Magnetic Resonance Imaging Based Radiomic Models of Prostate Cancer: A Narrative Review

 ,
,  , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Multiparametric MRI (mpMRI) of Prostate Cancer
3. Radiomics Pipeline for Predicting Tumor Grade
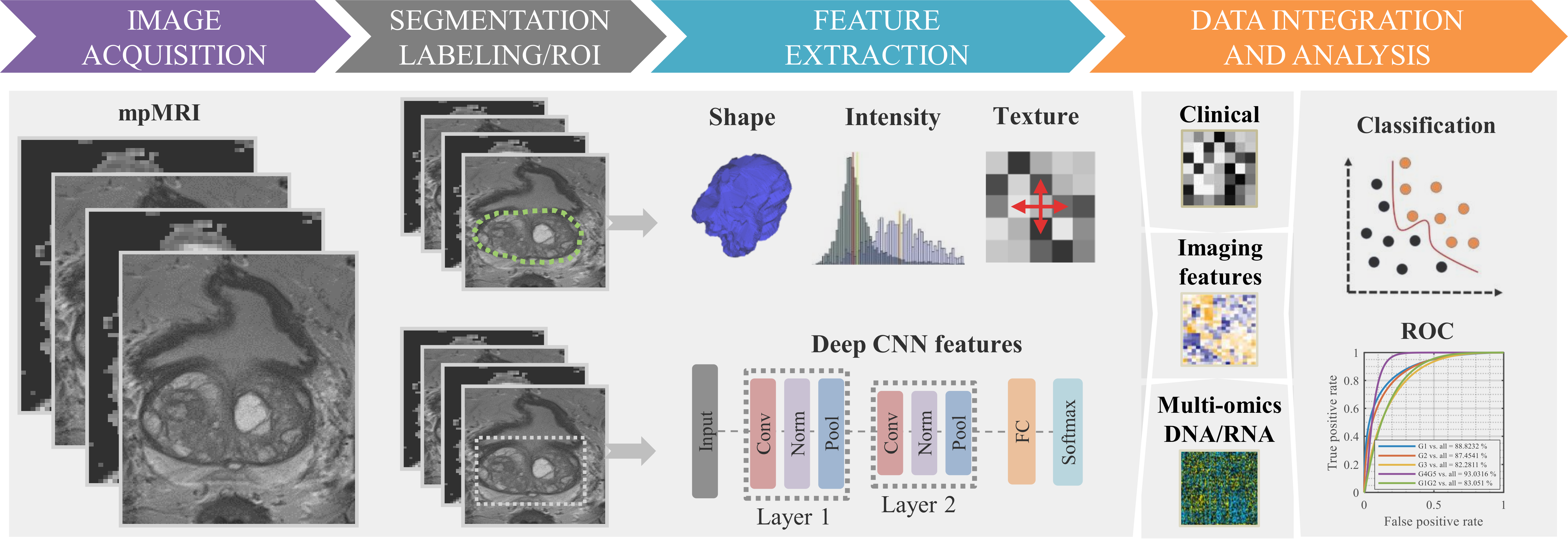
3.1. Basic Flowchart
3.2. Image Acquisition
3.3. Image Quality Assessment and Standardization
3.4. PCa Segmentation
3.5. Image Feature Extraction
3.6. Feature Analysis and Prediction Model Construction
4. Prostate Cancer Radiogenomics
5. Barriers and Strategies for Clinical Translation
6. Next Steps Involving AI with Radiomics
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Rawla, P. Epidemiology of prostate cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzmaurice, C.; Akinyemiju, T.F.; Lami, F.H.A.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the global burden of disease study. JAMA Oncol. 2018. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Zapatero, A.; Guerrero, A.; Maldonado, X.; Alvarez, A.; Segundo, C.G.S.; Rodríguez, M.A.C.; Macias, V.; Olive, A.P.; Casas, F.; Boladeras, A.; et al. High-dose radiotherapy with short-term or long-term androgen deprivation in localised prostate cancer (DART01/05 GICOR): A randomised, controlled, phase 3 trial. Lancet Oncol. 2015, 16, 320–327. [Google Scholar] [CrossRef]
- Epstein, J.I. Prostate cancer grading: A decade after the 2005 modified system. Mod. Pathol. 2018, 31, S47–S63. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. Grading committee the 2014 international society of urological pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Djavan, B.; Kadesky, K.; Klopukh, B.; Marberger, M.; Roehrborn, C.G. Gleason scores from prostate biopsies obtained with 18-Gauge biopsy needles poorly predict gleason scores of radical prostatectomy specimens. EUR 1998, 33, 261–270. [Google Scholar] [CrossRef]
- Pinthus, J.H.; Witkos, M.; Fleshner, N.E.; Sweet, J.; Evans, A.; Jewett, M.A.; Krahn, M.; Alibhai, S.; Trachtenberg, J. Prostate cancers scored as gleason 6 on prostate biopsy are frequently gleason 7 tumors at radical prostatectomy: Implication on outcome. J. Urol. 2006, 176, 979–984. [Google Scholar] [CrossRef]
- Allsbrook, W.C.; Mangold, K.A.; Johnson, M.H.; Lane, R.B.; Lane, C.G.; Amin, M.B.; Bostwick, D.G.; Humphrey, P.A.; Jones, E.C.; Reuter, V.E.; et al. Interobserver reproducibility of gleason grading of prostatic carcinoma: Urologic pathologists. Hum. Pathol. 2001, 32, 74–80. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, N.; Loblaw, D.A.; Mamedov, A.; Sugar, L.; Holden, L. Prostate cancer pathology audits: Is central pathology review still warranted? Can. J. Urol. 2012, 19, 6256–6260. [Google Scholar]
- Braun, K.; Ahallal, Y.; Sjoberg, D.D.; Ghoneim, T.; Dominguez Esteban, M.; Mulhall, J.; Vickers, A.; Eastham, J.; Scardino, P.T.; Touijer, K.A. Effect of repeated prostate biopsies on erectile function in men on active surveillance for prostate cancer. J. Urol. 2014, 191, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Ehdaie, B.; Vertosick, E.; Spaliviero, M.; Giallo-Uvino, A.; Taur, Y.; O’Sullivan, M.; Livingston, J.; Sogani, P.; Eastham, J.; Scardino, P.; et al. The impact of repeat biopsies on infectious complications in men with prostate cancer on active surveillance. J. Urol. 2014, 191, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Vellekoop, A.; Ahmed, H.U.; Catto, J.; Emberton, M.; Nam, R.; Rosario, D.J.; Scattoni, V.; Lotan, Y. Systematic review of complications of prostate biopsy. Eur. Urol. 2013, 64, 876–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, K.; Landis, P.; McNeil, B.K.; Pavlovich, C.P. Serial prostate biopsies are associated with an increased risk of erectile dysfunction in men with prostate cancer on active surveillance. J. Urol. 2009, 182, 2664–2669. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.M.; Robertson, N.L.; Arsanious, N.; Middleton, T.; Villers, A.; Klotz, L.; Taneja, S.S.; Emberton, M. Image-guided prostate biopsy using magnetic resonance imaging-derived targets: A systematic review. Eur. Urol. 2013, 63, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/ultrasound fusion–guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 2015, 313, 390–397. [Google Scholar] [CrossRef]
- Sun, Y.; Reynolds, H.M.; Parameswaran, B.; Wraith, D.; Finnegan, M.E.; Williams, S.; Haworth, A. Multiparametric MRI and radiomics in prostate cancer: A review. Australas. Phys. Eng. Sci. Med. 2019, 42, 3–25. [Google Scholar] [CrossRef]
- Klotz, L.; Loblaw, A.; Sugar, L.; Moussa, M.; Berman, D.M.; Van der Kwast, T.; Vesprini, D.; Milot, L.; Kebabdjian, M.; Fleshner, N.; et al. Active surveillance magnetic resonance imaging study (ASIST): Results of a randomized multicenter prospective trial. Eur. Urol. 2019, 75, 300–309. [Google Scholar] [CrossRef]
- Simmons, L.A.M.; Kanthabalan, A.; Arya, M.; Briggs, T.; Barratt, D.; Charman, S.C.; Freeman, A.; Gelister, J.; Hawkes, D.; Hu, Y.; et al. The PICTURE study: Diagnostic accuracy of multiparametric MRI in men requiring a repeat prostate biopsy. Br. J. Cancer 2017, 116, 1159–1165. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-targeted or standard biopsy for prostate-cancer diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Lotan, Y.; Haddad, A.Q.; Costa, D.N.; Pedrosa, I.; Rofsky, N.M.; Roehrborn, C.G. Decision analysis model comparing cost of multiparametric magnetic resonance imaging vs. repeat biopsy for detection of prostate cancer in men with prior negative findings on biopsy. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 266-e9. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.; Gontero, P.; Mostafid, A.H.; Palou, J. EAU Guidelines; Edn. Presented at the EAU Annual Congress Amsterdam; EAU Guidelines Office: Arnhem, The Netherlands, 2020; ISBN 978-94-92671-07-3. [Google Scholar]
- Chaddad, A.; Kucharczyk, M.J.; Niazi, T. Multimodal radiomic features for the predicting gleason score of prostate cancer. Cancers 2018, 10, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaddad, A.; Niazi, T.; Probst, S.; Bladou, F.; Anidjar, M.; Bahoric, B. Predicting gleason score of prostate cancer patients using radiomic analysis. Front. Oncol. 2018, 8, 630. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; Bukov, M.; Wang, C.-H.; Day, A.G.R.; Richardson, C.; Fisher, C.K.; Schwab, D.J. A high-bias, low-variance introduction to machine learning for physicists. Phys. Rep. 2019, 810, 1–124. [Google Scholar] [CrossRef] [PubMed]
- Chaddad, A.; Desrosiers, C.; Toews, M.; Abdulkarim, B. Predicting survival time of lung cancer patients using radiomic analysis. Oncotarget 2017, 8, 104393. [Google Scholar] [CrossRef]
