-associated acute pain syndrome: Prospective cohort study NCCTG N08C1. J. Clin. Oncol. 2011, 29, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Reeves, B.N.; Dakhil, S.R.; Sloan, J.A.; Wolf, S.L.; Burger, K.N.; Kamal, A.; Le-Lindqwister, N.A.; Soori, G.S.; Jaslowski, A.J.; Kelaghan, J.; et al. Further data supporting that paclitaxel-associated acute pain syndrome is associated with development of peripheral neuropathy: North Central Cancer Treatment Group trial N08C1. Cancer 2012, 118, 5171–5178. [Google Scholar] [CrossRef]
- Le-Rademacher, J.; Kanwar, R.; Seisler, D.; Pachman, D.R.; Qin, R.; Abyzov, A.; Ruddy, K.J.; Banck, M.S.; Lavoie Smith, E.M.; Dorsey, S.G.; et al. Patient-reported (EORTC QLQ-CIPN20) versus physician-reported (CTCAE) quantification of oxaliplatin- and paclitaxel/carboplatin-induced peripheral neuropathy in NCCTG/Alliance clinical trials. Support Care Cancer 2017, 25, 3537–3544. [Google Scholar] [CrossRef] [PubMed]
- Pachman, D.R.; Qin, R.; Seisler, D.K.; Smith, E.M.; Beutler, A.S.; Ta, L.E.; Lafky, J.M.; Wagner-Johnston, N.D.; Ruddy, K.J.; Dakhil, S.; et al. Clinical Course of Oxaliplatin-Induced Neuropathy: Results From the Randomized Phase III Trial N08CB (Alliance). J. Clin. Oncol. 2015, 33, 3416–3422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postma, T.J.; Aaronson, N.K.; Heimans, J.J.; Muller, M.J.; Hildebrand, J.G.; Delattre, J.Y.; Hoang-Xuan, K.; Lanteri-Minet, M.; Grant, R.; Huddart, R.; et al. The development of an EORTC quality of life questionnaire to assess chemotherapy-induced peripheral neuropathy: The QLQ-CIPN20. Eur. J. Cancer 2005, 41, 1135–1139. [Google Scholar] [CrossRef]
- Sloan, J.A.; Dueck, A. Issues for statisticians in conducting analyses and translating results for quality of life end points in clinical trials. J. Biopharm. Stat. 2004, 14, 73–96. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Closas, M.; Couch, F.J.; Lindstrom, S.; Michailidou, K.; Schmidt, M.K.; Brook, M.N.; Orr, N.; Rhie, S.K.; Riboli, E.; Feigelson, H.S.; et al. Genome-wide association studies identify four ER negative-specific breast cancer risk loci. Nat. Genet. 2013, 45, 392–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. Am. J. Hum. Genet. 2019, 104, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michailidou, K.; Hall, P.; Gonzalez-Neira, A.; Ghoussaini, M.; Dennis, J.; Milne, R.L.; Schmidt, M.K.; Chang-Claude, J.; Bojesen, S.E.; Bolla, M.K.; et al. Large-scale genotyping identifies 41 new loci associated with breast cancer risk. Nat. Genet. 2013, 45, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Manichaikul, A.; Mychaleckyj, J.C.; Rich, S.S.; Daly, K.; Sale, M.; Chen, W.M. Robust relationship inference in genome-wide association studies. Bioinformatics 2010, 26, 2867–2873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pritchard, J.K.; Stephens, M.; Donnelly, P. Inference of population structure using multilocus genotype data. Genetics 2000, 155, 945–959. [Google Scholar] [PubMed]
