
Partial and Total Flap Failure after Fibula Free Flap in Head and Neck Reconstructive Surgery: Retrospective Analysis of 180 Flaps over 19 Years

 ,
, 

Abstract
:Simple Summary
Abstract
1. Introduction
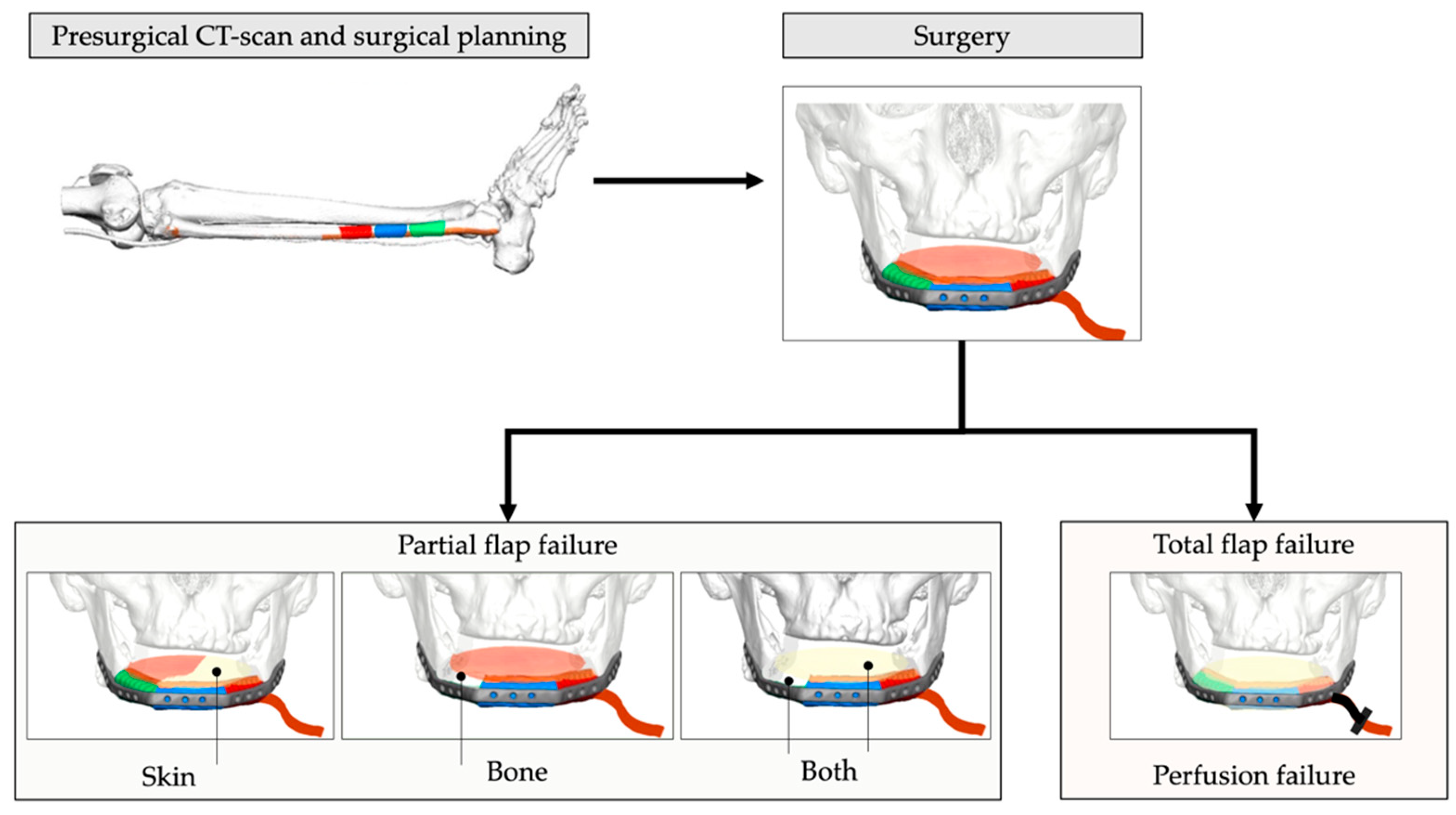
- to estimate the rate of partial flap loss ((sub-)total loss of skin paddle and/or failure of graft segments) and total flap failure over a long time period of 19 years, and to suggest further therapy procedures according to localization and defect type;
- to examine a correlation between age at flap transfer, BMI, ASA-Score, and risk factors in terms of partial and total flap failure; and
- to investigate whether there is a correlation between non-VSP vs. VSP and time of reconstruction (immediate vs. delayed).
