BRAF Mutation in Colorectal Cancers: From Prognostic Marker to Targetable Mutation



1
Department of Gastroenterological Chemotherapy, Cancer Institute Hospital of the Japanese Foundation for Cancer Research (JFCR), Tokyo 135-8550, Japan
2
Department of Experimental Pathology, Cancer Institute of the Japanese Foundation for Cancer Research (JFCR), Tokyo 135-8550, Japan
*
Authors to whom correspondence should be addressed.
Cancers 2020, 12(11), 3236; https://doi.org/10.3390/cancers12113236
Submission received: 23 September 2020
/
Revised: 28 October 2020
/
Accepted: 29 October 2020
/
Published: 3 November 2020
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Colorectal cancer with a mutation in an oncogene BRAF has paid much attention, as it comprises a population with dismal prognosis since two decades ago. A series of research since then has successfully changed this malignancy to be treatable with specific treatment. Here we thoroughly overviewed the basic, translational and clinical studies on colorectal cancer with BRAF mutation from a physician’s viewpoint. Accumulating lines of evidence suggest that intervention of the trunk cellular growth signal transduction pathway, namely EGFR-RAS-RAF-MEK-ERK pathway, is a clue to controlling this disease. However, it is not so straightforward. Recent studies unveil the diverse and plastic nature of this signal transduction pathway. We will introduce our endeavor to conquer this condition, based on newly arriving datasets, and discuss how we could open the door to future development of CRC treatment.
Abstract
The Raf murine sarcoma viral oncogene homolog B (BRAF) mutation is detected in 8–12% of metastatic colorectal cancers (mCRCs) and is strongly correlated with poor prognosis. The recent success of the BEACON CRC study and the development of targeted therapy have led to the determination of BRAF-mutated mCRCs as an independent category. For nearly two decades, a growing body of evidence has established the significance of the BRAF mutation in the development of CRC. Herein, we overview both basic and clinical data relevant to BRAF-mutated CRC, mainly focusing on the development of treatment strategies. This review is organized into eight sections, including clinicopathological features, molecular features, prognosis, the predictive value of anti-epidermal growth factor receptor (EGFR) therapy, resistant mechanisms for BRAF-targeting treatment, the heterogeneity of the BRAF mutation, future perspectives, and conclusions. A characterization of the canonical mitogen-activated protein kinase (MAPK) pathway is essential for controlling this malignancy, and the optimal combination of multiple interventions for treatments remains a point of debate.
1. Introduction
Raf murine sarcoma viral oncogene homolog B (BRAF)-mutated colorectal cancers (CRCs) are found in a subgroup of CRCs with distinctive clinicopathological features [1]. Within a decade, emerging evidence on the BRAF mutation led clinicians to recognize the prognostic and predictive value of this gene alteration. Recently, the BRAF mutation has come into consideration when deliberating possible treatment options in clinical practice [2,3]. Currently, targeted therapy for BRAF-mutated metastatic CRC (mCRC) has been established [4,5]. In this review, we summarize the findings that have shaped our current understanding of the BRAF mutation.
Progress in general basic oncology has accelerated the transition of the significance of the BRAF mutation into clinical practice. We also introduce recent developments in cancer precision medicine, which would serve as a tailwind for the widespread adoption of BRAF genetic testing [6,7]. Moreover, we refer to the key findings from basic science which rationally support the foundation of current clinical trials [8,9].
Finally, we mention the future perspectives of BRAF-mutated mCRC and extend our discussion beyond the BRAF gene, toward the comprehensive assessment of the RAS–RAF–MEK–MAPK pathway.
2. Dawn of Targeted Therapy for BRAF-Mutated CRC
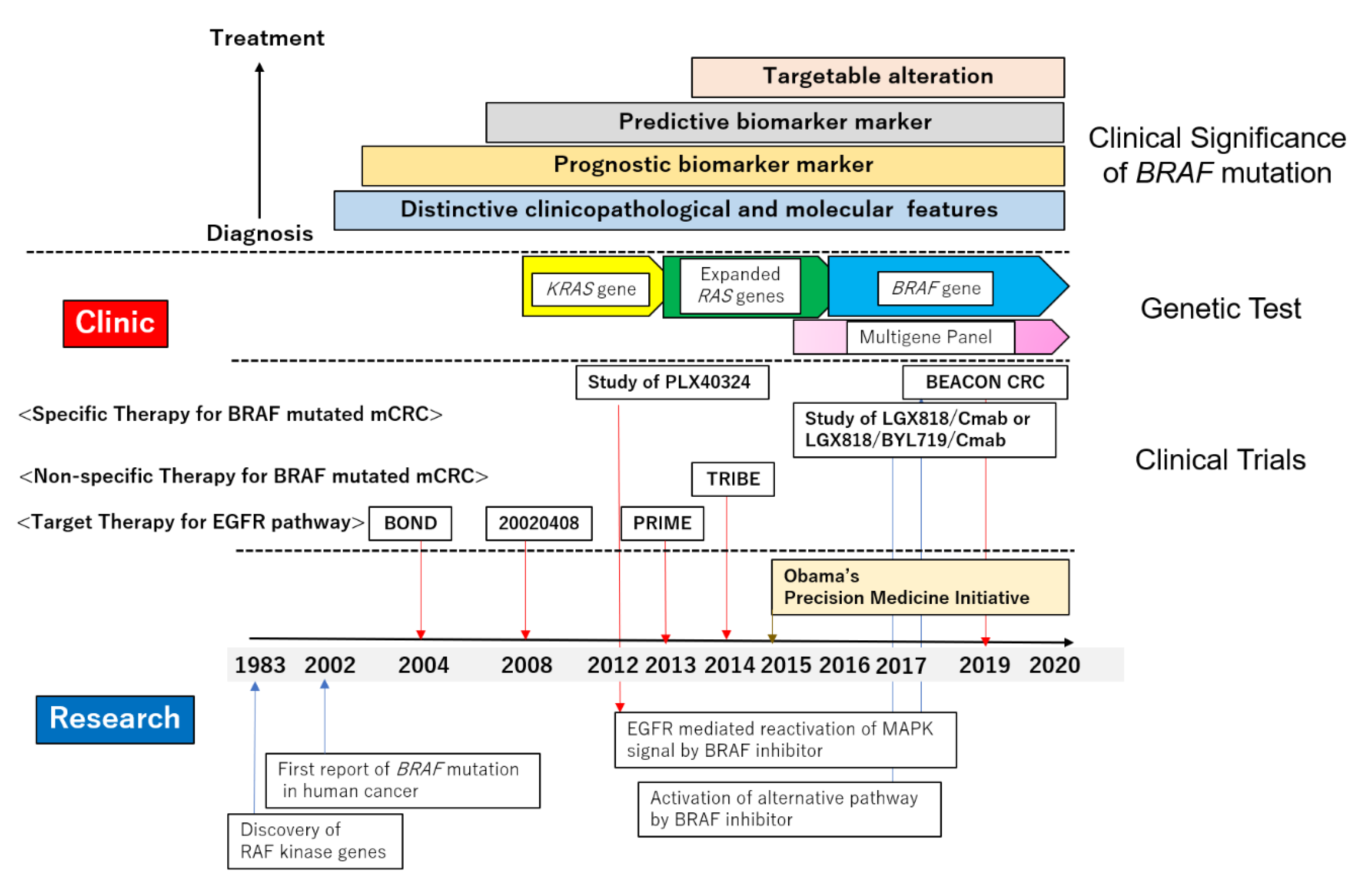
Two articles on the current RAF kinase genes were first published in 1983 [8,17,18], marking the beginning of such research. At this time, there were three RAF proteins—ARAF, BRAF, and CRAF—in mammalian cells known to display serine/threonine kinase activity [8,18]. Within the first decade of the discovery of RAF kinase, several studies have identified the function of RAF family proteins and their association with cancer. The RAF family proteins were shown to be activated by GTP-bound RAS and work as the effector to activate the signal transduction of the RAS–RAF–MEK–MAPK pathway, leading to cellular proliferation, differentiation, migration, and survival [8,9]. The RAS–RAF–MEK–MAPK pathway is dysregulated in many cancers. The constitutive activation of this signaling pathway occurs in oncogenic RAS- and RAF-driven cancers. In 2002, Davis et al. reported a high frequency of the BRAF mutation in human cancers, including melanoma, lung, and colorectal cancers [19]. Their findings highlighted BRAF-mutated CRC and marked the dawn of exploring targeted therapy for BRAF-mutated CRC.
3. Distinctive Characteristics of BRAF-Mutated CRC: Molecular and Clinicopathological Aspects
The BRAF mutation is detected in 8–12% of mCRCs and the BRAF gene encodes 766 amino acids [3]. The most prevalent point mutation occurs in the activation A-loop, near V600, and BRAFV600E accounts for >90% of mutations [3,8]. The positive association with microsatellite instability-high (MSI-H)/deficient mismatch repair (dMMR) tumors and mutual exclusiveness with the KRAS mutation of BRAFV600E-mutated CRC were initially well documented [20]. The BRAFV600E mutation was found in MSI-H/dMMR tumors with higher incidences, which were reported to range from 8% to 78% [20,21,22,23,24,25,26,27,28]. Hypermethylation is also one of the molecular features of BRAFV600E-mutated CRC. The BRAFV600E mutation was frequently observed more frequently in CpG island methylation phenotype (CIMP)-high CRC (77%), when compared to CIMP-low (18%) or negative (0%) CRC, with statistically significant differences [21]. These overlapping molecular features of BRAFV600E between MSI and CIMP would be organized by the understanding of the molecular pathogenesis of the serrated pathway [29]. Several studies recurrently identified the BRAFV600E mutation in precursor lesions, such as traditional serrated adenoma [21,29,30]. The BRAF mutation is thought to be the earliest event occurring in a precancerous lesion in the serrated pathway. Subsequently, the methylation of the CpG island at the promoter lesion would lead to the silencing of tumor suppressor genes, resulting in carcinogenesis [29]. Therefore, BRAFV600E-mutated CRC with sporadic microsatellite instability occurs as a consequence of the methylation of MutL homolog1 (MLH1) [29,30,31]. This is why a higher incidence of CpG island methylation is commonly seen in BRAFV600E-mutated CRC, regardless of the MSI status [22].
Several studies have consistently reported that BRAFV600E-mutated CRC had distinctive clinicopathological features. BRAFV600E-mutated CRCs were observed to be more prevalent in elderly or female patients and right-sided primary or mucinous histology tumors [1,2,3,4,5,14,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. In addition, several studies reported that BRAF-mutated CRC patients were more frequently observed in Caucasian than Asian or African American individuals [33,34,35,36]. Indeed, the prevalence of BRAF-mutated CRC was relatively low (6.4%) in the Japanese Nationwide Cancer Genome Screening Project (SCRUM-Japan), compared to those of large-scale studies mainly conducted in Western countries (8–12%) [3,37]. It is known that there are distinctive features in the metastatic site between BRAFV600E-mutated CRC and others. In general, the liver is the most prevalent metastatic site of CRC, but BRAFV600E-mutated CRCs tend to metastasize to the peritoneum, rather than the liver or lung [24,38]. However, these clinicopathological features are commonly seen in MSI-H or CIMP-high tumors [39,40]. MSI-H or CIMP-high tumors and BRAFV600E shared these features which cannot be attributed to their subtype.
In summary, clinicians at that time were aware of BRAF-mutated CRCs as a distinctive subtype of CRCs. Accumulating evidence in the initial period of research had significance for a profound understanding of the etiology, which is different from traditional adenoma–carcinoma sequencing [41]. At that time, the choice of treatment for CRC made by clinicians was not affected by BRAF status. The BRAF mutation is more frequently observed in sporadic CRC with a hypermethylated phenotype, but not in hereditary CRC, such as the Lynch syndrome. The clinical utility of BRAF genetic testing had only been found in the relatively convenient discriminator between sporadic and hereditary CRC [42,43].
4. BRAF Mutation Recognized as a Negative Prognostic Marker
We now discuss the prognostic impact of BRAF mutation in CRC patients. As is often the case, the crucial factor for the genetic testing of BRAF in clinical practice depends on whether the presence of the BRAF mutation affects clinicians’ decision making. First, we provide an overview of the association between the mutation and the indication of adjuvant chemotherapy for patients who underwent surgery with a curative intent. A retrospective cohort study conducted in multiple facilities in the Netherlands demonstrated that the BRAF mutation is an independent prognostic factor for overall survival (OS) (hazard ratio (HR) 2.22, 95% confidence interval (CI) 1.25–4.00), disease-free survival (DFS) (HR 2.33, 95% CI 1.22–4.55), and cancer-specific survival (CCS) (HR 2.13, 95% CI 1.01–4.55) in Stage Ⅱ/Ⅲ CRC by multivariate analysis [44]. However, as this study included patients treated between 1996 and 2004 and postoperative chemotherapy was not mentioned, this result cannot be directly applied to current practices. Two major clinical trials conducted in Europe and the United States reported consistent results: the retrospective study of the PETACC-3, EORTC 40993, SAKK 60-00 trials showed on one hand an independent negative prognostic value of the BRAF mutation in Stage Ⅱ/Ⅲ CRC (HR 1.78, 95% CI 1.15–2.76) [40]. On the other hand, the negative impact of the BRAF mutation on recurrence after curative resection was not statistically significant (HR 1.30, 95% CI 0.87–1.95) [45]. The other study using the results from the CALGB 89803 trial also provided an inferior effect on the survival of Stage Ⅲ CRC patients (HR 1.66, 95% CI 1.05–2.63) [46]. Thus, the negative prognostic impact of BRAF mutation on survival is reproducible, but the BRAF mutation is not useful as a negative predictive marker for recurrence after curative resection. It should be noted that these clinical trials assessed the efficacy of adding irinotecan to the fluoropyrimidine in the adjuvant setting, while oxaliplatin-based adjuvant chemotherapy had later been established as a standard regimen for Stage Ⅲ CRC patients who had received curative resection [47,48,49,50,51]. Therefore, the point becomes whether the BRAF mutation is indicative in making decisions on the adjuvant oxaliplatin-containing chemotherapy. The molecular profile of patients treated in another three pivotal clinical trials (MOSAIC, NSABP-C 07, and -C 08) was assessed and the significance of the BRAF mutation for survival and recurrence was evaluated [52,53]. However, their results were inconsistent: in a pooled analysis of NSABP-C 07 and -C 08, the BRAF mutation had a significant association with poor OS (HR 1.46, 95% CI 1.20–1.79) and survival after relapse (HR 2.31, 95% CI 1.83–2.95) [52], but in the MOSAIC study, a poor prognostic value of the BRAF mutation was not demonstrated. In clinical practice, however, oxaliplatin in addition to fluorouracil plus leucovorin were used, even in BRAF-mutated CRCs [53]. Thereby, oxaliplatin-containing adjuvant chemotherapy has been recommended for Stage Ⅲ CRC patients after curative resection, irrespectively of BRAF status, and to date, BRAF mutation has failed to become a game changer in the treatment of CRCs after curative resection.
Then, we will discuss the prognostic value of the BRAF mutation after metastasectomy. The resection of metastatic sites in general had been demonstrated to be key in the long-term survival or cure of mCRC patients, especially in cases of colorectal cancer liver-limited metastasis (CRLM) [54]. That said, tumor relapse is to occur in 50–75% of patients after R0 metastasectomy [55,56]. Therefore, a biomarker indicating the risk of recurrence is warranted. The prognostic value of the KRAS mutation in patients with resectable mCRCs has been pointed out [57,58,59,60,61,62,63]. That of BRAF mutation has not yet reached conclusive results to date, primarily because a very limited number of BRAF-mutated CRCs are subject to resection, unlike in cases of KRAS-mutated CRC (30–40%) [64]. The overall incidence of the BRAF mutation in mCRC is reported to be 8–12% [1] and recent studies show that patients with the BRAF mutation account for only 1–4% of mCRC patients who underwent metastasectomy [38,59,64,65,66,67,68,69]. Due to these very small numbers, the impact of the BRAF mutation on survival with other confounders remains unclear [59,70]. For instance, there are only 24 mCRC patients harboring the BRAF mutation in a systematic review and meta-analysis [68]. All reports on metastasectomy which we reviewed focused on hepatectomy, except for two articles [38,71]: Schweiger et al. could not find any BRAF mutation in mCRC patients who underwent lung metastasectomy (n = 44) [72]. The large population on lung metastasectomy for BRAF-mutated mCRC (n = 19) was reported by Renaud et al. [71]. There, the median overall survival time of patients with a BRAFV600E mutation was estimated to be 15.0 months (95% CI 12.2–17.8) and the survival rate at 5 years was 0% [71]. Yaeger reported that four patients underwent resection of lung metastases and all had a relapse within 20 months [38]. Thus, none of the reported BRAF-mutated mCRC patients that underwent lung metastasectomy (n = 23) were cured [38,71]. Along with this, these meta-analyses of hepatectomy showed the negative prognostic impact of BRAF mutation on survival, with statistical significance HR 3.06 and 95% CI 1.79–5.20 [68], and HR 3.90 and 95% CI 1.96–7.73 [73]. It is worth noting that these studies included the BRAF V600E and BRAF non-V600E mutations. A recently published study revealed the different prognostic impact between the BRAF V600E and non-V600E mutation in CRLM patients who had undergone hepatectomy. Patients without the BRAFnon-V600E mutation, but with the BRAFV600E mutation, had an association with worse OS (HR 2.76, 95% CI 1.74–4.37, p < 0.001) and DFS (HR 2.04, 95% CI 1.30–3.20, p = 0.002) when compared to the patients with BRAF wild type [64]. As mentioned above, BRAF mutation seems to be associated with distinctive clinicopathological features, such as older age, females, mucinous histology, or right-sided primary tumors. While some of these factors may contribute to survival outcome, due to the small sample size, multivariate analysis could not sufficiently eliminate these confounders. Case-matched analyses were conducted to compensate previous studies, and consistently demonstrated the negative prognostic significance, but outcomes after the relapse varied [64,68]. In contrast, Bachet et al. demonstrated that the BRAF mutation does not have an association with worse DFS [74]. They reported a shorter survival time after relapse in BRAF-mutated mCRC (23.0 months, 95% CI 11.0–35.0) than in the wild type (44.3 months, 95% CI 35.9–52.6) [74]. Metastasectomy maintained a positive impact on survival, both in the presence and absence of the BRAF mutation [65]. The examination of the BRAF status could be recognized as one reliable prognostic value but has not been accepted as a predictive marker in the selection for metastasectomy.
