Clinical Significance of Systemic Inflammation Markers in Newly Diagnosed, Previously Untreated Hepatocellular Carcinoma

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patients
2.2. Prognostic Significance and Optimal Cut-Off Values of Systemic Inflammation Markers for OS
2.3. Correlation Analysis between SIMs and Other Prognostic Factors
2.4. Prognostic Significance of SIMs on OS in Multivariate Analysis
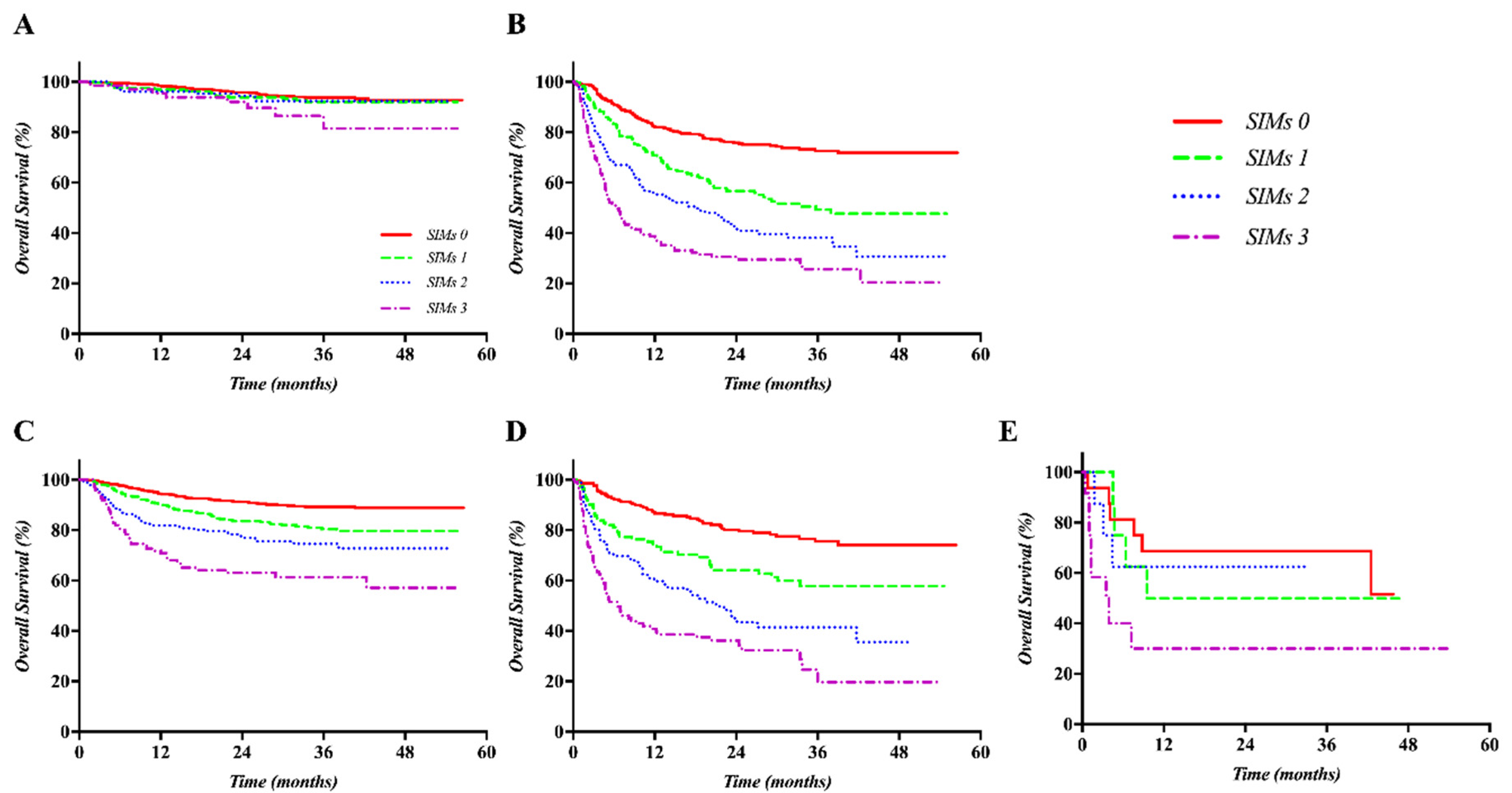
2.5. Clinical Significance of SIMs in the Validation Set
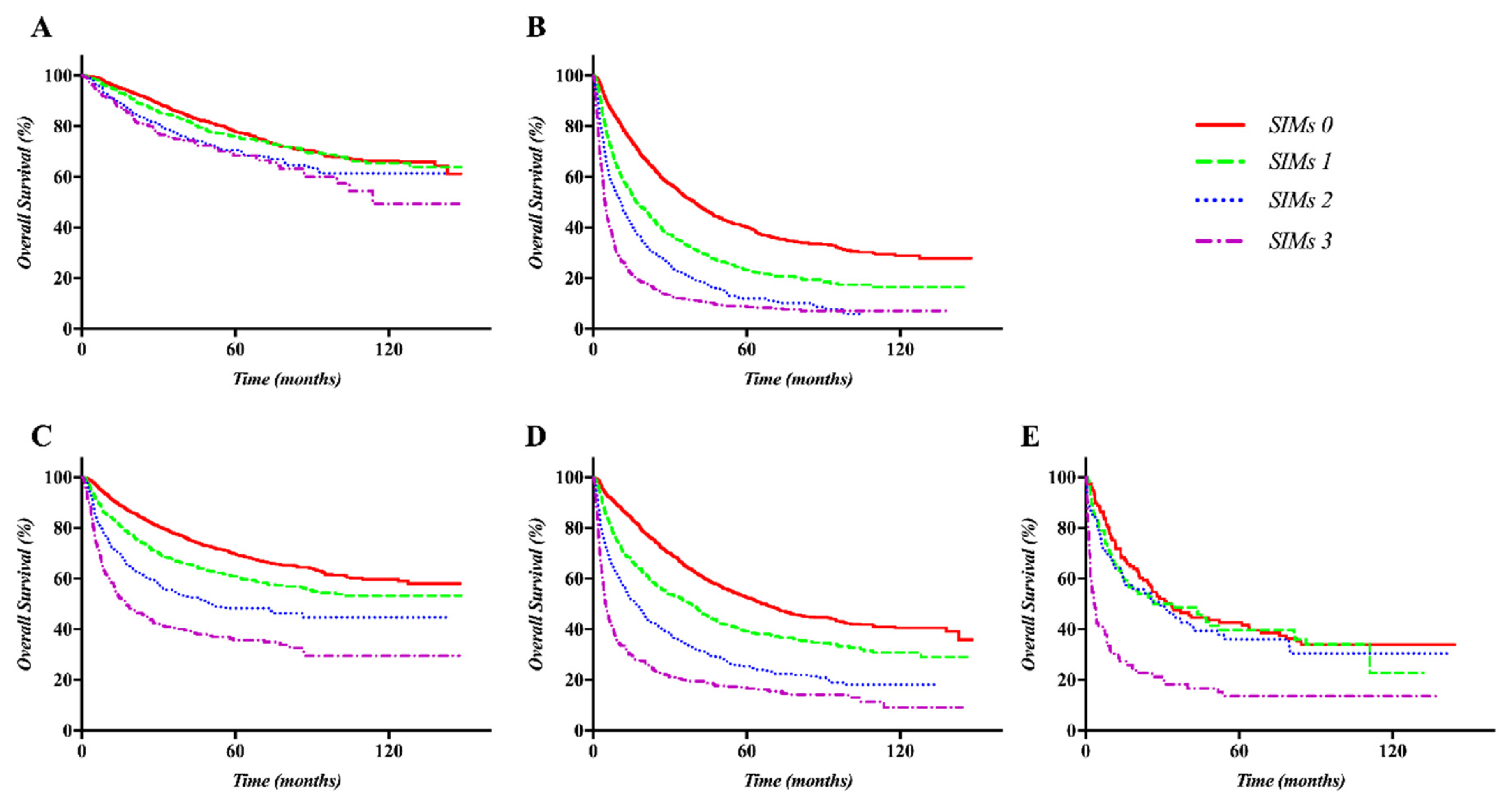
2.6. OS According to the Prognostic Model Based on SIMs in the Training and Validation Sets
3. Discussion
4. Materials and Methods
4.1. Cohorts from the Samsung Medical Center HCC Registry
4.2. Laboratoristic Methodology for Blood Count
4.3. Training Set
4.4. Validation Set
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HCC | Hepatocellular carcinoma |
| AJCC | American Joint Committee on Cancer |
| UICC | International Union Against Cancer |
| ALBI | Albumin-bilirubin |
| NLR | Neutrophil-to-lymphocyte ratio |
| PLR | Platelet-to-lymphocyte ratio |
| LMR | Lymphocyte-to-monocyte ratio |
| SIMs | systemic inflammation markers |
| GPS | Glasgow Prognostic Score |
| HSI | hepatic steatosis index |
| RFA | radiofrequency ablation |
| TACE | trans-arterial chemoembolization |
| BCLC | Barcelona Clinic Liver Cancer |
| ECOG | Eastern Cooperative Oncology Group |
| AFP | alpha-fetoprotein |
| PIVKA-II | Protein induced by vitamin K absence or antagonist-II |
| OS | overall survival |
| PVI | portal vein invasion |
| HR | hazard ratio |
| CI | confidence interval |
References
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar]
- Abdel-Rahman, O. Assessment of the discriminating value of the 8th AJCC stage grouping for hepatocellular carcinoma. Hpb Off. J. Int. Hepato Pancreato Biliary Assoc. 2018, 20, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Kudo, M.; Hirooka, M.; Tsuji, K.; Itobayashi, E.; Kariyama, K.; Ishikawa, T.; Tajiri, K.; Ochi, H.; et al. Albumin-Bilirubin (ALBI) Grade as Part of the Evidence-Based Clinical Practice Guideline for HCC of the Japan Society of Hepatology: A Comparison with the Liver Damage and Child- Pugh