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Study Parameters and Evaluator Calibration
2.3. Inclusion and Exclusion Criteria for Study Subjects
2.4. Statistical Analyses
2.5. Ethics Statement/Confirmation of Patients’ Permission
3. Results
4. Discussion
4.1. Rate of PFF and TFF
4.2. Influence of Age at Flap Transfer, BMI, ASA-Score and Risk Factors in Terms of Flap Success in Relation to PFF and TFF
4.3. PFF and TFF in Non-VSP vs. VSP and Reconstruction Methods (Immediate vs. Delayed)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hidalgo, D.A. Fibula free flap: A new method of mandible reconstruction. Plast. Reconstr. Surg. 1989, 84, 71–79. [Google Scholar]
- Zlotolow, I.M.; Huryn, J.M.; Piro, J.D.; Lenchewski, E.; Hidalgo, D.A. Osseointegrated implants and functional prosthetic rehabilitation in microvascular fibula free flap reconstructed mandibles. Am. J. Surg. 1992, 164, 677–681. [Google Scholar] [CrossRef]
- Attia, S.; Wiltfang, J.; Streckbein, P.; Wilbrand, J.-F.; El Khassawna, T.; Mausbach, K.; Howaldt, H.-P.; Schaaf, H. Functional and aesthetic treatment Outcomes after immediate jaw reconstruction using a fibula flap and dental implants. J. Cranio-Maxillofacial Surg. 2019, 47, 786–791. [Google Scholar] [CrossRef]
- Attia, S.; Wiltfang, J.; Pons-Kühnemann, J.; Wilbrand, J.-F.; Streckbein, P.; Kähling, C.; Howaldt, H.-P.; Schaaf, H. Survival of dental implants placed in vascularised fibula free flaps after jaw reconstruction. J. Cranio Maxillofac. Surg. 2018, 46, 1205–1210. [Google Scholar] [CrossRef]
- Attia, S.; Diefenbach, J.; Schmermund, D.; Böttger, S.; Pons-Kühnemann, J.; Scheibelhut, C.; Heiss, C.; Howaldt, H.-P. Donor-Site Morbidity after Fibula Transplantation in Head and Neck Tumor Patients: A Split-Leg Retrospective Study with Focus on Leg Stability and Quality of Life. Cancers 2020, 12, 2217. [Google Scholar] [CrossRef]
- Knitschke, M.; Siu, K.; Bäcker, C.; Attia, S.; Howaldt, H.-P.; Böttger, S. Heterotopic Ossification of the Vascular Pedicle after Maxillofacial Reconstructive Surgery Using Fibular Free Flap: Introducing New Classification and Retrospective Analysis. J. Clin. Med. 2020, 10, 109. [Google Scholar] [CrossRef]
- Kansy, K.; Mueller, A.A.; Mücke, T.; Kopp, J.-B.; Koersgen, F.; Wolff, K.D.; Zeilhofer, H.-F.; Hölzle, F.; Pradel, W.; Schneider, M.; et al. Microsurgical reconstruction of the head and neck—Current concepts of maxillofacial surgery in Europe. J. Cranio-Maxillofac. Surg. 2014, 42, 1610–1613. [Google Scholar] [CrossRef]
- Wolff, K.-D. The supramalleolar flap based on septocutaneous perforators from the peroneal vessels for intraoral soft tissue replacement. Br. J. Plast. Surg. 1993, 46, 151–155. [Google Scholar] [CrossRef]
- Ciocca, L.; Mazzoni, S.; Fantini, M.; Persiani, F.; Marchetti, C.; Scotti, R. CAD/CAM guided secondary mandibular reconstruction of a discontinuity defect after ablative cancer surgery. J. Cranio Maxillofac. Surg. 2012, 40, 511–515. [Google Scholar] [CrossRef]
- Weitz, J.; Bauer, F.; Hapfelmeier, A.; Rohleder, N.; Wolff, K.-D.; Kesting, M. Accuracy of mandibular reconstruction by three-dimensional guided vascularised fibular free flap after segmental mandibulectomy. Br. J. Oral Maxillofac. Surg. 2016, 54, 506–510. [Google Scholar] [CrossRef]
- Cornelius, C.-P.; Smolka, W.; Giessler, G.A.; Wilde, F.; Probst, F.A. Patient-specific reconstruction plates are the missing link in computer-assisted mandibular reconstruction: A showcase for technical description. J. Cranio Maxillofac. Surg. 2015, 43, 624–629. [Google Scholar] [CrossRef]
- Goetze, E.; Kämmerer, P.W.; Al-Nawas, B.; Moergel, M. Integration of Perforator Vessels in CAD/CAM Free Fibula Graft Planning: A Clinical Feasibility Study. J. Maxillofac. Oral Surg. 2019, 19, 61–66. [Google Scholar] [CrossRef]
- Battaglia, S.; Maiolo, V.; Savastio, G.; Zompatori, M.; Contedini, F.; Antoniazzi, E.; Cipriani, R.; Marchetti, C.; Tarsitano, A. Osteomyocutaneous fibular flap harvesting: Computer-assisted planning of perforator vessels using Computed Tomographic Angiography scan and cutting guide. J. Cranio Maxillofac. Surg. 2017, 45, 1681–1686. [Google Scholar] [CrossRef]