- Chaddad, A.; Desrosiers, C.; Bouridane, A.; Toews, M.; Hassan, L.; Tanougast, C. Multi texture analysis of colorectal cancer continuum using multispectral imagery. PLoS ONE 2016, 11, e0149893. [Google Scholar] [CrossRef]
- Chaddad, A.; Daniel, P.; Sabri, S.; Desrosiers, C.; Abdulkarim, B. Integration of radiomic and multi-omic analyses predicts survival of newly diagnosed IDH1 wild-type glioblastoma. Cancers 2019, 11, 1148. [Google Scholar] [CrossRef] [Green Version]
- Park, J.E.; Park, S.Y.; Kim, H.J.; Kim, H.S. Reproducibility and generalizability in radiomics modeling: Possible strategies in radiologic and statistical perspectives. Korean J. Radiol. 2019, 20, 1124–1137. [Google Scholar] [CrossRef]
- Szolovits, P. Artificial Intelligence in Medicine; Routledge: Abingdon, UK, 2019. [Google Scholar]
- Bardis, M.D.; Houshyar, R.; Chang, P.D.; Ushinsky, A.; Glavis-Bloom, J.; Chahine, C.; Bui, T.-L.; Rupasinghe, M.; Filippi, C.G.; Chow, D.S. Applications of artificial intelligence to prostate multiparametric MRI (MpMRI): Current and emerging trends. Cancers 2020, 12, 1204. [Google Scholar] [CrossRef]
- Mortensen, M.A.; Borrelli, P.; Poulsen, M.H.; Gerke, O.; Enqvist, O.; Ulén, J.; Trägardh, E.; Constantinescu, C.; Edenbrandt, L.; Lund, L. Artificial intelligence-based versus manual assessment of prostate cancer in the prostate gland: A method comparison study. Clin. Physiol. Funct. Imaging 2019, 39, 399–406. [Google Scholar] [CrossRef]
- Ström, P.; Kartasalo, K.; Olsson, H.; Solorzano, L.; Delahunt, B.; Berney, D.M.; Bostwick, D.G.; Evans, A.J.; Grignon, D.J.; Humphrey, P.A. Artificial intelligence for diagnosis and grading of prostate cancer in biopsies: A population-based, diagnostic study. Lancet Oncol. 2020, 21, 222–232. [Google Scholar] [CrossRef]
- Goldenberg, S.L.; Nir, G.; Salcudean, S.E. A new era: Artificial intelligence and machine learning in prostate cancer. Nat. Rev. Urol. 2019, 16, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Eminaga, O.; Loening, A.; Lu, A.; Brooks, J.D.; Rubin, D. Detection of Prostate Cancer and Determination of Its Significance Using Explainable Artificial Intelligence; American Society of Clinical Oncology: Alexandria, VA, USA, 2020. [Google Scholar]
- Raciti, P.; Sue, J.; Ceballos, R.; Godrich, R.; Kunz, J.D.; Kapur, S.; Reuter, V.; Grady, L.; Kanan, C.; Klimstra, D.S. Novel artificial intelligence system increases the detection of prostate cancer in whole slide images of core needle biopsies. Mod. Pathol. 2020, 33, 2058–2066. [Google Scholar] [CrossRef] [PubMed]
- Koçak, B.; Durmaz, E.Ş.; Ateş, E.; Kılıçkesmez, Ö. Radiomics with Artificial Intelligence: A Practical Guide for Beginners. Diagn. Interv. Radiol. 2019, 25, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Cuocolo, R.; Stanzione, A.; Ponsiglione, A.; Romeo, V.; Verde, F.; Creta, M.; La Rocca, R.; Longo, N.; Pace, L.; Imbriaco, M. Clinically significant prostate cancer detection on MRI: A radiomic shape features study. Eur. J. Radiol. 2019, 116, 144–149. [Google Scholar] [CrossRef]
- Castillo, J.M.T.; Starmans, M.P.A.; Niessen, W.J.; Schoots, I.; Klein, S.; Veenland, J.F. Classification of Prostate Cancer: High Grade versus Low Grade Using a Radiomics Approach. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 1319–1322. [Google Scholar]
- Gong, L.; Xu, M.; Fang, M.; Zou, J.; Yang, S.; Yu, X.; Xu, D.; Zhou, L.; Li, H.; He, B.; et al. Non-Invasive Prediction of Prostate Cancer Gleason Scores via Radiomics Analysis; Social Science Research Network: Rochester, NY, USA, 2019. [Google Scholar]
- Merisaari, H.; Taimen, P.; Shiradkar, R.; Ettala, O.; Pesola, M.; Saunavaara, J.; Boström, P.J.; Madabhushi, A.; Aronen, H.J.; Jambor, I. Repeatability of radiomics and machine learning for DWI: Short-term repeatability study of 112 patients with prostate cancer. Magn. Reson. Med. 2020, 83, 2293–2309. [Google Scholar] [CrossRef]
- Sunoqrot, M.R.S.; Selnæs, K.M.; Sandsmark, E.; Nketiah, G.A.; Zavala-Romero, O.; Stoyanova, R.; Bathen, T.F.; Elschot, M. A quality control system for automated prostate segmentation on T2-weighted MRI. Diagnostics 2020, 10, 714. [Google Scholar] [CrossRef]
- Khalvati, F.; Zhang, J.; Chung, A.G.; Shafiee, M.J.; Wong, A.; Haider, M.A. MPCaD: A multi-scale radiomics-driven framework for automated prostate cancer localization and detection. BMC Med. Imaging 2018, 18, 16. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.; Fong, A.; McVicar, N.; Smith, S.; Giambattista, J.; Wells, D.; Kolbeck, C.; Giambattista, J.; Gondara, L.; Alexander, A. Comparing deep learning-based auto-segmentation of organs at risk and clinical target volumes to expert inter-observer variability in radiotherapy planning. Radiother. Oncol. 2020, 144, 152–158. [Google Scholar] [CrossRef]
- Shiradkar, R.; Podder, T.K.; Algohary, A.; Viswanath, S.; Ellis, R.J.; Madabhushi, A. Radiomics based targeted radiotherapy planning (Rad-TRaP): A computational framework for prostate cancer treatment planning with MRI. Radiat. Oncol. 2016, 11, 148. [Google Scholar] [CrossRef] [Green Version]
- Macomber, M.W.; Phillips, M.; Tarapov, I.; Jena, R.; Nori, A.; Carter, D.; Folgoc, L.L.; Criminisi, A.; Nyflot, M.J. Autosegmentation of prostate anatomy for radiation treatment planning using deep decision forests of radiomic features. Phys. Med. Biol. 2018, 63, 235002. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Tahoun, M.; Klaan, B.; Thierfelder, K.M.; Weber, M.-A.; Krause, B.J.; Hakenberg, O.; Fuellen, G.; Hamed, M. A Radiogenomic approach for decoding molecular mechanisms underlying tumor progression in prostate cancer. Cancers 2019, 11, 1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamshidi, N.; Margolis, D.J.; Raman, S.; Huang, J.; Reiter, R.E.; Kuo, M.D. Multiregional radiogenomic assessment of prostate microenvironments with multiparametric MR imaging and DNA whole-exome sequencing of prostate glands with adenocarcinoma. Radiology 2017, 284, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.P.; Czarniecki, M.; Mehralivand, S.; Stoyanova, R.; Choyke, P.L.; Harmon, S.; Turkbey, B. Radiomics and radiogenomics of prostate cancer. Abdom. Radiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lo Gullo, R.; Daimiel, I.; Morris, E.A.; Pinker, K. Combining molecular and imaging metrics in cancer: Radiogenomics. Insights Imaging 2020, 11, 1. [Google Scholar] [CrossRef]
- Shiri, I.; Maleki, H.; Hajianfar, G.; Abdollahi, H.; Ashrafinia, S.; Hatt, M.; Zaidi, H.; Oveisi, M.; Rahmim, A. Next-generation radiogenomics sequencing for prediction of EGFR and KRAS mutation status in NSCLC patients using multimodal imaging and machine learning algorithms. Mol. Imaging Biol. 2020, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Norris, J.M.; Simpson, B.S.; Parry, M.A.; Allen, C.; Ball, R.; Freeman, A.; Kelly, D.; Kim, H.L.; Kirkham, A.; You, S.; et al. Genetic landscape of prostate cancer conspicuity on multiparametric magnetic resonance imaging: A systematic review and bioinformatic analysis. Eur. Urol. Open Sci. 2020, 20, 37–47. [Google Scholar] [CrossRef]
