Chemoembolization Plus Radiotherapy versus Chemoembolization Plus Sorafenib for the Treatment of Hepatocellular Carcinoma Invading the Portal Vein: A Propensity Score Matching Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Transarterial Chemoembolization
2.3. External Beam Radiation Therapy
2.4. Sorafenib Therapy
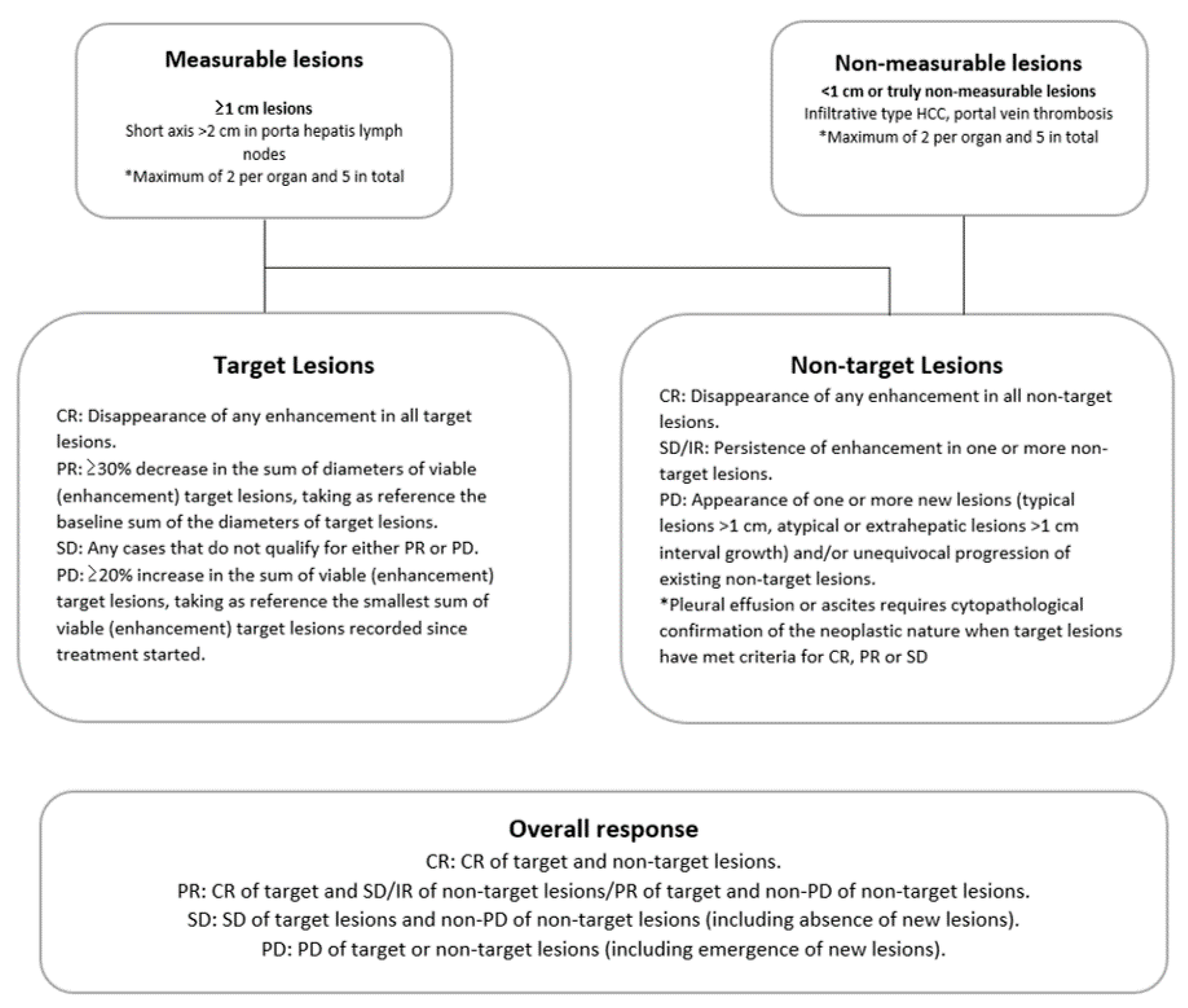
2.5. Definition and Data Assessments
3. Results
3.1. Patients
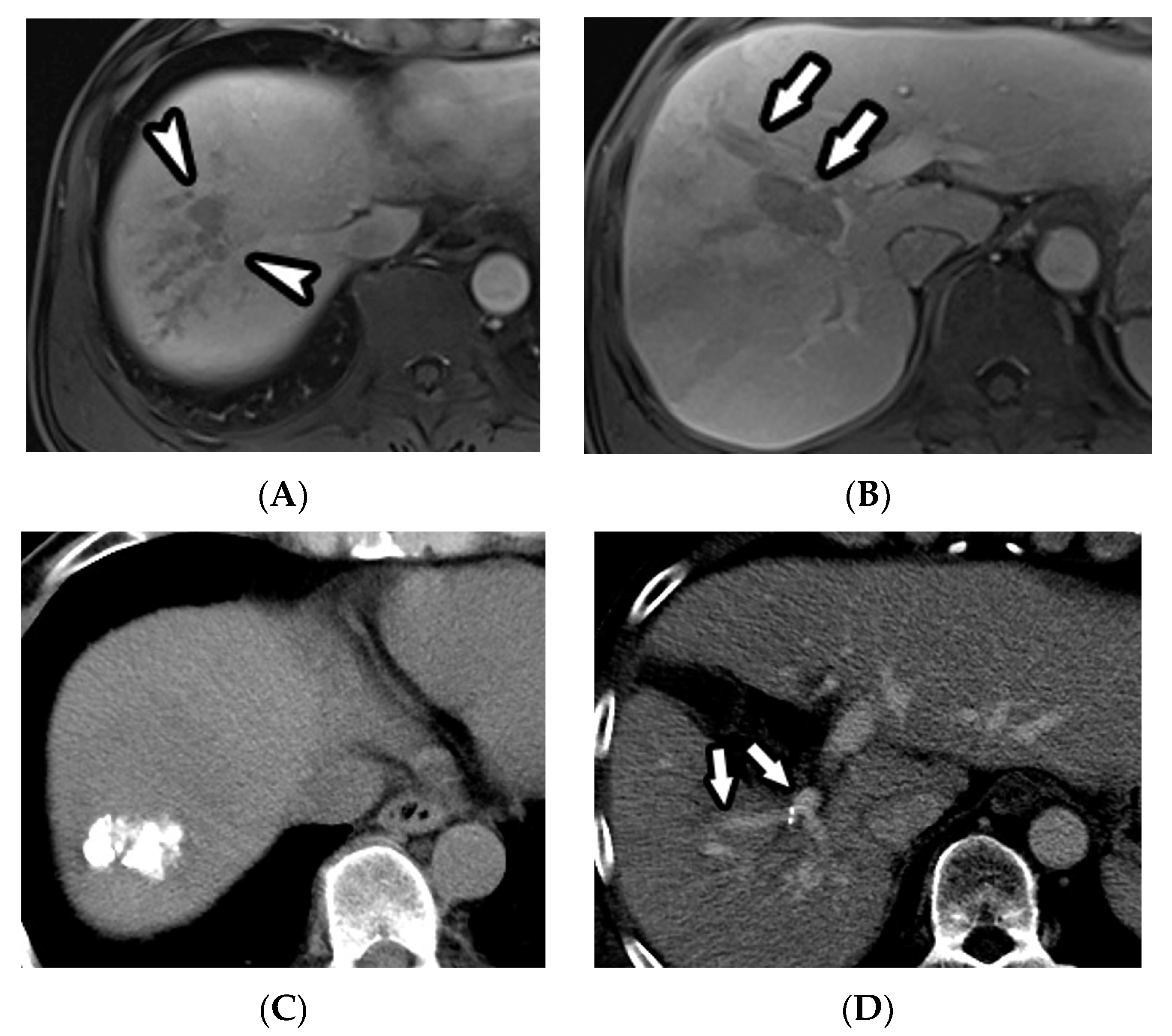
3.2. Radiologic Response after Treatment
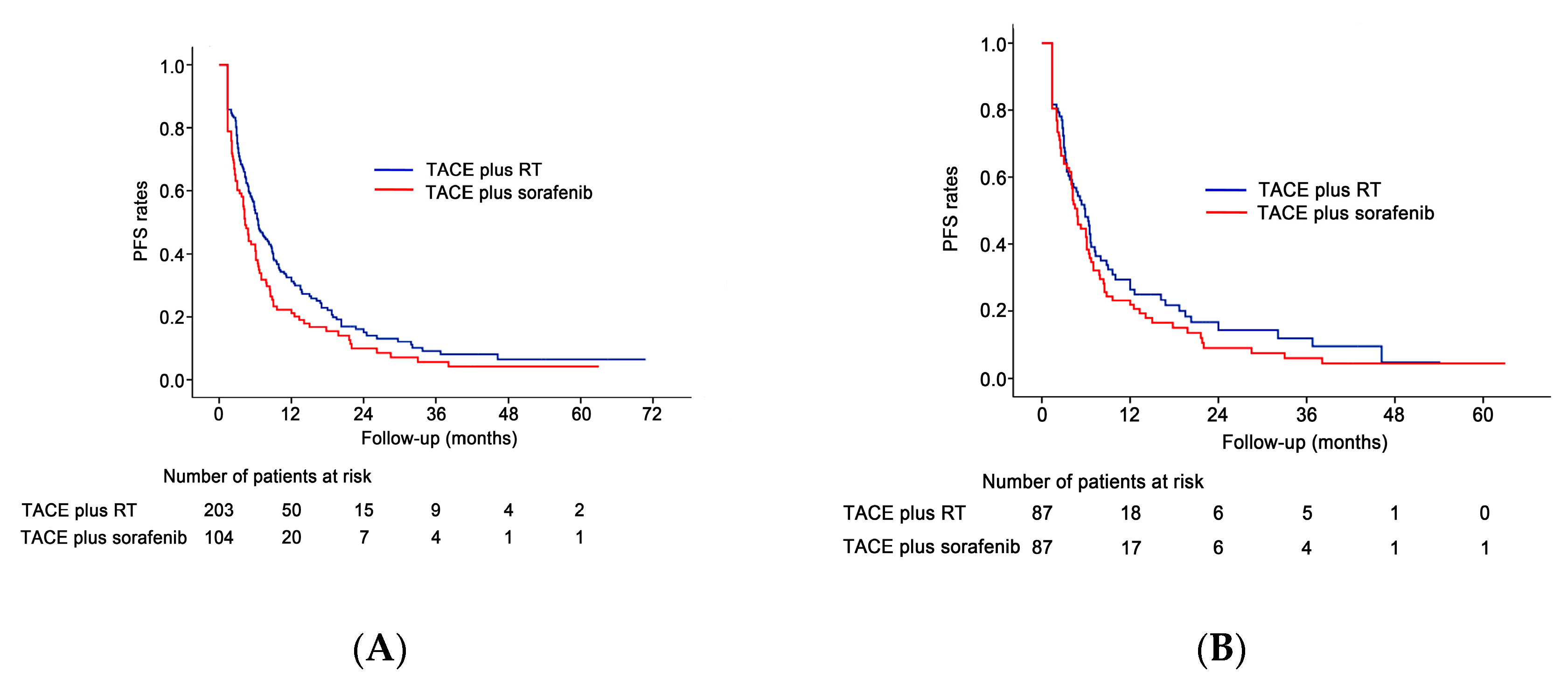
3.3. Progression-Free Survival Analyses
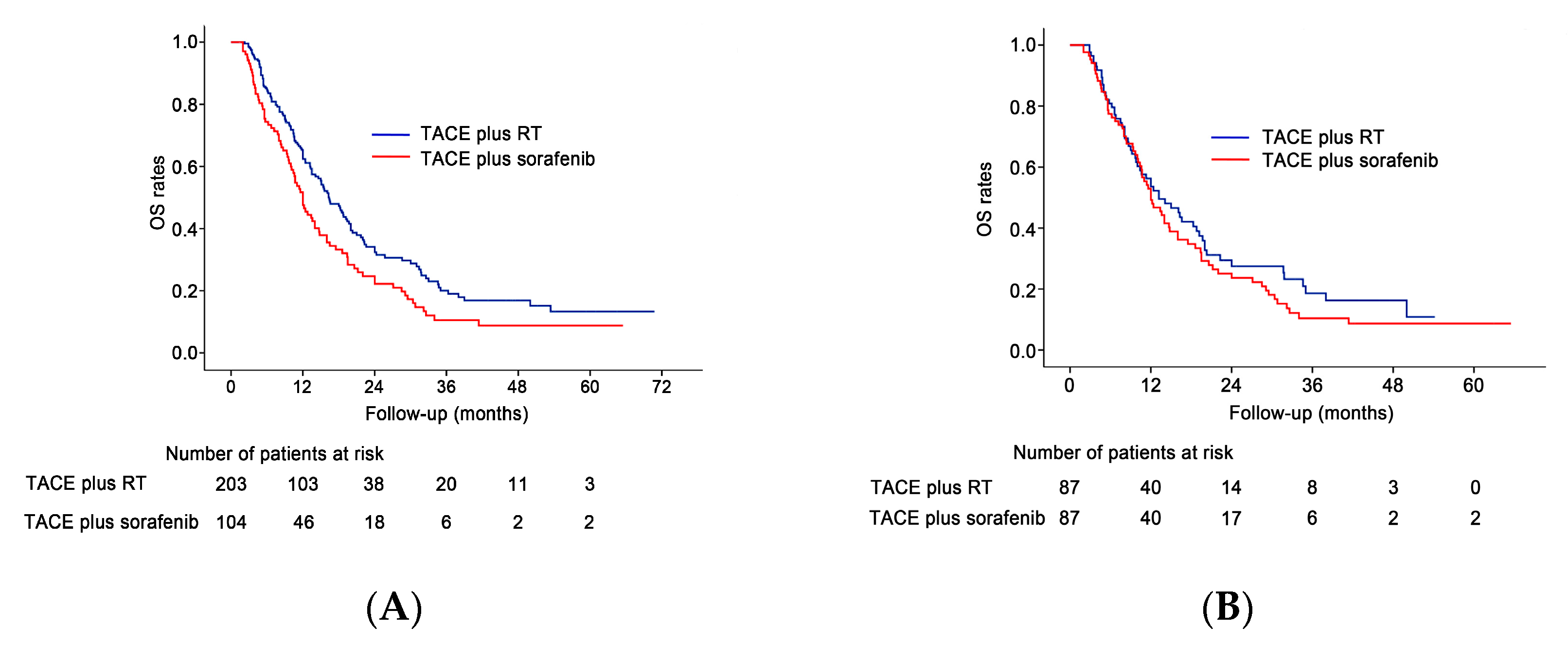
3.4. Overall Survival Analyses
3.5. Multivariable Analyses
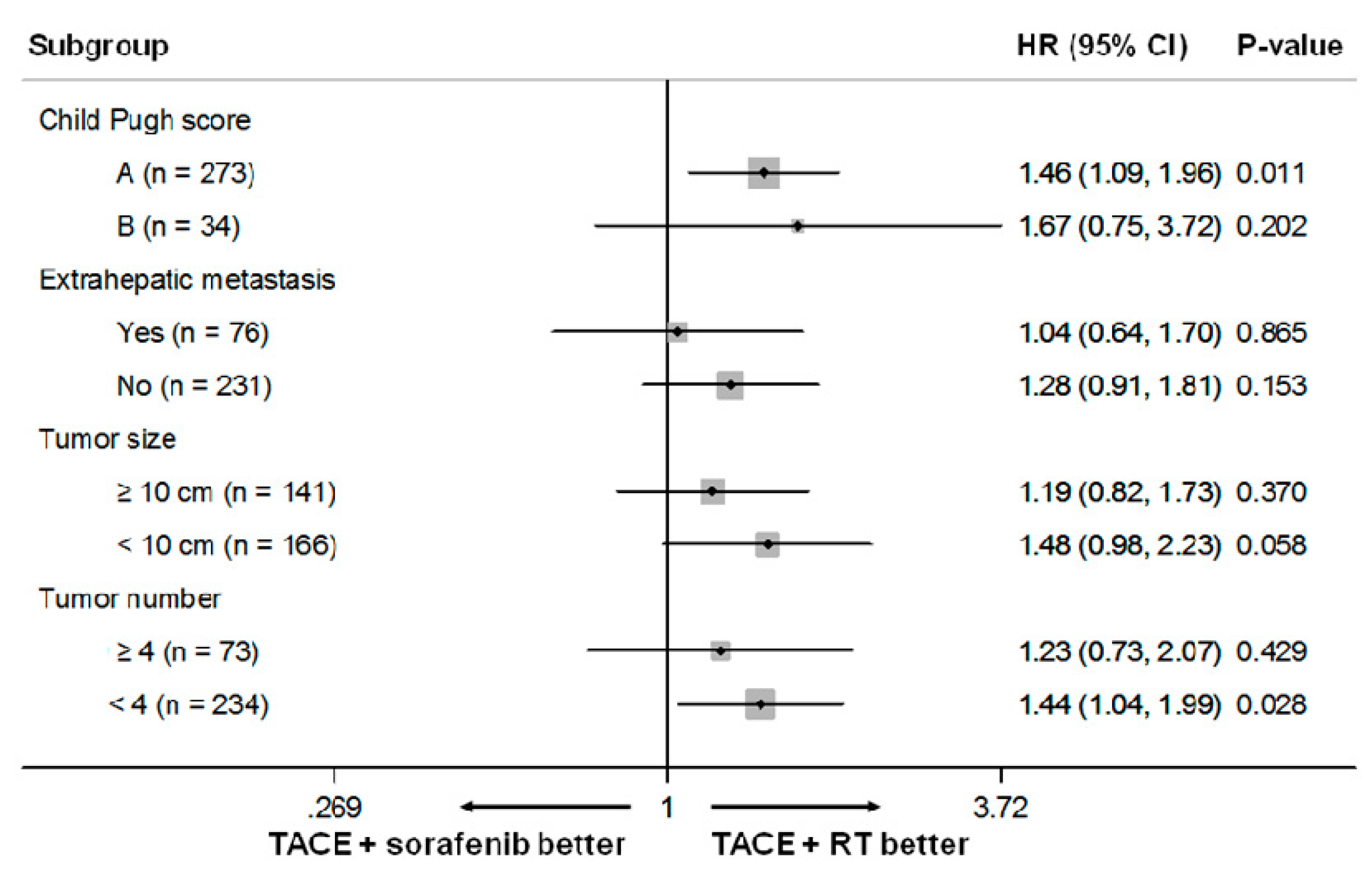
3.6. Subgroup Analyses
3.7. Major Complications (Grade 3 or 4 Toxicities)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcionoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcionoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Bruix, J.; Cheng, A.L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, J.M.; Bustamante, J.; Castells, A.; Vilana, R.; Ayuso Mdel, C.; Sala, M.; Bru, C.; Rodes, J.; Bruix, J. Natural history of untreated nonsurgical hepatocellular carcinoma: Rationale for the design and evaluation of therapeutic trials. Hepatology 1999, 29, 62–67. [Google Scholar] [CrossRef]
- Schöniger-Hekele, M.; Müller, C.; Kutilek, M.; Oesterreicher, C.; Ferenci, P.; Gangl, A. Hepatocellular carcinoma in Central Europe: Prognostic features and survival. Gut 2001, 48, 103–109. [Google Scholar] [CrossRef]
- Cabibbo, G.; Enea, M.; Attanasio, M.; Bruix, J.; Craxì, A.; Cammà, C. A meta-analysis of survival rates of untreated patients in randomized clinical trials of hepatocellular carcinoma. Hepatology 2010, 51, 1274–1283. [Google Scholar] [CrossRef] [Green Version]