In metastatic disease, the BRAF mutation has been widely accepted to have a strong negative impact on survival [2,3,22,75,76,77,78,79,80]. For those without K-ras mutation, treatment with an anti-EGFR monoclonal antibody (mAb) is the preferred choice; however, the status of BRAF should be considered when evaluating the prognostic value, because BRAF is located downstream of EGFR in the signal transduction pathway. In addition to being a prognostic factor, BRAF mutation will also be a predictive marker for anti-EGFR mAb therapy, which will be further discussed in the next section. In a recently conducted comprehensive analysis by Seigmann and colleagues, they focused on the BRAF-mutated mCRC patients treated using chemotherapy without anti-EGFR mAb. From datasets with a large sample size, they demonstrated the shorter OS of BRAF-mutated mCRC patients (10.8 vs. 16.4 months, HR 1.49 (95% CI 1.23–1.80), p < 0.001). Their result was consistent with the data from the other RCTs in the patients who did not undergo anti-EGFR mAb treatment [78,79,81]. Seligmann et al. showed similar disease control rates and progression free survival (PFS) between BRAF mutant-type and wild-type mCRCs in a first-line treatment setting, however, shorter PFS in the subsequent line and the lower rate of patients received the later-line treatment [2,82]. Thus, the inferior OS of BRAF-mutated mCRC is largely attributable to post-progression survival. [2,82]. However, the shorter PFSs of BRAF-mutated mCRC in first-line treatment were reported in some studies [81,83]. Despite these results being inconsistent with those of the efficacy of the standard doublet first-line regimen, a shorter OS of BRAF-mutated mCRC was consistently reported.
Additionally, the prognostic impact of the BRAF mutation was assessed in the context of its correlation with KRAS, MSI status, and CIMP, which made it difficult to interpret the prognostic impact of the BRAF mutation. An informative study by Phipps and colleagues [84] addressed the associations of the BRAF mutation with KRAS, MSI, and CIMP in a well-organized manner, in mainly resectable-stage CRCs. Their results indicated three key points: (a) MSI-H revealed a better survival impact, even for the BRAF-mutated CRC; (b) both KRAS- and BRAF-mutated CRC had a poor survival impact, but the prognostic impact of KRAS was weaker than that of BRAF; (c) CIMP status could be representative of the BRAF mutation or MSI-H in consideration of the prognostic impact. Therefore, MSI-H comprises a good prognosis group (even better without BRAF mutation), but the non-MSS group increasingly worsened with the KRAS mutation and further, with the BRAF mutation. As mentioned above, BRAF-mutated CRCs often overlap with MSI-H [20,21,22,23,24,25,26,27,28]; therefore, it is important to discuss the association of the BRAF mutation with MSI status in the prognosis of the BRAF-mutated CRC patients [85,86]. In MSS CRCs, a large-scale pooled analysis of prospective randomized trials (n = 3278) pointed out that BRAF-mutated CRC revealed a significantly worse association with OS (HR 1.84, 95% CI 1.14–2.97), but not with RFS (HR 1.36, 95% CI 0.86–2.16) in Stage Ⅱ/Ⅲ disease [45]. Likewise, in the meta-analysis of four clinical trials (n = 3603), statistically significantly worse outcomes were detected when focusing on the proficient mismatch repair (pMMR) (OS: HR 1.94, 95% CI 1.57–2.40, PFS: HR 1.34, 95% CI 1.10–1.64) [25]. Therefore, it seems reasonable to conclude that the BRAF mutation indicates poor prognosis in MSS/pMMR CRC [3,25,28]. In MSI-H CRCs, controversial conclusions were drawn: some studies concluded that the BRAF mutation did not have an association with a poor prognosis in MSI-H/dMMR group CRC [22,25,26,27,28,45,87,88], but the others concluded that the negative impact of the BRAF mutation was observed regardless of MSI/MMR status [24,46,89]. At first glance, these conclusions seem controversial, but the data themselves may not be very different. Due to the small number of BRAF-mutated CRC with MSI-H/dMMR and a favorable prognosis of MSI-H/dMMR, statistical power is to be limited, and these studies might have underestimated the negative prognosis of BRAF-mutated CRCs with MSI-H/dMMR. Although many studies analyzed all stages of CRCs together [22,26,27,87], an inverse effect of the MSI status on survival between the early and metastatic stages should be considered. Namely, MSI-H/dMMR CRCs are positive prognostic markers in Stage Ⅱ/Ⅲ, and negative in the metastatic stage [28]. Thus, the prognostic value of the BRAF mutation with MSI-H/dMMR should be dealt separately between resectable and metastatic stages, in theory; however, in reality, this will divide a small population into small pieces. These are the current technical limitations associated with the prognostic value of BRAF-mutated mCRC with MSI-H /dMMR.
In summary, although clinicians appear to share the idea that the BRAF mutation is associated with poor prognosis, the prognostic impact of the BRAF mutation alone cannot be the only consideration in decision making in clinical practice. Indeed, mandatory BRAF genetic testing was not recommended in the therapeutic guideline released in 2012 [90]. However, the dismal outcomes of BRAF-mutated mCRC patients were always a motivation of those developing therapeutics. As described in following section, the 2016 ESMO consensus guideline recommends the assessment of the BRAF mutation status along with the emergence of therapeutic strategies for BRAF-mutated mCRC patients [91].
5. BRAF Status Required as a Predictive Marker in Clinical Decision Making
Cetuximab (Cmab) and Panitumumab (Pmab) have been shown to have excellent effectiveness for the treatment of chemotherapy-resistant mCRC [92,93,94]. After these two anti-EGFR mAbs emerged in the clinical practice of mCRC, a new era of targeted therapy for the EGF/EGFR signaling pathway began. In 2006, Lievre et al. reported that the KRAS mutation potentially had a predictive value in the treatment of anti-EGFR mAb [95]. A significant role of the KRAS mutation as a negative predictive marker for anti-EGFR mAb had been proven by using tumor samples collected in randomized phase Ⅲ clinical trials. The KRAS mutation had been established as a negative predictor for the anti-EGFR antibody [96,97] and the KRAS mutation had become the first molecular marker for patient selection in the treatment of mCRC. While the KRAS genetic test had a high specificity and nearly 95% of patients harboring the KRAS mutation had no benefit from anti-EGFR mAb, it had insufficient efficacy. Approximately 40–60% of patients with KRAS wild type could not receive a clinical response to anti-EGFR therapy [98].
BRAF plays a key role as the effector molecule of KRAS in the activation of the RAS/RAF signaling pathway. Therefore, researchers focused on the BRAF mutation to elucidate its predictive value for the treatment of anti-EGFR therapy. Retrospective single-arm studies primarily showed that the BRAF mutation might be a negative predictive marker for the efficacy of Cmab or Pmab. No responder of anti-EGFR therapy was found in patients with the BRAFV600E mutation and shorter PFS and OS were observed in the BRAF-mutated patients compared to wild-type patients. These three analyses included a very limited number of BRAF-mutated CRC patients (n = 11, n = 5, and n = 11, respectively) [99,100,101]. The results were reproduced in a larger size cohort. In the KRAS wild-type cohort, BRAF-mutated mCRC patients who received C/Pmab monotherapy or C/Pmab plus chemotherapy had a significantly worse prognosis compared to those without the mutation (overall response rate (ORR): 8.3% vs. 38.0%, median PFS: 8 vs. 26 weeks, HR 3.74, 95% CI 2.44–5.75, p < 0.0001, median OS: 26 vs. 54 weeks, HR 3.03, 95% CI 1.98–4.63, p < 0.0001) [102]. Explorations of the predictive value of the BRAF mutation were conducted using the clinical specimens collected in randomized control trials (RCTs) [103,104,105,106,107,108,109,110,111,112]. Two meta-analyses of RCTs had already been published [108,109] and there were other meta-analyses that contained not only RCTs, but also retrospective studies, in the unselected population [113,114,115,116,117,118]. The former two meta-analyses used almost the same RCT data. Rowland et al. excluded two RCTs—NORDIC and FIRE-3—and included the data of BRAF wild-type patients to evaluate the efficacy of adding anti-EGFR mAb to backbone chemotherapy or the best supportive care [113]. The statistically significant benefits of adding anti-EGFR mAb in OS and PFS were consistently not proven in both Pietrantonio’s study (OS; HR 0.91, 95% CI 0.62–1.34) and Rowland’s study [113,119]. However, they drew the different conclusions. Pietrantonio et al. simply supported to avoid the administration of anti-EGFR for BRAF-mutated mCRC patients [119]. Rowland et al. pointed out not there were insufficient data to discard anti-EGFR mAbs from BRAF-mutated mCRC patients [113]. The relatively favorable trends of adding anti-EGFR mAbs were seen in a first-line setting compared to the later line. Both OS and PFS HRs were derived from the three RCTs, PRIME, and a pooled analysis of CRYSTAL and OPUS, were 0.90 (95% CI 0.46–1.16) and 0.58 (95% CI 0.29–1.15) (PRIME) and 0.62 (95% CI 0.36–1.06) and 0.67 (95% CI 0.34–1.29) (CRYSTAL and OPUS) [107,113,114]. The mutation analysis was prospectively conducted in the PRIME study and these RCTs were well designed and regarded as reliable data. On the other hand, the detrimental effect of adding Pmab to irinotecan for the treatment of KRAS wild/BRAF mutant mCRC patients in a second line setting was reported [110]. Based on these results, guideline members of CRC in the European Society of Medical Oncology (ESMO) committee concluded there was insufficient evidence to exclude anti-EGFR therapy for patients with BRAF mutant disease [92]. However, a meta-analysis of the effect of anti-EGFR therapy in a first-line setting demonstrated that a significantly decreased response rate was observed in BRAFV600E-mutated mCRC compared to BRAF wild-type [120]. Van Brummelen et al. reviewed eight meta-analyses, including RCTs and studies conducted in an unselected population [112,113,114,115,116,117,118,119,120,121]. They showed that the clinical benefit from anti-EGFR therapy for BRAF-mutated mCRC patients could not be found in terms of OS, PFS, and ORR [121]. Moreover, seven of eight meta-analyses other than Rowland’s demonstrated the statistically significant inferiority of anti-EGFR therapy in BRAF-mutated mCRC compared to BRAF wild type.
In the same period, the clinical utility of the BRAF mutation status came to be recognized in terms of another clinical aspect. The TRIBE study demonstrated the efficacy and safety of the FOLFOXIRI + Bevacizumab (BV) regimen and this triplet regimen came to be one of the standard treatments in mCRC [122,123]. Due to severe toxicity, the triplet regimen was considered to be the optimal treatment choice for select patients with aggressive tumors who expected to fail to receive second-line therapy after disease progression. BRAF-mCRC would be recognized as a tumor which had these characteristics. Phase Ⅱ study data of FOLFOXIRI + BV showed encouraging results in terms of the clinical outcome (RR: 72%, median PFS: 11.8 months, and median OS: 24.1 months) for patients with the BRAF mutation [124]. Although significant differences in OS, PFS, and ORR could not be observed between patients in the FOLFOXIRI + BV and FOLFIRI + BV group of the TRIBE phase Ⅲ study [125], the median survival time of the experimental group was reported to be 19.0 months, which was numerically longer than for BRAF-mutated mCRC patients treated in previous clinical trials (10–15 months) [24,75,79]. Notably, a recent analysis on the prognosis of BRAF-mutated mCRC demonstrated a significantly lower rate (33% vs. BRAF wild-type 51%, p < 0.001) for patients who received second-line chemotherapy after disease progression [2]. As mentioned above, a shorter PFS in the first-line group and post-progression survival (PPS) after the first-line treatment were also rationale for using all the key drugs, including 5-FU, oxaliplatin, and irinotecan, in the initial treatment [2,78]. That is why treatment guidelines encouraged such an up-front aggressive treatment to be considered for BRAF-mutated mCRC in clinical practice worldwide [92,126,127].
The cancer precision medicine era became a tailwind in raising awareness of the significance of BRAF-mutated CRC in clinical practice. A low incidence of the BRAF mutation had been the critical hazard preventing BRAF gene testing from entering clinical practice. Next generation sequencing (NGS) technology opened the door for comprehensive molecular analyses of cancer genomes with much higher speed and lower costs [128]. A gene mutation that recurrently appears in cancer genomes can be considered as a “driver mutation” candidate and is, therefore, a target in the precision medicine era. Clinical sequencing in the search for the driver genetic alterations has been widely conducted [6,7,129], and molecular targeting agents, mainly inhibitors, have been developed to suppress these. To overcome the low incidence, umbrella- or basket-type clinical trials enable a patient with a rare driver mutation in a specific organ to efficiently receive the targeted therapy [129], including mCRC patients with the BRAF mutation. BRAF gene testing had reached the bedside from the bench-side in the wind of cancer precision medicine.
In summary, although the BRAF mutation was shown to have a potential negative predictive value for treatment with anti-EGFR antibody, evidence was insufficient to make BRAF gene testing mandatory like RAS [130,131]. In the same period, several studies demonstrated that patient selection according to KRAS, NRAS, BRAF, and PIC3CA mutation could enrich the efficacy of molecular targeted therapy [102,132,133]. The BRAF mutation was one of these negative predictors, along with the EGFR pathway. After the success of the TRIBE trial, the triplet regimen emerged as one of the treatment options for aggressive types of CRCs, including BRAF-mutated ones. Thereby, the BRAF mutation is considered to be an actionable genetic alteration in clinical practice. However, BRAF-mutated CRCs had some associations with unfavorable clinical factors for the toxic regimen, such as elderly patients or peritoneum metastasis. Therefore, BRAF-mutated patients who actually received the triplet regimen were limited to a highly select population. Specific therapy targeting the BRAF mutation was urgently awaited.
6. BRAF Became a Targetable Molecule in mCRC Treatment
The great success of BRAFV600E targeting therapy in melanoma repositioned the BRAFV600E mutation from being a prognostic marker to targetable genetic alteration. In retrospect, the history of BRAFV600E targeting therapy had indeed begun in 2000, before the first reports on the BRAF mutation in human cancer were launched. Sorafenib entered clinical trials as the first RAF inhibitor aimed to treat RAS-mutated cancers. However, Sorafenib was a less potent BRAFV600E inhibitor because it preferentially bound to the inactive enzyme conformation [8]. The second generation of ATP-competitive RAF inhibitors, e.g., PLX4032 (vemurafenib), which selectively bound to the active form, were developed in 2008, which opened the door to the development of BRAFV600E targeting therapy [134]. In 2010, the result of a phase Ⅰ study on vemurafenib were published for the treatment of BRAFV600E-mutated metastatic melanoma [135]. A phase Ⅱ study demonstrated promising results, and the ORR reached 53% [136]. In 2011, vemurafenib was shown to have improved ORR and PFS compared with a standard treatment (dacarbazine) in a phase Ⅲ RCT, leading to the approval of the US Food and Drug Administration (FDA) [137]. Through these trials for melanoma, BRAFV600E-targeting agents became available in clinical practice.
Dissimilar to melanoma, however, the efficacy of vemurafenib was not reproduced in the treatment of BRAFV600E-mutated mCRC. A phase II study showed disappointing results, with an ORR of 5% (95% CI < 1–26), median PFS of 2.1 months (95% CI 1.8–3.6 months), and median OS of 7.7 months (95% CI 3.4–11.6 months) [138]. Observations in melanoma indicated that a profound inhibition (>80%) of the phosphorylation of ERK is required to obtain sufficient levels of clinical response with the BRAF inhibitor [139], and thus a modest inhibition of the RAF–MAPK pathway is related to the lack of efficacy in BRAFV600E-mutated mCRC treated with vemurafenib alone. Preclinical studies of mCRC revealed how BRAFV600E tumors could alleviate the suppression of this signal transduction by the BRAF inhibitor, and suggested how this resistance could be overcome.