- Stabile, A.; Giganti, F.; Rosenkrantz, A.B.; Taneja, S.S.; Villeirs, G.; Gill, I.S.; Allen, C.; Emberton, M.; Moore, C.M.; Kasivisvanathan, V. Multiparametric MRI for prostate cancer diagnosis: Current status and future directions. Nat. Rev. Urol. 2020, 17, 41–61. [Google Scholar] [CrossRef]
- Cai, W.; Zhu, D.; Byanju, S.; Chen, J.; Zhang, H.; Wang, Y.; Liao, M. Magnetic resonance spectroscopy imaging in diagnosis of suspicious prostate cancer. Medicine 2019, 98. [Google Scholar] [CrossRef]
- Dickinson, L.; Ahmed, H.U.; Allen, C.; Barentsz, J.O.; Carey, B.; Futterer, J.J.; Heijmink, S.W.; Hoskin, P.J.; Kirkham, A.; Padhani, A.R.; et al. Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: Recommendations from a european consensus meeting. Eur. Urol. 2011, 59, 477–494. [Google Scholar] [CrossRef]
- Barth, B.K.; De Visschere, P.J.; Cornelius, A.; Nicolau, C.; Vargas, H.A.; Eberli, D.; Donati, O.F. Detection of clinically significant prostate cancer: Short dual–Pulse sequence versus standard multiparametric MR imaging—A multireader study. Radiology 2017, 284, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Greer, M.D.; Shih, J.H.; Lay, N.; Barrett, T.; Kayat Bittencourt, L.; Borofsky, S.; Kabakus, I.M.; Law, Y.M.; Marko, J.; Shebel, H. Validation of the dominant sequence paradigm and role of dynamic contrast-enhanced imaging in PI-RADS version 2. Radiology 2017, 285, 859–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.M.; Turkbey, B.; Figg, W.D.; Choyke, P.L. Multiparametric MRI in prostate cancer management. Nat. Rev. Clin. Oncol. 2014, 11, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Daun, M.; Fardin, S.; Ushinsky, A.; Batra, S.; Nguyentat, M.; Lee, T.; Uchio, E.; Lall, C.; Houshyar, R. PI-RADS version 2 is an excellent screening tool for clinically significant prostate cancer as designated by the validated international society of urological pathology criteria: A retrospective analysis. Curr. Probl. Diagn. Radiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, E.; Stabile, A.; Pellegrino, F.; Basile, G.; Cignoli, D.; Cirulli, G.O.; Sorce, G.; Barletta, F.; Scuderi, S.; Bravi, C.A. Positive predictive value of prostate imaging reporting and data system version 2 for the detection of clinically significant prostate cancer: A systematic review and meta-analysis. Eur. Urol. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wadera, A.; Alabousi, M.; Pozdnyakov, A.; Kashif Al-Ghita, M.; Jafri, A.; McInnes, M.D.; Schieda, N.; van der Pol, C.B.; Salameh, J.-P.; Samoilov, L. Impact of PI-RADS category 3 lesions on the diagnostic accuracy of MRI for detecting prostate cancer and the prevalence of prostate cancer within each PI-RADS category: A systematic review and meta-analysis. Br. J. Radiol. 2020, 93, 20191050. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Mani, H.; Shah, V.; Rastinehad, A.R.; Bernardo, M.; Pohida, T.; Pang, Y.; Daar Dagane, R.T.; Benjamin, C.; McKinney, Y.L.; et al. Multiparametric 3T prostate MR imaging to detect cancer: Histopathologic correlation using prostatectomy specimens processed in customized MRI-based molds. J. Urol. 2011, 186, 1818–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westphalen, A.C.; McCulloch, C.E.; Anaokar, J.M.; Arora, S.; Barashi, N.S.; Barentsz, J.O.; Bathala, T.K.; Bittencourt, L.K.; Booker, M.T.; Braxton, V.G.; et al. Variability of the positive predictive value of PI-RADS for prostate MRI across 26 centers: Experience of the society of abdominal radiology prostate cancer disease-focused panel. Radiology 2020, 296, 76–84. [Google Scholar] [CrossRef]
- Leake, J.L.; Hardman, R.; Ojili, V.; Thompson, I.; Shanbhogue, A.; Hernandez, J.; Barentsz, J. Prostate MRI: Access to and current practice of prostate MRI in the United States. J. Am. Coll. Radiol. 2014, 11, 156–160. [Google Scholar] [CrossRef] [Green Version]
- Barentsz, J.O.; Weinreb, J.C.; Verma, S.; Thoeny, H.C.; Tempany, C.M.; Shtern, F.; Padhani, A.R.; Margolis, D.; Macura, K.J.; Haider, M.A.; et al. Synopsis of the PI-RADS v2 guidelines for multiparametric prostate magnetic resonance imaging and recommendations for use. Eur. Urol. 2016, 69, 41–49. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and data system: 2015, version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Fütterer, J.J. European society of urogenital radiology ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate imaging reporting and data system version 2.1: 2019 update of prostate imaging reporting and data system version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Greer, M.D.; Shih, J.H.; Lay, N.; Barrett, T.; Bittencourt, L.; Borofsky, S.; Kabakus, I.; Law, Y.M.; Marko, J.; Shebel, H.; et al. Interreader variability of prostate imaging reporting and data system version 2 in detecting and assessing prostate cancer lesions at prostate MRI. Am. J. Roentgenol. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kohestani, K.; Wallström, J.; Dehlfors, N.; Sponga, O.M.; Månsson, M.; Josefsson, A.; Carlsson, S.; Hellström, M.; Hugosson, J. Performance and inter-observer variability of prostate MRI (PI-RADS version 2) outside high-volume centres. Scand. J. Urol. 2019, 53, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W.; Shin, S.-J.; Taik Oh, Y.; Jung, D.C.; Cho, N.H.; Choi, Y.D.; Park, S.Y. PI-RADS version 2: Detection of clinically significant cancer in patients with biopsy gleason score 6 prostate cancer. Am. J. Roentgenol. 2017, 209, W1–W9. [Google Scholar] [CrossRef]
- Kristiansen, G. Diagnostic and prognostic molecular biomarkers for prostate cancer. Histopathology 2012, 60, 125–141. [Google Scholar] [CrossRef]
- Guo, T.; Li, L.; Zhong, Q.; Rupp, N.J.; Charmpi, K.; Wong, C.E.; Wagner, U.; Rueschoff, J.H.; Jochum, W.; Fankhauser, C.D.; et al. Multi-region proteome analysis quantifies spatial heterogeneity of prostate tissue biomarkers. Life Sci. Alliance 2018, 1. [Google Scholar] [CrossRef] [Green Version]
- Stewart, G.D.; Van Neste, L.; Delvenne, P.; Delrée, P.; Delga, A.; McNeill, S.A.; O’Donnell, M.; Clark, J.; Van Criekinge, W.; Bigley, J.; et al. Clinical utility of an epigenetic assay to detect occult prostate cancer in histopathologically negative biopsies: Results of the MATLOC study. J. Urol. 2013, 189, 1110–1116. [Google Scholar] [CrossRef]
- McRobbie, D.W.; Moore, E.A.; Graves, M.J.; Prince, M.R. MRI from Picture to Proton, 3rd ed.; Cambridge University Press: Cambridge, UK, 2017; ISBN 978-1-107-64323-9. [Google Scholar]