classifications. Liver Cancer 2017, 6, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Zhu, A.X.; Farah, W.; Almasri, J.; Zaiem, F.; Prokop, L.J.; Murad, M.H.; Mohammed, K. Therapies for advanced stage hepatocellular carcinoma with macrovascular invasion or metastatic disease: A systematic review and meta-analysis. Hepatology (Baltim. Md.) 2018, 67, 422–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Tsuji, K.; Takaguchi, K.; Itobayashi, E.; Kariyama, K.; Ochi, H.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Validation of Modified ALBI Grade for More Detailed Assessment of Hepatic Function in Hepatocellular Carcinoma Patients: A Multicenter Analysis. Liver Cancer 2019, 8, 121–129. [Google Scholar] [CrossRef]
- Hu, G.; Liu, Q.; Ma, J.Y.; Liu, C.Y. Prognostic Significance of Platelet-to-Lymphocyte Ratio in Cholangiocarcinoma: A Meta-Analysis. Biomed. Res. Int. 2018, 2018, 7375169. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.Y.; Hu, G.; Liu, Q. Prognostic Significance of the Lymphocyte-to-Monocyte Ratio in Bladder Cancer Undergoing Radical Cystectomy: A Meta-Analysis of 5638 Individuals. Dis. Mark. 2019, 2019, 7593560. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; McNamara, M.G.; Seruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocana, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Park, E.Y.; Kim, Y.S.; Choi, K.H.; Song, J.H.; Lee, H.C.; Hong, S.H.; Kang, J.H. Prognostic value of neutrophil-to-lymphocyte ratio in locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy. Radiat. Oncol. J. 2019, 37, 166–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, X.; Li, J.; Deng, H.; Li, H.; Su, C.; Guo, X. Neutrophil-to-lymphocyte ratio for the prognostic assessment of hepatocellular carcinoma: A systematic review and meta-analysis of observational studies. Oncotarget 2016, 7, 45283–45301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Tanaka, K.; Fushiya, N.; Koike, K.; Nishino, H.; Matsushima, M.; et al. The Glasgow Prognostic Score, an inflammation based prognostic score, predicts survival in patients with hepatocellular carcinoma. BMC Cancer 2013, 13, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Xu, R.; Huang, H.; Zhang, Z.; Wang, F.S. The role of neutrophils in the development of liver diseases. Cell. Mol. Immunol. 