Detection of Oral Dysplastic and Early Cancerous Lesions by Polarization-Sensitive Optical Coherence Tomography

 ,
,
Abstract
:1. Introduction
2. Results
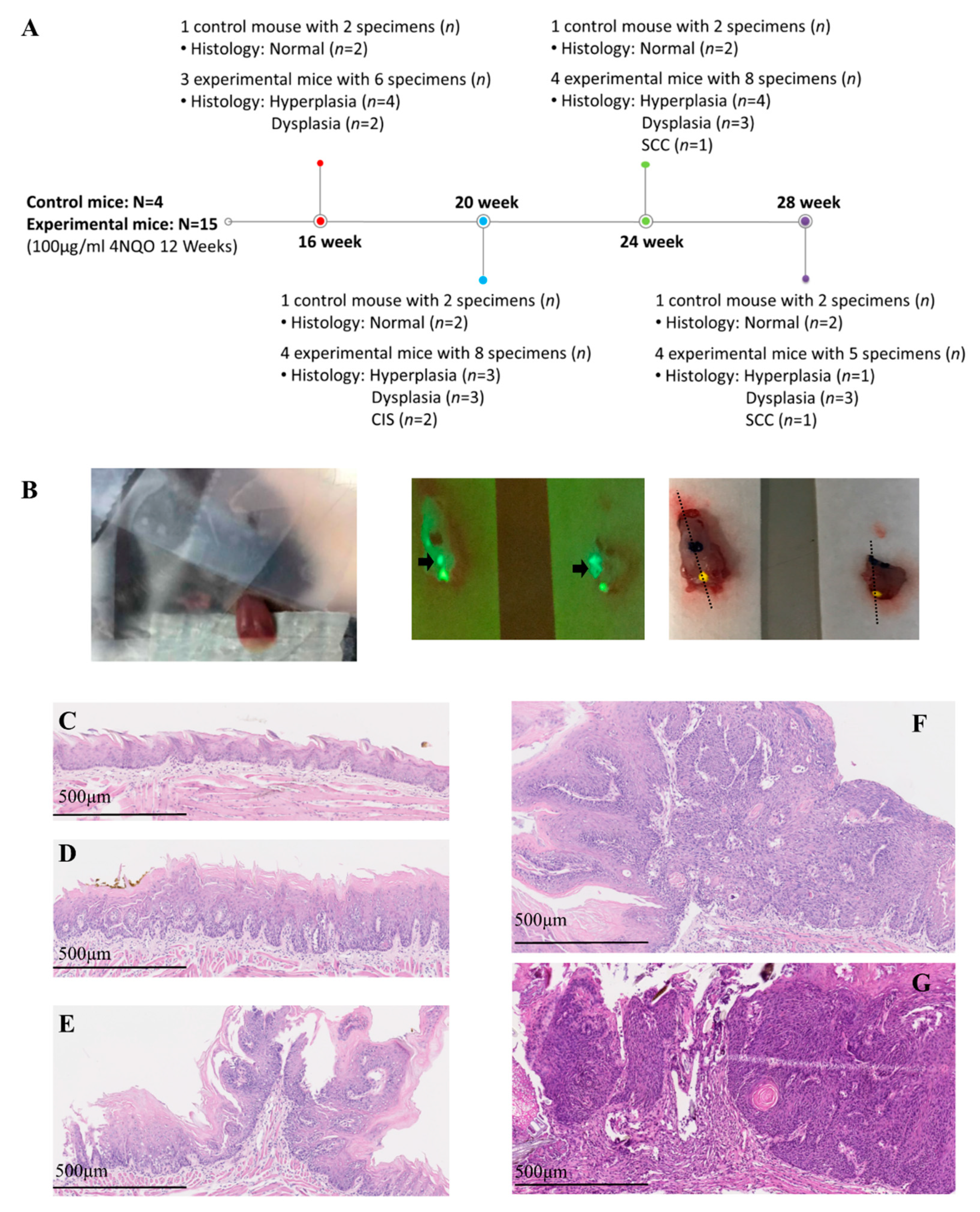
2.1. Animal Protocol and Histology Results
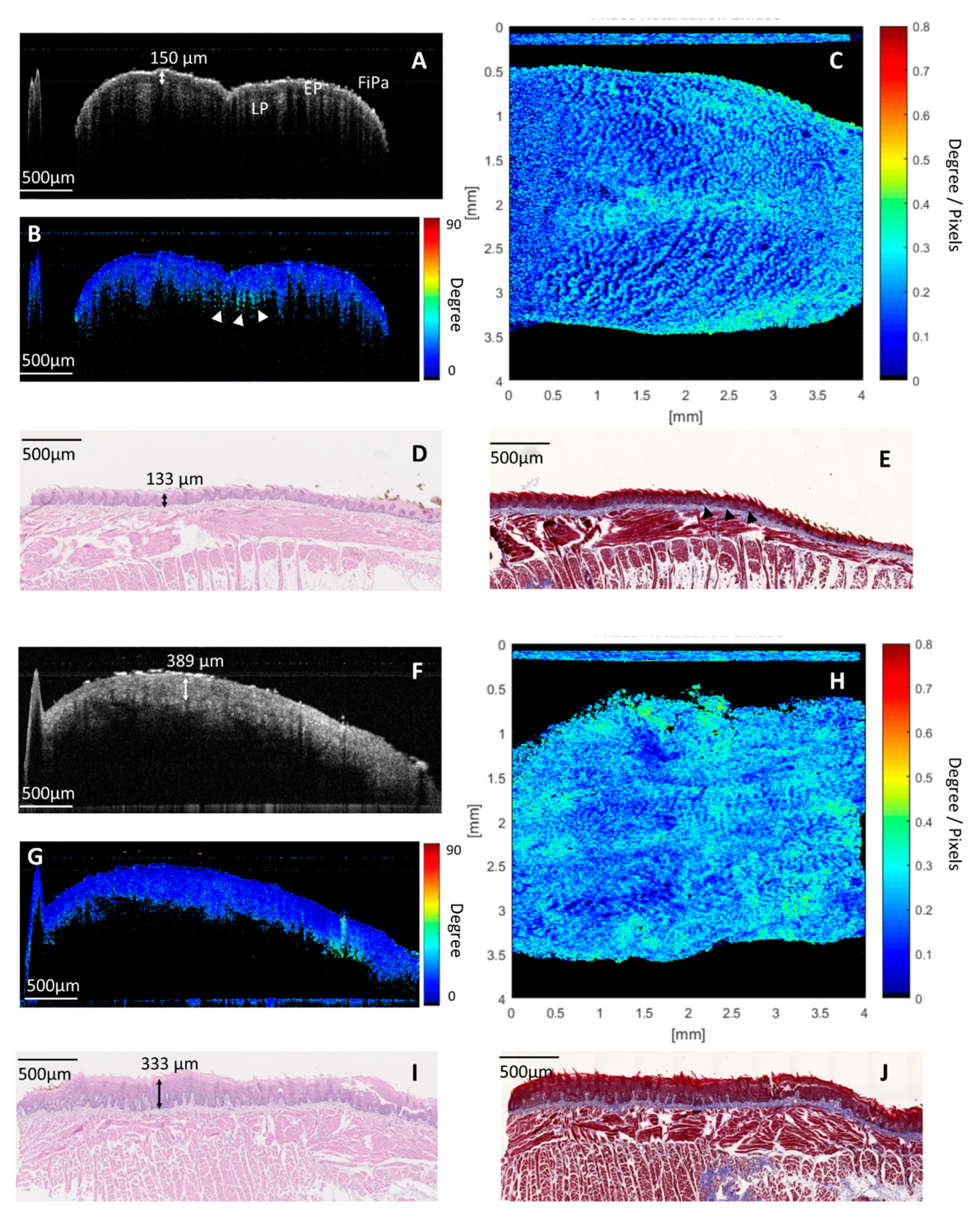
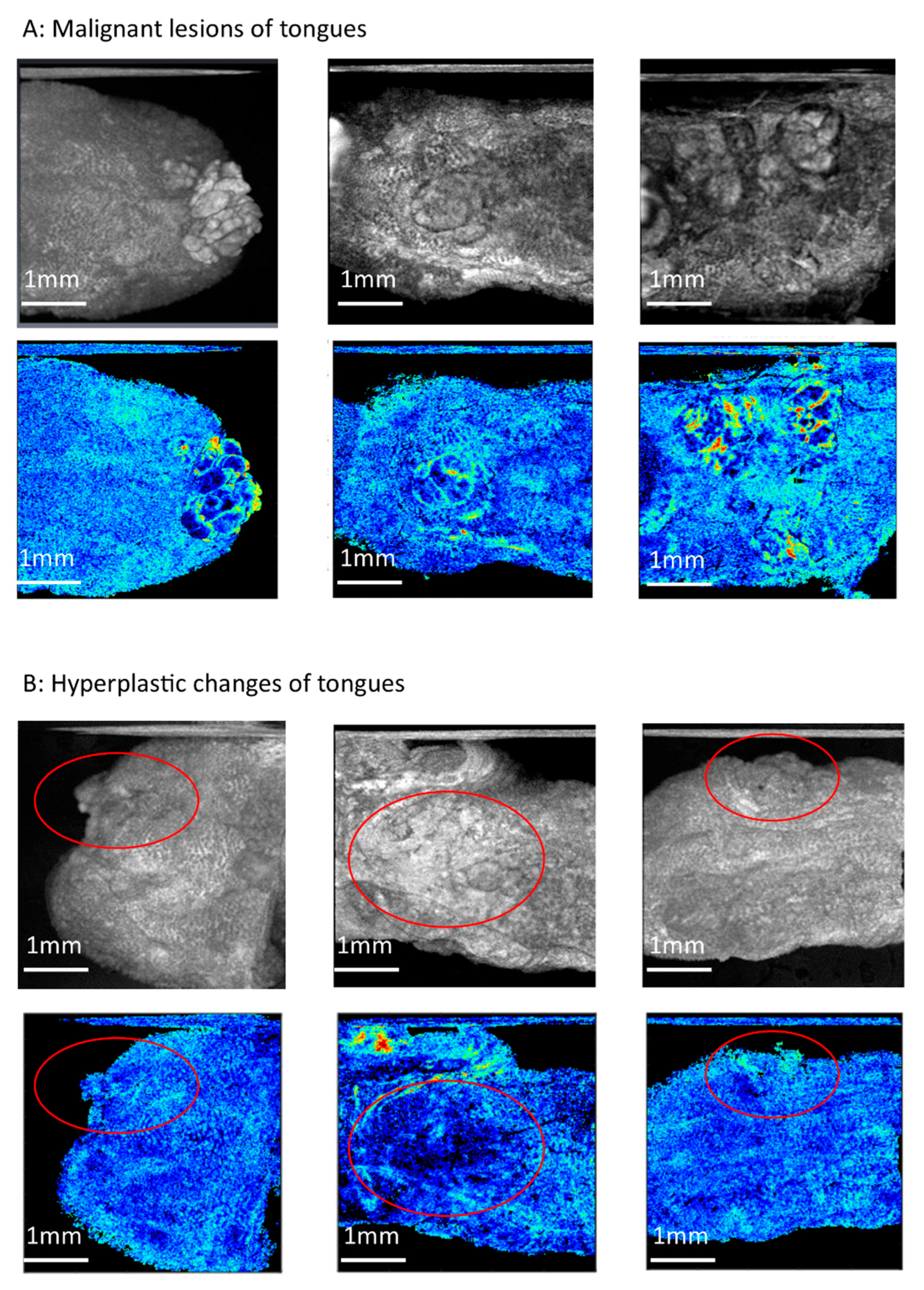
2.2. PS-OCT Imaging and Birefringence Maps in Benign Lesions (Normal and Hyperplasia)
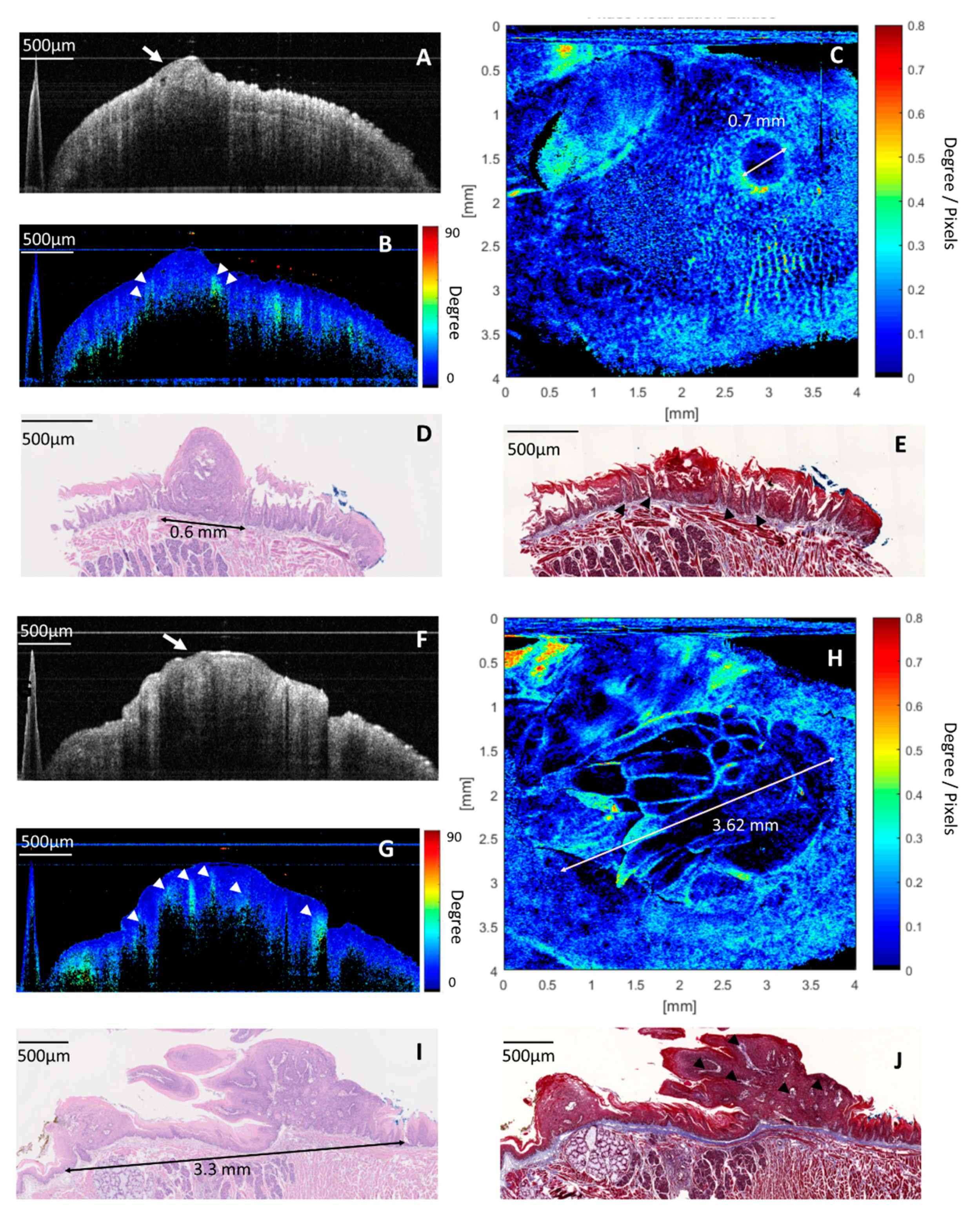
2.3. PS-OCT Image and Birefringence Map in Malignant Lesions (Dysplasia and Early-Stage Cancer)
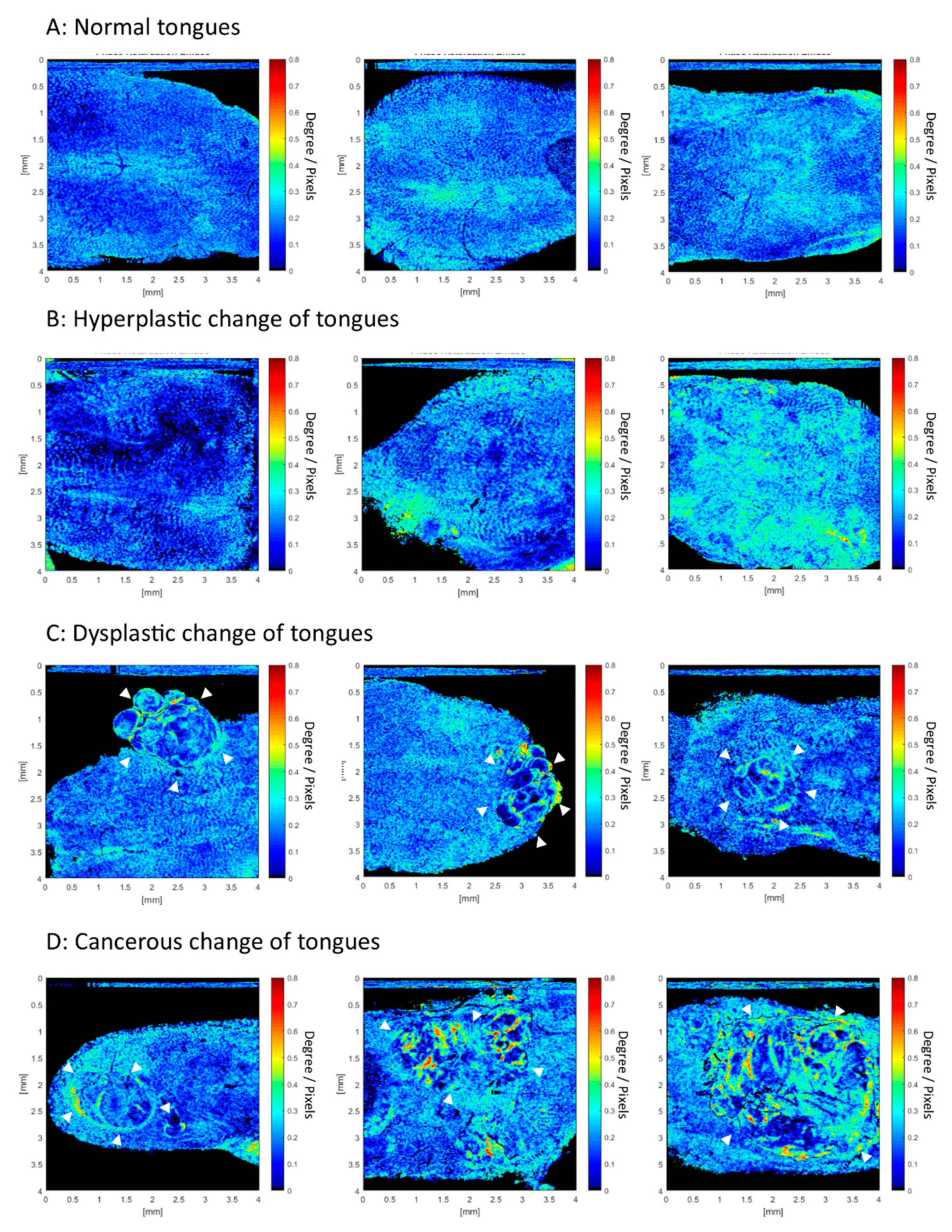
2.4. Accuracy of En-Face Birefringence Map to Detect Dysplasia and Early Cancerous Lesion
3. Discussion
4. Materials and Methods
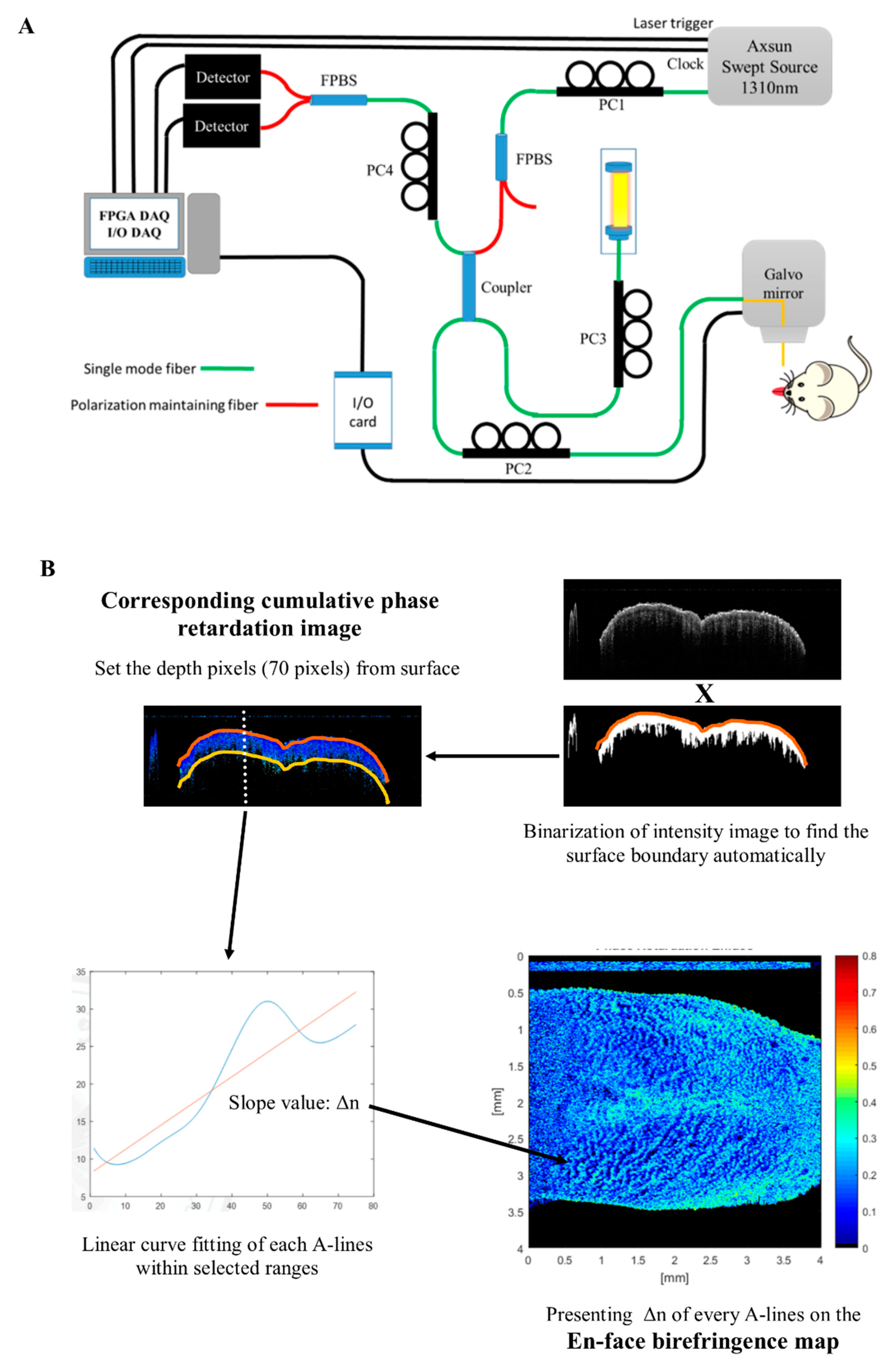
4.1. Swept-Source, Polarization-Sensitive Optical Coherence Tomography (SS PS-OCT) Imaging System
4.2. Process of PS-OCT Imaging and Build an En-Face Birefringence Map
4.3. Animal and Experimental Protocol
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ren, J.S.; Masuyer, E.; Ferlay, J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int. J. Cancer 2013, 132, 1133–1145. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- Downer, M.C.; Moles, D.R.; Palmer, S.; Speight, P.M. A systematic review of test performance in screening for oral cancer and precancer. Oral Oncol. 2004, 40, 264–273. [Google Scholar] [CrossRef]
- Mehanna, H.M.; Rattay, T.; Smith, J.; McConkey, C.C. Treatment and follow-up of oral dysplasia—A systematic review and meta-analysis. Head Neck 2009, 31, 1600–1609. [Google Scholar] [CrossRef]
- Yang, E.C.; Tan, M.T.; Schwarz, R.A.; Richards-Kortum, R.R.; Gillenwater, A.M.; Vigneswaran, N. Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: Current limitations and future directions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 670–681. [Google Scholar] [CrossRef]