- Latchamsetty, K.C.; Borden, L.S.; Porter, C.R.; Lacrampe, M.; Vaughan, M.; Lin, E.; Conti, N.; Wright, J.L.; Corman, J.M. Experience improves staging accuracy of endorectal magnetic resonance imaging in prostate cancer: What is the learning curve? Can. J. Urol. 2007, 14, 3429–3434. [Google Scholar]
- De Visschere, P.J.L.; Vral, A.; Perletti, G.; Pattyn, E.; Praet, M.; Magri, V.; Villeirs, G.M. Multiparametric magnetic resonance imaging characteristics of normal, benign and malignant conditions in the prostate. Eur. Radiol. 2017, 27, 2095–2109. [Google Scholar] [CrossRef]
- Schwier, M.; van Griethuysen, J.; Vangel, M.G.; Pieper, S.; Peled, S.; Tempany, C.; Aerts, H.J.W.L.; Kikinis, R.; Fennessy, F.M.; Fedorov, A. Repeatability of multiparametric prostate MRI radiomics features. Sci. Rep. 2019, 9, 9441. [Google Scholar] [CrossRef] [PubMed]
- Madabhushi, A.; Algohary, A.; Shiradkar, R. Predicting Prostate Cancer Risk of Progression with Multiparametric Magnetic Resonance Imaging Using Machine Learning and Peritumoral Radiomics. U.S. Patent Application 16/395,904, 2 January 2020. [Google Scholar]
- Abdollahi, H.; Mofid, B.; Shiri, I.; Razzaghdoust, A.; Saadipoor, A.; Mahdavi, A.; Galandooz, H.M.; Mahdavi, S.R. Machine learning-based radiomic models to predict intensity-modulated radiation therapy response, gleason score and stage in prostate cancer. Radiol. Med. 2019, 124, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Bleker, J.; Kwee, T.C.; Dierckx, R.A.J.O.; de Jong, I.J.; Huisman, H.; Yakar, D. Multiparametric MRI and auto-fixed volume of interest-based radiomics signature for clinically significant peripheral zone prostate cancer. Eur. Radiol. 2020, 30, 1313–1324. [Google Scholar] [CrossRef] [Green Version]
- Abreu-Gomez, J.; Shabana, W.; McInnes, M.D.F.; O’Sullivan, J.P.; Morash, C.; Schieda, N. Regional standardization of prostate multiparametric MRI performance and reporting: Is there a role for a director of prostate imaging? Am. J. Roentgenol. 2019, 213, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Alley, S.; Fedorov, A.; Menard, C.; Kadoury, S. Evaluation of intensity-based deformable registration of multi-parametric MRI for radiomics analysis of the prostate. In Proceedings of the Medical Imaging 2020: Biomedical Applications in Molecular, Structural, and Functional Imaging, Houston, TX, USA, 28 February 2020; Volume 11317, p. 113171H. [Google Scholar]
- Stanzione, A.; Gambardella, M.; Cuocolo, R.; Ponsiglione, A.; Romeo, V.; Imbriaco, M. Prostate MRI radiomics: A systematic review and radiomic quality score assessment. Eur. J. Radiol. 2020, 129, 109095. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Lee, K.; Shin, E.; Choy, G.; Do, S. How Much Data Is Needed to Train a Medical Image Deep Learning System to Achieve Necessary High Accuracy? arXiv 2016, arXiv:1511.06348. [Google Scholar]
- Woźnicki, P.; Westhoff, N.; Huber, T.; Riffel, P.; Froelich, M.F.; Gresser, E.; von Hardenberg, J.; Mühlberg, A.; Michel, M.S.; Schoenberg, S.O.; et al. Multiparametric MRI for prostate cancer characterization: Combined use of radiomics model with PI-RADS and clinical parameters. Cancers 2020, 12, 1767. [Google Scholar] [CrossRef]
- Castillo, T.J.M.; Arif, M.; Niessen, W.J.; Schoots, I.G.; Veenland, J.F. Automated classification of significant prostate cancer on MRI: A systematic review on the performance of machine learning applications. Cancers 2020, 12, 1606. [Google Scholar] [CrossRef]
- Chaddad, A.; Kucharczyk, M.J.; Desrosiers, C.; Okuwobi, I.P.; Katib, Y.; Zhang, M.; Rathore, S.; Sargos, P.; Niazi, T. Deep radiomic analysis to predict gleason score in prostate cancer. IEEE Access 2020, 8, 167767–167778. [Google Scholar] [CrossRef]
- Yuan, Y.; Qin, W.; Buyyounouski, M.; Ibragimov, B.; Hancock, S.; Han, B.; Xing, L. Prostate cancer classification with multiparametric MRI transfer learning model. Med. Phys. 2019, 46, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Cheddad, A.; Czene, K.; Shepherd, J.A.; Li, J.; Hall, P.; Humphreys, K. Enhancement of mammographic density measures in breast cancer risk prediction. Cancer Epidemiol. Prev. Biomark. 2014, 23, 1314–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourel, P.; Gibon, D.; Coste, E.; Daanen, V.; Rousseau, J. Automatic quality assessment protocol for MRI equipment. Med. Phys. 1999, 26, 2693–2700. [Google Scholar] [CrossRef] [PubMed]
- Aja-Fernandez, S.; Alberola-Lopez, C.; Westin, C.-F. Noise and signal estimation in magnitude MRI and rician distributed images: A LMMSE approach. IEEE Trans. Image Process. 2008, 17, 1383–1398. [Google Scholar] [CrossRef] [Green Version]
- Ellingson, B.M.; Zaw, T.; Cloughesy, T.F.; Naeini, K.M.; Lalezari, S.; Mong, S.; Lai, A.; Nghiemphu, P.L.; Pope, W.B. Comparison between intensity normalization techniques for dynamic susceptibility contrast (DSC)-MRI estimates of cerebral blood volume (CBV) in human gliomas. J. Magn. Reson. Imaging 2012, 35, 1472–1477. [Google Scholar] [CrossRef] [Green Version]
- Onofrey, J.A.; Casetti-Dinescu, D.I.; Lauritzen, A.D.; Sarkar, S.; Venkataraman, R.; Fan, R.E.; Sonn, G.A.; Sprenkle, P.C.; Staib, L.H.; Papademetris, X. Generalizable multi-site training and testing of deep neural networks using image normalization. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 348–351. [Google Scholar]
- Scalco, E.; Belfatto, A.; Mastropietro, A.; Rancati, T.; Avuzzi, B.; Messina, A.; Valdagni, R.; Rizzo, G. T2w-MRI signal normalization affects radiomics features reproducibility. Med. Phys. 2020, 47, 1680–1691. [Google Scholar] [CrossRef]
- Sollini, M.; Cozzi, L.; Antunovic, L.; Chiti, A.; Kirienko, M. PET radiomics in NSCLC: State of the art and a proposal for harmonization of methodology. Sci. Rep. 2017, 7, 358. [Google Scholar] [CrossRef] [Green Version]
- Rivera, S.C.; Liu, X.; Chan, A.-W.; Denniston, A.K.; Calvert, M.J. Guidelines for clinical trial protocols for interventions involving artificial intelligence: The Spirit-AI Extension. BMJ 2020, 370. [Google Scholar] [CrossRef]
- Ghose, S.; Oliver, A.; Martí, R.; Lladó, X.; Vilanova, J.C.; Freixenet, J.; Mitra, J.; Sidibé, D.; Meriaudeau, F. A survey of prostate segmentation methodologies in ultrasound, magnetic resonance and computed tomography images. Comput. Methods Programs Biomed. 2012, 108, 262–287. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.S.; Chaitanya, K.; Schawkat, K.; Muehlematter, U.J.; Hötker, A.M.; Konukoglu, E.; Donati, O.F. Variability of manual segmentation of the prostate in axial T2-weighted MRI: A multi-reader study. Eur. J. Radiol. 2019, 121, 108716. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ITK-SNAP Home. Available online: http://www.itksnap.org/pmwiki/pmwiki.php (accessed on 25 November 2020).