2014, 11, 224–231. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Uria, G.; Day, J.N.; Nasir, A.J.; Russell, S.K.; Vilar, F.J. Reduction in neutrophil count during hepatitis C treatment: Drug toxicity or predictor of good response? Dig. Dis. Sci. 2010, 55, 2058–2062. [Google Scholar] [CrossRef]
- Kang, C.; Jeong, S.Y.; Song, S.Y.; Choi, E.K. The emerging role of myeloid-derived suppressor cells in radiotherapy. Radiat. Oncol. J. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Coffelt, S.B.; Wellenstein, M.D.; de Visser, K.E. Neutrophils in cancer: Neutral no more. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef] [Green Version]
- Bald, T.; Quast, T.; Landsberg, J.; Rogava, M.; Glodde, N.; Lopez-Ramos, D.; Kohlmeyer, J.; Riesenberg, S.; van den Boorn-Konijnenberg, D.; Homig-Holzel, C.; et al. Ultraviolet-radiation-induced inflammation promotes angiotropism and metastasis in melanoma. Nature 2014, 507, 109–113. [Google Scholar] [CrossRef]
- Menter, D.G.; Tucker, S.C.; Kopetz, S.; Sood, A.K.; Crissman, J.D.; Honn, K.V. Platelets and cancer: A casual or causal relationship: Revisited. Cancer Metastasis Rev. 2014, 33, 231–269. [Google Scholar] [CrossRef] [Green Version]
- Pang, Q.; Zhang, J.Y.; Xu, X.S.; Song, S.D.; Qu, K.; Chen, W.; Zhou, Y.Y.; Miao, R.C.; Liu, S.S.; Dong, Y.F.; et al. Significance of platelet count and platelet-based models for hepatocellular carcinoma recurrence. World J. Gastroenterol. 2015, 21, 5607–5621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyo, J.S.; Sohn, J.H.; Kang, G. Diagnostic and prognostic roles of the mean platelet volume in malignant tumors: A systematic review and meta-analysis. Platelets 2016, 27, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Pang, Q.; Qu, K.; Zhang, J.Y.; Song, S.D.; Liu, S.S.; Tai, M.H.; Liu, H.C.; Liu, C. The Prognostic Value of Platelet Count in Patients With Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Medicine 2015, 94, e1431. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Jenrow, K.A.; Brown, S.L. Novel biological strategies to enhance the radiation therapeutic ratio. Radiat. Oncol. J. 2018, 36, 172–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhang, C. The Roles of Liver-Resident Lymphocytes in Liver Diseases. Front. Immunol. 2019, 10, 1582. [Google Scholar] [CrossRef]