- Wilder-Smith, P.; Jung, W.G.; Brenner, M.; Osann, K.; Beydoun, H.; Messadi, D.; Chen, Z. In vivo optical coherence tomography for the diagnosis of oral malignancy. Lasers Surg. Med. 2004, 35, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.T.; Lee, C.K.; Lee, H.C.; Chen, H.M.; Chiang, C.P.; Wang, Y.M.; Yang, C.C. Differentiating oral lesions in different carcinogenesis stages with optical coherence tomography. J. Biomed. Opt. 2009, 14, 044028. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.T.; Lee, H.C.; Lee, C.K.; Yu, C.H.; Chen, H.M.; Chiang, C.P.; Chang, C.C.; Wang, Y.M.; Yang, C.C. Effective indicators for diagnosis of oral cancer using optical coherence tomography. Opt. Express 2008, 16, 15847–15862. [Google Scholar]
- Lee, C.K.; Chi, T.T.; Wu, C.T.; Tsai, M.T.; Chiang, C.P.; Yang, C.C. Diagnosis of oral precancer with optical coherence tomography. Biomed. Opt. Express 2012, 3, 1632–1646. [Google Scholar] [CrossRef]
- Hamdoon, Z.; Jerjes, W.; Upile, T.; McKenzie, G.; Jay, A.; Hopper, C. Optical coherence tomography in the assessment of suspicious oral lesions: An immediate ex vivo study. Photodiagnosis Photodyn. Ther. 2013, 10, 17–27. [Google Scholar] [CrossRef]
- Vu, A.; Farah, C.S. Narrow band imaging: Clinical applications in oral and oropharyngeal cancer. Oral Dis. 2016, 22, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; Lucchese, A.; Gentile, E.; Zulli, C.; Petruzzi, M.; Lauritano, D.; Amato, M.R.; Esposito, P.; Riegler, G.; Serpico, R. Evaluation of the intraepithelial papillary capillary loops in benign and malignant oral lesions by in vivo virtual chromoendoscopic magnification: A preliminary study. J. Biol. Regul. Homeost. Agents 2017, 31, 11–22. [Google Scholar] [PubMed]