- Das, S.; Forer, L.; Schonherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; Vrieze, S.I.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-generation genotype imputation service and methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar] [CrossRef] [Green Version]
- Argyriou, A.A.; Cavaletti, G.; Antonacopoulou, A.; Genazzani, A.A.; Briani, C.; Bruna, J.; Terrazzino, S.; Velasco, R.; Alberti, P.; Campagnolo, M.; et al. Voltage-gated sodium channel polymorphisms play a pivotal role in the development of oxaliplatin-induced peripheral neurotoxicity: Results from a prospective multicenter study. Cancer 2013, 119, 3570–3577. [Google Scholar] [CrossRef] [PubMed]
- Hertz, D.L.; Motsinger-Reif, A.A.; Drobish, A.; Winham, S.J.; McLeod, H.L.; Carey, L.A.; Dees, E.C. CYP2C8*3 predicts benefit/risk profile in breast cancer patients receiving neoadjuvant paclitaxel. Breast Cancer Res. Treat 2012, 134, 401–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, P.L.; Furfari, A.; Wan, B.A.; Lam, H.; Charames, G.; Drost, L.; Fefekos, A.; Ohearn, S.; Blake, A.; Asthana, R.; et al. Predictive biomarkers of chemotherapy-induced peripheral neuropathy—A review. Biomark. Med. 2018, 12, 907–916. [Google Scholar] [CrossRef]
- Manolio, T.A. Genomewide association studies and assessment of the risk of disease. N. Engl. J. Med. 2010, 363, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Pe’er, I.; Yelensky, R.; Altshuler, D.; Daly, M.J. Estimation of the multiple testing burden for genomewide association studies of nearly all common variants. Genet. Epidemiol. 2008, 32, 381–385. [Google Scholar] [CrossRef]
- Pruim, R.J.; Welch, R.P.; Sanna, S.; Teslovich, T.M.; Chines, P.S.; Gliedt, T.P.; Boehnke, M.; Abecasis, G.R.; Willer, C.J. LocusZoom: Regional visualization of genome-wide association scan results. Bioinformatics 2010, 26, 2336–2337. [Google Scholar] [CrossRef] [Green Version]
- Alexander, T.A.; Machiela, M.J. LDpop: An interactive online tool to calculate and visualize geographic LD patterns. BMC Bioinform. 2020, 21, 14. [Google Scholar] [CrossRef]
- Myers, T.A.; Chanock, S.J.; Machiela, M.J. LDlinkR: An R Package for Rapidly Calculating Linkage Disequilibrium Statistics in Diverse Populations. Front. Genet. 2020, 11, 157. [Google Scholar] [CrossRef] [Green Version]
- Gamelin, L.; Capitain, O.; Morel, A.; Dumont, A.; Traore, S.; Anne le, B.; Gilles, S.; Boisdron-Celle, M.; Gamelin, E. Predictive factors of oxaliplatin neurotoxicity: The involvement of the oxalate outcome pathway. Clin. Cancer Res. 2007, 13, 6359–6368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inada, M.; Sato, M.; Morita, S.; Kitagawa, K.; Kawada, K.; Mitsuma, A.; Sawaki, M.; Fujita, K.; Ando, Y. Associations between oxaliplatin-induced peripheral neuropathy and polymorphisms of the ERCC1 and GSTP1 genes. Int. J. Clin. Pharmacol. Ther. 2010, 48, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Goekkurt, E.; Al-Batran, S.E.; Hartmann, J.T.; Mogck, U.; Schuch, G.; Kramer, M.; Jaeger, E.; Bokemeyer, C.; Ehninger, G.; Stoehlmacher, J. Pharmacogenetic analyses of a phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil and leucovorin plus either oxaliplatin or cisplatin: A study of the arbeitsgemeinschaft internistische onkologie. J. Clin. Oncol. 2009, 27, 2863–2873. [Google Scholar] [CrossRef] [PubMed]
