Muscle Characteristics Obtained Using Computed Tomography as Prognosticators in Patients with Castration-Resistant Prostate Cancer

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
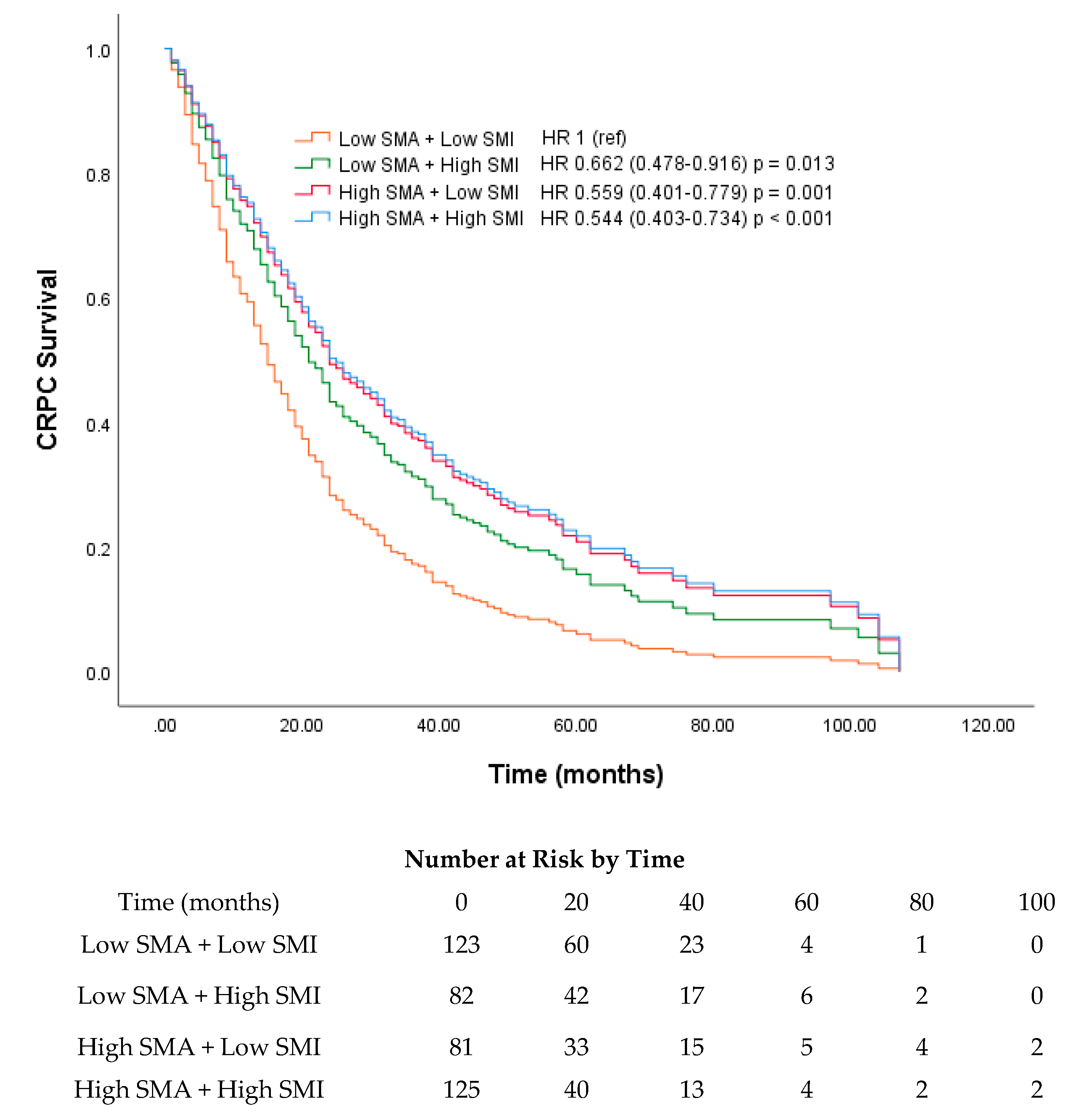
2.2. Muscle Measurements
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Anthropometric and Muscle Characteristic Assessment
4.3. Cut-Off Values for Dichotomization
4.4. Study Endpoints
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G. Definition and classification of cancer cachexia: An international consensus. Lancet 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; Macdonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- Shachar, S.S.; Williams, G.R.; Muss, H.B.; Nishijima, T.F. Prognostic value of sarcopenia in adults with solid tumours: A meta-analysis and systematic review. Eur. J. Cancer 2016, 57, 58–67. [Google Scholar] [CrossRef]
- Aubrey, J.; Esfandiari, N.; Baracos, V.E.; Buteau, F.A.; Frenette, J.; Putman, C.T.; Mazurak, V.C. Measurement of skeletal muscle radiation attenuation and basis of its biological variation. Acta Physiol. 2014, 210, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.J.; Park, J.W.; Kim, J.W.; Park, C.-S.; Gonzalez, J.P.S.; Lee, S.H.; Kim, K.G.; Oh, J.H. Computerized automated quantification of subcutaneous and visceral adipose tissue from computed tomography scans: Development and validation study. JMIR Med. Inform. 2016, 4, e2. [Google Scholar] [CrossRef]
- Bridge, C.P.; Rosenthal, M.; Wright, B.; Kotecha, G.; Fintelmann, F.; Troschel, F.; Miskin, N.; Desai, K.; Wrobel, W.; Babic, A. Fully-automated analysis of body composition from CT in cancer patients using convolutional neural networks. In OR 2.0 Context-Aware Operating Theaters, Computer Assisted Robotic Endoscopy, Clinical Image-Based Procedures, and Skin Image Analysis; Springer: Basel, Switzerland, 2018; pp. 204–213. [Google Scholar]
- Nguyen, P.L.; Alibhai, S.M.; Basaria, S.; D’Amico, A.V.; Kantoff, P.W.; Keating, N.L.; Penson, D.F.; Rosario, D.J.; Tombal, B.; Smith, M.R. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur. Urol. 2015, 67, 825–836. [Google Scholar] [CrossRef]
- Owen, P.J.; Daly, R.M.; Livingston, P.M.; Fraser, S.F. Lifestyle guidelines for managing adverse effects on bone health and body composition in men treated with androgen deprivation therapy for prostate cancer: An update. Prostate Cancer Prostatic Dis. 2017, 20, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Mitsiopoulos, N.; Baumgartner, R.N.; Heymsfield, S.B.; Lyons, W.; Gallagher, D.; Ross, R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J. Appl. Physiol. 