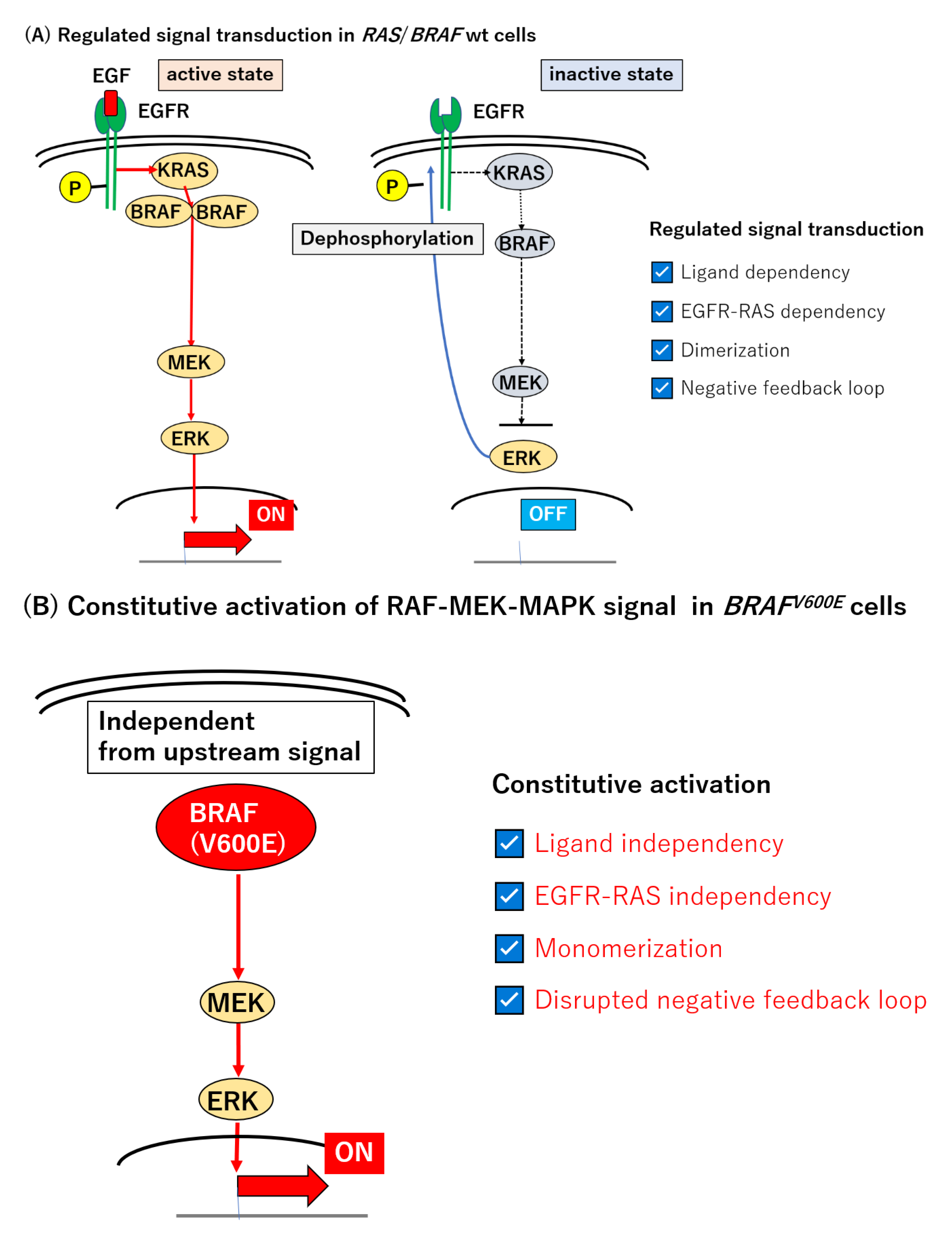
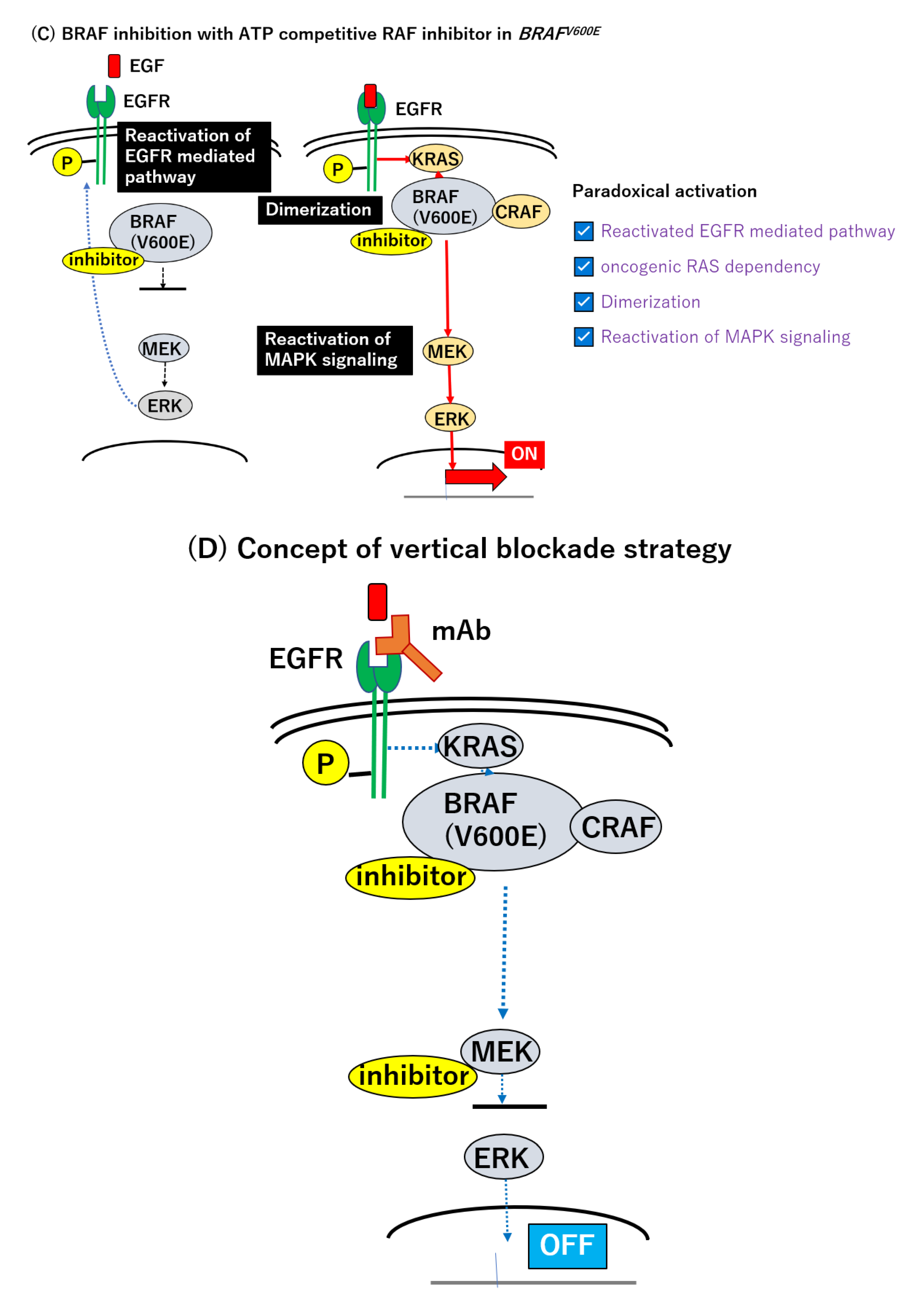
The MAPK signal transduction pathway, including RAS and BRAF, is normally regulated through several levels of feedback loops involving activated, phosphorylated ERK (pERK) [135,136,137,138,139,140,141,142]. Epidermal growth factor (EGF) binds to its specific receptor (EGFR) and initiates the signal transduction of this pathway. Activated RAS induces the dimerization of RAFs which are capable of phosphorylating downstream effectors, MEK and ERK [143,144,145,146]. The resulting pERK stimulates a subset of gene expression, but also inactivates EGFR and attenuates this signal transduction pathway [8,9] (Figure 1A). By contrast, in BRAFV600E-mutated tumors, the MEK–ERK axis is constitutively active, in a manner independent of the RAS-mediated dimerization of RAF [9,144], and is thereby refractory to the negative feedback circuit in this type of tumor (Figure 1B).
The use of an ATP-competitive BRAF kinase inhibitor, such as vemurafenib, revealed a transient suppression of the signal transduction and p-ERK levels [8,9,137]; however, the p-ERK level was recovered in the BRAF mutant cell line within 24 h [147]. The suppression of pERK reduces the power of the negative feedback circuit and preserves the activity of EGFR. This paradoxically activates RAS and the MEK–MAPK signaling axis, through the direct activation of another class of RAF, CRAF, or by facilitating BRAF–CRAF heterodimer formation [148,149,150,151,152,153,154,155] (Figure 1C). Given these alterations, a combinatory intervention of BRAF and EGFR and/or MEK seems promising [142,152] (Figure 1D). Corcoran et al. assessed the combined inhibition with dabrafenib (BRAF) and trametinib (MEK) in the treatment of BRAF-mutated mCRC. Among 43 patients, five patients achieved a partial or complete response and the median PFS was 3.5 months (95% CI 3.4–4.0 months) [155]. Compared to the BRAF inhibitor alone or standard chemotherapy, the dual MAPK signal pathway blockade using the BRAF and MEK inhibitors demonstrated modest efficacy [83,136,155]. The insufficient suppression of MAPK signaling was thought to be attributable to the limited response to the BRAF inhibitor [155]. Yaeger et al. conducted a pilot study to elucidate another dual blockade of the RAF–MEK–MAPK signaling pathway with Pmab and vemurafenib in the treatment of BRAFV600E-mutated mCRC [156]. For 12 patients treated with target lesions, only a subset of patients (n = 2) achieved a partial response (RR: 13%). The median PFS and OS were 3.2 months (95% CI 1.6–5.3 months) and 7.6 months (95% CI 2.1—not achieved months), respectively, and were still unsatisfactory [156].
Subsequently, another BRAF inhibitor, encorafenib, was developed and demonstrated encouraging results when combined with Cmab in BRAF-mutated mCRC patients [157]. The ORR was 19.2% and the median duration of response was 46 weeks in the doublet regimen (encorafenib and Cmab) group [157]. The first BRAFV600E targeting therapy was established by the positive results of the BEACON CRC trial [4,5]. The BEACON CRC trial was conducted for previously treated cases of BRAFV600E-mutated mCRC. Patients were assigned to three groups, and the effectiveness and safety of the triplet-therapy group (encorafenib, binimetinib, and Cmab), and the doublet-therapy group (encorafenib and Cmab) were compared with the control group (Cmab + FOLFIRI or irinotecan). The primary endpoints were the OS and ORR of the triplet-therapy group, and secondary endpoints these of the doublet-therapy group [5]. The median OS was 9.0 months in the triplet-therapy group vs. 5.4 months in the control group (HR 0.52, 95% CI 0.39–0.70). The median OS in the doublet-therapy group was calculated to be 8.4 months (HR was 0.60, 95% CI 0.45–0.79) [5]. A significant improvement in ORR was also observed in the triplet-therapy group (26%, 95% CI 18–35% vs. 2%, 95% CI 0–7%; p < 0.001) [5]. Besides, an exploration of up-front use of the triplet therapy, titled ANCHOR CRC, is currently ongoing [158].
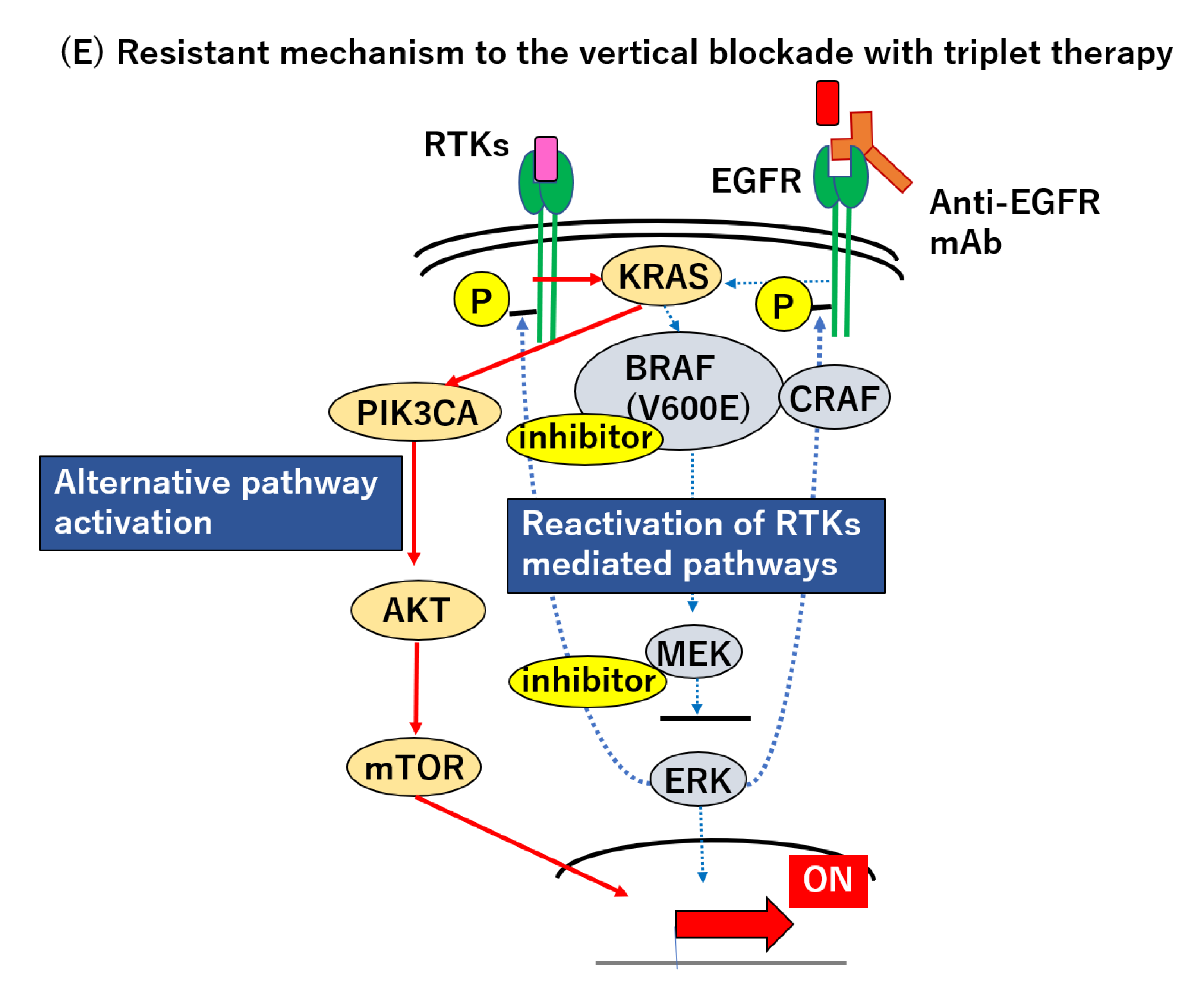
Thus, the BRAF mutation has been changed from a merely prognostic marker to a targetable gene mutation over the past two decades. Triplet therapy can be the first specific treatment for BRAFV600E-mutated mCRC, but there are several issues with this novel strategy that need to be resolved. First, whether MEK inhibitor is the optimal partner for BRAF inhibitor and anti-EGFR antibody should be addressed, because the PI3K/AKT signaling pathway exists downstream of receptor tyrosine kinases (RTKs), as well as the RAS–RAF–MEK–MAPK pathway, and there are interactions between these two downstream axes. The activation of the PI3K/AKT pathway is known to be involved in the mechanism of resistance to the BRAF inhibitor [151,155] (Figure 1E). A colorectal cancer cell line with the PIK3CA mutation or PTEN loss is more resistant to the BRAF inhibitor than wild-type cells. Mao et al. reported that the combination of a BRAF and PI3K inhibitor revealed synergistic anti-tumor activity in vitro and vivo [159,160]. A phase Ⅰ study of encorafenib and Cmab with alpelisib (a PI3Kα inhibitor) showed promising clinical outcomes (ORR: 17.9%, median PFS; 4.2 months, 95% CI; 4.1–5.4 months) [157]. Another observation questioning the combination is that triplet therapy using vemurafenib, Cmab, and irinotecan revealed favorable results in an early-phase clinical trial [161]. For 17 patients with BRAFV600E-mutated mCRC treated by triplet therapy, 14 patients (82.3%) exhibited tumor shrinkage and the ORR reached 35% (95% CI; 14–62%) [161]. This result indicated that irinotecan could be a candidate for treatment in combination with a BRAF inhibitor and anti-EGFR therapy. Moreover, a direct inhibition of ERK would potently suppress MAPK reactivation, regardless of the upstream signal [9,162]. Recently, Hazar-Rethinam et al. reported attractive results in vitro, demonstrating that convergent therapy using the ERK inhibitor could simultaneously overcome multiple heterogeneous resistant mechanisms. They proposed a novel up-front concept which can in theory eradicate the minority of resistant subclones that preexist in the population. Notably, their real-time cfDNA monitoring experiment demonstrated that triplet therapy targeting BRAF, EGFR, and ERK could potently suppress the outgrowth of subclones harboring RAS or MEK mutations, more strongly than the combination of BRAF, EGFR, and MEK inactivation [163]. This novel combination could lead to improved outcomes compared to those of the BEACON regimen; however, the treatment might also affect cells without the BRAF mutation. An anti-programed cell death 1 (PD-1) antibody could serve as a partner agent with a BRAF inhibitor and anti EGFR mAb. Recently, Corcoran et al. demonstrated the early results of their clinical trials (NCT03668431) using dabrafenib, trametinib and spartalizumab (anti-PD-1 antibody) in BRAFV600E-mutated mCRC patients at the ESMO World Congress on GI Cancers held in July 2020 [158]. They revealed promising data, i.e., ORR of 33%, in the patients with MSS (n = 17) and MSI-H (n = 8), which was superior to the previous result [158] (ORR 12%, dabrafenib and trametinib). Interestingly, this combination therapy was also effective for MSS CRC patients. This will raise the question of whether the anti-EGFR mAb or anti-PD-1/PD-L1 antibody is the preferred partner for the BRAF and MEK inhibitors. Further investigations for optimal combinations await.
Second, we should also pay attention to the toxicities by adding an MEK inhibitor and ask whether the clinical benefit still outweighs any negative side effects. The BEACON trial, while revealing the superiority of triplet therapy compared to the control (Cmab + FOLFIRI or irinotecan), could not evaluate the benefit of the triplet regimen over the doublet regimen for statistical reasons [5]. The following analysis of the BEACON trial reported the superiority of the triplet regimen in the ORR (27% vs. 20%, which was consistent with the previous report, but the median survival time was identical (9.3 months) between the triplet and doublet regimen [5,164]. Whereas adverse events, such as headache, musculoskeletal pain, arthralgia, and myalgia occurred frequently in the doublet group, gastrointestinal toxicities, such as diarrhea, nausea, and vomiting, were more frequently seen in the patients treated with the triplet therapy [5,164]. Although differences in the toxicity profile did not affect the treatment continuation or intensity [5], cases with severe headaches, musculoskeletal pain, arthralgia, and myalgia (grade ≥ 3) were rare (>1%) and severe-grade diarrhea was observed in 10% of patients with triplet therapy. Thus, the doublet therapy appears to be a less toxic regimen than triplet therapy. Corcoran et al. reported that the triplet therapy (dabrafenib (BRAF) + Pmab + trametinib (MEK)) showed a higher ORR (21% vs. 10% for doublet) and better tumor shrinkage than the doublet therapy (dabrafenib + Pmab) [165]. However, in terms of the disease control rate (DCR) and PFS, numerically similar results were observed for triplet (DCR: 86%, median PFS: 4.2 months) and doublet therapy (DCR: 90%, median PFS: 3.5 months) [165]. Considering these results, triplet therapy is not necessarily accepted as a standard regimen worldwide. In fact, according to the up-date results of the BEACON CRC study, the numerical difference of the ORR between the triplet (27%) and doublet (20%) were preserved, but the difference in OS was not observed. The principle investigator of this trial declared that only the doublet therapy for BRAF-mutated mCRC was considered to proceed for FDA approval [164], and triplet therapy would not be an option for all BRAFV600E-mutated mCRCs. Finally, in April 2020, the FDA approved encorafenib in combination with cetuximab for BRAFV600E-mutated mCRCs [166]. A careful assessment of patients in selecting triplet or doublet therapy is needed.
Third, the efficacy of triplet therapy might be modified by the MSI status. Among the patients treated with triplet therapy, the response rate of patients with MSI-H/dMMR tumors was 46% (95% CI 17–77%) and higher than that of MSS/pMMR (27%, 95% CI 17–77%). The PFS of patients with MSI-H/dMMR tumors exhibited a trend toward longer survival compared with that of MSS/pMMR (HR 2.62, 95% CI 1.00–6.91, p = 0.045) [165]. In addition, the MSI-H/dMMR tumor itself had already been established as a predictive biomarker in patient selection for anti-PD1 therapy [167,168,169]. Due to the very limited number of cases of BRAF-mutated MSI-H mCRC patients, it is presently too early to conclude whether the effectiveness of BRAF targeting therapy is affected by the BRAF status.