- McLeod, H.L.; Sargent, D.J.; Marsh, S.; Green, E.M.; King, C.R.; Fuchs, C.S.; Ramanathan, R.K.; Williamson, S.K.; Findlay, B.P.; Thibodeau, S.N.; et al. Pharmacogenetic predictors of adverse events and response to chemotherapy in metastatic colorectal cancer: Results from North American Gastrointestinal Intergroup Trial N9741. J. Clin. Oncol. 2010, 28, 3227–3233. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kang, H.G.; Yoo, S.S.; Kang, Y.R.; Choi, Y.Y.; Lee, W.K.; Choi, J.E.; Jeon, H.S.; Shin, K.M.; Oh, I.J.; et al. Polymorphisms in DNA repair and apoptosis-related genes and clinical outcomes of patients with non-small cell lung cancer treated with first-line paclitaxel-cisplatin chemotherapy. Lung Cancer 2013, 82, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Bao, T.; Basal, C.; Seluzicki, C.; Li, S.Q.; Seidman, A.D.; Mao, J.J. Long-term chemotherapy-induced peripheral neuropathy among breast cancer survivors: Prevalence, risk factors, and fall risk. Breast Cancer Res. Treat. 2016, 159, 327–333. [Google Scholar] [CrossRef]
- Cox-Martin, E.; Trahan, L.H.; Cox, M.G.; Dougherty, P.M.; Lai, E.A.; Novy, D.M. Disease burden and pain in obese cancer patients with chemotherapy-induced peripheral neuropathy. Support Care Cancer 2017, 25, 1873–1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenlee, H.; Hershman, D.L.; Shi, Z.; Kwan, M.L.; Ergas, I.J.; Roh, J.M.; Kushi, L.H. BMI, Lifestyle Factors and Taxane-Induced Neuropathy in Breast Cancer Patients: The Pathways Study. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiadens, A.A.; den Hollander, A.I.; Roosing, S.; Nabuurs, S.B.; Zekveld-Vroon, R.C.; Collin, R.W.; De Baere, E.; Koenekoop, R.K.; van Schooneveld, M.J.; Strom, T.M.; et al. Homozygosity mapping reveals PDE6C mutations in patients with early-onset cone photoreceptor disorders. Am. J. Hum. Genet. 2009, 85, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemler, M.E. Tetraspanin proteins mediate cellular penetration, invasion, and fusion events and define a novel type of membrane microdomain. Annu. Rev. Cell. Dev. Biol. 2003, 19, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.; Shoham, T. The tetraspanin web modulates immune-signalling complexes. Nat. Rev. Immunol. 2005, 5, 136–148. [Google Scholar] [CrossRef]
- Tarrant, J.M.; Robb, L.; van Spriel, A.B.; Wright, M.D. Tetraspanins: Molecular organisers of the leukocyte surface. Trends. Immunol. 2003, 24, 610–617. [Google Scholar] [CrossRef]
- Liu, J.; Li, M.; Su, B. GWAS-identified schizophrenia risk SNPs at TSPAN18 are highly diverged between Europeans and East Asians. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2016, 171, 1032–1040. [Google Scholar] [CrossRef]
- Ma, L.; Tang, J.; Wang, D.; Zhang, W.; Liu, W.; Wang, D.; Liu, X.H.; Gong, W.; Yao, Y.G.; Chen, X. Evaluating risk loci for schizophrenia distilled from genome-wide association studies in Han Chinese from Central China. Mol. Psychiatry 2013, 18, 638–639. [Google Scholar] [CrossRef]