1998, 85, 115–122. [Google Scholar] [CrossRef]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St.-Onge, M.-P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowke, J.H.; Motley, S.S.; Concepcion, R.S.; Penson, D.F.; Barocas, D.A. Obesity, body composition, and prostate cancer. BMC Cancer 2012, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pak, S.; Park, S.Y.; Shin, T.J.; You, D.; Jeong, I.G.; Hong, J.H.; Kim, C.S.; Ahn, H. Association of Muscle Mass with Survival after Radical Prostatectomy in Patients with Prostate Cancer. J. Urol. 2019, 202, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Lee, H.S.; Ha, J.S.; Han, K.S.; Rha, K.H.; Hong, S.J.; Chung, B.H.; Koo, K.C. Subcutaneous Fat Distribution is a Prognostic Biomarker for Men with Castration Resistant Prostate Cancer. J. Urol. 2018, 200, 114–120. [Google Scholar] [CrossRef]
- Antoun, S.; Bayar, A.; Ileana, E.; Laplanche, A.; Fizazi, K.; di Palma, M.; Escudier, B.; Albiges, L.; Massard, C.; Loriot, Y. High subcutaneous adipose tissue predicts the prognosis in metastatic castration-resistant prostate cancer patients in post chemotherapy setting. Eur. J. Cancer 2015, 51, 2570–2577. [Google Scholar] [CrossRef]
- van Londen, G.J.; Levy, M.E.; Perera, S.; Nelson, J.B.; Greenspan, S.L. Body composition changes during androgen deprivation therapy for prostate cancer: A 2-year prospective study. Crit. Rev. Oncol./Hematol. 2008, 68, 172–177. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.R.; Saad, F.; Egerdie, B.; Sieber, P.R.; Tammela, T.L.; Ke, C.; Leder, B.Z.; Goessl, C. Sarcopenia during androgen-deprivation therapy for prostate cancer. J. Clin. Oncol. 2012, 30, 3271–3276. [Google Scholar] [CrossRef] [Green Version]
- Haseen, F.; Murray, L.J.; Cardwell, C.R.; O’Sullivan, J.M.; Cantwell, M.M. The effect of androgen deprivation therapy on body composition in men with prostate cancer: Systematic review and meta-analysis. J. Cancer Surviv. 2010, 4, 128–139. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.; Joseph, D.J.; Ebert, M.A.; Galvao, D.A.; Taaffe, D.R.; Denham, J.W.; Newton, R.U.; Spry, N.A. Effect of androgen deprivation therapy on muscle attenuation in men with prostate cancer. J. Med. Imaging Radiat. Oncol. 2014, 58, 223–228. [Google Scholar] [CrossRef]