- Chung, G.E.; Lee, J.H.; Kim, H.Y.; Hwang, S.Y.; Kim, J.S.; Chung, J.W.; Yoon, J.H.; Lee, H.S.; Kim, Y.J. Transarterial chemoembolization can be safely performed in patients with hepatocellular carcinoma invading the main portal vein and may improve the overall survival. Radiology 2011, 258, 627–634. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.M.; Kim, J.H.; Park, I.S.; Ko, G.Y.; Yoon, H.K.; Sung, K.B.; Lim, Y.S.; Lee, H.C.; Chung, Y.H.; Lee, Y.S.; et al. Reappraisal of repeated transarterial chemoembolization in the treatment of hepatocellular carcinoma with portal vein invasion. J. Gastroenterol. Hepatol. 2009, 24, 806–814. [Google Scholar] [CrossRef]
- Kim, J.H.; Shim, J.H.; Yoon, H.K.; Ko, H.K.; Kim, J.W.; Gwon, D.I. Chemoembolization related to good survival for selected patients with hepatocellular carcinoma invading segmental portal vein. Liver Int. 2018, 38, 1646–1654. [Google Scholar] [CrossRef]
- Kim, G.A.; Shim, J.H.; Yoon, S.M.; Jung, J.; Kim, J.H.; Ryu, M.H.; Ryoo, B.Y.; Kang, Y.K.; Lee, D.; Kim, K.M.; et al. Comparison of chemoembolization with and without radiation therapy and sorafenib for advanced hepatocellular carcinoma with portal vein tumor thrombosis: A propensity score analysis. J. Vasc. Interv. Radiol. 2015, 26, 320–329. [Google Scholar] [CrossRef]
- Park, J.W.; Kim, Y.J.; Kim, D.Y.; Bae, S.H.; Paik, S.W.; Lee, Y.J.; Kim, H.Y.; Lee, H.C.; Han, S.Y.; Cheong, J.Y.; et al. Sorafenib with or without concurrent transarterial chemoembolization in patients with advanced hepatocellular carcinoma: The phase III STAH trial. J. Hepatol. 2019, 70, 684–691. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Ueshima, K.; Ikeda, M.; Torimura, T.; Tanabe, N.; Aikata, H.; Izumi, N.; Yamasaki, T.; Nojiri, S.; Hino, K.; et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut 2019. [Google Scholar] [CrossRef]