- Lu, X.; Zha, Y.; Qiao, Y.; Wang, D. Feature-based deformable registration using minimal spanning tree for prostate MR segmentation. IEEE Access 2019, 7, 138645–138656. [Google Scholar] [CrossRef]
- Steenbergen, P.; Haustermans, K.; Lerut, E.; Oyen, R.; De Wever, L.; Van den Bergh, L.; Kerkmeijer, L.G.W.; Pameijer, F.A.; Veldhuis, W.B.; van der Voort van Zyp, J.R.N.; et al. Prostate tumor delineation using multiparametric magnetic resonance imaging: Inter-observer variability and pathology validation. Radiother. Oncol. 2015, 115, 186–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, K.H.; Warfield, S.K.; Bharatha, A.; Tempany, C.M.C.; Kaus, M.R.; Haker, S.J.; Wells, W.M.; Jolesz, F.A.; Kikinis, R. Statistical validation of image segmentation quality based on a spatial overlap index. Acad. Radiol. 2004, 11, 178–189. [Google Scholar] [CrossRef] [Green Version]
- Rundo, L.; Militello, C.; Russo, G.; Garufi, A.; Vitabile, S.; Gilardi, M.C.; Mauri, G. Automated prostate gland segmentation based on an unsupervised fuzzy c-means clustering technique using multispectral T1w and T2w MR imaging. Information 2017, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Tian, Z.; Liu, L.; Zhang, Z.; Fei, B. PSNet: Prostate segmentation on MRI based on a convolutional neural network. J. Med. Imaging 2018, 5. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional networks for biomedical image segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Clark, T.; Wong, A.; Haider, M.A.; Khalvati, F. Fully deep convolutional neural networks for segmentation of the prostate gland in diffusion-weighted MR images. In Proceedings of the Image Analysis and Recognition, Montreal, QC, Canada, 5–7 July 2017; pp. 97–104. [Google Scholar]
- Zhu, Y.; Wei, R.; Gao, G.; Ding, L.; Zhang, X.; Wang, X.; Zhang, J. Fully automatic segmentation on prostate MR images based on cascaded fully convolution network. J. Magn. Reson. Imaging 2019, 49, 1149–1156. [Google Scholar] [CrossRef]
- Zhu, Q.; Du, B.; Turkbey, B.; Choyke, P.L.; Yan, P. Deeply-supervised CNN for prostate segmentation. In Proceedings of the 2017 International Joint Conference on Neural Networks (IJCNN), Anchorage, AK, USA, 14–19 May 2017; pp. 178–184. [Google Scholar]
- Liu, Q.; Dou, Q.; Yu, L.; Heng, P.A. MS-Net: Multi-site network for improving prostate segmentation with heterogeneous MRI data. IEEE Trans. Med. Imaging 2020, 39, 2713–2724. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Tao, X.; Wei, Z.; Lin, L. Automatic segmentation of 3D prostate MR images with iterative localization refinement. Digit. Signal Process. 2020, 98, 102649. [Google Scholar] [CrossRef]
- Astono, I.P.; Welsh, J.S.; Chalup, S.; Greer, P. Optimisation of 2D U-Net model components for automatic prostate segmentation on MRI. Appl. Sci. 2020, 10, 2601. [Google Scholar] [CrossRef] [Green Version]
- Aldoj, N.; Biavati, F.; Michallek, F.; Stober, S.; Dewey, M. Automatic Prostate and Prostate Zones Segmentation of Magnetic Resonance Images Using DenseNet-like U-Net. Sci. Rep. 2020, 10, 14315. [Google Scholar] [CrossRef] [PubMed]
- Haralick, R.M. Statistical and Structural Approaches to Texture. Proc. IEEE 1979, 67, 786–804. [Google Scholar] [CrossRef]
- Wang, J.; Wu, C.-J.; Bao, M.-L.; Zhang, J.; Wang, X.-N.; Zhang, Y.-D. Machine learning-based analysis of MR radiomics can help to improve the diagnostic performance of PI-RADS v2 in clinically relevant prostate cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef] [PubMed]
- Karimi, D.; Ruan, D. Synergistic combination of learned and hand-crafted features for prostate lesion classification in multiparametric magnetic resonance imaging. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2017, Quebec City, QC, Canada, 10–14 September 2017; pp. 391–398. [Google Scholar]
- Chaddad, A.; Desrosiers, C.; Niazi, T. Deep radiomic analysis of MRI Related to alzheimer’s disease. IEEE Access 2018, 6, 58213–58221. [Google Scholar] [CrossRef]
- Bourbonne, V.; Fournier, G.; Vallières, M.; Lucia, F.; Doucet, L.; Tissot, V.; Cuvelier, G.; Hue, S.; Le Penn Du, H.; Perdriel, L.; et al. External validation of an MRI-derived radiomics model to predict biochemical recurrence after surgery for high-risk prostate cancer. Cancers 2020, 12, 814. [Google Scholar] [CrossRef] [Green Version]
- Cheddad, A.; Czene, K.; Hall, P.; Humphreys, K. Pectoral muscle attenuation as a marker for breast cancer risk in full-field digital mammography. Cancer Epidemiol. Prev. Biomark. 2015, 24, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Abdi, H. Holm’s sequential bonferroni procedure. Encycl. Res. Des. 2010, 1, 1–8. [Google Scholar]
- Thenault, R.; Kaulanjan, K.; Darde, T.; Rioux-Leclercq, N.; Bensalah, K.; Mermier, M.; Khene, Z.; Peyronnet, B.; Shariat, S.; Pradère, B.; et al. The application of artificial intelligence in prostate cancer management—What improvements can be expected? A systematic review. Appl. Sci. 2020, 10, 6428. [Google Scholar] [CrossRef]
- Nuhić, J.; Kevrić, J. Prostate cancer detection using different classification techniques. In Proceedings of the CMBEBIH 2019, Banja Luka, Bosnia and Herzegovina, 16–18 May 2019; pp. 67–73. [Google Scholar]
- Radka, S.; Alan, P.; Mandeep, T.; Charles, L.; Nestor, P.; Lucia, L.C.L.; Mohammed, A.; Christine, B.; Rosa, C.; Merce, J.; et al. Association of multiparametric MRI quantitative imaging features with prostate cancer gene expression in MRI-targeted prostate biopsies. Oncotarget 2016, 7, 53362–53376. [Google Scholar] [CrossRef] [Green Version]
- Lapa, P.; Castelli, M.; Gonçalves, I.; Sala, E.; Rundo, L. A hybrid end-to-end approach integrating conditional random fields into CNNs for prostate cancer detection on MRI. Appl. Sci. 2020, 10, 338. [Google Scholar] [CrossRef] [Green Version]
- Otálora, S.; Atzori, M.; Khan, A.; Jimenez-del-Toro, O.; Andrearczyk, V.; Müller, H. A systematic comparison of deep learning strategies for weakly supervised gleason grading. In Proceedings of the Medical Imaging 2020: Digital Pathology, Houston, TX, USA, 15–20 February 2020; International Society for Optics and Photonics: Bellingham, WA, USA, 2020; Volume 11320, p. 113200L. [Google Scholar]
- Rundo, L.; Han, C.; Zhang, J.; Hataya, R.; Nagano, Y.; Militello, C.; Ferretti, C.; Nobile, M.S.; Tangherloni, A.; Gilardi, M.C.; et al. CNN-based prostate zonal segmentation on T2-weighted MR images: A cross-dataset study. In Neural Approaches to Dynamics of Signal Exchanges; Springer: Singapore, 2020; pp. 269–280. [Google Scholar] [CrossRef] [Green Version]
- Khan, Z.; Yahya, N.; Alsaih, K.; Ali, S.S.A.; Meriaudeau, F. Evaluation of deep neural networks for semantic segmentation of prostate in T2W MRI. Sensors 2020, 20, 3183. [Google Scholar] [CrossRef]
- Chaddad, A.; Toews, M.; Desrosiers, C.; Niazi, T. Deep radiomic analysis based on modeling information flow in convolutional neural networks. IEEE Access 2019, 7, 97242–97252. [Google Scholar] [CrossRef]