- van Dijk, D.P.J.; Bakens, M.J.A.M.; Coolsen, M.M.E.; Rensen, S.S.; van Dam, R.M.; Bours, M.J.L.; Weijenberg, M.P.; Dejong, C.H.C.; Olde Damink, S.W.M. Low skeletal muscle radiation attenuation and visceral adiposity are associated with overall survival and surgical site infections in patients with pancreatic cancer. J. Cachexia Sarcopeni. Muscle 2017, 8, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Antoun, S.; Lanoy, E.; Iacovelli, R.; Albiges-Sauvin, L.; Loriot, Y.; Merad-Taoufik, M.; Fizazi, K.; di Palma, M.; Baracos, V.E.; Escudier, B. Skeletal muscle density predicts prognosis in patients with metastatic renal cell carcinoma treated with targeted therapies. Cancer 2013, 119, 3377–3384. [Google Scholar] [CrossRef] [PubMed]
- Kazemi-Bajestani, S.M.; Mazurak, V.C.; Baracos, V. Computed tomography-defined muscle and fat wasting are associated with cancer clinical outcomes. Semin. Cell Dev. Biol. 2016, 54, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.J.; Boorjian, S.A.; Bhindi, B.; Rangel, L.; Frank, I.; Karnes, R.J.; Tollefson, M.K. The Association Between Sarcopenia and Oncologic Outcomes After Radical Prostatectomy. Clin. Genitourin. Cancer 2018, 16, e629–e636. [Google Scholar] [CrossRef] [PubMed]
- Ohtaka, A.; Aoki, H.; Nagata, M.; Kanayama, M.; Shimizu, F.; Ide, H.; Tsujimura, A.; Horie, S. Sarcopenia is a poor prognostic factor of castration-resistant prostate cancer treated with docetaxel therapy. Prostate Int. 2019, 7, 9–14. [Google Scholar] [CrossRef]
- Koo, K.C.; Lee, J.S.; Kim, J.W.; Han, K.S.; Lee, K.S.; Kim, D.K.; Ha, Y.S.; Rha, K.H.; Hong, S.J.; Chung, B.H. Impact of clinical trial participation on survival in patients with castration-resistant prostate cancer: A multi-center analysis. BMC Cancer 2018, 18, 468. [Google Scholar] [CrossRef] [Green Version]
- Baracos, V.E.; Arribas, L. Sarcopenic obesity: Hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann. Oncol. 2018, 29, ii1–ii9. [Google Scholar] [CrossRef]
- Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [CrossRef]
- Mosteller, R.D. Simplified calculation of body-surface area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar]
- Reinders, I.; Murphy, R.A.; Brouwer, I.A.; Visser, M.; Launer, L.; Siggeirsdottir, K.; Eiriksdottir, G.; Gudnason, V.; Jonsson, P.V.; Lang, T.F.; et al. Muscle Quality and Myosteatosis: Novel Associations with Mortality Risk: The Age, Gene/Environment Susceptibility (AGES)-Reykjavik Study. Am. J. Epidemiol. 2015, 183, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, C.S.; Chaves, G.V. Skeletal muscle quality beyond average muscle attenuation: A proposal of skeletal muscle phenotypes to predict short-term survival in patients with endometrial cancer. J. Natl. Compr. Cancer Netw. 2018, 16, 153–160. [Google Scholar] [CrossRef]