- Yoon, S.M.; Lim, Y.S.; Won, H.J.; Kim, J.H.; Kim, K.M.; Lee, H.C.; Chung, Y.H.; Lee, Y.S.; Lee, S.G.; Park, J.H.; et al. Radiotherapy plus transarterial chemoembolization for hepatocellular carcinoma invading the portal vein: Long-term patient outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Koo, J.E.; Kim, J.H.; Lim, Y.S.; Park, S.J.; Won, H.J.; Sung, K.B.; Suh, D.J. Combination of transarterial chemoembolization and three-dimensional conformal radiotherapy for hepatocellular carcinoma with inferior vena cava tumor thrombus. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.M.; Ryoo, B.Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.S. Efficacy and safety of transarterial chemoembolization plus external beam radiotherapy vs sorafenib in hepatocellular carcinoma with macroscopic vascular invasion: A randomized clinical trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef] [PubMed]
- European Association For The Study Of The Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Jung, J.; Joo, J.H.; Kim, S.Y.; Kim, J.H.; Lim, Y.S.; Lee, H.C.; Kim, J.H.; Yoon, S.M. Combined transarterial chemoembolization and radiotherapy as a first-line treatment for hepatocellular carcinoma with macroscopic vascular invasion: Necessity to subclassify Barcelona Clinic Liver Cancer stage C. Radiother. Oncol. 2019, 141, 95–100. [Google Scholar] [CrossRef]