How can we possibly improve upon the vertical blockade strategy? Initially, insufficient suppression of the RAS–RAF–MEK–MAPK pathway, as described above, was thought to account for the unsatisfying results with the vertical blockade; however, pharmacodynamic analysis of paired tumor specimens, before and after treatment, revealed that the degree of MAPK pathway suppression is not correlated with the clinical outcomes [165]. On the one hand, doublet therapy with trametinib and Pmab (T+P) could reduce the pERK level significantly, but no responder to this doublet regimen was found. On the other hand, doublet therapy with dabrafenib and Pmab (D+P) could not reduce p-ERK sufficiently and the median p-ERK level of the D+P regimen was higher than that of T+P. Despite the weaker suppression of the MAPK signaling pathway, a higher response rate (10% vs. 0%) and longer PFS (3.5 months vs. 2.6 months) were observed in patients treated with the D+P regimen for unknown reasons [165]. Western blotting analysis of the phosphorylation of MEK or ERK may not be the right assay to evaluate the activity of this RAS–RAF–MEK–MAPK pathway. The plastic and reversible nature of this pathway makes it difficult to overcome the associated malignancy. Resistance can be caused by the compensatory reactivation of the MAPK pathway, through the acquisition or preexistence of RTK amplification (not only EGFR, but also HER2, HER3 or MET), RAS mutation or RAS amplification, BRAF amplification, and MEK mutation, which could cause resistance to the BRAF inhibitor [8,9,151,163,165,170,171,172,173]. For instance, while the BRAF and RAS mutation are initially found in a mutually exclusive manner, these tumors additionally acquire NRAS or KRAS mutations after vemurafenib treatment, as indicated by the analysis of their circulating tumor DNA (ctDNA) [138]. In addition, Pietrantonio and Oddo et al. reported the case that combination therapy with crizotinib (MET inhibition) could transiently overcome the acquired resistance after BRAF inhibition, but MET hyper-amplification emerged as a second acquired resistance [172,173]. It seems therefore that the heterogeneous and plastic nature of the RTK signaling pathway prevents us from conquering this malignancy.
Paradoxically, however, these alterations underlying adaptive resistance can be toxic in the absence of treatment. A preclinical study of melanoma with BRAF-mutation indicated that cells with the acquired upregulation of EGFR expression were induced by using a BRAF inhibitor, but these cells became vulnerable when the treatment was ceased. The hyperactivated state of the RAS–RAF–MEK–MAPK pathway induced by the overexpression of EGFR led the cells into oncogene-induced senescence when the BRAF inhibitor was deprived [174]. The “addiction” to the BRAF inhibitor led to successful re-challenge cases of BRAF inhibition, i.e., the restored sensitivity, after a drug holiday [175]. Thus, using the optimal method and timing to evaluate the activity of this signaling pathway seems to be an important issue, and its “real-time monitoring” should be useful.
In summary, a novel triplet therapy with encorafenib, binimetinib, and Cmab emerged as the targeting therapy for BRAFV600E-mutated mCRC and has been used since 2020. Given the presence of specific treatment in clinical practice, BRAFV600E-mutated mCRC has become an independent subset of mCRCs. The constitutive activation of RAF–MEK–MAPK signaling is central to supporting the survival of BRAF-mutated cells in mCRC. Unlike melanoma, BRAF inhibition alone revealed limited efficacy, and acquired the alteration-mediated reactivation of the MAPK pathway which underlies the resistance mechanism to BRAF inhibitors. Therefore, comprehensive regulation of this pathway is required to conquer BRAFV600E-mutated mCRC. Bearing this in mind, a vertical blockade of signal transduction is a promising way to achieve a clinical response in mCRC but it still needs improvement. These resistance mechanisms seem to stem from the plastic and diverse nature of the RAS–RAF–MEK–MAPK pathway. Moreover, cancer cells opt to use signaling networks outside the RAF–MEK–MAPK pathway in an attempt to evade the vertical blockade strategy. The strategy to completely and effectively control BRAF-mutated mCRC is yet to be developed.
7. Future Perspectives on BRAF-Mutated mCRC and Beyond
Recently, experts in this field have paid attention to the heterogeneity of BRAF-mutated mCRC. All BRAF-mutated mCRCs do not necessarily belong to the same subset of mCRCs, and there are several variations in terms of DNA sequencing, RNA expression, kinase activity, clinicopathological features, sensitivity to anti-EGFR therapy, and prognosis. In this final chapter, we would like to describe the future perspectives, focusing on the accumulating data on the variations of BRAF-mutated mCRCs.
One of the explorations on the heterogeneity of BRAF-mutated CRCs was focused on the outside of codon 600 of BRAF—the BRAFnon-V600E mutation. More than 1000 unique BRAF mutations have been previously described in patients with various malignancies [176]. Recent advances in NGS technology have found several variants of the BRAFnon-V600E mutation, which account for approximately 2% of mCRCs. There are several differences in the clinicopathological features and prognosis between V600E and non-V600E mutations [177,178,179,180]. Patients with BRAFnon-V600E mutations were found to be younger, have left-sided primary disease, have a non-mucinous histology, and have less peritoneum metastasis compared to those with BRAFV600E mutations. Moreover, different molecular features were also reported for BRAFnon-V600E and BRAFV600E mutations. BRAFnon-V600E mutations had less association with MSI-H tumors, and some BRAFnon-V600E-mutated CRCs even had a co-occurrence with RAS mutations [177,178,179,180]. Not all these rare variants of BRAF mutations had been proven to have oncogenic activities in vivo/vitro. Constitutive activation of the RAF–MEK–MAPK pathway is thought to be an essence of the malignant nature of BRAFV600E mutations. However, kinase activity toward the phosphorylation of the MAPK pathway is impaired or even lost in some BRAFnon-V600E-mutated CRCs [144,181]. Oncogenic RAS is required for kinase-dead BRAF to drive tumor progression [151]. Recently, the novel classification of BRAF mutations based on kinase activity was proposed, including class 1 (activating RAS-independent BRAF mutations signaling as monomers), class 2 (activating RAS-independent BRAF mutations signaling as dimers with CRAF), and class 3 (RAS-dependent BRAF mutations with impaired kinase activity or kinase-dead) [182,183,184]. This proposal was, to some extent, clinically accepted to reflect the sensitivity to anti-EGFR antibodies. Patients with class 3 BRAF mutations potentially respond to anti-EGFR therapy [182,184].
Gene expression is controlled by several factors in terms of genomic and epigenomic aspects. Classification by gene expression analyses was thought to be the consequence of these complexities. Therefore, categorization based on gene expression could have more links to tumor behaviors and identify more biologically homogeneous subgroups than DNA sequencing. Previously, several studies have reported that classifications based on gene expression analyses have associations with clinicopathological features, predictions for treatment, or prognosis in other cancers [185,186,187,188]. Recently, the Colorectal Cancer Subtyping Consortium (CRCSC) suggested four consensus molecular subtypes (CMSs) of CRCs based on international transcriptomic data at the largest scale [189]. In their subtyping, BRAF-mutated CRCs were more enriched (>70%) in CMS1, which is characterized by high immunogenicity with a better prognosis. However, more than half of CMS1 cases were composed of BRAF wild CRCs. More recently, Barres et al. segregated BRAFV600E-mutated CRCs into two subtypes, called BRAF mutation (BM) 1 and 2, based on a gene expression analysis using a dataset of 218 BRAFV600E-mutated CRC patients. The BM1 subtype is highly active in KRAS/mTOR/AKT/4EBP1 signaling and the BM2 subtype is associated with cell cycle check point-related genes [190]. In addition, a recent study showed that the BM1 subtype was more sensitive to the triplet therapy with dabrafenib, trametinib, and panitumumab, and had better clinical outcomes compared to the treatment of the BM2 subtype. The BM subtype was an independent predictive factor in the multivariate analysis that includes other immune-related signatures [191]. Whether the BM subtyping is a robust biomarker, it requires future validation to be determined. This result indicated the transcriptional context could affect the significance of gene mutation. A paradigm shift from “one-gene, one-drug” based on a single driver mutation to “multi-gene, multi-drug”, which is expected regarding the future perspective of precision medicine [192].
Other approaches using gene expression data have been conducted to define the BRAF mutation signature and identify the subgroup of CRCs with BRAF-like malignant potential, without, having the BRAF mutation itself, in melanoma and breast cancer ahead of CRC [192,193,194]. Tian et al. reported that BRAF-mutated CRCs displayed more distinctive expression patterns than those of KRAS and PIK3CA mutations [195]. Popovici et al. identified BRAF-mutant like CRCs in KRAS mutations or double wild-type patients, with a poor prognosis similar to that of BRAF-mutated CRC patients [196]. Furthermore, Vecchione et al. conducted a functional analysis of BRAF-mutant-like cell lines and discovered the common vulnerability that the loss of RANBP2 was lethal to BRAF-mutant-like cells. In addition, they demonstrated the sensitivity of BRAF-mutant-like cells to vinorelbine in vitro and vivo. Surprisingly, they obtained an archival sample of the super responder which was enrolled in the clinical trial of vinorelbine for CRC in the 1990s. Notably, that tumor showed a BRAF-mutant-like expression pattern [197].
Moreover, the heterogeneity of BRAF-mutated CRCs has been reported in several studies by more practical and easily available methods, such as the immunohistochemistry of clinicopathological features. Several studies have reported the differences among BRAF-mutated CRCs in the methylation phenotype (CIMP-high and CIMP-low), expression of the cytokeratin (CK7 and CK20), the transcription factors (CDX2) and immunohistochemical (IHC)-based CMS classification [198,199,200,201,202]. Furthermore, Loupakis et al. suggested a more practical classification method by using data which were easily available in daily practice, such as performance status (PS) and laboratory data only. Interestingly, they revealed that the prognosis of BRAF-mutated CRCs was clearly divided according to their clinical subtyping [203]. These results indicated that BRAF-mutated CRCs were not one disease but that there was inter-tumor heterogeneity among BRAF-mutated CRCs.
In summary, several researchers have reported the heterogeneity of BRAF-mutated CRCs. Patients with BRAFnon-V600E mutations have different clinicopathological features compared to those with BRAFV600E mutations. Moreover, they could benefit from anti-EGFR antibodies. Different kinase activities of V600E and non-V600E in the RAF–MEK–MAPK pathway could explain the sensitivity to anti-EGFR therapy. Classification based on gene expression analysis could broaden the horizon of therapeutic targets for BRAF-mutant-like CRCs without any BRAF mutations. Currently, the results of these phenotyping studies are not consistent.
8. Summary and Conclusions
Since the first report of the BRAF mutation in human cancer was published in 2002, nearly two decades ago, the significance of BRAF-mutated CRC has been established in clinical practice, changing from being merely a prognostic biomarker marker, via being considered a moderate predictive marker for anti-EGFR therapy and actionable genetic alteration, and toward becoming a targetable mutation. As described in this review, cancer precision medicine based on driver mutations has accelerated the emergence of BRAF-mutated CRCs from basic research to clinical practice. Several research studies on the resistance mechanism of BRAF targeting therapy have demonstrated the importance of a profound understanding of the RAS–RAF–MEK–MAPK pathway in conquering this malignant tumor. Therefore, especially in CRC, we should recognize the therapeutic target as being not only the BRAF mutation alone, but also the entire RAS–RAF–MEK–MAPK signaling pathway. Combination therapy is necessary to overcome the resistance mechanism associated with multiple genes (Figure 2).
The BRAF mutation is also a tumor agnostic genetic alteration and therefore it could become targetable, regardless of the tumor origin. Indeed, current precision medicine based on the actionable genetic alteration has precisely attacked the target, but it cannot always predict the tumor’s Achilles heel. Driver mutation-guided clinical trials could provide additional therapeutic options for selecting patients, but these efficacies are far from being satisfactory. Inter- and intra-tumor heterogeneity always arises as a hazard in the treatment of BRAF-mutated CRCs. Several findings have indicated the variety and plasticity of this type of tumor which underly the resistant mechanisms. The variety and plasticity are derived from the mechanism acquired by normal cells to adapt to their changing environments for surviving at their original site. Therefore, understanding their tissue-specific natures is necessary for defeating this malignancy. Further investigations into the nature of the origin, including the surrounding immune cells, represent the future direction for the next developments in optimal precision medicine.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Li, W.Q.; Kawakami, K.; Ruszkiewicz, A.; Bennett, G.; Moore, J.; Iacopetta, B. BRAF mutations are associated with distinctive clinical, pathological and molecular features of colorectal cancer independently of microsatellite instability status. Mol. Cancer 2006, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seligmann, J.F.; Fisher, D.; Smith, C.G.; Richman, S.D.; Elliott, F.; Brown, S.; Adams, R.; Maughan, T.; Quirke, P.; Cheadle, J.; et al. Investigating the poor outcomes of BRAF-mutant advanced colorectal cancer: Analysis from 2530 patients in randomized clinical trials. Ann. Oncol. 2017, 28, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Garcia, E.; Argiles, G.; Elez, E.; Tabernero, J. BRAF mutant colorectal cancer: Prognosis, treatment, and new perspectives. Ann Oncol. 2017, 28, 2648–2657. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Huijberts, S.; Grothey, A.; Yaeger, R.; Cuyle, P.J.; Elez, E.; Fakih, M.; Montagut, C.; Peeters, M.; Yoshino, T.; et al. Binimetinib, Encorafenib, and Cetuximab Triplet Therapy for Patients with BRAF V600E-Mutant Metastatic Colorectal Cancer: Safety Lead-In Results from the Phase III BEACON Colorectal Cancer Study. J. Clin. Oncol. 2019, 37, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Kopetz, S.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Desai, J.; Yoshino, T.; Wasan, H.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N. Engl. J. Med. 2019, 381, 1632–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef] [PubMed]
- AACR Project GENIE Consortium. AACR Project GENIE: Powering precision medicine through an international consortium. Cancer Discov. 2017, 7, 818–831. [Google Scholar] [CrossRef] [Green Version]
- Holderfield, M.; Deuker, M.M.; McCormick, F.; McMahon, M. Targeting RAF kinases for cancer therapy: BRAF-mutated melanoma and beyond. Nat. Rev. Cancer 2014, 14, 455–467. [Google Scholar] [CrossRef] [Green Version]
- Yaeger, R.; Corcoran, R.B. Targeting Alterations in the RAF-MEK Pathway. Cancer Discov. 2019, 9, 329–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaman, A.; Wu, W.; Bivona, T.G. Targeting Oncogenic BRAF: Past, Present, and Future. Cancers 2019, 16, 1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, C.E.; Whitehall, V.L.J. How the BRAF V600E Mutation Defines a Distinct Subgroup of Colorectal Cancer. Gastroenterol. Res. Pract. 2018, 2018, 9250757. [Google Scholar] [CrossRef] [Green Version]
- Ng, J.Y.; Lu, C.T.; Lam, A.K. BRAF MUTATION: Current and Future Clinical Pathological Applications in Colorectal Carcinoma. Histol. Histopathol. 2019, 34, 469–477. [Google Scholar] [PubMed]
- Caputo, F.; Santini, C.; Bardasi, C.; Cerma, K.; Casadei-Gardini, A.; Spallanzani, A.; Andrikou, K.; Cascinu, S.; Gelsomino, F. BRAF-Mutated Colorectal Cancer: Clinical and Molecular Insights. Int. J. Mol. Sci. 2019, 20, 5369. [Google Scholar] [CrossRef] [Green Version]