- Yao, W.; He, J.C.; Yang, Y.; Wang, J.M.; Qian, Y.W.; Yang, T.; Ji, L. The Prognostic Value of Tumor-infiltrating Lymphocytes in Hepatocellular Carcinoma: A Systematic Review and Meta-analysis. Sci. Rep. 2017, 7, 7525. [Google Scholar] [CrossRef]
- Wang, M.; Li, C.; Wen, T.F.; Peng, W.; Chen, L.P. Postoperative Low Absolute Lymphocyte Counts may Predict Poor Outcomes of Hepatocellular Carcinoma After Liver Resection. Chin. Med. J. 2016, 129, 536–541. [Google Scholar] [CrossRef]
- Sasaki, A.; Iwashita, Y.; Shibata, K.; Matsumoto, T.; Ohta, M.; Kitano, S. Prognostic value of preoperative peripheral blood monocyte count in patients with hepatocellular carcinoma. Surgery 2006, 139, 755–764. [Google Scholar] [CrossRef]
- Pages, F.; Mlecnik, B.; Marliot, F.; Bindea, G.; Ou, F.S.; Bifulco, C.; Lugli, A.; Zlobec, I.; Rau, T.T.; Berger, M.D.; et al. International validation of the consensus Immunoscore for the classification of colon cancer: A prognostic and accuracy study. Lancet (Lond. Engl.) 2018, 391, 2128–2139. [Google Scholar] [CrossRef]
- Gibney, G.T.; Weiner, L.M.; Atkins, M.B. Predictive biomarkers for checkpoint inhibitor-based immunotherapy. Lancet. Oncol. 2016, 17, e542–e551. [Google Scholar] [CrossRef] [Green Version]
- Nixon, A.B.; Schalper, K.A.; Jacobs, I.; Potluri, S.; Wang, I.M.; Fleener, C. Peripheral immune-based biomarkers in cancer immunotherapy: Can we realize their predictive potential? J. Immunother. Cancer 2019, 7, 325. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Yu, J.I.; Park, H.C.; Park, S.Y.; Shin, J.S.; Shin, E.H.; Cho, S.; Jung, S.H.; Han, Y.Y.; Lim, D.H. Is higher dose always the right answer in stereotactic body radiation therapy for small hepatocellular carcinoma? Radiat. Oncol. J. 2018, 36, 129–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.I.; Yoo, G.S.; Cho, S.; Jung, S.H.; Han, Y.; Park, S.; Lee, B.; Kang, W.; Sinn, D.H.; Paik, Y.H.; et al. Initial clinical outcomes of proton beam radiotherapy for hepatocellular carcinoma. Radiat. Oncol. J. 2018, 36, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Sinn, D.H.; Choi, G.S.; Park, H.C.; Kim, J.M.; Kim, H.; Song, K.D.; Kang, T.W.; Lee, M.W.; Rhim, H.; Hyun, D.; et al. Multidisciplinary approach is associated with improved survival of hepatocellular carcinoma patients. PLoS ONE 2019, 14, e0210730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korean Liver Cancer Study Group; National Cancer Center; Korea. 2014 Korean Liver Cancer Study Group-National Cancer Center Korea practice guideline for the management of hepatocellular carcinoma. Korean J. Radiol. 2015, 16, 465–522. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Training Set (n = 6619) | Validation Set (n = 2084) | p-Value |
|---|---|---|---|
| Age (years) | <0.001 | ||
| Median | 57 | 59 | |
| Range | 13–88 | 21–89 | |
| Sex | 0.64 | ||
| Male | 2875 (82.0) | 2411 (77.5) | |
| Female | 633 (18.0) | 699 (22.5) | |
| ECOG performance status | <0.001 | ||
| 0 | 6020 (91.0) | 2004 (97.9) | |
| 1 | 467 (7.1) | 41 (8.1) | |
| 2 | 62 (0.9) | 1 (0.0) | |
| 3 | 46 (0.7) | 0 (0.0) | |
| 4 | 24 (0.4) | 1 (0.0) | |
| Cause of hepatitis | 0.002 | ||
| HBV | 4970 (75.1) | 1554 (74.6) | |
| HCV | 640 (9.7) | 182 (8.7) | |
| HBV/HCV | 59 (0.9) | 19 (0.9) | |
| Alcohol | 287 (4.3) | 134 (6.4) | |
| Unknown | 663 (10.0) | 195 (9.4) | |
| Child-Turcotte-Pugh class | <0.001 | ||
| A | 5602 (84.6) | 1856 (89.1) | |
| B | 895 (13.5) | 199 (9.5) | |
| C | 122 (1.8) | 29 (1.4) | |
| BCLC stage | <0.001 | ||
| 0 | 1020 (15.4) | 398 (19.1) | |
| A | 3016 (45.6) | 789 (39.7) | |
| B | 761 (11.5) | 175 (8.4) | |
| C | 1643 (24.8) | 694 (33.3) | |
| D | 179 (2.7) | 28 (1.3) | |
| ALBI grade | <0.001 | ||
| I | 3509 (53.0) | 1503 (72.1) | |
| II | 2787 (42.1) | 537 (25.8) | |
| III | 323 (4.9) | 44 (2.1) | |
| Portal vein invasion | <0.001 | ||
| Vp0 | 5489 (82.9) | 1476 (70.9) | |
| Vp1 | 431 (6.5) | 336 (16.1) | |
| Vp2 | 182 (2.7) | 1 (0.0) | |
| Vp3 | 125 (1.9) | 137 (6.6) | |
| Vp4 | 392 (5.9) | 133 (6.4) | |
| T stage | 0.19 | ||
| 1 | 1218 (18.4) | 366 (18.2) | |
| 2 | 2916 (44.1) | 856 (42.5) | |
| 3 | 1953 (29.5) | 602 (29.9) | |
| 4 | 532 (8.0) | 191 (9.5) | |
| N stage | 0.88 | ||
| 0 | 6195 (93.6) | 1952 (93.7) | |
| 1 | 424 (6.4) | 131 (6.3) | |