- Choi, G.H.; Shim, J.H.; Kim, M.J.; Ryu, M.H.; Ryoo, B.Y.; Kang, Y.K.; Shin, Y.M.; Kim, K.M.; Lim, Y.S.; Lee, H.C. Sorafenib alone versus sorafenib combined with transarterial chemoembolization for advanced-stage hepatocellular carcinoma: Results of propensity score analyses. Radiology 2013, 269, 603–611. [Google Scholar] [CrossRef]
- Zhu, K.; Chen, J.; Lai, L.; Meng, X.; Zhou, B.; Huang, W.; Cai, M.; Shan, H. Hepatocellular carcinoma with portal vein tumor thrombus: Treatment with transarterial chemoembolization combined with sorafenib—A retrospective controlled study. Radiology 2014, 272, 284–293. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lencioni, R.; Montal, R.; Torres, F.; Park, J.W.; Decaens, T.; Raoul, J.L.; Kudo, M.; Chang, C.; Rios, J.; Boige, V.; et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J. Hepatol. 2017, 66, 1166–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saad, E.D.; Katz, A. Progression-free survival and time to progression as primary end points in advanced breast cancer: Often used, sometimes loosely defined. Ann. Oncol. 2009, 20, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Ju, M.J.; Tu, G.W.; Han, Y.; He, H.Y.; He, Y.Z.; Mao, H.L.; Wu, Z.G.; Yin, Y.Q.; Luo, J.F.; Zhu, D.M.; et al. Effect of admission time on mortality in an intensive care unit in Mainland China: A propensity score matching analysis. Crit. Care 2013, 17, R230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNamara, M.G.; Slagter, A.E.; Nuttall, C.; Frizziero, M.; Pihlak, R.; Lamarca, A.; Tariq, N.; Valle, J.W.; Hubner, R.A.; Knox, J.J.; et al. Sorafenib as first-line therapy in patients with advanced Child-Pugh B hepatocellular carcinoma—A meta-analysis. Eur. J. Cancer 2018, 15, 1–9. [Google Scholar] [CrossRef]