- Ansari, U.H.; Wong, E.; Smith, M.; Singh, N.; Palme, C.E.; Smith, M.C.; Riffat, F. Validity of narrow band imaging in the detection of oral and oropharyngeal malignant lesions: A systematic review and meta-analysis. Head Neck 2019, 41, 2430–2440. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.H.; Wu, C.H.; Chen, Y.F.; Yeh, Y.C.; Lin, B.H.; Chang, K.W.; Lai, P.Y.; Hou, M.C.; Lu, C.L.; Kuo, W.C. Combination of structural and vascular optical coherence tomography for differentiating oral lesions of mice in different carcinogenesis stages. Biomed. Opt. Express 2018, 9, 1461–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.H.; Chen, Y.J.; Chen, Y.F.; Yeh, Y.C.; Chang, K.W.; Hou, M.C.; Kuo, W.C. Quantification of structural and microvascular changes for diagnosing early-stage oral cancer. Biomed. Opt. Express 2020, 11, 1244–1256. [Google Scholar] [CrossRef]
- Salo, T.; Vered, M.; Bello, I.O.; Nyberg, P.; Bitu, C.C.; Hurvitz, A.Z.; Dayan, D. Insights into the role of components of the tumor microenvironment in oral carcinoma call for new therapeutic approaches. Exp. Cell Res. 2014, 325, 58–64. [Google Scholar] [CrossRef]
- Muller, S. Oral epithelial dysplasia, atypical verrucous lesions and oral potentially malignant disorders: Focus on histopathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 591–602. [Google Scholar] [CrossRef] [Green Version]
- Arun Gopinathan, P.; Kokila, G.; Jyothi, M.; Ananjan, C.; Pradeep, L.; Humaira Nazir, S. Study of collagen birefringence in different grades of oral squamous cell carcinoma using picrosirius red and polarized light microscopy. Scientifica 2015, 2015, 802980. [Google Scholar] [CrossRef] [Green Version]
- Devendra, A.; Niranjan, K.C.; Swetha, A.; Kaveri, H. Histochemical analysis of collagen reorganization at the invasive front of oral squamous cell carcinoma tumors. J. Investig. Clin. Dent. 2018, 9, e12283. [Google Scholar] [CrossRef]
- Mostaco-Guidolin, L.; Rosin, N.L.; Hackett, T.L. Imaging collagen in scar tissue: Developments in second harmonic generation microscopy for biomedical applications. Int. J. Mol. Sci. 2017, 18, 1772. [Google Scholar] [CrossRef]