- Yuan, J.; Jin, C.; Qin, H.D.; Wang, J.; Sha, W.; Wang, M.; Zhang, Y.; Zhang, F.; Li, J.; Li, J.; et al. Replication study confirms link between TSPAN18 mutation and schizophrenia in Han Chinese. PLoS ONE 2013, 8, e58785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Li, D.X.; Lu, N.; Fan, Q.R.; Li, W.H.; Feng, Z.F. Lack of Association between the TSPAN18 Gene and Schizophrenia Based on New Data from Han Chinese and a Meta-Analysis. Int. J. Mol. Sci. 2015, 16, 11864–11872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, G.S.; Lee, B.; Wee, J.; Chun, H.; Kim, H.; Jung, J.; Cha, J.Y.; Riew, T.R.; Kim, G.H.; Kim, I.B.; et al. Tentonin 3/TMEM150c Confers Distinct Mechanosensitive Currents in Dorsal-Root Ganglion Neurons with Proprioceptive Function. Neuron 2016, 91, 107–118. [Google Scholar] [CrossRef]
- Chhibber, A.; Mefford, J.; Stahl, E.A.; Pendergrass, S.A.; Baldwin, R.M.; Owzar, K.; Li, M.; Winer, E.P.; Hudis, C.A.; Zembutsu, H.; et al. Polygenic inheritance of paclitaxel-induced sensory peripheral neuropathy driven by axon outgrowth gene sets in CALGB 40101 (Alliance). Pharm. J. 2014, 14, 336–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipton, R.B.; Apfel, S.C.; Dutcher, J.P.; Rosenberg, R.; Kaplan, J.; Berger, A.; Einzig, A.I.; Wiernik, P.; Schaumburg, H.H. Taxol produces a predominantly sensory neuropathy. Neurology 1989, 39, 368–373. [Google Scholar] [CrossRef]
- Sloan, J.A.; Aaronson, N.; Cappelleri, J.C.; Fairclough, D.L.; Varricchio, C.; Clinical Significance Consensus Meeting Group. Assessing the clinical significance of single items relative to summated scores. Mayo Clin. Proc. 2002, 77, 479–487. [Google Scholar] [CrossRef]
- Sprangers, M.A.; Thong, M.S.; Bartels, M.; Barsevick, A.; Ordoñana, J.; Shi, Q.; Wang, X.S.; Klepstad, P.; Wierenga, E.A.; Singh, J.A.; et al. Biological pathways, candidate genes, and molecular markers associated with quality-of-life domains: An update. Qual. Life Res. 2014, 23, 1997–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motsinger-Reif, A.A.; Jorgenson, E.; Relling, M.V.; Kroetz, D.L.; Weinshilboum, R.; Cox, N.J.; Roden, D.M. Genome-wide association studies in pharmacogenomics: Successes and lessons. Pharm. Genom. 2013, 23, 383–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Study (Participants a) | ||||
|---|---|---|---|---|---|
| N08C1 (246) | N08CA (150) | N08CB (296) | Total (692) | ||
| Age | Mean (SD) | 56.5 (11.4) | 61.0 (10.4) | 56.7 (11.3) | 57.6 (11.3) |
| Median (Q1, Q3) | 56.0 (48.2, 64.0) | 61.5 (55.0, 68.0) | 56.0 (50.0, 65.0) | 57.0 (50.0, 65.2) | |
| Range | 23.0–85.0 | 28.0–85.0 | 24.0–83.0 | 23.0–85.0 | |
| Sex (%) | Female | 213 (86.6%) | 122 (81.3%) | 157 (53.0%) | 492 (71.1%) |
| Male | 33 (13.4%) | 28 (18.7%) | 139 (47.0%) | 200 (28.9%) | |
| Race (%) | White | 202 (82.1%) | 139 (92.7%) | 252 (85.1%) | 593 (85.7%) |
| Black/African American | 30 (12.2%) | 9 (6.0%) | 34 (11.5%) | 73 (10.5%) | |
| Native Hawaiian or Other Pacific Islander | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Asian | 11 (4.5%) | 2 (1.3%) | 5 (1.7%) | 18 (2.6%) | |
| American Indian or Alaska Native | 1 (0.4%) | 0 (0.0%) | 3 (1.0%) | 4 (0.6%) | |