- Clarke, C.N.; Kopetz, E.S. BRAF mutant colorectal cancer as a distinct subset of colorectal cancer: Clinical characteristics, clinical behavior, and response to targeted therapies. J. Gastrointest. Oncol. 2015, 6, 660–667. [Google Scholar]
- Taieb, J.; Lapeyre-Prost, A.; Puig, P.L.; Zaanan, A. Exploring the best treatment options for BRAF-mutant metastatic colon cancer. Br. J. Cancer 2019, 121, 434–442. [Google Scholar] [CrossRef]
- Afrăsânie, V.A.; Marinca, M.V.; Alexa-Stratulat, T.; Gafton, B.; Păduraru, M.; Adavidoaiei, A.M.; Miron, L.; Rusu, C. KRAS, NRAS, BRAF, HER2 and microsatellite instability in metastatic colorectal cancer—practical implications for the clinician. Radiol. Oncol. 2019, 53, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Rapp, U.R.; Goldsborough, M.D.; Bonner, T.I.; Groffen, J.; Reynolds, F.H., Jr.; Stephenson, J.R. Structure and biological activity of v-raf, a unique oncogene transduced by a retrovirus. Proc. Natl. Acad. Sci. USA 1983, 80, 4218–4222. [Google Scholar] [CrossRef] [Green Version]
- Jansen, H.W.; Ruckert, B.; Lurz, R.; Bister, K. Two unrelated cell-derived sequences in the genome of avian leukemia and carcinoma inducing retrovirus MH2. EMBO J. 1983, 2, 1969–1975. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Zhou, Y.; Li, P.; Chen, F.; Chen, H.; Xia, D.; Xu, E.; Lai, M.; Wu, Y. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, H.; Bardelli, A.; Lengauer, C.; Kinzler, K.W.; Vogelstein, B.; Velculescu, V.E. Tumorigenesis: RAF/RAS oncogenes and mismatch-repair status. Nature 2002, 418, 934. [Google Scholar] [CrossRef]
- Kambara, T.; Simms, L.A.; Whitehall, V.L.; Spring, K.J.; Wynter, C.V.; Walsh, M.D.; Barker, M.A.; Arnold, S.; McGivern, A.; Matsubara, N. BRAF mutation is associated with DNA methylation in serrated polyps and cancers of the colorectum. Gut 2004, 53, 1137–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samowitz, W.S.; Sweeney, C.; Herrick, J.; Albertsen, H.; Levin, T.R.; Murtaugh, M.A.; Wolff, R.K.; Slattery, M.L. Poor survival associated with the BRAF V600E mutation in microsatellite-stable colon cancers. Cancer Res. 2005, 65, 6063–6069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saridaki, Z.; Papadatos-Pastos, D.; Mavroudis, D.; Bairaktari, E.; Arvanity, H.; Stathopoulos, E.; Georgoulias, V.; Souglakos, J. BRAF mutations, microsatellite instability status and cyclin D1 expression predict metastatic colorectal patients’ outcome. Br. J. Cancer 2010, 102, 1762–1768. [Google Scholar] [CrossRef] [Green Version]
- Tran, B.; Kopetz, S.; Tie, J.; Gibbs, P.; Jiang, Z.Q.; Lieu, C.H.; Agarwal, A.; Maru, D.M.; Sieber, O.; Desai, J. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer 2011, 117, 4623–4632. [Google Scholar] [CrossRef] [Green Version]
- Venderbosch, S.; Nagtegaal, I.D.; Maughan, T.S.; Smith, C.G.; Cheadle, J.P.; Fisher, D.; Kaplan, R.; Quirke, P.; Seymour, M.T.; Richman, S.D. Mismatch repair status and BRAF mutation status in metastatic colorectal cancer patients: A pooled analysis of the CAIRO, CAIRO2, COIN, and FOCUS studies. Clin. Cancer Res. 2014, 20, 5322–5330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lochhead, P.; Kuchiba, A.; Imamura, Y.; Liao, X.; Yamauchi, M.; Nishihara, R.; Qian, Z.R.; Morikawa, T.; Shen, J.; Meyerhardt, J.A.; et al. Microsatellite instability and BRAF mutation testing in colorectal cancer prognostication. J. Natl. Cancer Inst. 2013, 105, 1151–1156. [Google Scholar] [CrossRef] [Green Version]
- Seppälä, T.T.; Böhm, J.P.; Friman, M.; Lahtinen, L.; Väyrynen, V.M.J.; Liipo, T.K.E.; Ristimäki, A.P.; Kairaluoma, M.V.J.; Kellokumpu, I.H.; Mecklin, J.P.; et al. Combination of microsatellite instability and BRAF mutation status for subtyping colorectal cancer. Br. J. Cancer 2015, 112, 1966–1975. [Google Scholar] [CrossRef] [Green Version]
- Aasebø, K.Ø.; Dragomir, A.; Sundström, M.; Mezheyeuski, A.; Edqvist, P.H.; Eide, G.E.; Ponten, F.; Pfeiffer, P.; Glimelius, B.; Sorbye, H. Consequences of a high incidence of microsatellite instability and BRAF-mutated tumors: A population-based cohort of metastatic colorectal cancer patients. Cancer Med. 2019, 8, 3623–3635. [Google Scholar] [CrossRef] [Green Version]
- Leggett, B.; Whitehall, V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology 2010, 138, 2088–2100. [Google Scholar] [CrossRef]
- McCarthy, A.J.; Serra, S.; Chetty, R. Traditional serrated adenoma: An overview of pathology and emphasis on molecular pathogenesis. BMJ Open Gastroenterol. 2019, 6, e000317. [Google Scholar] [CrossRef]
- Weisenberger, D.J.; Siegmund, K.D.; Campan, M.; Young, J.; Long, T.I.; Faasse, M.A.; Kang, G.H.; Widschwendter, M.; Weener, D.; Buchanan, D.; et al. CpG island methylator phenotype underlies sporadic microsatellite instability and is tightly associated with BRAF mutation in colorectal cancer. Nat. Genet. 2006, 38, 787–793. [Google Scholar] [CrossRef]
- Catalano, V.; Loupakis, F.; Arnold, D.; Österlund, P.; Greil, R.; Van Cutsem, E.; von Moos, R.; Viéitez, J.M.; Bouché, O.; Borg, C.; et al. Mucinous histology predicts for poor response rate and overall survival of patients with colorectal cancer and treated with first-line oxaliplatin- and/or irinotecan-based chemotherapy. Br. J. Cancer 2009, 100, 881–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samowitz, W.S.; Albertsen, H.; Sweeney, C.; Herrick, J.; Caan, B.J.; Anderson, K.E.; Wolff, R.K.; Slattery, M.L. Association of smoking, CpG island methylator phenotype, and V600E BRAF mutations in colon cancer. J. Natl. Cancer Inst. 2006, 98, 1731–1738. [Google Scholar] [CrossRef] [Green Version]
- Gonsalves, W.I.; Mahoney, M.R.; Sargent, D.J.; Nelson, G.D.; Alberts, S.R.; Sinicrope, F.A.; Goldberg, R.M.; Limburg, P.J.; Thibodeau, S.N.; Grothey, A.; et al. Patient and tumor characteristics and BRAF and KRAS mutations in colon cancer, NCCTG/Alliance N0147. J. Natl. Cancer Inst. 2014, 106, dju106. [Google Scholar] [CrossRef]
- Yoon, H.H.; Shi, Q.; Alberts, S.R.; Goldberg, R.M.; Thibodeau, S.N.; Sargent, D.J.; Sinicrope, F.A.; Alliance for Clinical Trials in Oncology. Racial Differences in BRAF/KRAS Mutation Rates and Survival in Stage III Colon Cancer Patients. J. Natl. Cancer Inst. 2015, 107, djv186. [Google Scholar] [CrossRef] [Green Version]
- Nagahashi, M.; Wakai, T.; Shimada, Y.; Ichikawa, H.; Kameyama, H.; Kobayashi, T.; Sakata, J.; Yagi, R.; Sato, N.; Kitagawa, Y.; et al. Genomic landscape of colorectal cancer in Japan: Clinical implications of comprehensive genomic sequencing for precision medicine. Genome Med. 2016, 8, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuki, S.; Kato, T.; Taniguchi, H.; Hamaguchi, T.; Akagi, K.; Denda, T.; Mizukami, T.; Oki, E.; Yamada, T.; Shiozawa, M.; et al. The nationwide cancer genome screening project in Japan, SCRUM-Japan GI-SCREEN: Efficient identification of cancer genome alterations in advanced colorectal cancer. Ann. Oncol. 2017, 28 (Suppl. 5), v192. [Google Scholar] [CrossRef]
- Yaeger, R.; Cercek, A.; Chou, J.F.; Sylvester, B.E.; Kemeny, N.E.; Hechtman, J.F.; Ladanyi, M.; Rosen, N.; Weiser, M.R.; Capanu, M.; et al. BRAF mutation predicts for poor outcomes after metastasectomy in patients with metastatic colorectal cancer. Cancer 2014, 120, 2316–2324. [Google Scholar] [CrossRef]
- Goldstein, J.; Tran, B.; Gibbs, P.; Wong, H.L.; Wong, S.F.; Vilar, E.; Tie, J.; Broaddus, R.; Kopetz, S.; Desai, J.; et al. Multicenter retrospective analysis of metastatic colorectal cancer (CRC) with high-level microsatellite instability (MSI-H). Ann. Oncol. 2014, 25, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Zong, L.; Abe, M.; Ji, J.; Zhu, W.G.; Yu, D. Tracking the Correlation between CpG Island Methylator Phenotype and Other Molecular Features and Clinicopathological Features in Human Colorectal Cancers: A Systematic Review and Meta-Analysis. Clin. Transl. Gastroenterol. 2016, 7, e151. [Google Scholar] [CrossRef]
- Vogelstein, B.; Fearon, E.R.; Hamilton, S.R.; Kern, S.E.; Preisinger, A.C.; Leppert, M.; Nakamura, Y.; White, R.; Smits, A.M.; Bos, J.L. Genetic alterations during colorectal tumor development. N. Engl. J. Med. 1988, 319, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Deng, G.; Bell, I.; Crawley, S.; Gum, J.; Terdiman, J.P.; Allen, B.A.; Truta, B.; Sleisenger, M.H.; Kim, Y.S. BRAF mutation is frequently present in sporadic colorectal cancer with methylated hMLH1, but not in hereditary nonpolyposis colorectal cancer. Clin. Cancer Res. 2004, 10, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Domingo, E.; Laiho, P.; Ollikainen, M.; Pinto, M.; Wang, L.; French, A.J.; Westra, J.; Frebourg, T.; Espín, E.; Armengol, M.; et al. BRAF screening as a low-cost effective strategy for simplifying HNPCC genetic testing. J. Med. Genet. 2004, 41, 664–668. [Google Scholar] [CrossRef]
- Farina-Sarasqueta, A.; van Lijnschoten, G.; Moerland, E.; Creemers, G.J.; Lemmens, V.E.P.P.; Rutten, H.J.T.; van den Brule, A.J.C. The BRAF V600E mutation is an independent prognostic factor for survival in stage II and stage III colon cancer patients. Ann. Oncol. 2010, 21, 2396–2402. [Google Scholar] [CrossRef]
- Roth, A.D.; Tejpar, S.; Delorenzi, M.; Yan, P.; Fiocca, R.; Klingbiel, D.; Dietrich, D.; Biesmans, B.; Bodoky, G.; Barone, C.; et al. Prognostic role of KRAS and BRAF in stage II and III resected colon cancer: Results of the translational study on the PETACC-3, EORTC 40993, SAKK 60-00 trial. J. Clin. Oncol. 2010, 28, 466–474. [Google Scholar] [CrossRef]
- Ogino, S.; Shima, K.; Meyerhardt, J.A.; McCleary, N.J.; Ng, K.; Hollis, D.; Saltz, L.B.; Mayer, R.J.; Schaefer, P.; Whittom, R.; et al. Predictive and prognostic roles of BRAF mutation in stage III colon cancer: Results from intergroup trial CALGB 89803. Clin. Cancer Res. 2012, 18, 890–900. [Google Scholar] [CrossRef] [Green Version]
- Andre, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [Green Version]
- Andre, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef] [Green Version]
- Kuebler, J.P.; Wieand, H.S.; Allegra, C.J.; Kuebler, J.P.; Colangelo, L.H.; Petrelli, N.J.; Wolmark, N. Oxaliplatin combined with weekly bolus fluorouracil and leucovorin as surgical adjuvant chemotherapy for stage II and III colon cancer: Results from NSABP C-07. J. Clin. Oncol. 2007, 25, 2198–2204. [Google Scholar] [CrossRef]
- Haller, D.G.; Tabernero, J.; Maroun, J.; de Braud, F.; Price, T.; Van Cutsem, E.; Hill, M.; Gilberg, F.; Rittweger, K.; Schmoll, H.J. Capecitabine plus oxaliplatin compared with fluorouracil and folinic acid as adjuvant therapy for stage III colon cancer. J. Clin. Oncol. 2011, 29, 1465–1471. [Google Scholar] [CrossRef]
- Yothers, G.; O’Connell, M.J.; Allegra, C.J.; Kuebler, J.P.; Colangelo, L.H.; Petrelli, N.J.; Wolmark, N. Oxaliplatin as adjuvant therapy for colon cancer: Updated results of NSABP C-07 trial, including survival and subset analyses. J. Clin. Oncol. 2011, 29, 3768–3774. [Google Scholar] [CrossRef] [Green Version]
- Gavin, P.G.; Colangelo, L.H.; Fumagalli, D.; Tanaka, N.; Remillard, M.Y.; Yothers, G.; Kim, C.; Taniyama, Y. Mutation profiling and microsatellite instability in stage II and III colon cancer: An assessment of their prognostic and oxaliplatin predictive value. Clin. Cancer Res. 2012, 18, 6531–6541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- André, T.; de Gramont, A.; Vernerey, D.; Chibaudel, B.; Bonnetain, F.; Tijeras-Raballand, A.; Scriva, A.; Hickish, T.; Tabernero, J.; Van Laethem, J.L.; et al. Adjuvant Fluorouracil, Leucovorin, and Oxaliplatin in Stage II to III Colon Cancer: Updated 10-Year Survival and Outcomes According to BRAF Mutation and Mismatch Repair Status of the MOSAIC Study. J. Clin. Oncol. 2015, 33, 4176–4187. [Google Scholar] [CrossRef]
- Tomlinson, J.S.; Jarnagin, W.R.; DeMatteo, R.P.; Fong, Y.; Kornprat, P.; Gonen, M.; Kemeny, N.; Brennan, M.F.; Blumgart, L.H.; D’Angelica, M. Actual 10-year survival after resection of colorectal liver metastases defines cure. J. Clin. Oncol. 2007, 25, 4575–4580. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Guiguet, M.; Vaillant, J.C.; Balladur, P.; Boudjema, K.; Bachellier, P.; Jaeck, D. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Cancer 1996, 77, 1254–1262. [Google Scholar] [CrossRef]
- De Jong, M.C.; Pulitano, C.; Ribero, D.; Strub, J.; Mentha, G.; Schulick, R.D.; Choti, M.A.; Aldrighetti, L.; Capussotti, L.; Pawlik, T.M. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: An international multi-institutional analysis of 1669 patients. Ann. Surg. 2009, 250, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Vauthey, J.N.; Zimmitti, G.; Kopetz, S.E.; Shindoh, J.; Chen, S.S.; Andreou, A.; Curley, S.A.; Aloia, T.A.; Maru, D.M. RAS mutation status predicts survival and patterns of recurrence in patients undergoing hepatectomy for colorectal liver metastases. Ann. Surg. 2013, 258, 619–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Margonis, G.A.; Kim, Y.; Spolverato, G.; Ejaz, A.; Gupta, R.; Cosgrove, D.; Anders, R.; Karagkounis, G.; Choti, M.A.; Pawlik, T.M. Association between specific mutations in KRAS codon12 and colorectal liver metastasis. JAMA Surg. 2015, 150, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Karagkounis, G.; Torbenson, M.S.; Daniel, H.D.; Azad, N.S.; Diaz, L.A., Jr.; Donehower, R.C.; Hirose, K.; Ahuja, N.; Pawlik, T.M.; Choti, M.A. Incidence and prognostic impact of KRAS and BRAF mutation in patients undergoing liver surgery for colorectal metastases.al. Cancer 2013, 119, 4137–4144. [Google Scholar] [CrossRef] [Green Version]
- Margonis, G.A.; Kim, Y.; Sasaki, K.; Samaha, M.; Amini, N.; Pawlik, T.M. Codon13 KRAS mutation predicts patterns of recurrence in patients undergoing hepatectomy for colorectal liver metastases. Cancer 2016, 122, 2698–2707. [Google Scholar] [CrossRef] [Green Version]
- Osumi, H.; Shinozaki, E.; Suenaga, M.; Matsusaka, S.; Konishi, T.; Akiyoshi, T.; Fujimoto, Y.; Nagayama, S.; Fukunaga, Y.; Ueno, M.; et al. RAS mutation is a prognostic biomarker in colorectal cancer patients with metastasectomy. Int. J. Cancer 2016, 139, 803–811. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, K.; Margonis, G.A.; Wilson, A.; Kim, Y.; Buettner, S.; Andreatos, N.; Gani, F.; Amini, N. Prognostic implication of KRAS status after hepatectomy for colorectal liver metastases varies according to primary colorectal tumor location. Ann. Surg. Oncol. 2016, 23, 3736–3743. [Google Scholar] [CrossRef] [PubMed]
- Frankel, T.L.; Vakiani, E.; Nathan, H.; DeMatteo, R.P.; Kingham, T.P.; Allen, P.J.; Jarnagin, W.R.; Kemeny, N.E.; Solit, D.B.; D’Angelica, M.I. Mutation location on the RAS oncogene affects pathologic features and survival after resection of colorectal liver metastases. Cancer 2017, 123, 568–575. [Google Scholar] [CrossRef] [Green Version]
- Margonis, G.A.; Buettner, S.; Andreatos, N.; Kim, Y.; Wagner, D.; Sasaki, K.; Beer, A.; Schwarz, C.; Løes, I.M.; Smolle, M.; et al. Association of BRAF mutations with survival and recurrence in surgically treated patients with metastatic colorectal liver cancer. JAMA Surg. 2018, 153, e180996. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.; Jin, Z.; Truty, M.J.; Smoot, R.L.; Nagorney, D.M.; Kendrick, M.L.; Kipp, B.R.; Grothey, A. Impact of metastasectomy in the multimodality approach for BRAFV600E metastatic colorectal cancer: The mayo clinic experience. Oncologist 2018, 23, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teng, H.W.; Huang, Y.C.; Lin, J.K.; Chen, W.S.; Lin, T.C.; Jiang, J.K.; Yen, C.C.; Li, A.F.; Wang, H.W.; Chang, S.C.; et al. BRAF mutation is a prognostic biomarker for colorectal liver metastasectomy. J. Surg. Oncol. 2012, 106, 123–129. [Google Scholar] [CrossRef]
- Schirripa, M.; Bergamo, F.; Cremolini, C.; Casagrande, M.; Lonardi, S.; Aprile, G.; Yang, D.; Marmorino, F.; Pasquini, G.; Sensi, E.; et al. BRAF and RAS mutations as prognostic factors in metastatic colorectal cancer patients undergoing liver resection. Br. J. Cancer 2015, 112, 1921–1928. [Google Scholar] [CrossRef] [Green Version]
- Tosi, F.; Magni, E.; Amatu, A.; Mauri, G.; Bencardino, K.; Truini, M.; Veronese, S.; De Carlis, L.; Ferrari, G.; Nichelatti, M.; et al. Effect of KRAS and BRAF mutations on survival of metastatic colorectal cancer after liver resection: A systematic review and meta-analysis. Clin. Colorectal Cancer 2017, 16, e153–e163. [Google Scholar] [CrossRef]
- Gagnière, J.; Dupré, A.; Gholami, S.S.; Pezet, D.; Boerner, T.; Gönen, M.; Kingham, T.K.; Allen, P.J.; Balachandran, V.P.; De Matteo, R.P.; et al. Is hepatectomy justified for BRAF mutant colorectal liver metastases? A multi-institutional analysis of 1497 patients. Ann. Surg. 2018, 271, 147–154. [Google Scholar] [CrossRef]