- Bettinger, D.; Spode, R.; Glaser, N.; Buettner, N.; Boettler, T.; Neumann-Haefelin, C.; Brunner, T.B.; Gkika, E.; Maruschke, L.; Thimme, R.; et al. Survival benefit of transarterial chemoembolization in patients with metastatic hepatocellular carcinoma: A single center experience. BMC Gastroenterol. 2017, 17, 98. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Sinn, D.H.; Choi, M.S.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Lee, J.H.; Koh, K.C.; Paik, S.W. Hepatocellular carcinoma with extrahepatic metastasis: Are there still candidates for transarterial chemoembolization as an initial treatment? PLoS ONE 2019, 14, e0213547. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.; Ducreux, M.; Zhu, A.; Kim, T.Y.; Kudo, M.; Breder, V.; Merie, P.; et al. IMbrave 150: Efficacy and safety results from a ph III study evaluating atezolizumab (atezo) + bevacizumab (bev) vs sorafenib (Sor) as first treatment (tx) for patients (pts) with unresectable hepatocellular carcinoma (HCC). Ann. Oncol. 2019, 30 (Suppl. 9), ix186–ix187. [Google Scholar] [CrossRef]
- Stein, S.; Pishvaian, M.J.; Lee, M.S.; Lee, K.H.; Hernandez, S.; Kwan, A.; Liu, B.; Grossman, W.; Iizuka, K.; Ryoo, B.Y. Safety and clinical activity of 1L atezolizumab + bevacizumab in a phase Ib study in hepatocellular carcinoma (HCC). J. Clin. Oncol. 2018, 36 Suppl. 15, 4074. [Google Scholar] [CrossRef]
- Ikeda, M.; Sung, M.W.; Kudo, M.; Kobayashi, M.; Baron, A.D.; Finn, R.S.; Kaneko, S.; Zhu, A.X.; Kubota, T.; Kraljevic, S.; et al. A Phase 1B trial of lenvatinib (LEN) plus pembrolizumab (PEM) in patients (PTS) with unresectable hepatocellular carcinoma (uHCC). J. Clin. Oncol. 2018, 36 (Suppl. 15), 4076. [Google Scholar] [CrossRef]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M.; et al. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. J. Hepatol. 