- Assel, M.; Sjoberg, D.; Elders, A.; Wang, X.; Huo, D.; Botchway, A.; Delfino, K.; Fan, Y.; Zhao, Z.; Koyama, T.; et al. Guidelines for reporting of statistics for clinical research in urology. BJU Int. 2019, 123, 401–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 411) | Low SMA (<32.4 HU) (n = 206) | High SMA (≥32.4 HU) (n = 205) | p-Value | Low SMI (<45.2 cm2/m2) (n = 207) | High SMI (≥45.2 cm2/m2) (n = 204) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age at CRPC diagnosis, years (IQR) | 70 | (65–76) | 72 | (67–77) | 69 | (63–73) | <0.001 | 72 | (67–77) | 68 | (62–74) | <0.001 |
| BMI > 23 kg/m2 (%) | 250 | 117 | (57) | 133 | (65) | 0.106 | 88 | (43) | 162 | (79) | <0.001 | |
| BSA, m2 (IQR) | 1.73 | (1.64–1.83) | 1.72 | (1.63–1.83) | 1.74 | (1.66–1.85) | 0.137 | 1.7 | (1.60–1.79) | 1.77 | (1.68–1.90) | <0.001 |
| Intermuscular area, cm2 (IQR) | 6.11 | (4.14–8.31) | 7.40 | (5.30–9.51) | 4.89 | (3.57–6.90) | <0.001 | 6.21 | (4.26–8.78) | 6.06 | (4.08–7.87) | 0.328 |
| Age inclusive CCI > 3 (%) | 271 | 122 | (59) | 149 | (73) | 0.005 | 127 | (61) | 144 | (71) | 0.061 | |
| KPS > 70 (%) | 370 | 183 | (92) | 187 | (94) | 0.441 | 185 | (89) | 185 | (91) | 0.701 | |
| PSA at CRPC diagnosis, ng/mL (IQR) | 44.2 | (12.5–159.1) | 63.5 | (14.3–175) | 31.3 | (10.8–110) | 0.006 | 48.5 | (12.4–184) | 39.1 | (12.3–127) | 0.109 |
| Hb at CRPC diagnosis (IQR) | 12.4 | (11.0–13.4) | 11.9 | (10.8–13.1) | 12.7 | (11.3–13.6) | <0.001 | 11.9 | (10.8–13.2) | 12.5 | (11.3–13.4) | 0.009 |
| ALP at CRPC diagnosis (IQR) | 93.0 | (69.0–151.0) | 108 | (75–194) | 86 | (65–140) | 0.004 | 103 | (72–202) | 89 | (66–138) | 0.019 |
| Albumin at CRPC diagnosis (IQR) | 4.2 | (3.9–4.5) | 4.1 | (3.8–4.4) | 4.3 | (4.1–4.6) | <0.001 | 4.1 | (3.9–4.4) | 4.3 | (4.0–4.6) | 0.001 |
| Initial treatment (%) | 0.055 | 0.122 | ||||||||||
| Prostatectomy | 129 | (31) | 73 | (35) | 56 | (27) | 64 | (31) | 65 | (32) | ||
| Radiotherapy | 13 | (3) | 9 | (4) | 4 | (2) | 3 | (1) | 10 | (5) | ||
| Hormonal therapy | 269 | (65) | 124 | (60) | 145 | (71) | 140 | (68) | 129 | (63) | ||
| HSPC ADT period, months (IQR) | 88 | (4–168) | 18 | (12–39) | 27 | (15–43) | 0.004 | 21 | (12–39) | 24 | (14–45) | 0.109 |
| Docetaxel cycle (IQR) | 3 | (5–9) | 3 | (2–7) | 6 | (3–12) | <0.001 | 4 | (2–7) | 6 | (3–11) | <0.001 |
| Metastasis (%) | ||||||||||||
| Bone | 344 | 173 | (84) | 171 | (83) | 0.895 | 179 | (87) | 165 | (81) | 0.142 | |
| Lymph node | 199 | 104 | (51) | 95 | (45) | 0.278 | 90 | (44) | 106 | (52) | 0.094 | |
| Visceral | 70 | 46 | (22) | 24 | (12) | 0.006 | 43 | (21) | 27 | (13) | 0.049 | |
| Overall survival (%) | ||||||||||||
| 1 year | 257 | 107 | (55) | 150 | (81) | <0.001 | 116 | (61) | 141 | (75) | 0.004 | |