- Chen, W.S.; Wang, Y.; Liu, N.R.; Zhang, J.X.; Chen, R. Multiphoton microscopic imaging of human normal and cancerous oesophagus tissue. J. Microsc. 2014, 253, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Hee, M.R.; Huang, D.; Swanson, E.A.; Fujimoto, J.G. Polarization-sensitive low-coherence reflectometer for birefringence characterization and ranging. J. Opt. Soc. Am. B 1992, 9, 903–908. [Google Scholar] [CrossRef]
- Walther, J.; Li, Q.; Villiger, M.; Farah, C.S.; Koch, E.; Karnowski, K.; Sampson, D.D. Depth-resolved birefringence imaging of collagen fiber organization in the human oral mucosa in vivo. Biomed. Opt. Express 2019, 10, 1942–1956. [Google Scholar] [CrossRef] [PubMed]
- Walther, J.; Golde, J.; Kirsten, L.; Tetschke, F.; Hempel, F.; Rosenauer, T.; Hannig, C.; Koch, E. In vivo imaging of human oral hard and soft tissues by polarization-sensitive optical coherence tomography. J. Biomed. Opt. 2017, 22. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.M.; Cahill, L.; Liu, K.; MacAulay, C.; Poh, C.; Lane, P. Wide-field in vivo oral oct imaging. Biomed. Opt. Express 2015, 6, 2664–2674. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Verma, Y.; Sahu, K.; Kumar, S.; Varma, A.V.; Kumawat, J.; Gupta, P.K. Human ex-vivo oral tissue imaging using spectral domain polarization sensitive optical coherence tomography. Lasers Med. Sci. 2017, 32, 143–150. [Google Scholar] [CrossRef]
- Kardam, P.; Mehendiratta, M.; Rehani, S.; Kumra, M.; Sahay, K.; Jain, K. Stromal fibers in oral squamous cell carcinoma: A possible new prognostic indicator? J. Oral Maxillofac. Pathol. 2016, 20, 405–412. [Google Scholar] [CrossRef] [Green Version]