2017, 66, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, C.; Ruohoniemi, D.; Shanbhogue, K.P.; Wei, J.; Welling, T.H.; Gu, P.; Park, J.S.; Dagher, N.N.; Taslakian, B.; Hickey, R.M. Safety of combined yttrium-90 radioembolization and immune checkpoint inhibitor immunotherapy for hepatocellular carcinoma. J. Vasc. Interv. Radiol. 2020, 31, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.H.; Kim, J.H.; Kim, P.N.; Kim, S.Y.; Lim, Y.S.; Park, S.H.; Ko, H.K.; Lee, S.G. Surgical resection versus radiofrequency ablation very early-stage HCC (</=2 cm Single HCC): A propensity score analysis. Liver Int. 2019, 39, 2397–2407. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population before PSM | Study Population after PSM | |||||
|---|---|---|---|---|---|---|
| Variable | TACE + Sorafenib | TACE + RT | p Value | TACE + Sorafenib | TACE + RT | p Value |
| Patients | 104 | 203 | 87 | 87 | ||
| Age (years old, mean ± SD) | 56.4 ± 10.8 | 55.6 ± 9.3 | 0.485 | 56.1 ± 10.6 | 55.8 ± 9.9 | 0.883 |
| Male sex, n (%) | 91 (87.5) | 175 (86.2) | 0.753 | 75 (86.2) | 76 (87.4) | 0.823 |
| Etiology, n (%) | 0.002 | 0.889 | ||||
| HBV | 82 (78.8) | 188 (92.6) | 75 (86.2) | 7 (88.5) | ||
| HCV | 9 (8.7) | 6 (3) | 4 (4.6) | 3 (3.4) | ||
| Others | 13 (12.5) | 9 (4.4) | 8 (9.2) | 7 (8) | ||
| ECOG PS | 0.747 | 0.564 | ||||
| 0 | 63 (59.6) | 112 (55.2) | 52 (59.8) | 55 (63.2) | ||
| 1 | 41 (38.5) | 86 (42.4) | 34 (39.1) | 32 (36.8) | ||
| 2 | 2 (1.9) | 5 (2.5) | 1 (1.1) | 0 (0) | ||
| Child–Pugh score, n (%) | 0.569 | 0.635 | ||||
| A | 91 (87.5) | 182 (89.7) | 76 (87.4) | 78 (89.7) | ||
| B | 13 (12.5) | 21 (10.3) | 11 (12.6) | 9 (10.3) | ||
| Presence of extrahepatic metastasis | 39 (37.5) | 37 (18.2) | < 0.001 | 29 (33.3) | 25 (28.7) | 0.512 |