- Chaddad, A.; Zhang, M.; Desrosiers, C.; Niazi, T. Deep radiomic features from MRI scans predict survival outcome of recurrent glioblastoma. In Proceedings of the Radiomics and Radiogenomics in Neuro-Oncology, Shenzhen, China, 13 October 2019; pp. 36–43. [Google Scholar]
- Chaddad, A.; Sargos, P.; Desrosiers, C. Modeling texture in deep 3D CNN for survival analysis. IEEE J. Biomed. Health Inform. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chaddad, A.; Daniel, P.; Zhang, M.; Rathore, S.; Sargos, P.; Desrosiers, C.; Niazi, T. Deep radiomic signature with immune cell markers predicts the survival of glioma patients. Neurocomputing 2020. [Google Scholar] [CrossRef]
- Jensen, C.; Carl, J.; Boesen, L.; Langkilde, N.C.; Østergaard, L.R. Assessment of prostate cancer prognostic gleason grade group using zonal-specific features extracted from biparametric MRI using a KNN classifier. J. Appl. Clin. Med. Phys. 2019, 20, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Powers, D. Evaluation: From Precision, Recall and F-Measure to ROC, Informedness, Markedness and Correlation. J. Mach. Learn. Technolo. 2011, 2, 37–63. [Google Scholar]
- Fürnkranz, J.; Flach, P.A. An analysis of rule evaluation metrics. In Proceedings of the Twentieth International Conference on International Conference on Machine Learning, Washington, DC, USA, 21–24 August 2003; pp. 202–209. [Google Scholar]
- Sajjadi, M.S.M.; Bachem, O.; Lucic, M.; Bousquet, O.; Gelly, S. Assessing generative models via precision and recall. Adv. Neural Inf. Process. Syst. 2018, 31, 5228–5237. [Google Scholar]
- Li, M.; Chen, T.; Zhao, W.; Wei, C.; Li, X.; Duan, S.; Ji, L.; Lu, Z.; Shen, J. Radiomics prediction model for the improved diagnosis of clinically significant prostate cancer on biparametric MRI. Quant. Imaging Med. Surg. 2020, 10, 368–379. [Google Scholar] [CrossRef]
- Min, X.; Li, M.; Dong, D.; Feng, Z.; Zhang, P.; Ke, Z.; You, H.; Han, F.; Ma, H.; Tian, J.; et al. Multi-parametric MRI-based radiomics signature for discriminating between clinically significant and insignificant prostate cancer: Cross-validation of a machine learning method. Eur. J. Radiol. 2019, 115, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Toivonen, J.; Perez, I.M.; Movahedi, P.; Merisaari, H.; Pesola, M.; Taimen, P.; Boström, P.J.; Pohjankukka, J.; Kiviniemi, A.; Pahikkala, T.; et al. Radiomics and machine learning of multisequence multiparametric prostate MRI: Towards improved non-invasive prostate cancer characterization. PLoS ONE 2019, 14, e0217702. [Google Scholar] [CrossRef] [Green Version]
- Cao, R.; Mohammadian Bajgiran, A.; Afshari Mirak, S.; Shakeri, S.; Zhong, X.; Enzmann, D.; Raman, S.; Sung, K. Joint prostate cancer detection and gleason score prediction in Mp-MRI via FocalNet. IEEE Trans. Med. Imaging 2019, 38, 2496–2506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodalal, Z.; Trebeschi, S.; Nguyen-Kim, T.D.L.; Schats, W.; Beets-Tan, R. Radiogenomics: Bridging imaging and genomics. Abdom. Radiol. 2019, 44, 1960–1984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, M.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Survival with olaparib in metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2020, 383, 2345–2357. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of observation vs stereotactic ablative radiation for oligometastatic prostate cancer: The ORIOLE phase 2 randomized clinical trial. JAMA Oncol. 2020, 6, 650. [Google Scholar] [CrossRef] [Green Version]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Mohammad, T.A.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N. Engl. J. Med. 2014, 371, 1028–1038. [Google Scholar] [CrossRef] [Green Version]
- Niazi, T.; Williams, S.; Davis, I.D.; Stockler, M.R.; Martin, A.J.; Hague, W.; Bracken, K.; Gorzeman, M.; Roncolato, F.; Yip, S.; et al. DASL-HiCAP (ANZUP1801): The impact of darolutamide on standard therapy for localized very high-risk cancer of the prostate—A randomized phase III double-blind, placebo-controlled trial of adding darolutamide to androgen deprivation therapy and definitive or salvage radiation in very high-risk, clinically localized prostate cancer. JCO 2020, 38, TPS385. [Google Scholar] [CrossRef]
- Wedge, D.C.; Gundem, G.; Mitchell, T.; Woodcock, D.J.; Martincorena, I.; Ghori, M.; Zamora, J.; Butler, A.; Whitaker, H.; Kote-Jarai, Z.; et al. Sequencing of prostate cancers identifies new cancer genes, routes of progression and drug targets. Nat. Genet. 2018, 50, 682–692. [Google Scholar] [CrossRef] [Green Version]
- Abida, W.; Armenia, J.; Gopalan, A.; Brennan, R.; Walsh, M.; Barron, D.; Danila, D.; Rathkopf, D.; Morris, M.; Slovin, S.; et al. Prospective genomic profiling of prostate cancer across disease states reveals germline and somatic alterations that may affect clinical decision making. JCO Precis. Oncol. 2017, 2017. [Google Scholar] [CrossRef]
- Zhao, S.G.; Chen, W.S.; Li, H.; Foye, A.; Zhang, M.; Sjöström, M.; Aggarwal, R.; Playdle, D.; Liao, A.; Alumkal, J.J.; et al. The DNA methylation landscape of advanced prostate cancer. Nat. Genet. 2020, 52, 778–789. [Google Scholar] [CrossRef]
- Kucharczyk, M.J.; So, J.; Gravis, G.; Sweeney, C.; Saad, F.; Niazi, T. A combined biological and clinical rationale for evaluating metastasis directed therapy in the management of oligometastatic prostate cancer. Radiother. Oncol. 2020, 152, 80–88. [Google Scholar] [CrossRef]
- Chaddad, A.; Daniel, P.; Desrosiers, C.; Toews, M.; Abdulkarim, B. Novel radiomic features based on joint intensity matrices for predicting glioblastoma patient survival time. IEEE J. Biomed. Health Inform. 2018, 23, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Chaddad, A.; Desrosiers, C.; Abdulkarim, B.; Niazi, T. Predicting the gene status and survival outcome of lower grade glioma patients with multimodal MRI features. IEEE Access 2019, 7, 75976–75984. [Google Scholar] [CrossRef]
- Thawani, R.; McLane, M.; Beig, N.; Ghose, S.; Prasanna, P.; Velcheti, V.; Madabhushi, A. Radiomics and radiogenomics in lung cancer: A review for the clinician. Lung Cancer 2018, 115, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Iwatate, Y.; Hoshino, I.; Yokota, H.; Ishige, F.; Itami, M.; Mori, Y.; Chiba, S.; Arimitsu, H.; Yanagibashi, H.; Nagase, H.; et al. Radiogenomics for predicting P53 status, PD-L1 expression, and prognosis with machine learning in pancreatic cancer. Bri. J. Cancer 2020, 123, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Pinker, K.; Chin, J.; Melsaether, A.N.; Morris, E.A.; Moy, L. Precision medicine and radiogenomics in breast cancer: New approaches toward diagnosis and treatment. Radiology 2018, 287, 732–747. [Google Scholar] [CrossRef] [PubMed]
- PubChem PTEN-Phosphatase and Tensin Homolog (Human). Available online: https://pubchem.ncbi.nlm.nih.gov/gene/PTEN/human (accessed on 25 November 2020).