- Shroff, S.S.; Nair, S.C.; Shah, A.; Kumar, B. Versatility of Fibula Free Flap in Reconstruction of Facial Defects: A Center Study. J. Maxillofac. Oral Surg. 2016, 16, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Hölzle, F.; Kesting, M.; Hölzle, G.; Watola, A.; Loeffelbein, D.; Ervens, J.; Wolff, K.-D. Clinical outcome and patient satisfaction after mandibular reconstruction with free fibula flaps. Int. J. Oral Maxillofac. Surg. 2007, 36, 802–806. [Google Scholar] [CrossRef]
- Colletti, G.; Autelitano, L.; Rabbiosi, D.; Biglioli, F.; Chiapasco, M.; Mandalà, M.; Allevi, F. Technical refinements in mandibular reconstruction with free fibula flaps: Outcome-oriented retrospective review of 99 cases. Acta Otorhinolaryngol. Ital. 2014, 34, 342–348. [Google Scholar]
- Chang, E.I.; Carlsen, B.T.; Festekjian, J.H.; Da Lio, A.L.; Crisera, C.A. Salvage Rates of Compromised Free Flap Breast Reconstruction After Recurrent Thrombosis. Ann. Plast. Surg. 2013, 71, 68–71. [Google Scholar] [CrossRef]
- Koshima, I.; Fukuda, H.; Yamamoto, H.; Moriguchi, T.; Soeda, S.; Ohta, S. Free anterolateral thigh flaps for reconstruction of head and neck defects. Plast. Reconstr. Surg. 1993, 92, 421–428; discussion 429–430. [Google Scholar]
- Siemionow, M.; Arslan, E. Ischemia/reperfusion injury: A review in relation to free tissue transfers. Microsurgery 2004, 24, 468–475. [Google Scholar] [CrossRef]
- Yang, Q.; Ren, Z.; Chickooree, D.; Wu, H.; Tan, H.; Wang, K.; He, Z.; Gong, C.; Ram, V.; Zhang, S. The effect of early detection of anterolateral thigh free flap crisis on the salvage success rate, based on 10 years of experience and 1072 flaps. Int. J. Oral Maxillofac. Surg. 2014, 43, 1059–1063. [Google Scholar] [CrossRef]
- Verhelst, P.-J.; Dons, F.; Van Bever, P.-J.; Schoenaers, J.; Nanhekhan, L.; Politis, C. Fibula Free Flap in Head and Neck Reconstruction: Identifying Risk Factors for Flap Failure and Analysis of Postoperative Complications in a Low Volume Setting. Craniomaxillofacial Trauma Reconstr. 2019, 12, 183–192. [Google Scholar] [CrossRef]
- Seruya, M.; Fisher, M.; Rodriguez, E.D. Computer-Assisted versus Conventional Free Fibula Flap Technique for Craniofacial Reconstruction. Plast. Reconstr. Surg. 2013, 132, 1219–1228. [Google Scholar] [CrossRef]
- Momoh, A.O.; Yu, P.; Skoracki, R.J.; Liu, S.; Feng, L.; Hanasono, M.M. A Prospective Cohort Study of Fibula Free Flap Donor-Site Morbidity in 157 Consecutive Patients. Plast. Reconstr. Surg. 2011, 128, 714–720. [Google Scholar] [CrossRef]
- Yadav, P.S.; Ahmad, Q.G.; Shankhdhar, V.K.; Nambi, G. Skin paddle vascularity of free fibula flap—A study of 386 cases and a classification based on contribution from axial vessels of the leg. Indian J. Plast. Surg. 2012, 45, 058–061. [Google Scholar] [CrossRef]
- Yu, P.; Chang, E.I.; Hanasono, M.M. Design of a Reliable Skin Paddle for the Fibula Osteocutaneous Flap: Perforator Anatomy Revisited. Plast. Reconstr. Surg. 2011, 128, 440–446. [Google Scholar] [CrossRef]
- Gennaro, P.; Della Monaca, M.; Aboh, I.V.; Priore, P.; Facchini, A.; Valentini, V. “Naked Microvascular Bone Flap” in Oral Reconstruction. Ann. Plast. Surg. 2014, 73, 164–169. [Google Scholar] [CrossRef]
- Gilbert, A. Vascularised transfer of the fibula shaft. Int. J. Microsurg. 1979, 1, 100. [Google Scholar]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Brown, J.S.; Shaw, R.J. Reconstruction of the maxilla and midface: Introducing a new classification. Lancet Oncol. 2010, 11, 1001–1008. [Google Scholar] [CrossRef]
- Brown, J.S.; Barry, C.; Ho, M.; Shaw, R. A new classification for mandibular defects after oncological resection. Lancet Oncol. 2016, 17, 23–30. [Google Scholar] [CrossRef]
- Freeman, G.H.; Halton, J.H. Note on an exact treatment of contingency, goodness of fit and other problems of significance. Biometrika 1951, 38, 141–149. [Google Scholar]
- Gluckman, J.L.; McDonough, J.; Donegan, J.O. The role of the free jejunal graft in reconstruction of the pharynx and cervical esophagus. Head Neck Surg. 1982, 4, 360–369. [Google Scholar] [CrossRef]