| Maximal tumor size (cm, mean ± SD) | 10.6 ± 4.2 | 9.2 ± 4.0 | 0.003 | 10.2 ± 4.1 | 10.1 ± 4.0 | 0.762 |
| Tumor number ≥ 4 | 31 (29.8) | 42 (20.7) | 0.076 | 21 (24.1) | 20 (23) | 0.858 |
| Bilirubin (mg/dL, mean ± SD) | 0.91 ± 0.49 | 0.90 ± 0.50 | 0.843 | 0.90 ± 0.50 | 0.88 ± 0.58 | 0.846 |
| Albumin (≤ 3.5 mg/dL), n (%) | 52 (50) | 76 (37.4) | 0.038 | 38 (43.7) | 40 (46) | 0.76 |
| AFP ≥400 ng/mL, n (%) | 60 (57.7) | 113 (55.7) | 0.735 | 49 (56.3) | 49 (56.3) | > 0.999 |
| Tumor type, n (%) | 0.678 | 0.436 | ||||
| Nodular | 42 (40.4) | 87 (42.9) | 36 (41.4) | 31 (35.6) | ||
| Infiltrative | 62 (59.6) | 116 (57.1) | 51 (58.6) | 56 (64.4) | ||
| Tumor involvement, n (%) | 0.629 | 0.609 | ||||
| Unilobar | 71 (68.3) | 133 (65.5) | 62 (71.3) | 65 (74.7) | ||
| Bilobar | 33 (31.7) | 70 (34.5) | 25 (28.7) | 22 (25.3) | ||
| Extent of PVTT | 0.102 | 0.803 | ||||
| Main portal vein | 12 (11.6) | 20 (9.9) | 9 (10.4) | 9 (10.4) | ||
| First-order portal vein branch | 59 (56.7) | 93 (45.8) | 47 (54) | 51 (58.6) | ||
| Second- or lower-order portal vein branches | 33 (31.7) | 90 (44.3) | 31 (35.6) | 27 (31) | ||
| Combined hepatic vein invasion | 19 (18.3) | 24 (11.8) | 0.123 | 14 (16.1) | 16 (18.4) | 0.688 |
| Analysis | Hazard Ratio | 95% Confidence Interval | p Value | ||
|---|---|---|---|---|---|
| PFS | |||||
| Unadjusted | TACE plus sorafenib | 1.354 | 1.048–1.751 | 0.021 | |
| TACE plus RT | 1 | ||||
| Adjusted † | TACE plus sorafenib | 1.015 | 0.766–1.245 | 0.917 | |
| TACE plus RT | 1 | ||||
| Propensity matched * | TACE plus sorafenib | 1.2 | 0.88–1.635 | 0.248 | |
| TACE plus RT | 1 | ||||
| OS | |||||
| Unadjusted | TACE plus sorafenib | 1.451 | 1.102–1.909 | 0.008 | |
| TACE plus RT | 1 | ||||