| Not Reported | 2 (0.8%) | 0 (0.0%) | 1 (0.3%) | 3 (0.4%) | |
| Unknown | 0 (0.0%) | 0 (0.0%) | 1 (0.3%) | 1 (0.1%) | |
| Body Mass Index | Missing data b | 246 | 0 | 1 | 247 |
| Mean (SD) | NA | 27.7 (8.0) | 28.9 (7.1) | 28.5 (7.4) | |
| Median (Q1, Q3) | NA | 25.5 (22.2, 30.5) | 27.6 (24.4, 31.9) | 26.9 (23.6, 31.8) | |
| Range | NA | 16.7–62.5 | 15.3–64.8 | 15.3–64.8 | |
| ECOG Performance Status (PS), (%) | 0 | 152 (61.8%) | 70 (46.7%) | 195 (65.9%) | 417 (60.3%) |
| 1 | 94 (38.2%) | 70 (46.7%) | 98 (33.1%) | 262 (37.9%) | |
| 2 | 0 (0.0%) | 10 (6.7%) | 3 (1.0%) | 13 (1.9%) | |
| Baseline Neuropathy- National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) v4 (%) | None | 246 (100.0%) | 133 (88.7%) | 296 (100.0%) | 675 (97.5%) |
| Grade 1 | 0 (0.0%) | 17 (11.3%) | 0 (0.0%) | 17 (2.5%) | |
| Baseline CIPN20 Sensory Score | Mean (SD) | 97.3 (5.1) | 94.7 (8.7) | 98.1 (5.0) | 97.1 (6.2) |
| Median (Q1, Q3) | 100.0 (96.3, 100.0) | 100.0 (92.6, 100.0) | 100.0 (100.0, 100.0) | 100.0 (96.3, 100.0) | |
| Range | 70.4–100.0 | 33.3–100.0 | 44.4–100.0 | 33.3–100.0 | |
| Cancer Type (%) | Breast | 143 (58.1%) | ND | 0 | ND |
| Lung | 38 (15.4%) | 43 (28.7%) | 0 | 81 (11.7%) | |
| c Ovarian | 36 (14.6%) | 54 (36.0%) | 0 | 90 (13.0%) | |
| d Colorectal | ND | ND | 296 (100.0%) | ND | |
| Other | 29 (11.8%) | 39 (26.0%) | 0 | ND | |
| Not reported | 0 | 14 (9.3%) | 0 | 14 (2.0%) | |
| Clinical Feature | Covariate | Coefficient | p-Value | Overall p-Value | |
|---|---|---|---|---|---|
| Estimate | SE | ||||
| Sex | Female (reference) | - | - | - | - |
| Male | 3.29 | 1.77 | 0.06 | ||
| Chemotherapy Regimen | Oxaliplatin 2 wk (reference) | - | - | - | 3.0 × 10−8 |
| Pac Only 1 wk | −9.01 | 2.55 | 0.0004 | ||
| Pac Only 2 wk | −15.32 | 3.94 | 0.0001 | ||
| Pac Only 3 wk | −7.23 | 6.02 | 0.23 | ||
| Pac and Carb 1 wk | 3.71 | 2.66 | 0.16 | ||
| Pac and Carb 3 wk | −8.26 | 1.82 | 6.77 × 10−6 | ||
| Genetic Ancestry | European (reference) | - | - | - | 0.007 |
| African | −7.63 | 2.43 | 0.002 | ||
| Asian | 0.98 | 4.86 | 0.84 | ||
| Characteristics of Participants (n = 381) | |||
|---|---|---|---|
| Cancer Diagnosis | CIPN Reported | ||
| Age | Mean (SD) | 48.4 (9.5) | 55.5 (10.8) |
| Median (SD) | 48.4 (42.2–53.8) | 56.0 (48.8–62.4) | |
| Range | 24.9–82.7 | 28.6–87.6 | |
| Sex (Gender) | Female | 380 (99.7%) | |
| Male | 1 (0.3%) | ||
| Race | White | 374 (98.2%) | |
| Non-white, unknown, or undisclosed | 7 (1.8%) | ||
| Body Mass Index (N) | Missing data | 32 | |
| Mean (SD) | 27.9 (5.7) | ||
| Median (Q1, Q3) | 27.0 (23.9, 31.1) | ||
| Range | 15.8–46.0 | ||
| Years from Cancer Diagnosis to CIPN20 | Mean (SD) | 7.1 (3.7) | |
| Median (Q1, Q3) | 7.2 (3.2, 10.0) | ||
| Range | 1.8–15.7 | ||
| Treatment | Taxane only | 342 (89.8%) | |
| Taxane and platin | 39 (10.2%) | ||
| Genotyping Platform | OncoArray | 233 (61.2%) | |
| iCOGS | 148 (38.8%) | ||
| Clinical Feature | Covariate | Coefficient | p-Value | |
|---|---|---|---|---|
| Estimate | SE | |||
| Age (Years) | −0.31 | 0.09 | 0.0004 | |
| Years from Cancer Diagnosis to CIPN20 | 0.33 | 0.35 | 0.34 | |
| Treatment | Taxane only | - | - | - |