| M stage | <0.001 | ||
| 0 | 6313 (95.4) | 2026 (97.3) | |
| 1 | 306 (4.6) | 57 (2.7) | |
| AFP (ng/mL) | <0.001 | ||
| Median | 38 | 20 | |
| Range | 1–600,000 | 1–200,000 | |
| PIVKA-II (mAU/mL) | <0.001 | ||
| Median | 53 | 77 | |
| Range | 2–75,000 | 6–75,000 | |
| Primary treatment | <0.001 | ||
| Liver transplantation | 130 (2.0) | 21 (1.0) | |
| Hepatectomy | 1873 (28.3) | 781 (37.5) | |
| Radiofrequency ablation | 1321 (20.0) | 350 (16.8) | |
| TACE | 2630 (39.7) | 693 (33.3) | |
| Systemic therapy | 255 (3.9) | 77 (3.7) | |
| Radiotherapy | 32 (0.5) | 37 (1.8) | |
| None | 378 (5.7) | 125 (6.0) | |
| NLR | 0.006 | ||
| Median | 1.8 | 1.88 | |
| Range | 0.1–47.8 | 0.3–46.9 | |
| PLR | <0.001 | ||
| Median | 82.1 | 88.5 | |
| Range | 2.8–793.7 | 13.0–1491.7 | |
| LMR | 0.01 | ||
| Median | 4.0 | 3.9 | |
| Range | 0.3–92.0 | 0.2–40.0 |
| Variables | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (years) | 1.001 | 0.997–1.004 | 0.61 | |
| Sex | Female | 1 | - | <0.0001 |
| Male | 1.211 | 1.108–1.323 | ||
| ECOG performance status | 0–1 | 1 | - | <0.0001 |
| 2–4 | 3.229 | 2.680–3.891 | ||
| Etiology | HBV | 1 | - | 0.24 |
| HCV | 0.952 | 0.846–1.072 | ||
| Alcohol | 0.847 | 0.706–1.017 | ||
| Others | 0.953 | 0.853–1.065 | ||
| ALBI grade | I | 1 | - | <0.0001 |
| II | 1.931 | 1.797–2.075 | ||
| III | 2.392 | 2.073–2.759 | ||
| AFP | <100 ng/mL | 1 | - | <0.0001 |
| ≥100 ng/mL | 2.392 | 2.232–2.562 | ||
| PIVKA-II | <100 IU/mL | 1 | - | <0.0001 |
| ≥100 IU/mL | 3.271 | 3.042–3.518 | ||
| T stage | 1 | 1 | - | <0.0001 |
| 2 | 1.988 | 1.746–2.264 | ||
| 3 | 5.100 | 4.484–5.801 | ||
| 4 | 14.488 | 12.477–16.823 | ||
| N stage | 0 | 1 | - | <0.0001 |
| 1 | 3.977 | 3.556–4.448 | ||
| M stage | 0 | 1 | - | <0.0001 |
| 1 | 7.537 | 6.654–8.537 | ||
| Portal vein invasion | Vp0 | 1 | - | <0.0001 |
| Vp1 | 4.353 | 3.887–4.875 | ||
| Vp2 | 4.862 | 4.119–5.739 | ||
| Vp3 | 6.996 | 5.771–8.481 | ||
| Vp4 | 8.581 | 7.653–9.622 | ||
| Treatment aim | Curative | 1 | - | <0.0001 |
| Palliative | 1.248 | 0.847–1.839 | ||
| None | 4.265 | 2.920–6.230 | ||
| NLR | <3.0 | 1 | - | <0.0001 |
| ≥3.0 | 2.501 | 2.318–2.698 | ||
| PRL | <100.0 | 1 | - | <0.0001 |
| ≥100.0 | 1.863 | 1.737–1.997 | ||