- Bui, D.T.; Cordeiro, P.G.; Hu, Q.-Y.; Disa, J.J.; Pusic, A.; Mehrara, B.J. Free Flap Reexploration: Indications, Treatment, and Outcomes in 1193 Free Flaps. Plast. Reconstr. Surg. 2007, 119, 2092–2100. [Google Scholar] [CrossRef]
- Chaine, A.; Pitak-Arnnop, P.; Dhanuthai, K.; Ruhin-Poncet, B.; Bertrand, J.-C.; Bertolus, C. A treatment algorithm for managing giant mandibular ameloblastoma: 5-year experiences in a Paris university hospital. Eur. J. Surg. Oncol. (EJSO) 2009, 35, 999–1005. [Google Scholar] [CrossRef] [Green Version]
- Gallegos-Hernández, J.F.; Martínez-Miramón, A.; Reyes-Vivanco, A. Seguimiento a largo plazo del colgajo libre de peroné en la reconstrucción mandibular. Cirugía y Cirujanos 2019, 87, 267–271. [Google Scholar] [CrossRef]
- López-Arcas, J.M.; Arias, J.; del Castillo, J.L.; Burgueño, M.; Navarro, I.; Moran, M.J.; Chamorro, M.; Martorell, V. The Fibula Osteomyocutaneous Flap for Mandible Reconstruction: A 15-Year Experience. J. Oral Maxillofac. Surg. 2010, 68, 2377–2384. [Google Scholar] [CrossRef]
- Mücke, T.; Ritschl, L.M.; Roth, M.; Güll, F.D.; Rau, A.; Grill, S.; Kesting, M.R.; Wolff, K.-D.; Loeffelbein, D.J. Predictors of free flap loss in the head and neck region: A four-year retrospective study with 451 microvascular transplants at a single centre. J. Cranio Maxillofac. Surg. 2016, 44, 1292–1298. [Google Scholar] [CrossRef]
- Las, D.E.; de Jong, T.; Zuidam, J.M.; Verweij, N.M.; Hovius, S.E.; Mureau, M.A. Identification of independent risk factors for flap failure: A retrospective analysis of 1530 free flaps for breast, head and neck and extremity reconstruction. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 894–906. [Google Scholar] [CrossRef]
- Suh, J.D.; Sercarz, J.A.; Abemayor, E.; Calcaterra, T.C.; Rawnsley, J.D.; Alam, D.; Blackwell, K.E. Analysis of Outcome and Complications in 400 Cases of Microvascular Head and Neck Reconstruction. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 962–966. [Google Scholar] [CrossRef] [Green Version]
- Tan, N.C.; Lin, P.-Y.; Chiang, Y.-C.; Chew, K.-Y.; Chen, C.-C.; Fujiwara, T.; Kuo, Y.-R. Influence of neck dissection and preoperative irradiation on microvascular head and neck reconstruction-Analysis of 853 cases. Microsurgery 2014, 34, 602–607. [Google Scholar] [CrossRef]
- Bourget, A.; Chang, J.T.C.; Wu, D.B.-S.; Chang, C.J.; Wei, F.C. Free Flap Reconstruction in the Head and Neck Region following Radiotherapy: A Cohort Study Identifying Negative Outcome Predictors. Plast. Reconstr. Surg. 2011, 127, 1901–1908. [Google Scholar] [CrossRef]
- Deek, N.F.A.L.; Wei, F.-C. Computer-Assisted Surgery for Segmental Mandibular Reconstruction with the Osteoseptocutaneous Fibula Flap. Plast. Reconstr. Surg. 2016, 137, 963–970. [Google Scholar] [CrossRef]
- He, Y.; Zhang, Z.Y.; Zhu, H.G.; Sader, R.; He, J.; Kovacs, A.F. Free Fibula Osteocutaneous Flap for Primary Reconstruction of T3-T4 Gingival Carcinoma. J. Craniofacial Surg. 2010, 21, 301–305. [Google Scholar] [CrossRef]
- Cvek, J.; Kubes, J.; Skacelikova, E.; Otahal, B.; Kominek, P.; Halamka, M.; Feltl, D. Hyperfractionated accelerated radiotherapy with concomitant integrated boost of 70–75 Gy in 5 weeks for advanced head and neck cancer. Strahlenther. Onkol. 2012, 188, 666–670. [Google Scholar] [CrossRef]
- Wygoda, A.; Rutkowski, T.; Hutnik, M.; Składowski, K.; Goleń, M.; Pilecki, B. Acute mucosal reactions in patients with head and neck cancer. Strahlenther. Onkol. 2013, 189, 547–551. [Google Scholar] [CrossRef]
- Moura, J.F.B.; Mota, J.M.S.C.; Leite, C.A.V.; Wong, D.V.T.; Bezerra, N.P.; Brito, G.A.D.C.; Lima, V.; Cunha, F.Q.; Ribeiro, R.A. A novel model of megavoltage radiation-induced oral mucositis in hamsters: Role of inflammatory cytokines and nitric oxide. Int. J. Radiat. Biol. 2015, 91, 500–509. [Google Scholar] [CrossRef]
- Logan, R.M.; Gibson, R.J.; Sonis, S.T.; Keefe, D.M. Nuclear factor-κB (NF-κB) and cyclooxygenase-2 (COX-2) expression in the oral mucosa following cancer chemotherapy. Oral Oncol. 2007, 43, 395–401. [Google Scholar] [CrossRef]