| Taxane and platin | −1.28 | 2.7 | 0.64 | |
| Genotyping Platform | OncoArray | - | - | - |
| iCOGS | −1.15 | 2.24 | 0.64 | |
| RSID | 1 Gene | Chr | Position (bp) | Allele | Sample numbers (Genotype) | Minor Allele Freq (alt.freq) | Coefficient | p-value | p-value in MCBDR | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref -Major | Alt -Minor | Major -ref/ref | Hetero-zygous -ref/alt | Variant -alt/alt | Estimate | SE | |||||||
| rs56360211 | PDE6C | 10 | 95374453 | T | G | 623 | 66 | 3 | 0.054 | −12.92 | 2.38 | 7.92 × 10−8 | 0.34 |
| rs1515252 | - | 2 | 146779243 | G | A | 314 | 302 | 76 | 0.328 | −5.96 | 1.11 | 1.18 × 10−7 | 0.07 |
| rs10769096 | TSPAN18 | 11 | 44943260 | G | A | 479 | 180 | 33 | 0.174 | −7.74 | 1.46 | 1.65 × 10−7 | 0.82 |
| rs16825861 | - | 2 | 146742030 | G | A | 318 | 301 | 73 | 0.323 | −5.87 | 1.12 | 2.32 × 10−7 | 0.11 |
| rs13026986 | - | 2 | 146753902 | T | G | 318 | 301 | 73 | 0.321 | −5.91 | 1.13 | 2.36 × 10−7 | 0.11 |
| rs1606806 | - | 2 | 146758685 | C | T | 317 | 302 | 73 | 0.322 | −5.91 | 1.13 | 2.39 × 10−7 | 0.10 |
| rs34053477 | - | 2 | 146742600 | G | A | 318 | 301 | 73 | 0.321 | −5.90 | 1.13 | 2.43 × 10−7 | 0.11 |
| rs16825916 | - | 2 | 146768842 | A | G | 317 | 301 | 74 | 0.322 | −5.88 | 1.13 | 2.56 × 10−7 | 0.10 |
| rs7583107 | - | 2 | 146819721 | C | T | 71 | 325 | 296 | 0.663 | 5.74 | 1.12 | 3.91 × 10−7 | 0.04 |
| rs4662450 | - | 2 | 146806610 | A | C | 71 | 325 | 296 | 0.659 | 5.77 | 1.13 | 3.92 × 10−7 | 0.05 |
| rs7565993 | - | 2 | 146803053 | A | G | 71 | 325 | 296 | 0.659 | 5.77 | 1.13 | 3.97 × 10−7 | 0.05 |
| rs4969675 | - | X | 95803439 | T | C | 15 | 244 | 433 | 0.788 | 13.27 | 2.62 | 5.16 × 10−7 | - |
| rs36049952 | - | 2 | 146839632 | T | C | 346 | 286 | 60 | 0.292 | −5.84 | 1.18 | 9.25 × 10−7 | 0.04 |
| rs12991309 | - | 2 | 146822623 | G | A | 346 | 286 | 60 | 0.292 | −5.83 | 1.18 | 9.38 × 10−7 | 0.04 |
| rs73538805 | - | X | 97724436 | T | C | 486 | 186 | 20 | 0.162 | 7.02 | 1.42 | 9.42 × 10−7 | - |
| RSID | 1 Gene | Chr | Position (bp) | Allele | Sample Numbers (Genotype) | Minor Allele Freq (alt.freq) | Coefficient | p-Value | p-Value in N08Cx | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref -Major | Alt -Minor | Major -ref/ref | Hetero-zygous -ref/alt | Variant -alt/alt | Estimate | SE | |||||||
| rs113807868 | TMEM150C | 4 | 83439324 | G | A | 346 | 32 | 3 | 0.068 | −16.18 | 2.78 | 1.27 × 10−8 | 0.77 |
| rs78825864 | - | 12 | 98169501 | C | A | 316 | 60 | 5 | 0.093 | −9.76 | 1.92 | 5.84 × 10−7 | 0.18 |
| rs77885228 | - | 12 | 98174620 | A | G | 315 | 61 | 5 | 0.095 | −9.67 | 1.91 | 6.05 × 10−7 | 0.10 |
| rs77880756 | - | 5 | 124192458 | G | A | 280 | 96 | 5 | 0.143 | −9.08 | 1.79 | 6.54 × 10−7 | 0.54 |
| rs76151599 | - | 12 | 98169090 | T | C | 315 | 61 | 5 | 0.095 | −9.64 | 1.91 | 6.65 × 10−7 | 0.10 |
| rs76505485 | - | 12 | 98169019 | A | C | 315 | 61 | 5 | 0.095 | −9.64 | 1.91 | 6.65 × 10−7 | 0.10 |
| rs76175313 | - | 12 | 98167034 | C | T | 315 | 61 | 5 | 0.095 | −9.64 | 1.91 | 6.67 × 10−7 | 0.11 |
| s75111732 | - | 12 | 98161392 | T | C | 315 | 61 | 5 | 0.095 | −9.65 | 1.91 | 6.88 × 10−7 | 0.11 |