- Løes, I.M.; Immervoll, H.; Sorbye, H.; Angelsen, J.H.; Horn, A.; Knappskog, S.; Lønning, P.E. Impact of KRAS, BRAF, PIK3CA, TP53 status and intraindividual mutation heterogeneity on outcome after liver resection for colorectal cancer metastases. Int. J. Cancer 2016, 139, 647–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renaud, S.; Romain, B.; Falcoz, P.E.; Olland, A.; Santelmo, N.; Brigand, C.; Rohr, S.; Guenot, D.; Massard, G. KRAS and BRAF mutations are prognostic biomarkers in patients undergoing lung metastasectomy of colorectal cancer. Br. J. Cancer 2015, 112, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Schweiger, T.; Hegedus, B.; Nikolowsky, C.; Hegedüs, Z.; Szirtes, I.; Mair, R.; Birner, P.; Döme, B.; Lang, G.; Klepetko, W.; et al. EGFR, BRAF and KRAS status in patients undergoing pulmonary metastasectomy from primary colorectal carcinoma: A prospective follow up study. Ann. Surg. Oncol. 2014, 21, 946–954. [Google Scholar] [CrossRef]
- Passiglia, F.; Bronte, G.; Bazan, V.; Galvano, A.; Vincenzi, B.; Russo, A. Can KRAS and BRAF mutations limit the benefit of liver resection in metastatic colorectal cancer patients? A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 99, 150–157. [Google Scholar] [CrossRef] [Green Version]
- Bachet, J.B.; Moreno-Lopez, N.; Vigano, L.; Marchese, U.; Gelli, M.; Raoux, L.; Truant, S.; Laurent, C.; Herrero, A.; Roy, B.L.; et al. BRAF mutation is not associated with an increased risk of recurrence in patients undergoing resection of colorectal liver metastases. Br. J. Surg. 2019, 106, 1237–1247. [Google Scholar] [CrossRef]
- Tol, J.; Nagtegaal, I.D.; Punt, C.J.A. BRAF mutation in metastatic colorectal cancer. N. Engl. J. Med. 2009, 361, 98–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souglakos, J.; Philips, J.; Wang, R.; Marwah, S.; Silver, M.; Tzardi, M.; Silver, J.; Ogino, S.; Hooshmand, S.; Kwak, E.; et al. Prognostic and predictive value of common mutations for treatment response and survival in patients with metastatic colorectal cancer. Br. J. Cancer 2009, 101, 465–472. [Google Scholar] [CrossRef]
- Tie, J.; Gibbs, P.; Lipton, L.; Christie, M.; Jorissen, R.N.; Burgess, A.W.; Croxford, M.; Jones, I.; Langland, R.; Kosmider, S.; et al. Optimizing targeted therapeutic development: Analysis of a colorectal cancer patient population with the BRAF(V600E) mutation. Int. J. Cancer 2011, 128, 2075–2084. [Google Scholar] [CrossRef]
- Price, T.J.; Hardingham, J.E.; Lee, C.K.; Weickhardt, A.; Townsend, A.R.; Wrin, J.W.; Chua, A.; Shivasami, A.; Cummins, M.M.; Murone, C.; et al. Impact of KRAS and BRAF gene mutation status on outcomes from the phase III AGITG MAX trial of capecitabine alone or in combination with bevacizumab and mitomycin in advanced colorectal cancer. J. Clin. Oncol. 2011, 29, 2675–2682. [Google Scholar] [CrossRef] [PubMed]
- Chambers, P.; Elliott, F.; Daly, C.L.; Meade, A.M.; Taylor, G.; Barrett, J.H.; Quirke, P. KRAS and BRAF mutations in advanced colorectal cancer are associated with poor prognosis but do not preclude benefit from oxaliplatin or irinotecan: Results from the MRC FOCUS trial. J. Clin. Oncol. 2009, 27, 5931–5937. [Google Scholar]
- Safaee, A.G.; Jafarnejad, S.M.; Tan, L.; Saeedi, A.; Li, G. The prognostic value of BRAF mutation in colorectal cancer and melanoma: A systematic review and meta-analysis. PLoS ONE 2012, 7, e47054. [Google Scholar]
- Modest, D.P.; Ricard, I.; Heinemann, V.; Hegewisch-Becker, S.; Schmiegel, W.; Porschen, R.; Stintzing, S.; Graeven, U.; Arnold, D.; Weikersthalan, L.F.; et al. Outcome according to KRAS-, NRAS- and BRAF-mutation as well as KRAS mutation variants: Pooled analysis of five randomized trials in metastatic colorectal cancer by the AIO colorectal cancer study group. Ann. Oncol. 2016, 27, 1746–1753. [Google Scholar] [CrossRef] [PubMed]
- Kayhanian, H.; Goode, E.; Sclafani, F.; Ang, J.E.; Gerlinger, M.; de Castro, G.D.; Shepherd, S.; Peckitt, C.; Rao, S.; Watkins, D.; et al. Treatment and Survival Outcome of BRAF-Mutated Metastatic Colorectal Cancer: A Retrospective Matched Case-Control Study. Clin. Colorectal Cancer 2018, 17, e69–e76. [Google Scholar] [CrossRef] [Green Version]
- Morris, V.; Overman, M.J.; Jiang, Z.Q.; Garrett, C.; Agarwal, S.; Eng, C.; Kee, B.; Fogelman, D.; Dasari, A.; Wolff, R.; et al. Progression free survival remains poor over sequential lines of systemic therapy in patients with BRAF-mutated colorectal cancer. Clin. Colorectal Cancer 2014, 13, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Phipps, A.I.; Limburg, P.J.; Baron, J.A.; Burnett-Hartman, A.N.; Weisenberger, D.J.; Laird, P.W.; Sinicrope, F.A.; Rosty, C.; Buchanan, D.D.; Potter, J.D.; et al. Association between molecular subtypes of colorectal cancer and patient survival. Gastroenterology 2015, 148, e72. [Google Scholar] [CrossRef] [Green Version]
- Halling, K.C.; French, A.J.; McDonnell, S.K.; Burgart, L.J.; Schaid, D.J.; Peterson, B.J.; Moon-Tasson, L.; Mahoney, M.R.; Sargent, D.J.; O’Connell, M.J.; et al. Microsatellite instability and 8p allelic imbalance in stage B2 and C colorectal cancers. J. Natl. Cancer Inst. 1999, 91, 1295–1303. [Google Scholar] [CrossRef] [Green Version]
- Samowitz, W.S.; Curtin, K.; Ma, K.N.; Schaffer, D.; Coleman, L.W.; Leppert, M.; Slattery, M.L. Microsatellite instability in sporadic colon cancer is associated with an improved prognosis at the population level. Cancer Epidemiol. Biomark. Prev. 2001, 10, 917–923. [Google Scholar]
- Phipps, A.I.; Buchanan, D.D.; Makar, K.W.; Burnett-Hartman, A.N.; Coghill, A.E.; Passarelli, M.N.; Baron, J.A.; Ahnen, D.J.; Win, A.K.; Potter, J.D.; et al. BRAF mutation status and survival after colorectal cancer diagnosis according to patient and tumor characteristics. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1792–1798. [Google Scholar] [CrossRef] [Green Version]
- Nakaji, Y.; Oki, E.; Nakanishi, R.; Ando, K.; Sugiyama, M.; Nakashima, Y.; Yamashita, N.; Saeki, H.; Oda, Y.; Maehara, Y. Prognostic value of BRAF V600E mutation and microsatellite instability in Japanese patients with sporadic colorectal cancer. J. Cancer Res. Clin. Oncol. 2017, 143, 151–160. [Google Scholar] [CrossRef]
- French, A.J.; Sargent, D.J.; Burgart, L.J.; Foster, N.R.; Kabat, B.F.; Goldberg, R.; Shepherd, L.; Windschitl, H.E.; Thibodeau, S.N. Prognostic significance of defective mismatch repair and BRAF V600E in patients with colon cancer. Clin. Cancer Res. 2008, 14, 3408–3415. [Google Scholar] [CrossRef] [Green Version]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Cunningham, D.; Humblet, Y.; Siena, S.; Khayat, D.; Bleiberg, H.; Santoro, A.; Bets, D.; Mueser, M.; Harstrick, A.; Verslype, C.; et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N. Engl. J. Med. 2004, 351, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Peeters, M.; Siena, S.; Humblet, Y.; Hendlisz, A.; Neyns, B.; Canon, J.L.; Van Laethem, J.L.; Maurel, J.; Richardson, G.; et al. Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J. Clin. Oncol. 2007, 25, 1658–1664. [Google Scholar] [CrossRef]
- Sobrero, A.F.; Maurel, J.; Fehrenbacher, L.; Scheithauer, W.; Abubakr, Y.A.; Lutz, M.P.; Vega-Villegas, M.E.; Eng, C.; Steinhauer, E.U.; Prausova, J.; et al. EPIC: Phase III trial of cetuximab plus irinotecan after fluoropyrimidine and oxaliplatin failure in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 2311–2319. [Google Scholar] [CrossRef] [Green Version]
- Lievre, A.; Bachet, J.B.; Le Corre, D.; Boige, V.; Landi, B.; Emile, J.F.; Côté, J.F.; Tomasic, G.; Penna, C.; Ducreux, M.; et al. KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Cancer Res. 2006, 66, 3992–3995. [Google Scholar] [CrossRef] [Green Version]
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.; et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef] [Green Version]
- Amado, R.G.; Wolf, M.; Peeters, M.; Van Cutsem, E.; Siena, S.; Freeman, D.J.; Juan, T.; Sikorski, R.; Suggs, S.; Radinsky, R.; et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1626–1634. [Google Scholar] [CrossRef]
- Linardou, H.; Dahabreh, I.J.; Kanaloupiti, D.; Siannis, F.; Bafaloukos, D.; Kosmidis, P.; Papadimitriou, C.A.; Murray, S. Assessment of somatic k-RAS mutations as a mechanism associated with resistance to EGFR-targeted agents: A systematic review and meta-analysis of studies in advanced non-small-cell lung cancer and metastatic colorectal cancer. Lancet Oncol. 2008, 9, 962–972. [Google Scholar] [CrossRef]
- Benvenuti, S.; Sartore-Bianchi, A.; Di Nicolantonio, F.; Zanon, C.; Moroni, M.; Veronese, S.; Siena, S.; Bardelli, A. Oncogenic activation of the RAS/RAF signaling pathway impairs the response of metastatic colorectal cancers to anti epidermal growth factor receptor antibody therapies. Cancer Res. 2007, 67, 2643–2648. [Google Scholar] [CrossRef] [Green Version]
- Di Nicolantonio, F.; Martini, M.; Molinari, F.; Sartore-Bianchi, A.; Arena, S.; Saletti, P.; De Dosso, S.; Mazzucchelli, L. Wild-type BRAF is required for response to panitumumab or cetuximab in metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 5705–5712. [Google Scholar] [CrossRef]
- Loupakis, F.; Ruzzo, A.; Vincenzi, L.B.; Salvatore, D.; Santini, G.; Masi, I.; Stasi, E.; Canestrari, E.; Rulli, I.; Floriani, I.; et al. KRAS codon 61, 146 and BRAF mutations predict resistance to cetuximab plus irinotecan in KRAS codon 12 and 13 wild-type metastatic colorectal cancer. Br. J. Cancer 2009, 101, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Roock, W.; Claes, B.; Bernasconi, D.; De Schutter, J.; Biesmans, B.; Fountzilas, G.; Penault-Llorca, F. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: A retrospective consortium analysis. Lancet Oncol. 2010, 11, 753–762. [Google Scholar] [CrossRef]
- Douillard, J.-Y.; Oliner, K.S.; Bernasconi, D.; De Schutter, J.; Biesmans, B.; Fountzilas, G.; Kalogeras, K.T.; Kotoula, V.; Papamichael, D.; Laurent-Puig, P.; et al. Panitumumab–FOLFOX4 treatment and RAS mutations in colorectal cancer. N. Engl. J. Med. 2013, 369, 1023–1034. [Google Scholar] [CrossRef] [Green Version]
- Tol, J.; Dijkstra, J.R.; Klomp, M.; Teerenstra, S.; Dommerholt, M.; Vink-Börger, M.E.; van Cleef, P.H.; van Krieken, J.H.; Punt, C.J.A.; Nagtegaal, I.D. Markers for EGFR pathway activation as predictor of outcome in metastatic colorectal cancer patients treated with or without cetuximab. Eur. J. Cancer 2010, 46, 1997–2009. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, C.; Bondarenko, I.; Hartmann, J.T.; de Braud, F.; Schuch, G.; Zubel, A.; Celik, I.; Schlichting, M.; Koralewsk, P. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: The OPUS study. Ann. Oncol. 2011, 22, 1535–1546. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Köhne, C.H.; Láng, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: Updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef] [Green Version]
- Bokemeyer, C.; Van Cutsem, E.; Rougier, P.; Ciardiello, F.; Heeger, S.; Schlichting, M.; Celik, I.; Köhne, C.H. Addition of cetuximab to chemotherapy as first-line treatment for KRAS wild-type metastatic colorectal cancer: Pooled analysis of the CRYSTAL and OPUS randomised clinical trials. Eur. J. Cancer 2012, 48, 1466–1475. [Google Scholar] [CrossRef]
- Tveit, K.M.; Guren, T.; Glimelius, B.; Pfeiffer, P.; Sorbye, H.; Pyrhonen, S.; Sigurdsson, F.; Kure, E.; Ikdahl, T.; Skovlund, E.; et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: The NORDIC-VII study. J. Clin. Oncol. 2012, 30, 1755–1762. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Miller-Phillips, L.; Modest, D.P.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.E.; Heintges, T.; Kahl, C.; et al. Impact of BRAF and RAS mutations on first-line efficacy of FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab: Analysis of the FIRE-3 (AIO KRK0306) study. Eur. J. Cancer 2017, 79, 50–60. [Google Scholar] [CrossRef]
- Seymour, M.T.; Brown, S.R.; Middleton, G.; Maughan, T.; Richman, S.; Gwyther, S.; Lowe, C.; Jennifer, F.; Seligmann, J.F. Panitumumab and irinotecan versus irinotecan alone for patients with KRAS wild-type, fluorouracil-resistant advanced colorectal cancer (PICCOLO): A prospectively stratified randomised trial. Lancet Oncol. 2013, 14, 749–759. [Google Scholar] [CrossRef] [Green Version]
- Peeters, M.; Oliner, K.S.; Price, T.J.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y.; André, T.; Chan, E.; Lordick, F.; et al. Analysis of KRAS/NRAS mutations in a phase III study of panitumumab with FOLFIRI compared with FOLFIRI alone as second-line treatment for metastatic colorectal cancer. Clin. Cancer Res. 2015, 21, 5469–5479. [Google Scholar] [CrossRef] [Green Version]
- Karapetis, C.S.; Jonker, D.; Daneshmand, M.; Hanson, J.E.; O’Callaghan, C.J.; Marginean, C.; Zalcberg, J.R.; Simes, J.; Moore, M.J.; Tebbutt, N.C.; et al. PIK3CA, BRAF, and PTEN status and benefit from cetuximab in the treatment of advanced colorectal cancer—Results from NCIC CTG/AGITG CO.17. Clin. Cancer Res. 2014, 20, 744–753. [Google Scholar] [CrossRef] [Green Version]
- Rowland, A.; Dias, M.M.; Wiese, M.D.; Kichenadasse, G.; McKinnon, R.A.; Karapetis, C.S.; Sorich, M.J. Meta-analysis of BRAF mutation as a predictive biomarker of benefit from anti-EGFR monoclonal antibody therapy for RAS wild-type metastatic colorectal cancer. Br. J. Cancer 2015, 112, 1888–1894. [Google Scholar] [CrossRef] [Green Version]
- Therkildsen, C.; Bergmann, T.K.; Wiese, M.D.; Kichenadasse, G.; McKinnon, R.A.; Karapetis, C.S.; Sorich, M.J. The predictive value of KRAS, NRAS, BRAF, PIK3CA and PTEN for anti-EGFR treatment in metastatic colorectal cancer: A systematic review and meta-analysis. Acta Oncol. 2014, 53, 852–864. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Z.X.; Wang, X.Y.; Qin, Q.Y.; Chen, D.F.; Zhong, Q.H.; Wang, L.; Wang, J.P. The prognostic role of BRAF mutation in metastatic colorectal cancer receiving anti-EGFR monoclonal antibodies: A meta-analysis. PLoS ONE 2013, 8, e65995. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.G.; Fisher, D.; Claes, B.; Maughan, T.S.; Idziaszczyk, S.; Peuteman, G.; Harris, R.; James, M.D.; Meade, A.; Jasani, B.; et al. Somatic profiling of the epidermal growth factor receptor pathway in tumors from patients with advanced colorectal cancer treated with chemotherapy ± cetuximab. Clin. Cancer Res. 2013, 19, 4104–4113. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Xu, A.T.; Zhu, M.M.; Tong, J.L.; Xu, X.T.; Ran, Z.H. Predictive and prognostic roles of BRAF mutation in patients with metastatic colorectal cancer treated with anti-epidermal growth factor receptor monoclonal antibodies: A meta-analysis. J. Dig. Dis. 2013, 14, 409–416. [Google Scholar] [CrossRef]
- Wang, Q.; Hu, W.; Zhu, M.M.; Tong, J.L.; Xu, X.T.; Ran, Z.H. BRAF V600E mutation as a predictive factor of anti-EGFR monoclonal antibodies therapeutic effects in metastatic colorectal cancer: A meta-analysis. Chin. Med. Sci. J. 2014, 29, 197–203. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Petrelli, F.; Coinu, A.; Di Bartolomeo, M.; Borgonovo, K.; Maggi, C.; Cabiddu, M.; Iacovelli, R.; Bossi, I.; Lonati, V.; et al. Predictive role of BRAF mutations in patients with advanced colorectal cancer receiving cetuximab and panitumumab: A meta-analysis. Eur. J. Cancer 2015, 51, 587–594. [Google Scholar] [CrossRef]
- Cui, D.; Cao, D.; Yang, Y.; Qiu, M.; Huang, Y.; Yi, C. Effect of BRAF V600E mutation on tumor response of anti-EGFR monoclonal antibodies for first-line metastatic colorectal cancer treatment: A meta-analysis of randomized studies. Mol. Biol. Rep. 2014, 41, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Van Brummelen, E.M.J.; de Boer, A.; Beijnen, J.H.; Schellens, J.H.M. BRAF Mutations as Predictive Biomarker for Response to Anti-EGFR Monoclonal Antibodies. Oncologist 2017, 22, 864–872. [Google Scholar] [CrossRef] [Green Version]
- Masi, G.; Loupakis, F.; Salvatore, L.; Fornaro, L.; Cremolini, C.; Cupini, S.; Ciarlo, A.; Del Monte, F.; Cortesi, E.; Amoroso, D.; et al. Bevacizumab with FOLFOXIRI (irinotecan, oxaliplatin, fluorouracil, and folinate) as first-line treatment for metastatic colorectal cancer: A phase 2 trial. Lancet Oncol. 2010, 11, 845–852. [Google Scholar] [CrossRef]
- Loupakis, F.; Cremolini, C.; Masi, G.; Lonardi, S.; Zagonel, V.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Ronzoni, M.; Spadi, R.; et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N. Engl. J. Med. 2014, 371, 1609–1618. [Google Scholar] [CrossRef] [Green Version]
- Loupakis, F.; Cremolini, C.; Salvatore, L.; Masi, G.; Sensi, E.; Schirripa, M.; Michelucci, A.; Pfanner, E.; Brunetti, I.; Lupi, C.; et al. FOLFOXIRI plus bevacizumab as first-line treatment in BRAF mutant metastatic colorectal cancer. Eur. J. Cancer 2014, 50, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Colon Cancer. Version 2. 2016. Available online: https://www2.tri-kobe.org/nccn/guideline/archive/colorectal2016/english/colon.pdf (accessed on 3 March 2020).