- Fang, H.; Liu, F.; Sun, C.; Pang, P. Impact of wound closure on fibular donor-site morbidity: A meta-analysis. BMC Surg. 2019, 19, 1–6. [Google Scholar] [CrossRef]
- Ling, X.F.; Peng, X. What Is the Price to Pay for a Free Fibula Flap? A Systematic Review of Donor-Site Morbidity following Free Fibula Flap Surgery. Plast. Reconstr. Surg. 2012, 129, 657–674. [Google Scholar] [CrossRef]
- Bach, C.A.; Guilleré, L.; Yildiz, S.; Wagner, I.; Darmon, S.; Chabolle, F. Comparison of negative pressure wound therapy and conventional dressing methods for fibula free flap donor site management in patients with head and neck cancer. Head Neck 2015, 38, 696–699. [Google Scholar] [CrossRef]
- Schusterman, M.A.; Reece, G.P.; Miller, M.J.; Harris, S. The osteocutaneous free fibula flap: Is the skin paddle reliable? Plast. Reconstr. Surg. 1992, 90, 787–794; discussion 794–798. [Google Scholar]
- Torroni, A.; Gennaro, P.; Aboh, I.V.; Longo, G.; Valentini, V.; Iannetti, G. Microvascular Reconstruction of the Mandible in Irradiated Patients. J. Craniofacial Surg. 2007, 18, 1359–1369. [Google Scholar] [CrossRef]
- Thome, J. Das mikrovaskuläre Fibulatransplantat in der Mund-, Kiefer—Und Gesichtschirurgie—Eine Literaturübersicht—Dissertation. University Cologne, Cologne, Germany, 2008. [Google Scholar]
- Jones, N.F.; Monstrey, S.; Gambier, B.A. Reliability of the Fibular Osteocutaneous Flap for Mandibular Reconstruction: Anatomical and Surgical Confirmation. Plast. Reconstr. Surg. 1996, 97, 707–716. [Google Scholar] [CrossRef]
- Wong, C.-H.; Tan, B.-K.; Wei, F.-C.; Song, C. Use of the Soleus Musculocutaneous Perforator for Skin Paddle Salvage of the Fibula Osteoseptocutaneous Flap: Anatomical Study and Clinical Confirmation. Plast. Reconstr. Surg. 2007, 120, 1576–1584. [Google Scholar] [CrossRef]
- Winters, H.A.H.; de Jongh, G.J. Reliability of the Proximal Skin Paddle of the Osteocutaneous Free Fibula Flap: A Prospective Clinical Study. Plast. Reconstr. Surg. 1999, 103, 846–849. [Google Scholar] [CrossRef]
- Millican, P.; Poole, M. Peripheral neovascularisation of muscle and musculocutaneous flaps. Br. J. Plast. Surg. 1985, 38, 369–374. [Google Scholar] [CrossRef]
- Khoo, C.; Bailey, B. The behaviour of free muscle and musculocutaneous flaps after early loss of axial blood supply. Br. J. Plast. Surg. 1982, 35, 43–46. [Google Scholar] [CrossRef]
- Kumar, K.; Jaffe, W.; London, N.J.M.; Varma, S.K. Free Flap Neovascularization: Myth or Reality? J. Reconstr. Microsurg. 2004, 21, 31–34. [Google Scholar] [CrossRef]
- Mücke, T.; Wolff, K.-D.; Rau, A.; Kehl, V.; Mitchell, D.A.; Steiner, T. Autonomization of free flaps in the oral cavity: A prospective clinical study. Microsurgery 2012, 32, 201–206. [Google Scholar] [CrossRef]
- Goldwaser, B.R.; Chuang, S.-K.; Kaban, L.B.; August, M. Risk Factor Assessment for the Development of Osteoradionecrosis. J. Oral Maxillofac. Surg. 2007, 65, 2311–2316. [Google Scholar] [CrossRef]
- Celik, N.; Wei, F.-C.; Chen, H.-C.; Cheng, M.-H.; Huang, W.-C.; Tsai, F.-C.; Chen, Y.-C. Osteoradionecrosis of the Mandible after Oromandibular Cancer Surgery. Plast. Reconstr. Surg. 2002, 109, 1875–1881. [Google Scholar] [CrossRef]
- Aarup-Kristensen, S.; Hansen, C.R.; Forner, L.; Brink, C.; Eriksen, J.G.; Johansen, J. Osteoradionecrosis of the mandible after radiotherapy for head and neck cancer: Risk factors and dose-volume correlations. Acta Oncol. 2019, 58, 1373–1377. [Google Scholar] [CrossRef]
- Cummins, D.M.; Kim, B.; Kaleem, A.; Zaid, W. Pedicle Orientation in Free-Flap Microvascular Maxillofacial Reconstruction. J. Oral Maxillofac. Surg. 2017, 75, 875.e1–875.e4. [Google Scholar] [CrossRef]
- Zhang, C.; Sun, J.; Zhu, H.; Xu, L.; Ji, T.; He, Y.; Yang, W.; Hu, Y.; Yang, X.; Zhang, Z. Microsurgical free flap reconstructions of the head and neck region: Shanghai experience of 34 years and 4640 flaps. Int. J. Oral Maxillofac. Surg. 2015, 44, 675–684. [Google Scholar] [CrossRef]
- Chiu, Y.-H.; Chang, D.-H.; Perng, C.-K. Vascular Complications and Free Flap Salvage in Head and Neck Reconstructive Surgery. Ann. Plast. Surg. 2017, 78, S83–S88. [Google Scholar] [CrossRef]