| rs11109196 | - | 12 | 98155827 | A | G | 315 | 61 | 5 | 0.095 | −9.65 | 1.91 | 7.25 × 10−7 | 0.09 |
| rs2868379 | TMEM150C | 4 | 83438645 | T | C | 325 | 52 | 4 | 0.104 | −11.35 | 2.26 | 7.54 × 10−7 | 0.61 |
| rs4331859 | LOC105377763 | 5 | 179094108 | A | C | 266 | 106 | 9 | 0.163 | −7.55 | 1.51 | 9.17 × 10−7 | 0.04 |
| rs12317534 | LOC643711 | 12 | 98139760 | A | C | 312 | 64 | 5 | 0.098 | −9.55 | 1.91 | 9.31 × 10−7 | 0.07 |
| RSID | Gene | Chr | BP | Allele | MCBDR cohort | N08Cx cohort | Cited Articles | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref | Alt | Freq. | Beta/Effect | SE | p-Value | Freq. | Beta/Effect | SE. | p-Value | |||||
| rs1056836 | CYP1B1 | 2 | 38298203 | C | G | 0.596 | −1.00 | 1.15 | 0.38 | 0.541 | −2.08 | 1.12 | 0.06 | [19] |
| rs10771973 | FGD4 | 12 | 32792974 | G | A | 0.283 | −0.15 | 1.22 | 0.90 | 0.313 | 2.44 | 1.10 | 0.03 | [21] |
| rs8187710 | ABCC2 | 10 | 101611294 | G | A | 0.062 | −3.34 | 2.46 | 0.17 | 0.067 | −1.79 | 2.16 | 0.41 | [19] |
| rs4141404 | LIMK2 | 22 | 31675185 | A | C | 0.697 | −0.21 | 1.24 | 0.87 | 0.734 | 2.45 | 1.18 | 0.04 | [26] |
| rs11572080 | CYP2C8 | 10 | 96827030 | C | T | 0.112 | 0.00 | 1.77 | 1.00 | 0.095 | −2.81 | 1.83 | 0.13 | [54,55] |
| rs17222723 | ABCC2 | 10 | 101595996 | T | A | 0.062 | −3.31 | 2.46 | 0.18 | 0.055 | −0.38 | 2.32 | 0.87 | [19] |
| rs17781082 | GRIP1/CAND1 | 12 | 67476327 | C | T | 0.409 | 0.38 | 1.31 | 0.77 | 0.384 | 1.12 | 1.12 | 0.32 | [21] |
| rs10509681 | CYP2C8 | 10 | 96798749 | T | C | 0.114 | 0.23 | 1.72 | 0.90 | 0.095 | −2.73 | 1.83 | 0.14 | [54,55] |
| rs4737264 | XKR4 | 8 | 56111322 | A | C | 0.223 | 2.82 | 1.47 | 0.06 | 0.213 | −0.98 | 1.30 | 0.45 | [21,26] |
| rs1903216 | BCL6 | 3 | 187629503 | A | G | 0.510 | −0.10 | 1.25 | 0.93 | 0.546 | −0.75 | 1.08 | 0.49 | [21] |
| rs2233335 | NDRG1 | 8 | 134261065 | T | G | 0.363 | 0.19 | 1.27 | 0.88 | 0.341 | 0.69 | 1.12 | 0.54 | [21] |
| rs7001034 | MIR4288 -FZD3 | 8 | 28363378 | A | G | 0.603 | −0.59 | 1.15 | 0.61 | 0.563 | −0.04 | 1.07 | 0.97 | [21] |
| rs16916932 | CACNB2 | 10 | 18476276 | C | T | 0.079 | −1.57 | 2.07 | 0.45 | 0.063 | 2.75 | 2.15 | 0.20 | [21] |
| rs8110536 | C19orf21 | 19 | 756985 | T | G | 0.162 | −1.66 | 2.18 | 0.45 | 0.150 | 0.21 | 1.47 | 0.89 | [26] |
| rs10932374 | ERBB4 | 2 | 212244403 | G | A | 0.231 | 0.18 | 1.36 | 0.90 | 0.248 | −0.56 | 1.20 | 0.64 | [26] |
| rs17683288 | ARHGEF10 | 8 | 1877480 | T | G | 0.063 | −4.55 | 3.02 | 0.13 | 0.059 | 1.62 | 2.15 | 0.45 | [36,37] |
| rs7833751 | FZD3 | 8 | 28362792 | T | G | 0.598 | −0.81 | 1.15 | 0.48 | 0.539 | 0.31 | 1.04 | 0.77 | [21] |
| rs2032582 | ABCB1 | 7 | 87160618 | A | C | 0.556 | −0.64 | 1.20 | 0.59 | 0.589 | 0.89 | 1.09 | 0.41 | [19] |
| rs7349683 | EPHA5 | 4 | 66197804 | C | T | 0.345 | 0.25 | 1.30 | 0.85 | 0.329 | −0.53 | 1.12 | 0.64 | [21,26] |
| rs9657362 | ARHGEF10 | 8 | 1833801 | G | C | 0.147 | −3.24 | 1.96 | 0.10 | 0.138 | 1.66 | 1.53 | 0.28 | [36,37] |
| rs1045642 | ABCB1 | 7 | 87138645 | A | G | 0.470 | 0.20 | 1.16 | 0.86 | 0.502 | −0.05 | 1.05 | 0.96 | [19] |