| Adjusted ‡ | TACE plus sorafenib | 1.164 | 0.874–1.551 | 0.299 | |
| TACE plus RT | 1 | ||||
| Propensity matched * | TACE plus sorafenib | 1.199 | 0.865–1.661 | 0.276 | |
| TACE plus RT | 1 | ||||
| Analysis | Hazard Ratio | 95% Confidence Interval | p Value | ||
|---|---|---|---|---|---|
| PFS | |||||
| Unadjusted | TACE plus sorafenib | 1.271 | 0.925–1.747 | 0.139 | |
| TACE plus RT | 1 | ||||
| Adjusted † | TACE plus sorafenib | 1.345 | 0.975–1.856 | 0.071 | |
| TACE plus RT | 1 | ||||
| OS | |||||
| Unadjusted | TACE plus sorafenib | 1.285 | 0.909–1.815 | 0.155 | |
| TACE plus RT | 1 | ||||
| Adjusted ‡ | TACE plus sorafenib | 1.424 | 1.001–2.026 | 0.05 | |
| TACE plus RT | 1 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, H.H.; Kim, J.H.; Shim, J.H.; Yoon, S.M.; Kim, P.H.; Alrashidi, I. Chemoembolization Plus Radiotherapy versus Chemoembolization Plus Sorafenib for the Treatment of Hepatocellular Carcinoma Invading the Portal Vein: A Propensity Score Matching Analysis. Cancers 2020, 12, 1116. https://doi.org/10.3390/cancers12051116
Chu HH, Kim JH, Shim JH, Yoon SM, Kim PH, Alrashidi I. Chemoembolization Plus Radiotherapy versus Chemoembolization Plus Sorafenib for the Treatment of Hepatocellular Carcinoma Invading the Portal Vein: A Propensity Score Matching Analysis. Cancers. 2020; 12(5):1116. https://doi.org/10.3390/cancers12051116
Chicago/Turabian StyleChu, Hee Ho, Jin Hyoung Kim, Ju Hyun Shim, Sang Min Yoon, Pyeong Hwa Kim, and Ibrahim Alrashidi. 2020. "Chemoembolization Plus Radiotherapy versus Chemoembolization Plus Sorafenib for the Treatment of Hepatocellular Carcinoma Invading the Portal Vein: A Propensity Score Matching Analysis" Cancers 12, no. 5: 1116. https://doi.org/10.3390/cancers12051116