- Costa, H.; Zenha, H.; Sequeira, H.; Coelho, G.; Gomes, N.; Pinto, C.; Martins, J.; Santos, D.; Andresen, C. Microsurgical reconstruction of the maxilla: Algorithm and concepts. J. Plast. Reconstr. Aesthetic Surg. 2015, 68, e89–e104. [Google Scholar] [CrossRef]
- Cao, Y.; Yu, C.; Liu, W.; Miao, C.; Han, B.; Yang, J.; Li, L.; Li, C. Obturators versus flaps after maxillary oncological ablation: A systematic review and best evidence synthesis. Oral Oncol. 2018, 82, 152–161. [Google Scholar] [CrossRef]
- Colmenero, C.; Martorell, V.; Colmenero, B.; Sierra, I. Temporalis myofascial flap for maxillofacial reconstruction. J. Oral Maxillofac. Surg. 1991, 49, 1067–1073. [Google Scholar] [CrossRef]
- Ariyan, S. The Pectoralis Major Myocutaneous Flap A Versatile Flap for Reconstruction in the Head and Neck. Plast. Reconstr. Surg. 1979, 63, 73–81. [Google Scholar] [CrossRef]
- Ariyan, S. Pectoralis Major, Sternomastoid, and Other Musculocutaneous Flaps for Head and Neck Reconstruction. Clin. Plast. Surg. 1980, 7, 89–109. [Google Scholar] [CrossRef]
- Bakamjian, V.; Poole, M. Maxillo-facial and palatal reconstructions with the deltopectoral flap. Br. J. Plast. Surg. 1977, 30, 17–37. [Google Scholar] [CrossRef]
- de Pablo, A.; Chen, Y.-T.; Chen, J.-K.; Tsao, C.-K. Trismus surgical release and free flap reconstruction after radiation therapy in oral and oropharyngeal squamous cell carcinoma. J. Surg. Oncol. 2018, 117, 142–149. [Google Scholar] [CrossRef]
- Chang, T.S.; Wang, W.; Hsu, C.Y. The free forearm flap--a report of 25 cases. Ann. Acad. Med. Singap. 1982, 11, 236–240. [Google Scholar]
- Ludolph, I.; Lehnhardt, M.; Arkudas, A.; Kneser, U.; Pierer, G.; Harder, Y.; Horch, R.E. Plastisch rekonstruktive Mikrochirurgie beim alten Patienten. Handchir. · Mikrochir. · Plast. Chir. 2017, 50, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Wolfer, S.; Wohlrath, R.; Kunzler, A.; Foos, T.; Ernst, C.; Schultze-Mosgau, S. Scapular free flap as a good choice for mandibular reconstruction: 119 out of 280 cases after resection of oral squamous cell carcinoma in a single institution. Br. J. Oral Maxillofac. Surg. 2020, 58, 451–457. [Google Scholar] [CrossRef]
- Hwang, K.; Lee, J.P.; Yoo, S.Y.; Kim, H. Relationships of comorbidities and old age with postoperative complications of head and neck free flaps: A review. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 1627–1635. [Google Scholar] [CrossRef]
- Sierakowski, A.; Nawar, A.; Parker, M.; Mathur, B. Free flap surgery in the elderly: Experience with 110 cases aged ≥70 years. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 189–195. [Google Scholar] [CrossRef]
- Kesting, M.R.; Hölzle, F.; Wolff, K.-D.; Wagenpfeil, S.; Hasler, R.J.; Wales, C.J.; Steinstraesser, L.; Rohleder, N.H. Use of microvascular flap technique in older adults with head and neck cancer: A persisting dilemma in reconstructive surgery? J. Am. Geriatr. Soc. 2011, 59, 398–405. [Google Scholar] [CrossRef]
- Grill, F.D.; Wasmaier, M.; Mücke, T.; Ritschl, L.M.; Wolff, K.-D.; Schneider, G.; Loeffelbein, D.J.; Kadera, V. Identifying perioperative volume-related risk factors in head and neck surgeries with free flap reconstructions—An investigation with focus on the influence of red blood cell concentrates and noradrenaline use. J. Cranio Maxillofac. Surg. 2020, 48, 67–74. [Google Scholar] [CrossRef]
- Clark, J.R.; McCluskey, S.A.; Hall, F.; Lipa, J.; Neligan, P.; Brown, D.; Irish, J.; Gullane, P.; Gilbert, R. Predictors of morbidity following free flap reconstruction for cancer of the head and neck. Head Neck 2007, 29, 1090–1101. [Google Scholar] [CrossRef]
- Loeffelbein, D.; Ritschl, L.; Güll, F.; Roth, M.; Wolff, K.-D.; Mücke, T. Influence of possible predictor variables on the outcome of primary oral squamous cell carcinoma: A retrospective study of 392 consecutive cases at a single centre. Int. J. Oral Maxillofac. Surg. 2017, 46, 413–421. [Google Scholar] [CrossRef]