- John, R.E.; Murthy, S. Morphological analysis of collagen and elastic fibers in oral squamous cell carcinoma using special stains and comparison with broder’s and bryne’s grading systems. Indian J. Dent. Res. 2016, 27, 242–248. [Google Scholar] [CrossRef]
- Patel, R.; Khan, A.; Quinlan, R.; Yaroslavsky, A.N. Polarization-sensitive multimodal imaging for detecting breast cancer. Cancer Res. 2014, 74, 4685–4693. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Xu, Y.; Mesa, K.J.; South, F.A.; Chaney, E.J.; Spillman, D.R., Jr.; Barkalifa, R.; Marjanovic, M.; Carney, P.S.; Higham, A.M.; et al. Complementary use of polarization-sensitive and standard oct metrics for enhanced intraoperative differentiation of breast cancer. Biomed. Opt. Express 2018, 9, 6519–6528. [Google Scholar] [CrossRef]
- Chi, A.C.; Day, T.A.; Neville, B.W. Oral cavity and oropharyngeal squamous cell carcinoma—An update. CA Cancer J. Clin. 2015, 65, 401–421. [Google Scholar] [CrossRef]
- McGurk, M.; Chan, C.; Jones, J.; O’Regan, E.; Sherriff, M. Delay in diagnosis and its effect on outcome in head and neck cancer. Br. J. Oral Maxillofac Surg 2005, 43, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Volgger, V.; Stepp, H.; Ihrler, S.; Kraft, M.; Leunig, A.; Patel, P.M.; Susarla, M.; Jackson, K.; Betz, C.S. Evaluation of optical coherence tomography to discriminate lesions of the upper aerodigestive tract. Head Neck 2013, 35, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Farah, C.S.; Fox, S.A. Dysplastic oral leukoplakia is molecularly distinct from leukoplakia without dysplasia. Oral Dis. 2019, 25, 1715–1723. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, K.; Girish, H.C.; Murgod, S.; Alshame, A.M.J.; Shyamala, K.; Nayak, V.N. A comparative immunohistochemical study of presence and distribution pattern of stromal myofibroblast in oral dysplasia and in different grades of oral squamous cell carcinoma. J. Int. Soc. Prev. Community Dent. 2018, 8, 451–456. [Google Scholar]