- McCann, S.M.; Jiang, Y.; Fan, X.; Wang, J.; Antic, T.; Prior, F.; VanderWeele, D.; Oto, A. Quantitative multiparametric MRI features and PTEN expression of peripheral zone prostate cancer: A pilot study. Am. J. Roentgenol. 2016, 206, 559–565. [Google Scholar] [CrossRef]
- Switlyk, M.D.; Salberg, U.B.; Geier, O.M.; Vlatkovic, L.; Lilleby, W.; Lyng, H.; Seierstad, T. PTEN expression in prostate cancer: Relationship with clinicopathologic features and multiparametric MRI findings. Am. J. Roentgenol. 2019, 212, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Stoyanova, R.; Takhar, M.; Tschudi, Y.; Ford, J.C.; Solórzano, G.; Erho, N.; Balagurunathan, Y.; Punnen, S.; Davicioni, E.; Gillies, R.J.; et al. Prostate cancer radiomics and the promise of radiogenomics. Transl. Cancer Res. 2016, 5, 432–447. [Google Scholar] [CrossRef] [Green Version]
- Brastianos, H.C.; Murgic, J.; Salcedo, A.; Chua, M.L.K.; Meng, A.; Fraser, M.; Brundage, M.; Fleshner, N.E.; van der Kwast, T.; Bristow, R.G.; et al. Determining the impact of spatial heterogeneity on genomic prognostic biomarkers for localized prostate cancer. Eur. Urol. Oncol. 2020. [Google Scholar] [CrossRef]
- Beksac, A.T.; Cumarasamy, S.; Falagario, U.; Xu, P.; Takhar, M.; Alshalalfa, M.; Gupta, A.; Prasad, S.; Martini, A.; Thulasidass, H.; et al. Multiparametric magnetic resonance imaging features identify aggressive prostate cancer at the phenotypic and transcriptomic level. J. Urol. 2018, 200, 1241–1249. [Google Scholar] [CrossRef]
- Li, L.; Shiradkar, R.; Algohary, A.; Leo, P.; Magi-Galluzzi, C.; Klein, E.; Purysko, A.; Madabhushi, A. Radiomic features derived from pre-operative multi-parametric MRI of prostate cancer are associated with decipher risk score. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis, San Diego, CA, USA, 16–21 February 2019; Volume 10950, p. 109503Y. [Google Scholar]
- Hectors, S.J.; Cherny, M.; Yadav, K.K.; Beksaç, A.T.; Thulasidass, H.; Lewis, S.; Davicioni, E.; Wang, P.; Tewari, A.K.; Taouli, B. Radiomics features measured with multiparametric magnetic resonance imaging predict prostate cancer aggressiveness. J. Urol. 2019, 202, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Houlahan, K.E.; Salmasi, A.; Sadun, T.Y.; Pooli, A.; Felker, E.R.; Livingstone, J.; Huang, V.; Raman, S.S.; Ahuja, P.; Sisk, A.E.; et al. Molecular hallmarks of multiparametric magnetic resonance imaging visibility in prostate cancer. Eur. Urol. 2019, 76, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Williams, S.; Byrne, D.; Keam, S.; Reynolds, H.M.; Mitchell, C.; Wraith, D.; Murphy, D.; Haworth, A. Association analysis between quantitative MRI features and hypoxia-related genetic profiles in prostate cancer: A pilot study. Br. J. Radiol. 2019, 92, 20190373. [Google Scholar] [CrossRef] [PubMed]
- Kesch, C.; Radtke, J.-P.; Wintsche, A.; Wiesenfarth, M.; Luttje, M.; Gasch, C.; Dieffenbacher, S.; Pecqueux, C.; Teber, D.; Hatiboglu, G.; et al. Correlation between genomic index lesions and MpMRI and 68Ga-PSMA-PET/CT imaging features in primary prostate cancer. Sci. Rep. 2018, 8, 16708. [Google Scholar] [CrossRef] [Green Version]
- Taylor, B.S.; Schultz, N.; Hieronymus, H.; Gopalan, A.; Xiao, Y.; Carver, B.S.; Arora, V.K.; Kaushik, P.; Cerami, E.; Reva, B.; et al. Integrative genomic profiling of human prostate cancer. Cancer Cell 2010, 18, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Gao, J.; Zhang, Q.; Fu, Y.; Liu, G.; Shi, J.; Li, D.; Wang, F.; Guo, H. Diagnostic value of 68Ga-PSMA PET/CT for detection of phosphatase and tensin homolog expression in prostate cancer: A pilot study. J. Nucl. Med. 2020, 61, 873–880. [Google Scholar] [CrossRef]
- Le, J.D.; Tan, N.; Shkolyar, E.; Lu, D.Y.; Kwan, L.; Marks, L.S.; Huang, J.; Margolis, D.J.A.; Raman, S.S.; Reiter, R.E. Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: Correlation with whole-mount histopathology. Eur. Urol. 2015, 67, 569–576. [Google Scholar] [CrossRef]
- Ahmed, H.U.; Bosaily, A.E.-S.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; You, S.; Nguyen, C.; Wang, Y.; Kim, J.; Sirohi, D.; Ziembiec, A.; Luthringer, D.; Lin, S.-C.; Daskivich, T.; et al. Genes involved in prostate cancer progression determine MRI visibility. Theranostics 2018, 8, 1752–1765. [Google Scholar] [CrossRef]
- Eineluoto, J.T.; Sandeman, K.; Pohjonen, J.; Sopyllo, K.; Nordling, S.; Stürenberg, C.; Malén, A.; Kilpeläinen, T.P.; Santti, H.; Petas, A.; et al. Associations of PTEN and ERG with magnetic resonance imaging visibility and assessment of non–organ-confined pathology and biochemical recurrence after radical prostatectomy. Eur. Urol. Focus 2020. [Google Scholar] [CrossRef]
- Lee, D.; Fontugne, J.; Gumpeni, N.; Park, K.; MacDonald, T.Y.; Robinson, B.D.; Sboner, A.; Rubin, M.A.; Mosquera, J.M.; Barbieri, C.E. Molecular alterations in prostate cancer and association with MRI features. Prostate Cancer Prostatic Dis. 2017, 20, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Parry, M.A.; Srivastava, S.; Ali, A.; Cannistraci, A.; Antonello, J.; Barros-Silva, J.D.; Ubertini, V.; Ramani, V.; Lau, M.; Shanks, J. Genomic evaluation of multiparametric magnetic resonance imaging-visible and-nonvisible lesions in clinically localised prostate cancer. Eur. Urol. Oncol. 2019, 2, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Salami, S.S.; Kaplan, J.B.; Nallandhighal, S.; Takhar, M.; Tosoian, J.J.; Lee, M.; Yoon, J.; Hovelson, D.H.; Plouffe, K.R.; Kaffenberger, S.D. Biologic significance of magnetic resonance imaging invisibility in localized prostate cancer. JCO Precis. Oncol. 2019, 3, 1–12. [Google Scholar] [CrossRef] [PubMed]
- NCCN—Evidence-Based Cancer Guidelines, Oncology Drug Compendium, Oncology Continuing Medical Education. Available online: https://www.nccn.org/ (accessed on 25 November 2020).