- Chen, A.M.; Chen, L.M.; Vaughan, A.; Farwell, D.G.; Luu, Q.; Purdy, J.A.; Vijayakumar, S. Head and Neck Cancer Among Lifelong Never-Smokers and Ever-Smokers. Am. J. Clin. Oncol. 2011, 34, 270–275. [Google Scholar] [CrossRef]
- Fortin, A.; Wang, C.S.; Vigneault, É. Influence of Smoking and Alcohol Drinking Behaviors on Treatment Outcomes of Patients With Squamous Cell Carcinomas of the Head and Neck. Int. J. Radiat. Oncol. 2009, 74, 1062–1069. [Google Scholar] [CrossRef]
- Van Imhoff, L.C.; Kranenburg, G.G.; Macco, S.; Nijman, N.L.; van Overbeeke, E.J.; Wegner, I.; Grolman, W.; Pothen, A.J. Prognostic value of continued smoking on survival and recurrence rates in patients with head and neck cancer: A systematic review. Head Neck 2015, 38, E2214–E2220. [Google Scholar] [CrossRef]
- Crippen, M.M.; Brady, J.S.; Mozeika, A.M.; Eloy, J.A.; Baredes, S.; Park, R.C.W. Impact of Body Mass Index on Operative Outcomes in Head and Neck Free Flap Surgery. Otolaryngol. Neck Surg. 2018, 159, 817–823. [Google Scholar] [CrossRef]
- Gama, R.R.; Song, Y.; Zhang, Q.; Brown, M.C.; Wang, J.; Habbous, S.; Tong, L.; Huang, S.H.; O’Sullivan, B.; Waldron, J.; et al. Body mass index and prognosis in patients with head and neck cancer. Head Neck 2017, 39, 1226–1233. [Google Scholar] [CrossRef]
- de La Garza, G.; Militsakh, O.N.; Panwar, A.; Galloway, T.L.; Jorgensen, J.B.; Ledgerwood, L.G.; Kaiser, K.; Bs, C.K.; Shnayder, Y.; Neumann, C.A.; et al. Obesity and perioperative complications in head and neck free tissue reconstruction. Head Neck 2016, 38, E1188–E1191. [Google Scholar] [CrossRef]
- Khan, M.N.; Russo, J.; Spivack, J.; Pool, C.; Likhterov, I.; Teng, M.; Genden, E.M.; Miles, B.A. Association of Body Mass Index With Infectious Complications in Free Tissue Transfer for Head and Neck Reconstructive Surgery. JAMA Otolaryngol. Neck Surg. 2017, 143, 574–579. [Google Scholar] [CrossRef]
- Thai, L.; McCarn, K.; Stott, W.; Watts, T.; Wax, M.K.; Andersen, P.E.; Gross, N.D. Venous thromboembolism in patients with head and neck cancer after surgery. Head Neck 2012, 35, 4–9. [Google Scholar] [CrossRef]
- Eskander, A.; Kang, S.; Tweel, B.; Sitapara, J.; Old, M.; Ozer, E.; Agrawal, A.; Carrau, R.; Rocco, J.W.; Teknos, T.N. Predictors of Complications in Patients Receiving Head and Neck Free Flap Reconstructive Procedures. Otolaryngol. Neck Surg. 2018, 158, 839–847. [Google Scholar] [CrossRef]
- Cannady, S.B.; Hatten, K.M.; Bur, A.M.; Brant, J.; Fischer, J.P.; Newman, J.G.; Chalian, A.A. Use of free tissue transfer in head and neck cancer surgery and risk of overall and serious complication(s): An American College of Surgeons-National Surgical Quality Improvement Project analysis of free tissue transfer to the head and neck. Head Neck 2017, 39, 702–707. [Google Scholar] [CrossRef]
- Offodile, A.C.; Aherrera, A.; Wenger, J.; Rajab, T.K.; Guo, L. Impact of increasing operative time on the incidence of early failure and complications following free tissue transfer? A risk factor analysis of 2,008 patients from the ACS-NSQIP database. Microsurgery 2015, 37, 12–20. [Google Scholar] [CrossRef]
- Tang, N.S.; Ahmadi, I.; Ramakrishnan, A. Virtual surgical planning in fibula free flap head and neck reconstruction: A systematic review and meta-analysis. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 1465–1477. [Google Scholar] [CrossRef]
- Rendenbach, C.; Steffen, C.; Hanken, H.; Schluermann, K.; Henningsen, A.; Beck-Broichsitter, B.; Kreutzer, K.; Heiland, M.; Precht, C. Complication rates and clinical outcomes of osseous free flaps: A retrospective comparison of CAD/CAM versus conventional fixation in 128 patients. Int. J. Oral Maxillofac. Surg. 2019, 48, 1156–1162. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 36 | PFF N = 16 (44.4%) | TFF N = 20 (56.6%) | p-Value |
|---|---|---|---|
| Age (years), SD | 59.9 ± 14.4 | 62.5 ± 9.5 | p = 0.520 |
| Follow-up (months), SD | 48 ± 42.9 | 31.5 ± 31.6 | p = 0.193 |
| Type of flap loss | |||
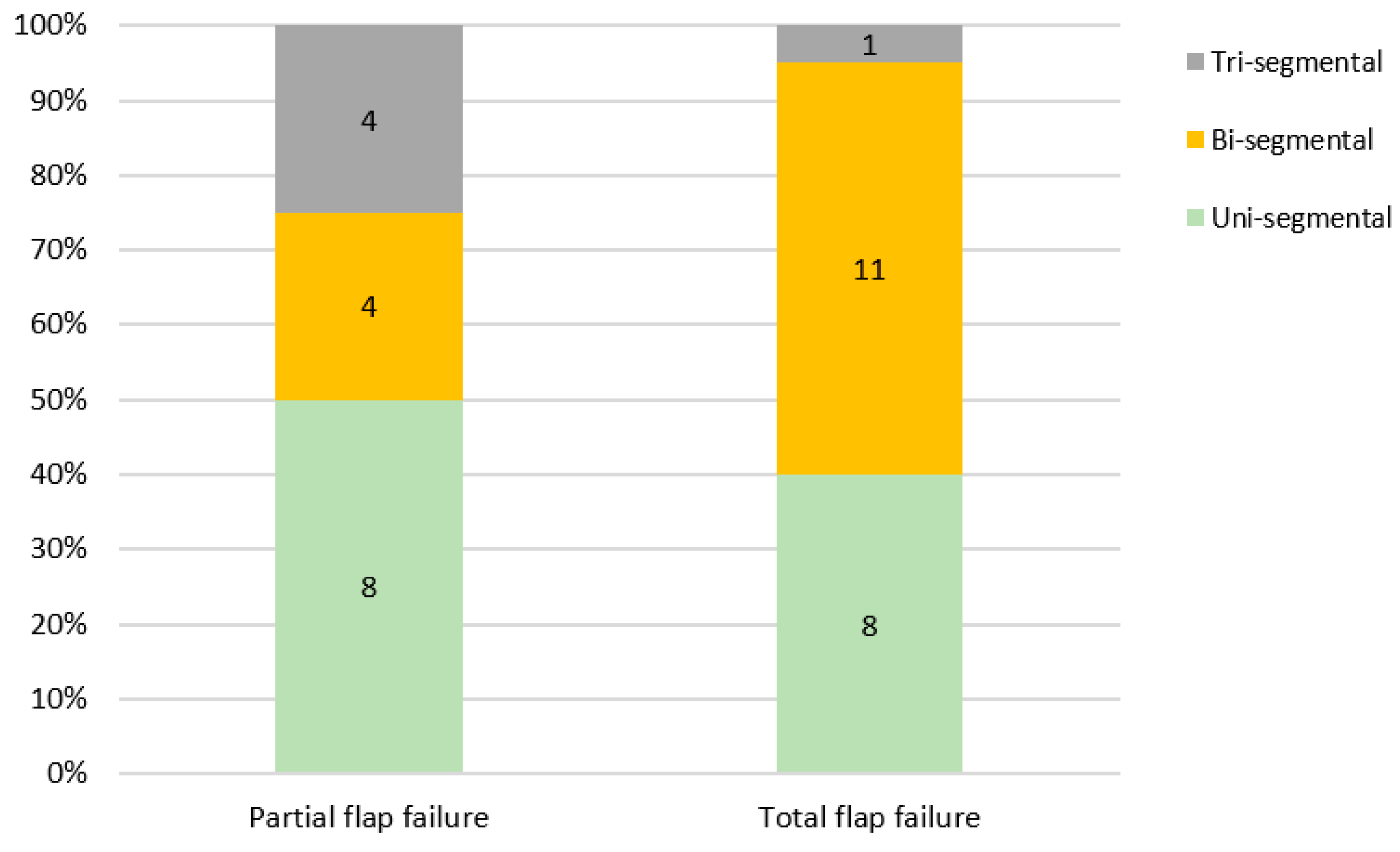
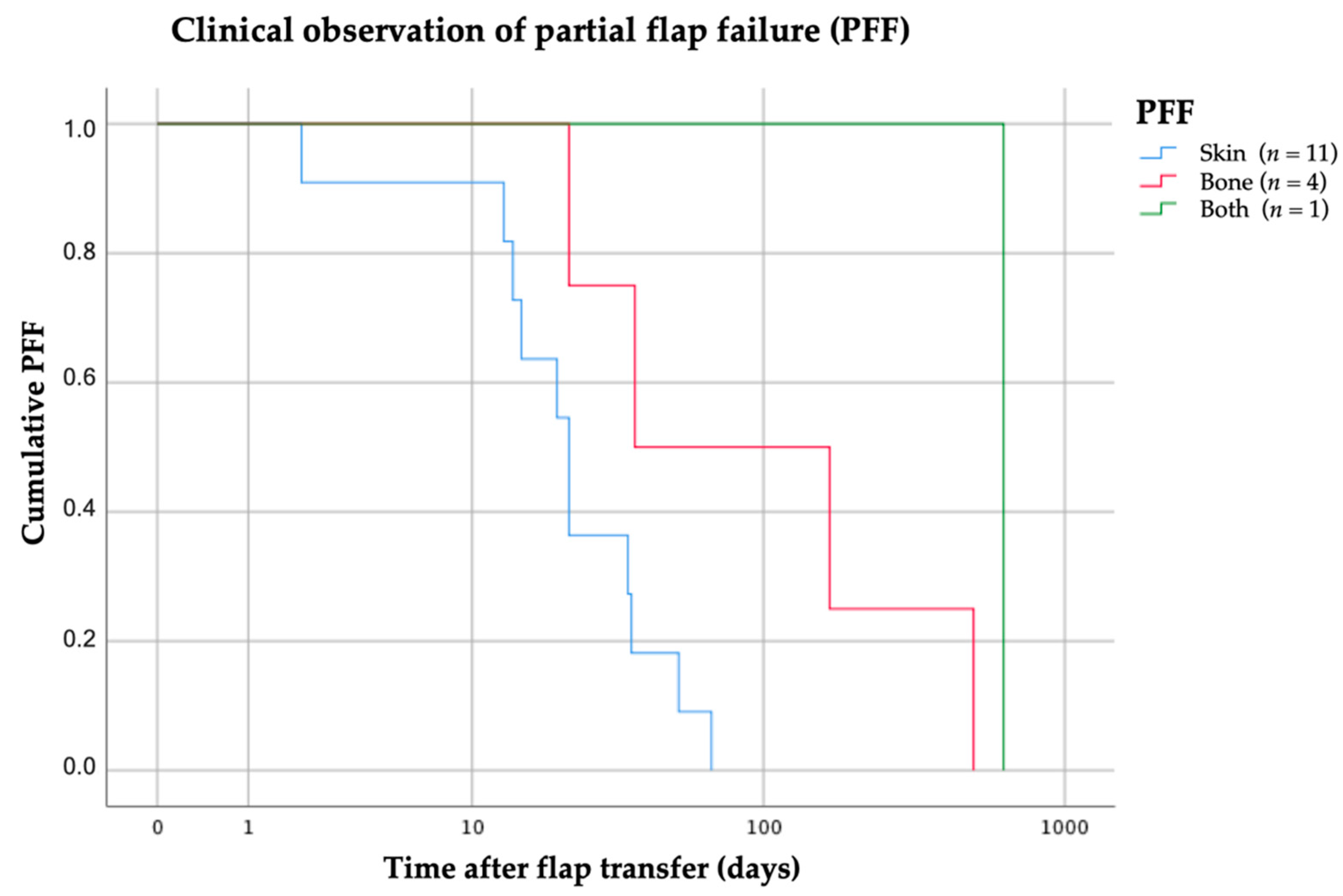
| PFF, Skin paddle | 11 | ||
| PFF, Bone segment | 4 | ||
| PFF, Both | 1 | ||