- Yoshino, T.; Arnold, D.; Taniguchi, H.; Pentheroudakis, G.; Yamazaki, K.; Xu, R.H.; Kim, T.W.; Ismail, F.; Tan, I.B.; Yeh, K.H.; et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: A JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann. Oncol. 2018, 29, 44–70. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaeger, R.; Chatila, W.K.; Lipsyc, M.D.; Hechtman, J.F.; Cercek, A.; Sanchez-Vega, F.; Jayakumaran, G.; Middha, S.; Zehir, A.; Donoghue, M.T.A.; et al. Clinical sequencing defines the genomic landscape of metastatic colorectal cancer. Cancer Cell. 2018, 33, 125–136.e3. [Google Scholar] [CrossRef]
- Allegra, C.J.; Jessup, J.M.; Somerfield, M.R.; Hamilton, S.R.; Hammond, E.H.; Hayes, D.F.; McAllister, P.K.; Morton, R.F.; Schilsky, R.L. American Society of Clinical Oncology provisional clinical opinion: Testing for KRAS gene mutations in patients with metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy. J. Clin. Oncol. 2009, 27, 2091–2096. [Google Scholar] [CrossRef] [Green Version]
- Allegra, C.J.; Rumble, R.B.; Hamilton, S.R.; Mangu, P.B.; Roach, N.; Hantel, A.; Schilsky, R.L. Extended RAS Gene Mutation Testing in Metastatic Colorectal Carcinoma to Predict Response to Anti-Epidermal Growth Factor Receptor Monoclonal Antibody Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update 2015. J. Clin. Oncol. 2016, 34, 179–185. [Google Scholar] [CrossRef]
- De Roock, W.; De Vriendt, V.; Normanno, N.; Ciardiello, F.; Tejpar, S. KRAS, BRAF, PIK3CA, and PTEN mutations: Implications for targeted therapies in metastatic colorectal cancer. Lancet Oncol. 2011, 12, 594–603. [Google Scholar] [CrossRef]
- Nakayama, I.; Shinozaki, E.; Matsushima, T.; Wakatsuki, T.; Ogura, M.; Ichimura, T.; Ozaka, M.; Takahari, D.; Suenaga, M.; Chin, K.; et al. Retrospective study of RAS/PIK3CA/BRAF tumor mutations as predictors of response to first-line chemotherapy with bevacizumab in metastatic colorectal cancer patients. BMC Cancer 2017, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Tsai, J.; Lee, J.T.; Wang, W.; Zhang, J.; Cho, H.; Mamo, S.; Bremer, R.; Gillette, S.; Kong, J.; Haass, N.K.; et al. Discovery of a selective inhibitor of oncogenic B-Raf kinase with potent antimelanoma activity. Proc. Natl. Acad. Sci. USA 2008, 105, 3041–3046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaherty, K.T.; Puzanov, I.; Kim, K.B.; Ribas, A.; McArthur, G.A.; Sosman, J.A.; O’Dwyer, P.J.; Lee, R.J.; Grippo, J.F.; Nolop, K.; et al. Inhibition of Mutated, Activated BRAF in Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 809–819. [Google Scholar] [CrossRef] [Green Version]
- Ribas, A.; Kim, K.B.; Schuchter, L.M.; Gonzalez, R.; Pavlick, A.C.; WeberG, J.S.; McArthur, A.; Hutson, T.E.; Flaherty, K.T.; Moschos, S.J.; et al. BRIM-2: An open-label, multicenter phase II study of vemurafenib in previously treated patients with BRAFV600E mutation-positive melanoma. J. Clin. Oncol. 2011, 29 (Suppl. 15), 8509. [Google Scholar] [CrossRef]
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N. Engl. J. Med. 2011, 364, 2507–2516. [Google Scholar] [CrossRef] [Green Version]
- Kopetz, S.; Desai, J.; Chan, E.; Hecht, J.R.; O’Dwyer, P.J.; Maru, D.; Morris, V.; Janku, F.; Dasari, A.; Chung, W.; et al. Phase II pilot study of vemurafenib in patients with metastatic BRAF-mutated colorectal cancer. J. Clin. Oncol. 2015, 33, 4032–4038. [Google Scholar] [CrossRef]
- Bollag, G.; Hirth, P.; Zhang, J.; Ibrahim, P.N.; Cho, H.; Spevak, W.; Zhang, C.; Zhang, Y.; Habets, G.; Burton, E.A.; et al. Clinical efficacy of a RAF inhibitor needs broad target blockade in BRAF-mutant melanoma. Nature 2010, 467, 596–599. [Google Scholar] [CrossRef]
- Dougherty, M.K.; Müller, J.; Ritt, D.A.; Zhou, M.; Zhou, X.Z.; Copeland, T.D.; Conrads, T.P.; Veenstra, T.D.; Lu, K.P.; Morrison, D.K. Regulation of Raf-1 by direct feedback phosphorylation. Mol. Cell 2005, 17, 215–224. [Google Scholar] [CrossRef]
- Pratilas, C.A.; Taylor, B.S.; Ye, Q.; Viale, A.; Sander, C.; Solit, D.B.; Rosen, N. (V600E)BRAF is associated with disabled feedback inhibition of RAF-MEK signaling and elevated transcriptional output of the pathway. Proc. Natl. Acad. Sci. USA 2009, 106, 4519–4524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lake, D.; Corrêa, S.A.; Müller, J. Negative feedback regulation of the ERK1/2 MAPK pathway. Cell Mol. Life Sci. 2016, 73, 4397–4413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, C.K.; Slupsky, J.R.; Kalmes, H.A.; Rapp, U.R. Active Ras induces heterodimerization of cRaf and BRaf. Cancer Res. 2001, 61, 3595–3598. [Google Scholar]
- Wan, P.T.C.; Garnett, M.J.; Roe, S.M.; Lee, S.; Niculescu-Duvaz, D.; Good, V.M.; Jones, C.M.; Marshall, C.J.; Springer, C.J.; Barford, D.; et al. Mechanism of activation of the RAF-ERK signaling pathway by oncogenic mutations of B-RAF. Cell 2004, 116, 855–867. [Google Scholar] [CrossRef] [Green Version]
- Garnett, M.J.; Rana, S.; Kalmes, H.A.; Rapp, U.R. Wildtype and mutant B-RAF activate C-RAF through distinct mechanisms involving heterodimerization. Mol. Cell 2005, 20, 963–969. [Google Scholar] [CrossRef]
- Rushworth, L.K.; Hindley, A.D.; O’Neill, E.; Kolch, W. Regulation and role of Raf1/B-Raf heterodimerization. Mol. Cell. Biol. 2006, 26, 2262–2272. [Google Scholar] [CrossRef] [Green Version]
- Joseph, E.W.; Pratilas, C.A.; Poulikakos, P.I.; Tadi, M.; Wang, W.; Taylor, B.S.; Halilovic, E.; Persaud, Y.; Xing, F.; Viale, A.; et al. The RAF inhibitor PLX4032 inhibits ERK signaling and tumor cell proliferation in a V600E BRAF selective manner. Proc. Natl. Acad. Sci. USA 2010, 107, 14903–14908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulikakos, P.I.; Zhang, C.; Bollag, G.; Shokat, K.M.; Rosen, N. RAF inhibitors transactivate RAF dimers and ERK signalling in cells with wild-type BRAF. Nature 2010, 464, 427–430. [Google Scholar] [CrossRef] [Green Version]
- Hatzivassiliou, G.; Song, K.; Yen, I.; Brandhuber, B.J.; Anderson, D.J.; Alvarado, R.; Ludlam, M.J.; Stokoe, D.; Gloor, S.L.; Vigers, G.; et al. RAF inhibitors prime wild-type RAF to activate the MAPK pathway and enhance growth. Nature 2010, 464, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidorn, S.J.; Milagre, C.; Whittaker, S.; Nourry, A.; Niculescu-Duvas, I.; Dhomen, N.; Hussain, J.; Reis-Filho, J.S.; Springer, C.J.; Pritchard, C.; et al. Kinase-dead BRAF and oncogenic RAS cooperate to drive tumor progression through CRAF. Cell 2010, 140, 209–221. [Google Scholar] [CrossRef]
- Prahallad, A.; Sun, C.; Huang, S.; Di Nicolantonio, F.; Salazar, R.; Zecchin, D.; Beijersbergen, R.L.; Bardelli, A.; Bernards, R. Unresponsiveness of colon cancer to BRAF(V600E) inhibition through feedback activation of EGFR. Nature 2012, 483, 100–103. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; He, G.; Nelman-Gonzalez, M.; Ashorn, C.L.; Gallick, G.E.; Stukenberg, P.T.; Kirschner, M.W.; Kuang, J. Regulation of Cdc25C by ERK-MAP kinases during the G2/M transition. Cell 2007, 128, 1119–1132. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, R.B.; Ebi, H.; Turke, A.B.; Coffee, E.M.; Nishino, M.; Cogdill, A.P.; Brown, R.D.; Pelle, P.D.; Dias-Santagata, D.; Hung, K.E.; et al. EGFR-mediated re-activation of MAPK signaling contributes to insensitivity of BRAF mutant colorectal cancers to RAF inhibition with vemurafenib. Cancer Discov. 2012, 2, 227–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lito, P.; Pratilas, C.A.; Joseph, E.W.; Tadi, M.; Halilovic, E.; Zubrowski, M.; Huang, A.; Wong, W.L.; Callahan, M.K.; Merghoub, T.; et al. Relief of profound feedback inhibition of mitogenic signaling by RAF inhibitors attenuates their activity in BRAFV600E melanomas. Cancer Cell 2012, 22, 668–682. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, R.B.; Atreya, C.E.; Falchook, G.S.; Kwak, E.L.; Ryan, D.P.; Bendell, J.C.; Hamid, O.; Messersmith, W.A.; Daud, A.; Kurzrock, R.; et al. Combined BRAF and MEK inhibition with dabrafenib and trametinib in BRAF V600-mutant colorectal cancer. J. Clin. Oncol. 2015, 33, 4023–4031. [Google Scholar] [CrossRef] [Green Version]
- Yaeger, R.; Cercek, A.; O’Reilly, E.M.; Reidy, D.L.; Kemeny, N.; Wolinsky, T.; Capanu, M.; Gollub, M.J.; Rosen, N.; Berger, M.F.; et al. Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin. Cancer Res. 2015, 21, 1313–1320. [Google Scholar] [CrossRef] [Green Version]
- Van Geel, R.M.J.M.; Tabernero, J.; Elez, E.; Bendell, J.C.; Spreafico, A.; Schuler, M.; Yoshino, T.; Delord, J.P.; Yamada, Y.; Lolkema, M.P.; et al. A Phase Ib Dose-Escalation Study of Encorafenib and Cetuximab with or without Alpelisib in Metastatic BRAF-Mutant Colorectal Cancer. Cancer Discov. 2017, 7, 610–619. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, R.B.; Giannakis, M.; Allen, J.; Chen, J.; Pelka, K.; Chao, S.; Meyerhardt, J.; Enzinger, A.; Enzinger, P.; McCleary, N.; et al. Clinical efficacy of combined BRAF, MEK, and PD-1 inhibition in BRAFV600E colorectal cancer patients. Ann. Oncol. 2020, 31, S226–S227. [Google Scholar] [CrossRef]
- Mao, M.; Tian, F.; Mariadason, J.M.; Tsao, C.C.; Lemos, R., Jr.; Dayyani, F.; Gopal, Y.N.V.; Jiang, Z.Q.; Wistuba, I.I.; Tang, X.M.; et al. Resistance to BRAF inhibition in BRAF-mutant colon cancer can be overcome with PI3K inhibition or demethylating agents. Clin. Cancer Res. 2013, 19, 657–667. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Higgins, B.; Kolinsky, K.; Packman, K.; Bradley, W.D.; Lee, R.J.; Schostack, K.; Simcox, M.E.; Kopetz, S.; Heimbrook, D.; et al. Antitumor activity of BRAF inhibitor vemurafenib in preclinical models of BRAF-mutant colorectal cancer. Cancer Res. 2012, 72, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Hong, D.S.; Morris, V.K.; Osta, B.E.; Sorokin, A.V.; Janku, F.; Fu, S.; Overman, M.J.; Piha-Paul, S.; Subbiah, V.; Kee, B.; et al. Phase IB study of vemurafenib in combination with irinotecan and cetuximab in patients with metastatic colorectal cancer with BRAFV600E mutation. Cancer Discov. 2016, 6, 1352–1365. [Google Scholar] [CrossRef] [Green Version]
- Germann, U.A.; Furey, B.F.; Markland, W.; Hoover, R.R.; Aronov, A.M.; Roix, J.J.; Hale, M.; Boucher, D.M.; Sorrell, D.A.; Martinez-Botella, G.; et al. Targeting the MAPK Signaling Pathway in Cancer: Promising Preclinical Activity with the Novel Selective ERK1/2 Inhibitor BVD-523 (Ulixertinib). Mol. Cancer Ther. 2017, 16, 2351–2363. [Google Scholar] [CrossRef] [Green Version]
- Hazar-Rethinam, M.; Kleyman, M.; Han, G.C.; Liu, D.; Ahronian, L.G.; Shahzade, H.A.; Chen, L.; Parikh, A.R.; Allen, J.N.; Clark, J.W.; et al. Convergent Therapeutic Strategies to Overcome the Heterogeneity of Acquired Resistance in BRAFV600E Colorectal Cancer. Cancer Discov. 2018, 8, 417–427. [Google Scholar] [CrossRef] [Green Version]
- Kopetz, S.; Grothey, A.; Van Cutsem, E.; Yaeger, R.; Wasan, H.S.; Yoshino, T.; Desai, J.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib plus cetuximab with or without binimetinib for BRAF V600E-mutant metastatic colorectal cancer: Quality-of-life results from a randomized, three-arm, phase III study versus the choice of either irinotecan or FOLFIRI plus cetuximab (BEACON CRC). In Proceedings of the ASCO Gastrointestinal Cancers Symposium 2020, San Francisco, CA, USA, 23–25 January 2020. [Google Scholar]
- Corcoran, R.B.; Andre, T.; Atreya, C.E.; Schellens, J.H.M.; Yoshino, T.; Bendell, J.C.; Hollebecque, A.; McRee, A.J.; Siena, S.; Middleton, G.; et al. Combined BRAF, EGFR, and MEK Inhibition in Patients with BRAF(V600E)-Mutant Colorectal Cancer. Cancer Discov. 2018, 8, 428–443. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-encorafenib-combination-cetuximab-metastatic-colorectal-cancer-braf-v600e-mutation (accessed on 26 April 2020).