| 2 year | 127 | 51 | (29) | 76 | (47) | 0.001 | 53 | (39) | 74 | (45) | 0.005 | |
| 3 year | 78 | 33 | (19) | 45 | (30) | 0.027 | 33 | (20) | 45 | (29) | 0.07 | |
| Clinical trial (%) | 84 | 33 | (16) | 51 | (25) | 0.028 | 43 | (21) | 41 | (20) | 0.903 | |
| Variables | Univariate | Multivariate a | ||||
|---|---|---|---|---|---|---|
| HR | CI | p-Value | HR | CI | p-Value | |
| Age at CRPC diagnosis | 1.01 | (0.99–1.02) | 0.526 | |||
| BMI (<23 vs. ≥23 kg/m2) | 0.60 | (0.48–0.76) | <0.001 | 0.85 | (0.62–1.17) | 0.329 |
| BSA for every 0.2 increase | 0.71 | (0.61–0.83) | <0.001 | 0.83 | (0.67–1.03) | 0.084 |
| Age inclusive CCI (<4 vs. ≥4) | 1.04 | (0.81–1.33) | 0.777 | |||
| KPS (≥70 vs. <70) | 1.85 | (1.24–2.78) | 0.003 | 0.89 | (0.54–1.46) | 0.649 |
| PSA at CRPC diagnosis for every 1.0 increase | 1.00 | (1.00–1.00) | <0.001 | 1.00 | (1.00–1.00) | <0.001 |
| Hb at CRPC diagnosis for every 1.0 increase | 0.77 | (0.72–0.82) | <0.001 | 0.88 | (0.81–0.95) | 0.002 |
| ALP at CRPC diagnosis for every 1.0 increase | 1.00 | (1.00–1.00) | <0.001 | 1.00 | (1.00–1.00) | <0.001 |
| Albumin at CRPC diagnosis for every 1.0 increase | 0.49 | (0.38–0.63) | <0.001 | 1.02 | (0.73–1.44) | 0.899 |
| Bone metastasis (no vs. yes) | 1.88 | (1.30–2.72) | 0.001 | 1.55 | (1.04–2.32) | 0.03 |
| Lymph node metastasis (no vs. yes) | 1.43 | (1.14–1.81) | 0.002 | 1.56 | (1.20–2.01) | 0.001 |
| Visceral metastasis (no vs. yes) | 2.35 | (1.77–3.13) | <0.001 | 2.00 | (1.47–2.73) | <0.001 |
| SMI (low vs. high) | 0.75 | (0.60–0.95) | 0.017 | 1.01 | (0.78–1.32) | 0.92 |
| SMA (low vs. high) | 0.65 | (0.52–0.83) | <0.001 | 0.70 | (0.55–0.90) | 0.005 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Park, J.S.; Heo, J.E.; Ahn, H.K.; Jang, W.S.; Ham, W.S.; Rha, K.H.; Choi, Y.D. Muscle Characteristics Obtained Using Computed Tomography as Prognosticators in Patients with Castration-Resistant Prostate Cancer. Cancers 2020, 12, 1864. https://doi.org/10.3390/cancers12071864
Lee J, Park JS, Heo JE, Ahn HK, Jang WS, Ham WS, Rha KH, Choi YD. Muscle Characteristics Obtained Using Computed Tomography as Prognosticators in Patients with Castration-Resistant Prostate Cancer. Cancers. 2020; 12(7):1864. https://doi.org/10.3390/cancers12071864
Chicago/Turabian StyleLee, Jongsoo, Jee Soo Park, Ji Eun Heo, Hyun Kyu Ahn, Won Sik Jang, Won Sik Ham, Koon Ho Rha, and Young Deuk Choi. 2020. "Muscle Characteristics Obtained Using Computed Tomography as Prognosticators in Patients with Castration-Resistant Prostate Cancer" Cancers 12, no. 7: 1864. https://doi.org/10.3390/cancers12071864