| Total flap loss (TFF) | 20 | ||
| Sex | |||
| Female | 5 | 6 | p = 0.609 |
| Male | 11 | 14 | |
| Diagnosis | |||
| Benign tumor Malignant tumor MRONJ ORN | 1 15 | 15 2 3 | |
| Reconstruction | |||
| Immediate | 14 | 17 | p = 0.610 |
| Delayed | 2 | 3 | |
| Reconstruction | |||
| Non-VSP | 10 | 10 | p = 0.341 |
| VSP | 6 | 10 | |
| Neck dissection | |||
| Unilateral | 11 | 13 | n.s. |
| Bilateral | 3 | 3 | |
| None | 2 | 4 | |
| Tracheostomy | |||
| None | 6 | 8 | n.s. |
| Primary | 9 | 11 | |
| Secondary | 1 | 1 | |
| Irradiation | |||
| Preoperative | 1 | 3 | n.s. |
| Postoperative | 8 | 4 | |
| None | 7 | 13 | |
| Risk factors | |||
| Alcohol abuse | 5 | 9 | p = 0.348 |
| Tobacco abuse | 9 | 13 | p = 0.546 |
| Operating time (min) | 546.2 ± 94.9 | 524.4 ± 97.2 | p = 0.504 |
| Duration ICU (days) | 2 ± 1.3 | 2.1 ± 1.7 | p = 0.847 |
| Hospitalization (days) | 22.6 ± 9.7 | 33.8 ± 18.8 | p = 0.038 |
| BMI ≤18 18 ≤ 25 25 ≤ 30 30 ≤ 35 >35 | 9 3 4 | 1 9 7 2 1 | |
| ASA-Score | |||
| ASA 2 | 10 | 7 | |
| ASA 3 | 6 | 12 | |
| ASA 4 | 1 |
| Type of Defect | PFF Skin (n = 11) | PFF Bone (n = 4) | PFF Both (n = 1) | TFF (n = 20) |
|---|---|---|---|---|
| Maxilla | ||||
| II | 1 | - | - | 2 |
| III | 1 | - | - | 1 |
| Mandible | ||||
| I | 4 | - | 1 | 7 |
| Ic | - | - | - | 1 |
| II | 2 | 2 | - | 6 |
| IIc | - | 1 | - | - |
| III | 3 | 1 | - | 2 |
| IV | - | - | - | 1 |
| N = 20 | Maxilla (n = 3) | Mandible (n = 17) | Overall (n = 20) | p |
|---|---|---|---|---|
| Age (years), SD | 73.3 ± 1.8 | 60.6 ± 8.9 | 62.5 ± 9.5 | p = 0.001 ^ |
| Follow-up (months), SD | 10.3 ± 9.7 | 35.2 ± 32.8 | 31 ± 31.6 | |
| The earliest sign of flap dysfunction (days) | 3. 3 ± 3.5 (Median 3) | 14.4 ± 11.1 (Median 10) | 12 ± 10.9 (Median 8.5) | p = 0.007 ^ |
| Surgical validation and avital flap treatment procedure (days) | 54 ± 60.1 (Median 36) | 92.1 ± 132.0 (Median 21) | 86.5 ± 123.6 (Median 22.5) | p = 0.449 ^ |
| Anastomosis revisions | 2 | 6 | 8 | |
| Arterial thrombosis ‡ | 2 | 2 | 4 | |
| Venous thrombosis ‡ | - | 4 | 4 | n.s |
| Unknown | 1 | 11 | 12 | |
| Explantation of bone graft | 2 | 16 | 18 | |
| Osteosynthesis (PSI) removal | 1 | 11 | 12 | |
| Re-osteosynthesis | - | 3 | 3 | |
| Second flap | 1 | 8 | 9 | |
| Temporalis muscle flap | 1 | 1 | 2 | |
| Deltopectoral flap | - | 1 | 1 | |
| Pectoralis major flap | - | 2 | 2 | |
| RFF | - | 1 | 1 | |
| FFF | - | 2 | 2 | |
| Hip graft (non-DCIA) | - | 1 | 1 |
| Authors | Investigation Period | n | Total Flap Failure | Partial Flap Failure |
|---|---|---|---|---|
| This study | 2002–2020 | 180 | 11.1% | 8.9% |
| Colletti et al. [16] | 2002–2010 | 99 | 7% | 3% |
| Gallegos-Hernandez et al. [35] | 1996–2006 | 87 | 16.1% | - |
| Götze et al. [12] | 2013–2015 | 24 | 12.5% | 8.3% |
| Lopez-Arcas et al. [36] | 1992–2006 | 117 | - | 8.5% |
| Momoh et al. [23] | 2005–2009 | 157 | 1% | 14% |
| Mücke et al. [37] | 2009–2013 | 76 | 9.2% | - |
| Seruya et al. [22] | 2003–2012 | 68 | 4.41% | 11.76% |
| Shroff et al. [14] | 2009–2013 | 30 | 6.66% | - |
| Verhelst et al. [21] | 1996–2016 | 129 | 12.4% | 7.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knitschke, M.; Sonnabend, S.; Bäcker, C.; Schmermund, D.; Böttger, S.; Howaldt, H.-P.; Attia, S. Partial and Total Flap Failure after Fibula Free Flap in Head and Neck Reconstructive Surgery: Retrospective Analysis of 180 Flaps over 19 Years. Cancers 2021, 13, 865. https://doi.org/10.3390/cancers13040865
Knitschke M, Sonnabend S, Bäcker C, Schmermund D, Böttger S, Howaldt H-P, Attia S. Partial and Total Flap Failure after Fibula Free Flap in Head and Neck Reconstructive Surgery: Retrospective Analysis of 180 Flaps over 19 Years. Cancers. 2021; 13(4):865. https://doi.org/10.3390/cancers13040865
Chicago/Turabian StyleKnitschke, Michael, Sophia Sonnabend, Christina Bäcker, Daniel Schmermund, Sebastian Böttger, Hans-Peter Howaldt, and Sameh Attia. 2021. "Partial and Total Flap Failure after Fibula Free Flap in Head and Neck Reconstructive Surgery: Retrospective Analysis of 180 Flaps over 19 Years" Cancers 13, no. 4: 865. https://doi.org/10.3390/cancers13040865