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Overman, M.J.; Lonardi, S.; Wong, K.Y.M.W.; Lenz, H.F.; Gelsomino, F.; Aglietta, M.; Morse, M.A.; Van Cutsem, E.; McDermott, R.; Hill, A. Durable Clinical Benefit with Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J. Clin. Oncol. 2018, 36, 773–779. [Google Scholar] [CrossRef]
- Ahronian, L.G.; Sennott, E.M.; Van Allen, E.M.; Wagle, N.; Kwak, E.L.; Faris, J.E.; Godfrey, J.T.; Nishimura, K.; Lynch, K.D.; Mermel, C.H.; et al. Clinical Acquired Resistance to RAF Inhibitor Combinations in BRAF-Mutant Colorectal Cancer through MAPK Pathway Alterations. Cancer Discov. 2015, 5, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Oddo, D.; Sennott, E.M.; Barault, L.; Valtorta, E.; Arena, S.; Cassingena, A.; Filiciotto, G.; Marzolla, G.; Elez, E.; van Geel, R.M.J.M.; et al. Molecular Landscape of Acquired Resistance to Targeted Therapy Combinations in BRAF-Mutant Colorectal Cancer. Cancer Res. 2016, 76, 4504–4515. [Google Scholar] [CrossRef] [Green Version]
- Pietrantonio, F.; Oddo, D.; Gloghini, A.; Valtorta, E.; Berenato, R.; Barault, L.; Caporale, M.; Busico, A.; Morano, F.; Gualeni, A.V.; et al. MET-Driven Resistance to Dual EGFR and BRAF Blockade May Be Overcome by Switching from EGFR to MET Inhibition in BRAF-Mutated Colorectal Cancer. Cancer Discov. 2016, 6, 963–971. [Google Scholar] [CrossRef] [Green Version]
- Oddo, D.; Siravegna, G.; Gloghini, A.; Vernieri, C.; Mussolin, B.; Morano, F.; Crisafulli, G.; Berenato, R.; Corti, G.; Volpi, C.C.; et al. Emergence of MET hyper-amplification at progression to MET and BRAF inhibition in colorectal cancer. Br. J. Cancer 2017, 117, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, L.; Huang, S.; Heynen, G.J.; Prahallad, A.; Robert, C.; Haanen, J.; Blank, C.; Wesseling, J.; Willems, S.M.; et al. Reversible and adaptive resistance to BRAF(V600E) inhibition in melanoma. Nature 2014, 508, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Seghers, A.C.; Wilgenhof, S.; Lebbé, C.; Neyns, B. Successful rechallenge in two patients with BRAF-V600-mutant melanoma who experienced previous progression during treatment with a selective BRAF inhibitor. Melanoma Res. 2012, 22, 466–472. [Google Scholar] [CrossRef]
- Forbes, S.A.; Beare, D.; Gunasekaran, P.; Leung, K.; Bindal, N.; Boutselakis, H.; Ding, M.; Bamford, S.; Cole, C.; Ward, S.; et al. COSMIC: Exploring the world’s knowledge of somatic mutations in human cancer. Nucleic Acids Res. 2015, 43, D805–D811. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Di Bartolomeo, M.; Amatu, A.; Antoniotti, C.; Moretto, R.; Berenato, R.; Perrone, F.; Tamborini, E.; Aprile, G.; Lonardi, S.; et al. BRAF codons 594 and 596 mutations identify a new molecular subtype of metastatic colorectal cancer at favorable prognosis. Ann. Oncol. 2015, 26, 2092–2097. [Google Scholar] [CrossRef]
- Shinozaki, E.; Yoshino, T.; Yamazaki, K.; Muro, K.; Yamaguchi, K.; Nishina, T.; Yuki, S.; Shitara, K.; Bando, H.; Mimaki, S.; et al. Clinical significance of BRAF non-V600E mutations on the therapeutic effects of anti-EGFR monoclonal antibody treatment in patients with pretreated metastatic colorectal cancer: The Biomarker Research for anti-EGFR monoclonal Antibodies by Comprehensive Cancer genomics (BREAC) study. Br. J. Cancer 2017, 117, 1450–1458. [Google Scholar]
- Jones, J.C.; Renfro, L.A.; Al-Shamsi, H.O.; Schrock, A.B.; Rankin, A.; Zhang, B.Y.; Kasi, P.M.; Voss, J.S.; Leal, A.D.; Sun, J.; et al. (nonV600) BRAF mutations define a clinically distinct molecular subtype of metastatic colorectal cancer. J. Clin. Oncol. 2017, 35, 2624–2630. [Google Scholar] [CrossRef]
- Osumi, H.; Shinozaki, E.; Wakatsuki, T.; Suenaga, M.; Ichimura, T.; Ogura, M.; Takahari, D.; Ooki, A.; Suzuki, T.; Ota, Y.; et al. Non-V600E BRAF mutations and EGFR signaling pathway in colorectal cancer. Int. J. Cancer 2019, 145, 2488–2495. [Google Scholar] [CrossRef]
- Ikenoue, T.; Hikiba, Y.; Kanai, F.; Tanaka, Y.; Imamura, J.; Imamura, T.; Ohta, M.; Ijichi, H.; Tateishi, K.; Kawakami, T.; et al. Functional analysis of mutations within the kinase activation segment of B-Raf in human colorectal tumors. Cancer Res. 2003, 63, 8132–8137. [Google Scholar]
- Yao, Z.; Yaeger, R.; Rodrik-Outmezguine, V.S.; Tao, A.; Torres, N.M.; Chang, M.T.; Drosten, M.; Zhao, H.; Cecchi, F.; Hembrough, T.; et al. Tumours with class 3 BRAF mutants are sensitive to the inhibition of activated RAS. Nature 2017, 548, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Schirripa, M.; Biason, P.; Lonardi, S.; Pella, N.; Pino, M.S.; Urbano, F.; Antoniotti, C.; Cremolini, C.; Corallo, S.; Pietrantonio, F.; et al. Class 1, 2, and 3 BRAF-Mutated Metastatic Colorectal Cancer: A Detailed Clinical, Pathologic, and Molecular Characterization. Clin. Cancer Res. 2019, 25, 3954–3961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaeger, R.; Kotani, D.; Mondaca, S.; Parikh, A.R.; Bando, H.; Van Seventer, E.E.; Taniguchi, H.; Zhao, H.; Thant, C.N.; de Stanchina, E.; et al. Response to Anti-EGFR Therapy in Patients with BRAF non-V600-Mutant Metastatic Colorectal Cancer. Clin. Cancer Res. 2019, 25, 7089–7097. [Google Scholar] [CrossRef] [Green Version]
- Van ’t Veer, L.J.; Dai, H.; van de Vijver, M.J.; He, Y.D.; Hart, A.A.; Mao, M.; Peterse, H.L.; van der Kooy, K.; Marton, M.J.; Witteveen, A.T.; et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002, 415, 530.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweet-Cordero, A.; Mukherjee, S.; Subramanian, A.; You, H.; Roix, J.J.; Ladd-Acosta, C.; Mesirov, J.; Golub, T.R.; Jacks, T. An oncogenic KRAS2 expression signature identified by cross-species gene-expression analysis. Nat. Genet. 2005, 37, 48.e55. [Google Scholar] [CrossRef]
- Bild, A.H.; Yao, G.; Chang, J.T.; Wang, Q.; Potti, A.; Chasse, D.; Joshi, M.B.; Harpole, D.; Lancaster, J.M.; Berchuck, A.; et al. Oncogenic pathway signatures in human cancers as a guide to targeted therapies. Nature 2006, 439, 353.e7. [Google Scholar] [CrossRef]
- Van’t Veer, L.J.; Bernards, R. Enabling personalized cancer medicine through analysis of gene-expression patterns. Nature 2008, 452, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Barras, D.; Missiaglia, E.; Wirapati, P.; Sieber, O.M.; Jorissen, R.N.; Love, C.; Molloy, P.L.; Jones, I.T.; McLaughlin, S.; Gibbs, P.; et al. BRAF V600E mutant colorectal cancer subtypes based on gene expression. Clin. Cancer Res. 2017, 23, 104–115. [Google Scholar] [CrossRef] [Green Version]
- Middleton, G.; Yang, Y.; Campbell, C.D.; André, T.; Atreya, C.E.; Schellens, J.H.M.; Yoshino, T.; Bendell, J.C.; Hollebecque, A.; McRee, A.J.; et al. BRAF-mutant Transcriptional Subtypes Predict Outcome of Combined BRAF, MEK, and EGFR Blockade with Dabrafenib, Trametinib, and Panitumumab in Patients with Colorectal Cancer. Clin. Cancer Res. 2020, 26, 2466–2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dienstmann, R.; Vermeulen, L.; Guinney, J.; Kopetz, S.; Tejpar, S.; Tabernero, J. Consensus molecular subtypes and the evolution of precision medicine in colorectal cancer. Nat. Rev. Cancer 2017, 17, 79–92. [Google Scholar] [CrossRef]
- Pavey, S.; Johansson, P.; Packer, L.; Taylor, J.; Stark, M.; Pollock, P.M.; Walker, G.J.; Boyle, G.M.; Harper, U.; Cozzi, S.J.; et al. Microarray expression profiling in melanoma reveals a BRAF mutation signature. Oncogene 2004, 23, 4060–4067. [Google Scholar] [CrossRef] [Green Version]
- Kannengiesser, C.; Spatz, A.; Michiels, S.; Eychène, A.; Dessen, P.; Lazar, V.; Winnepenninckx, V.; Lesueur, F.; Druillennec, S.; Robert, C.; et al. Gene expression signature associated with BRAF mutations in human primary cutaneous melanomas. Mol. Oncol. 2008, 1, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Tian, S.; Simon, I.; Moreno, V.; Roepman, P.; Tabernero, J.; Snel, M.; van’t Veer, L.; Salazar, R.; Bernards, R.; Capella, G.A. combined oncogenic pathway signature of BRAF, KRAS and PI3KCA mutation improves colorectal cancer classification and cetuximab treatment prediction. Gut 2013, 62, 540–549. [Google Scholar] [CrossRef] [Green Version]
- Popovici, V.; Budinska, E.; Tejpar, S.; Weinrich, S.; Estrella, H.; Hodgson, G.; Van Cutsem, E.; Xie, T.; Bosman, F.T.; Roth, A.D.; et al. Identification of a Poor-prognosis BRAF Mutant-Like population of patients with colon cancer. J. Clin. Oncol. 2012, 30, 1288.e95. [Google Scholar] [CrossRef]
- Vecchione, L.; Gambino, V.; Raaijmakers, J.; Schlicker, A.; Fumagalli, A.; Russo, M.; Villanueva, A.; Beerling, E.; Bartolini, A.; Mollevi, D.G.; et al. A vulnerability of a subset of colon cancers with potential utility. Cell 2016, 165, 317–330. [Google Scholar] [CrossRef] [Green Version]
- Zlobec, I.; Bihl, M.; Foerster, A.; Rufle, A.; Lugli, A. Comprehensive analysis of CpG island methylator phenotype (CIMP)-high, -low, and -negative colorectal cancers based on protein marker expression and molecular features. J. Pathol. 2011, 225, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Rhee, Y.Y.; Bae, J.M.; Cho, N.Y.; Kang, G.H. Loss of CDX2/CK20 expression is associated with poorly differentiated carcinoma, the CpG island methylator phenotype, and adverse prognosis in microsatellite-unstable colorectal cancer. Am. J. Surg. Pathol. 2013, 37, 1532–1541. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, E.M.F.; Wang, X.; Jansen, M.; Fessler, E.; Trinh, A.; de Rooij, L.P.M.H.; de Jong, J.H.; de Boer, O.J.; van Leersum, R.; Bijlsma, M.F.; et al. Poor-prognosis Colon Cancer Is Defined by a Molecularly Distinct Subtype and Develops from Serrated Precursor Lesions. Nat. Med. 2013, 19, 614–618. [Google Scholar] [CrossRef]
- Trinh, A.; Trumpi, K.; Melo, F.D.S.E.; Wang, X.; de Jong, J.H.; Fessler, E.; Kuppen, P.J.K.; Reimers, M.S.; Swets, M.; Koopman, M.; et al. Practical and robust identification of molecular subtypes in colorectal cancer by immunohistochemistry. Clin. Cancer Res. 2017, 23, 387–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loupakis, F.; Biason, P.; Prete, A.A.; Cremolini, C.; Pietrantonio, F.; Pella, N.; Dell’Aquila, E.; Sperti, E.; Zichi, C.; Intini, R.; et al. CK7 and consensus molecular subtypes as major prognosticators in V600EBRAF mutated metastatic colorectal cancer. Br. J. Cancer 2019, 121, 593–599. [Google Scholar] [CrossRef]
- Loupakis, F.; Intini, R.; Cremolini, C.; Orlandi, A.; Sartore-Bianchi, A.; Pietrantonio, F.; Pella, N.; Spallanzani, A.; Dell’Aquila, E.; Scartozzi, M.; et al. A validated prognostic classifier for V600EBRAF-mutated metastatic colorectal cancer: The ‘BRAF BeCool’ study. Eur. J. Cancer 2019, 118, 121–130. [Google Scholar] [CrossRef]
Figure 1.
Signal transduction in the EGF/EGFR–RAS–RAF–MEK–MAPK pathway. (A) Regulated signal transduction in RAS/BRAF wt cells. EGFR is activated by the binding of EGF, a specific ligand to become an active homodimer. Homodimerization stimulates the autophosphorylation of tyrosine residues in the EGFR domain, which initiates the downstream signal cascade via RAS–RAF–MEK–MAPK signal transduction. Activated RAS-induced dimerization of RAFs is necessary for phosphorylating downstream effectors, MEK and ERK (left). This signal transduction pathway comprises a negative feedback loop, i.e., elevated pERK in turn causes the de-phosphorylation of EGFR and thereby attenuates this signal (right). (B) The constitutive activation of the RAF–MEK–MAPK signal in BRAFV600E cells. BRAFV600E-mutated cells constitutively activate its downstream effectors as a monomer in the absence of upstream signals. Given this independence, the activation of the MAPK pathway is refractory to the pERK-mediated negative feedback regulation. This explains why RAF–MEK–MAPK signal transduction is constitutively active in BRAFV600E cells. (C) BRAF inhibition with ATP competitive RAF inhibitors in BRAFV600E. ATP-competitive inhibitors such as vemurafenib act on monomeric BRAF and suppress downstream signal transduction. These kind of kinase inhibitors can initially control the constitutive activation; however, because of the reduction of pERK, they attenuate the negative feedback. EGFR-mediated signal transduction will be reactivated before long in CRCs, as activated RAS induces RAF dimerization, between BRAF and CRAF, which is refractory to vemurafenib. Therefore, BRAF-mutated CRCs can easily overcome the monomer inhibition treatment. (D) The concept of the vertical blockade strategy: blocking both upstream and downstream of BRAF using anti-EGFR mAb and MEK inhibitor in EGFR signal axis, respectively, were developed to overcome the resistance mechanism. Theoretically, this vertical blockade can suppress the growth signaling if and only if the EGFR–RAS–MEK–MAPK pathway remains the prime pathway throughout treatment. (E) A possible signaling pathway providing resistance to the vertical blockade triplet therapy. The EGFR signal axis is not the only pathway for the proliferation of BRAF-mutated CRCs. Reactivation of other receptor tyrosine kinases (RTKs), such as HER2 and MET, was pointed out in vitro. Moreover, the RAS–RAF–MEK–MAPK pathway is known to interact with the PI3K/AKT pathway. BRAF-mutated CRCs can therefore evade the vertical blockade with triplet therapy through these alternative means. EGFR: epidermal growth factor receptor, EGF: epidermal growth Factor, Wt: wild type, pERK: phosphorylated ERK, mAb: monoclonal antibody, CRC: colorectal cancer.
Figure 1.
Signal transduction in the EGF/EGFR–RAS–RAF–MEK–MAPK pathway. (A) Regulated signal transduction in RAS/BRAF wt cells. EGFR is activated by the binding of EGF, a specific ligand to become an active homodimer. Homodimerization stimulates the autophosphorylation of tyrosine residues in the EGFR domain, which initiates the downstream signal cascade via RAS–RAF–MEK–MAPK signal transduction. Activated RAS-induced dimerization of RAFs is necessary for phosphorylating downstream effectors, MEK and ERK (left). This signal transduction pathway comprises a negative feedback loop, i.e., elevated pERK in turn causes the de-phosphorylation of EGFR and thereby attenuates this signal (right). (B) The constitutive activation of the RAF–MEK–MAPK signal in BRAFV600E cells. BRAFV600E-mutated cells constitutively activate its downstream effectors as a monomer in the absence of upstream signals. Given this independence, the activation of the MAPK pathway is refractory to the pERK-mediated negative feedback regulation. This explains why RAF–MEK–MAPK signal transduction is constitutively active in BRAFV600E cells. (C) BRAF inhibition with ATP competitive RAF inhibitors in BRAFV600E. ATP-competitive inhibitors such as vemurafenib act on monomeric BRAF and suppress downstream signal transduction. These kind of kinase inhibitors can initially control the constitutive activation; however, because of the reduction of pERK, they attenuate the negative feedback. EGFR-mediated signal transduction will be reactivated before long in CRCs, as activated RAS induces RAF dimerization, between BRAF and CRAF, which is refractory to vemurafenib. Therefore, BRAF-mutated CRCs can easily overcome the monomer inhibition treatment. (D) The concept of the vertical blockade strategy: blocking both upstream and downstream of BRAF using anti-EGFR mAb and MEK inhibitor in EGFR signal axis, respectively, were developed to overcome the resistance mechanism. Theoretically, this vertical blockade can suppress the growth signaling if and only if the EGFR–RAS–MEK–MAPK pathway remains the prime pathway throughout treatment. (E) A possible signaling pathway providing resistance to the vertical blockade triplet therapy. The EGFR signal axis is not the only pathway for the proliferation of BRAF-mutated CRCs. Reactivation of other receptor tyrosine kinases (RTKs), such as HER2 and MET, was pointed out in vitro. Moreover, the RAS–RAF–MEK–MAPK pathway is known to interact with the PI3K/AKT pathway. BRAF-mutated CRCs can therefore evade the vertical blockade with triplet therapy through these alternative means. EGFR: epidermal growth factor receptor, EGF: epidermal growth Factor, Wt: wild type, pERK: phosphorylated ERK, mAb: monoclonal antibody, CRC: colorectal cancer.



Figure 2.
History of basic studies, genetic tests, and clinical trials that together established the significance of the BRAF mutation in the treatment of CRCs. The RAF genes, ARAF, BRAF, and CRAF, were discovered in 1983. The first report of BRAF mutation in human cancers was published in 2002 and included melanoma, lung cancer, and colorectal cancer. Early studies on BRAF mutation in CRC were focused on its characteristic molecular and clinicopathological features. Although BRAF mutation had a strong negative impact on the survival, the presence of the BRAF mutation itself had little influence when making decisions on treatment options at this time. At that stage, the BRAF genetic test was not mandatory in clinical practice. Since the success of clinical trials with anti-EGFR mAbs in 2004, targeting the EGF/EGFR pathway became technically feasible in treating metastatic colorectal cancer (mCRC). Unlike for the KRAS mutation, the BRAF mutation alone was insufficient to determine indication or anti-EGFR mAb therapy. Studies using clinical samples pointed out a loss of EGFR-mediated negative feedback to be the mechanism of resistance to the BRAF inhibitor. Combination therapies suppress not only activated BRAF but the entire RAF–MEK–MAPK signal transduction pathway, successfully controlling the BRAF-mutated mCRC. ARAF, BRAF, CRAF: Raf murine sarcoma viral oncogene homolog A, B, C; EGFR: epidermal growth factor receptor; mAb: monoclonal antibody; CRC: colorectal cancer.
Figure 2.
History of basic studies, genetic tests, and clinical trials that together established the significance of the BRAF mutation in the treatment of CRCs. The RAF genes, ARAF, BRAF, and CRAF, were discovered in 1983. The first report of BRAF mutation in human cancers was published in 2002 and included melanoma, lung cancer, and colorectal cancer. Early studies on BRAF mutation in CRC were focused on its characteristic molecular and clinicopathological features. Although BRAF mutation had a strong negative impact on the survival, the presence of the BRAF mutation itself had little influence when making decisions on treatment options at this time. At that stage, the BRAF genetic test was not mandatory in clinical practice. Since the success of clinical trials with anti-EGFR mAbs in 2004, targeting the EGF/EGFR pathway became technically feasible in treating metastatic colorectal cancer (mCRC). Unlike for the KRAS mutation, the BRAF mutation alone was insufficient to determine indication or anti-EGFR mAb therapy. Studies using clinical samples pointed out a loss of EGFR-mediated negative feedback to be the mechanism of resistance to the BRAF inhibitor. Combination therapies suppress not only activated BRAF but the entire RAF–MEK–MAPK signal transduction pathway, successfully controlling the BRAF-mutated mCRC. ARAF, BRAF, CRAF: Raf murine sarcoma viral oncogene homolog A, B, C; EGFR: epidermal growth factor receptor; mAb: monoclonal antibody; CRC: colorectal cancer.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nakayama, I.; Hirota, T.; Shinozaki, E. BRAF Mutation in Colorectal Cancers: From Prognostic Marker to Targetable Mutation. Cancers 2020, 12, 3236. https://doi.org/10.3390/cancers12113236
AMA Style
Nakayama I, Hirota T, Shinozaki E. BRAF Mutation in Colorectal Cancers: From Prognostic Marker to Targetable Mutation. Cancers. 2020; 12(11):3236. https://doi.org/10.3390/cancers12113236
Chicago/Turabian StyleNakayama, Izuma, Toru Hirota, and Eiji Shinozaki. 2020. "BRAF Mutation in Colorectal Cancers: From Prognostic Marker to Targetable Mutation" Cancers 12, no. 11: 3236. https://doi.org/10.3390/cancers12113236
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.