- Schoots, I.G.; Roobol, M.J.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Hunink, M.G.M. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: A systematic review and meta-analysis. Eur. Urol. 2015, 68, 438–450. [Google Scholar] [CrossRef]
- Ahmed, H.U. The index lesion and the origin of prostate cancer. N. Engl. J. Med. 2009, 361, 1704–1706. [Google Scholar] [CrossRef]
- Ploug, T.; Holm, S. The four dimensions of contestable AI diagnostics-A patient-centric approach to explainable AI. Artif. Intell. Med. 2020, 107, 101901. [Google Scholar] [CrossRef]
- Suh, J.; Yoo, S.; Park, J.; Cho, S.Y.; Cho, M.C.; Son, H.; Jeong, H. Development and validation of an explainable artificial intelligence-based decision-supporting tool for prostate biopsy. BJU Int. 2020, 126, 694–703. [Google Scholar] [CrossRef]
- Barredo Arrieta, A.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; Garcia, S.; Gil-Lopez, S.; Molina, D.; Benjamins, R.; et al. Explainable Artificial Intelligence (XAI): Concepts, Taxonomies, Opportunities and Challenges toward Responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Asan, O.; Bayrak, A.E.; Choudhury, A. Artificial intelligence and human trust in healthcare: Focus on clinicians. J. Med. Internet Res. 2020, 22, e15154. [Google Scholar] [CrossRef]
- Olsson, H.; Nordström, T.; Jäderling, F.; Egevad, L.; Vigneswaran, H.T.; Annerstedt, M.; Grönberg, H.; Eklund, M.; Lantz, A. Incorporating magnetic resonance imaging and biomarkers in active surveillance protocols—Results from the prospective stockholm3 active surveillance trial (STHLM3AS). JNCI J. Natl. Cancer Inst. 2020. [Google Scholar] [CrossRef]
- Spjuth, O.; Karlsson, A.; Clements, M.; Humphreys, K.; Ivansson, E.; Dowling, J.; Eklund, M.; Jauhiainen, A.; Czene, K.; Grönberg, H. E-science technologies in a workflow for personalized medicine using cancer screening as a case study. J. Am. Med. Inform. Assoc. 2017, 24, 950–957. [Google Scholar] [CrossRef] [PubMed]
- The molecular taxonomy of primary prostate cancer. Cell 2015, 163, 1011–1025. [CrossRef] [PubMed] [Green Version]
- Zuley, M.L.; Jarosz, R.; Drake, B.F.; Rancilio, D.; Klim, A.; Rieger-Christ, K.; Lemmerman, J. Radiology Data from The Cancer Genome Atlas Prostate Adenocarcinoma [TCGA-PRAD] Collection. Cancer Imaging Arch. 2016. [CrossRef]
- Fedorov, A.; Tempany, C.; Mulkern, R.; Fennessy, F. Data from QIN PROSTATE. Cancer Imaging Arch. 2016. [Google Scholar] [CrossRef]
- Mostert, M.; Bredenoord, A.L.; Biesaart, M.C.I.H.; van Delden, J.J.M. Big data in medical research and EU data protection law: Challenges to the consent or anonymise approach. Eur. J. Hum. Genet. 2016, 24, 956–960. [Google Scholar] [CrossRef]
- Ploug, T.; Holm, S. Informed consent and registry-based research—The case of the danish circumcision registry. BMC Med. Eth. 2017, 18. [Google Scholar] [CrossRef] [Green Version]
- Sultana, S.; Robinson, A.; Song, D.Y.; Lee, J. CNN-Based Hierarchical Coarse-to-Fine Segmentation of Pelvic CT Images for Prostate Cancer Radiotherapy. In Proceedings of the Medical Imaging 2020: Image-Guided Procedures, Robotic Interventions, and Modeling, Houston, TX, USA, 16 March 2020; Volume 11315, p. 113151I. [Google Scholar]
- Ushinsky, A.; Bardis, M.; Glavis-Bloom, J.; Uchio, E.; Chantaduly, C.; Nguyentat, M.; Chow, D.; Chang, P.; Houshyar, R. A 3D/2D hybrid U-net CNN approach to prostate organ segmentation of MpMRI. Am. J. Roentgenol. 2020. [Google Scholar] [CrossRef]
- Yaniv, O.; Portnoy, O.; Talmon, A.; Kiryati, N.; Konen, E.; Mayer, A. V-net light—Parameter-efficient 3-D convolutional neural network for prostate MRI segmentation. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI); IEEE, Iowa, IA, USA, 3–7 April 2020; pp. 442–445. [Google Scholar]
- Ren, J.; Hacihaliloglu, I.; Singer, E.A.; Foran, D.J.; Qi, X. Adversarial domain adaptation for classification of prostate histopathology whole-slide images. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2018, Granada, Spain, 16–20 September 2018; pp. 201–209. [Google Scholar]
- Zamboglou, C.; Carles, M.; Fechter, T.; Kiefer, S.; Reichel, K.; Fassbender, T.F.; Bronsert, P.; Koeber, G.; Schilling, O.; Ruf, J.; et al. Radiomic features from PSMA PET for non-invasive intraprostatic tumor discrimination and characterization in patients with intermediate- and high-risk prostate cancer—A comparison study with histology reference. Theranostics 2019, 9, 2595–2605. [Google Scholar] [CrossRef]


{kind=link}
| Gleason Score | 6 (3 + 3) | 7 (3 + 4) | 7 (4 + 3) | 8 (4 + 4; 3 + 5; or 5 + 3) | 9 (4 + 5; 5 + 4) or 10 (5 + 5) |
|---|---|---|---|---|---|
| ISUP Grade Group | 1 | 2 | 3 | 4 | 5 |
| Reference | Feature Methods | GS ≤ 6 | GS = 7 | GS ≥ 7 | GS ≥ 8 | GS ≤ 7 |
|---|---|---|---|---|---|---|
| Chaddad et al. [88] | Deep entropy features | 88.82 | 87.45 | 82.28 | 93.03 | 84.72 |
| Woznicki et al. [86] | 1 Standard features + Shape + PI-RADS + PSAD + DRE | 88.9 | - | 84.4 | - | - |
| Li et al. [137] | 1 Standard features + Clinical | - | - | 98.00 | - | - |
| Min et al. [138] | 1 Standard features + Shape | 82.30 | - | - | - | - |
| Chaddad et al. [24] | 1 Standard features | 83.40 | 72.71 | 77.35 | - | - |
| Cuocolo et al. [38] | Shape | 78.00 | - | - | - | - |
| Chaddad et al. [23] | Joint intensity matrices (JIM) + GLCM | 78.40 | 82.35 | 64.76 | - | - |
| Toivonen et al. [139] | GLCM + LBP + HOG + Gabor + Haar + filters | 88.00 | - | - | - | - |
| Jesen et al. [133] | 1 Standard features | 85.00 | 89.00 | 94.00 | 86.00 | 83.00 |
| Cao et al. [140] | FocalNet | - | 81.00 | 79.00 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaddad, A.; Kucharczyk, M.J.; Cheddad, A.; Clarke, S.E.; Hassan, L.; Ding, S.; Rathore, S.; Zhang, M.; Katib, Y.; Bahoric, B.; et al. Magnetic Resonance Imaging Based Radiomic Models of Prostate Cancer: A Narrative Review. Cancers 2021, 13, 552. https://doi.org/10.3390/cancers13030552
Chaddad A, Kucharczyk MJ, Cheddad A, Clarke SE, Hassan L, Ding S, Rathore S, Zhang M, Katib Y, Bahoric B, et al. Magnetic Resonance Imaging Based Radiomic Models of Prostate Cancer: A Narrative Review. Cancers. 2021; 13(3):552. https://doi.org/10.3390/cancers13030552
Chicago/Turabian StyleChaddad, Ahmad, Michael J. Kucharczyk, Abbas Cheddad, Sharon E. Clarke, Lama Hassan, Shuxue Ding, Saima Rathore, Mingli Zhang, Yousef Katib, Boris Bahoric, and et al. 2021. "Magnetic Resonance Imaging Based Radiomic Models of Prostate Cancer: A Narrative Review" Cancers 13, no. 3: 552. https://doi.org/10.3390/cancers13030552