- Sharma, R.; Rehani, S.; Mehendiratta, M.; Kardam, P.; Kumra, M.; Mathias, Y.; Yadav, J.; Sahay, K. Architectural analysis of picrosirius red stained collagen in oral epithelial dysplasia and oral squamous cell carcinoma using polarization microscopy. J. Clin. Diagn. Res. 2015, 9, EC13–EC16. [Google Scholar] [CrossRef]
- Kiseleva, E.; Kirillin, M.; Feldchtein, F.; Vitkin, A.; Sergeeva, E.; Zagaynova, E.; Streltzova, O.; Shakhov, B.; Gubarkova, E.; Gladkova, N. Differential diagnosis of human bladder mucosa pathologies in vivo with cross-polarization optical coherence tomography. Biomed. Opt. Express 2015, 6, 1464–1476. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Kao, M.C.; Lai, C.M.; Huang, J.C.; Kuo, W.C. All fiber optics circular-state swept source polarization-sensitive optical coherence tomography. J. Biomed. Opt. 2013, 19, 21110. [Google Scholar] [CrossRef] [Green Version]
- Syu, J.P.; Buddhakosai, W.; Chen, S.J.; Ke, C.C.; Chiou, S.H.; Kuo, W.C. Supercontinuum source-based multi-contrast optical coherence tomography for rat retina imaging. Biomed. Opt. Express 2018, 9, 6132–6144. [Google Scholar] [CrossRef]
- Wojtkowski, M.; Srinivasan, V.; Ko, T.; Fujimoto, J.; Kowalczyk, A.; Duker, J. Ultrahigh-resolution, high-speed, fourier domain optical coherence tomography and methods for dispersion compensation. Opt. Express 2004, 12, 2404–2422. [Google Scholar] [CrossRef]
- Hitzenberger, C.; Goetzinger, E.; Sticker, M.; Pircher, M.; Fercher, A. Measurement and imaging of birefringence and optic axis orientation by phase resolved polarization sensitive optical coherence tomography. Opt. Express 2001, 9, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.F.; Yang, C.C.; Kao, S.Y.; Liu, C.J.; Lin, S.C.; Chang, K.W. Microrna-211 enhances the oncogenicity of carcinogen-induced oral carcinoma by repressing tcf12 and increasing antioxidant activity. Cancer Res. 2016, 76, 