| LMR | >3.0 | 1 | - | <0.0001 |
| ≤3.0 | 2.343 | 2.181–2.517 | ||
| Variables | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Sex | Female | 1 | - | 0.008 |
| Male | 1.138 | 1.035–1.252 | ||
| ECOG performance status | 0–1 | 1 | - | 0.01 |
| 2–4 | 1.304 | 1.062–1.600 | ||
| ALBI grade | I | 1 | - | <0.0001 |
| II | 1.746 | 1.617–1.884 | ||
| III | 1.786 | 1.518–2.101 | ||
| AFP | <100 ng/mL | 1 | - | <0.0001 |
| ≥100 ng/mL | 1.483 | 1.372–1.602 | ||
| PIVKA-II | <100 IU/mL | 1 | - | <0.0001 |
| ≥100 IU/mL | 1.620 | 1.488–1.764 | ||
| T stage | 1 | 1 | - | <0.0001 |
| 2 | 1.375 | 1.198–1.578 | ||
| 3 | 1.812 | 1.562–2.103 | ||
| 4 | 2.291 | 1.883–2.786 | ||
| N stage | 0 | 1 | - | 0.001 |
| 1 | 1.233 | 1.088–1.397 | ||
| M stage | 0 | 1 | - | <0.0001 |
| 1 | 2.219 | 1.922–2.562 | ||
| Portal vein invasion | Vp0 | 1 | - | <0.0001 |
| Vp1 | 1.545 | 1.344–1.775 | ||
| Vp2 | 1.661 | 1.377–2.002 | ||
| Vp3 | 1.713 | 1.358–2.161 | ||
| Vp4 | 2.135 | 1.841–2.475 | ||
| Treatment aim | Curative | 1 | - | <0.0001 |
| Palliative | 2.696 | 2.462–2.952 | ||
| None | 10.025 | 8.496–11.829 | ||
| NLR | <3.0 | 1 | - | <0.0001 |
| ≥3.0 | 1.261 | 1.141–1.393 | ||
| PRL | <100.0 | 1 | - | <0.0001 |
| ≥100.0 | 1.249 | 1.145–1.361 | ||
| LMR | >3.0 | 1 | - | <0.0001 |
| ≤3.0 | 1.163 | 1.062–1.273 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, J.I.; Park, H.C.; Yoo, G.S.; Paik, S.W.; Choi, M.S.; Kim, H.-S.; Sohn, I.; Nam, H. Clinical Significance of Systemic Inflammation Markers in Newly Diagnosed, Previously Untreated Hepatocellular Carcinoma. Cancers 2020, 12, 1300. https://doi.org/10.3390/cancers12051300
Yu JI, Park HC, Yoo GS, Paik SW, Choi MS, Kim H-S, Sohn I, Nam H. Clinical Significance of Systemic Inflammation Markers in Newly Diagnosed, Previously Untreated Hepatocellular Carcinoma. Cancers. 2020; 12(5):1300. https://doi.org/10.3390/cancers12051300
Chicago/Turabian StyleYu, Jeong Il, Hee Chul Park, Gyu Sang Yoo, Seung Woon Paik, Moon Seok Choi, Hye-Seung Kim, Insuk Sohn, and Heerim Nam. 2020. "Clinical Significance of Systemic Inflammation Markers in Newly Diagnosed, Previously Untreated Hepatocellular Carcinoma" Cancers 12, no. 5: 1300. https://doi.org/10.3390/cancers12051300