| RSID | Gene | Chr | BP | Allele | MCBDR Cohort | N08Cx Cohort | Cited Articles | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref | Alt | Freq. | Beta/Effect | SE | p-Value | Freq. | Beta/Effect | SE. | p-Value | |||||
| rs34116584 | AGXT | 2 | 241808314 | C | T | 0.190 | 1.65 | 1.54 | 0.29 | 0.179 | 3.03 | 1.38 | 0.03 | [61] |
| rs797519 | DLEU7 | 13 | 51231132 | G | C | 0.417 | −1.45 | 1.26 | 0.25 | 0.392 | −1.60 | 1.10 | 0.15 | [33] |
| rs4936453 | BTG4 | 11 | 111300782 | T | G | 0.339 | −2.55 | 1.27 | 0.04 | 0.326 | −0.50 | 1.16 | 0.67 | [33] |
| rs1695 | GSTP1 | 11 | 67352689 | A | G | 0.374 | −1.04 | 1.17 | 0.38 | 0.358 | −1.54 | 1.12 | 0.17 | [62] |
| rs843748 | ACYP2 | 2 | 54502912 | G | A | 0.508 | 0.12 | 1.15 | 0.92 | 0.426 | 2.04 | 1.07 | 0.06 | [33] |
| rs6924717 | FARS2 | 6 | 5304851 | C | T | 0.156 | 0.07 | 1.61 | 0.97 | 0.140 | 2.57 | 1.52 | 0.09 | [33] |
| rs2338 | FOXC1 | 6 | 1573613 | G | A | 0.278 | 2.33 | 1.44 | 0.11 | 0.280 | 0.21 | 1.18 | 0.86 | [33] |
| rs3212986 | ERCC1 | 19 | 45912736 | C | A | 0.264 | 0.67 | 1.29 | 0.61 | 0.258 | 1.33 | 1.21 | 0.27 | [63] |
| rs1138272 | GSTP1 | 11 | 67353579 | C | T | 0.102 | −2.08 | 1.89 | 0.27 | 0.075 | −0.53 | 2.07 | 0.80 | [64] |
| rs12632942 | SCN10A | 3 | 38764998 | A | G | 0.258 | 0.65 | 1.37 | 0.63 | 0.255 | 0.85 | 1.20 | 0.48 | [53] |
| rs2302237 | SCN4A | 17 | 62048707 | C | T | 0.400 | −1.12 | 1.33 | 0.40 | 0.363 | 1.76 | 1.14 | 0.12 | [53] |
| rs25487 | XRCC1 | 19 | 44055726 | T | C | 0.643 | −1.89 | 1.18 | 0.11 | 0.659 | 0.72 | 1.11 | 0.52 | [65] |
| rs10486003 | TAC1 | 7 | 97229778 | C | T | 0.102 | 0.05 | 2.35 | 0.98 | 0.086 | −1.34 | 1.79 | 0.45 | [33] |
| rs2230641 | CCNH | 5 | 86695274 | A | G | 0.232 | −1.48 | 1.41 | 0.30 | 0.200 | 0.36 | 1.36 | 0.79 | [22] |
| rs3114018 | ABCG2 | 4 | 89064581 | A | C | 0.557 | 0.85 | 1.22 | 0.49 | 0.487 | −0.13 | 1.09 | 0.90 | [22] |
| rs17140129 | FARS2 | 6 | 5298362 | A | G | 0.151 | 0.72 | 1.62 | 0.66 | 0.128 | −0.39 | 1.61 | 0.81 | [33] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adjei, A.A.; Lopez, C.L.; Schaid, D.J.; Sloan, J.A.; Le-Rademacher, J.G.; Loprinzi, C.L.; Norman, A.D.; Olson, J.E.; Couch, F.J.; Beutler, A.S.; et al. Genetic Predictors of Chemotherapy-Induced Peripheral Neuropathy from Paclitaxel, Carboplatin and Oxaliplatin: NCCTG/Alliance N08C1, N08CA and N08CB Study. Cancers 2021, 13, 1084. https://doi.org/10.3390/cancers13051084
Adjei AA, Lopez CL, Schaid DJ, Sloan JA, Le-Rademacher JG, Loprinzi CL, Norman AD, Olson JE, Couch FJ, Beutler AS, et al. Genetic Predictors of Chemotherapy-Induced Peripheral Neuropathy from Paclitaxel, Carboplatin and Oxaliplatin: NCCTG/Alliance N08C1, N08CA and N08CB Study. Cancers. 2021; 13(5):1084. https://doi.org/10.3390/cancers13051084
Chicago/Turabian StyleAdjei, Araba A., Camden L. Lopez, Daniel J. Schaid, Jeff A. Sloan, Jennifer G. Le-Rademacher, Charles L. Loprinzi, Aaron D. Norman, Janet E. Olson, Fergus J. Couch, Andreas S. Beutler, and et al. 2021. "Genetic Predictors of Chemotherapy-Induced Peripheral Neuropathy from Paclitaxel, Carboplatin and Oxaliplatin: NCCTG/Alliance N08C1, N08CA and N08CB Study" Cancers 13, no. 5: 1084. https://doi.org/10.3390/cancers13051084