4872–4886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, X.H.; Knudsen, B.; Bemis, D.; Tickoo, S.; Gudas, L.J. Oral cavity and esophageal carcinogenesis modeled in carcinogen-treated mice. Clin. Cancer Res. 2004, 10, 301–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, N.; Blagus, R.; El-Mofty, S.K.; Helliwell, T.; Prasad, M.L.; Sandison, A.; Volavsek, M.; Wenig, B.M.; Zidar, N.; Cardesa, A. Evaluation of a new grading system for laryngeal squamous intraepithelial lesions—A proposed unified classification. Histopathology 2014, 65, 456–464. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mice | Histology | Maximal Tumor Diameter by Histology | Maximal Tumor Diameter by Birefringence Map |
|---|---|---|---|
| 16 weeks | |||
| Control | |||
| Ant. Tongue | Normal | Nil | Nil |
| Pos. Tongue | Normal | Nil | Nil |
| E-Mouse 1 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | Hyperplasia | Nil | Nil |
| E-Mouse 2 | |||
| Ant. Tongue | Dysplasia | 1.41 mm | 1.58 mm |
| Pos. Tongue | Dysplasia | 0.60 mm | 0.70 mm |
| E-Mouse 3 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | Hyperplasia | Nil | Nil |
| 20 weeks | |||
| Control | |||
| Ant. Tongue | Normal | Nil | Nil |
| Pos. Tongue | Normal | Nil | Nil |
| E-Mouse 1 | |||
| Ant. Tongue | Dysplasia | 1.26 mm | 1.53 mm |
| Pos. Tongue | Dysplasia | 1.26 mm | 1.30 mm |
| E-Mouse 2 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | Dysplasia | 0.60 mm | 0.70 mm |
| E-Mouse 3 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | CIS | 3.30 mm | 3.62 mm |
| E-Mouse 4 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | CIS | 1.17 mm | 1.51 mm |
| 24 weeks | |||
| Control | |||
| Ant. Tongue | Normal | Nil | Nil |
| Pos. Tongue | Normal | Nil | Nil |
| E-Mouse 1 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | Hyperplasia | Nil | 0.70 mm |
| E-Mouse 2 | |||
| Ant. Tongue | Multifocal dysplasia | 1.15 mm and 0.46 mm | 1.31 mm and 0.60 mm |
| Pos. Tongue | Hyperplasia | Nil | Nil |
| E-Mouse 3 | |||
| Ant. Tongue | SCC | 1.73 mm | 1.81 mm |
| Pos. Tongue | Dysplasia | 0.70 mm | 0.78 mm |
| E-Mouse 4 | |||
| Ant. Tongue | Dysplasia | 0.71 mm | 1.07 mm |
| Pos. Tongue | Hyperplasia | Nil | Nil |
| 28 weeks | |||
| Control | |||
| Ant. Tongue | Normal | Nil | Nil |
| Pos. Tongue | Normal | Nil | Nil |
| E-Mouse 1 | |||
| Ant. Tongue | Hyperplasia | Nil | Nil |
| Pos. Tongue | Dysplasia | 2.20 mm | 2.64 mm |
| E-Mouse 2 | |||
| Mid. Tongue | Dysplasia | 2.44 mm | 2.61 mm |
| E-Mouse 3 | |||
| Mid. Tongue | Dysplasia | 1.30 mm | 1.43 mm |
| E-Mouse 4 | |||
| Mid. Tongue | Squamous cell carcinoma (SCC) | 3.23 mm | 3.30 mm |
| Histology | Malignancy | Benign | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|
| (Dysplasia–SCC) | (Normal–Hyperplasia) | |||||
| (n = 15) | (n = 20) | |||||
| Birefringence Map | ||||||
| Malignancy | 15 | 1 | 100% | 95% | 93.75% | 100% |
| Benign | 0 | 19 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-H.; Lee, H.-Y.; Chen, Y.-F.; Yeh, Y.-C.; Chang, K.-W.; Hou, M.-C.; Kuo, W.-C. Detection of Oral Dysplastic and Early Cancerous Lesions by Polarization-Sensitive Optical Coherence Tomography. Cancers 2020, 12, 2376. https://doi.org/10.3390/cancers12092376
Chen P-H, Lee H-Y, Chen Y-F, Yeh Y-C, Chang K-W, Hou M-C, Kuo W-C. Detection of Oral Dysplastic and Early Cancerous Lesions by Polarization-Sensitive Optical Coherence Tomography. Cancers. 2020; 12(9):2376. https://doi.org/10.3390/cancers12092376
Chicago/Turabian StyleChen, Ping-Hsien, Hung-Yi Lee, Yi-Fen Chen, Yi-Chen Yeh, Kuo-Wei Chang, Ming-Chih Hou, and Wen-Chuan Kuo. 2020. "Detection of Oral Dysplastic and Early Cancerous Lesions by Polarization-Sensitive Optical Coherence Tomography" Cancers 12, no. 9: 2376. https://doi.org/10.3390/cancers12092376