Validation of an Automated Quantitative Digital Pathology Approach for Scoring TMEM: A Prognostic Biomarker for Metastasis

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Algorithm Development
- 1.
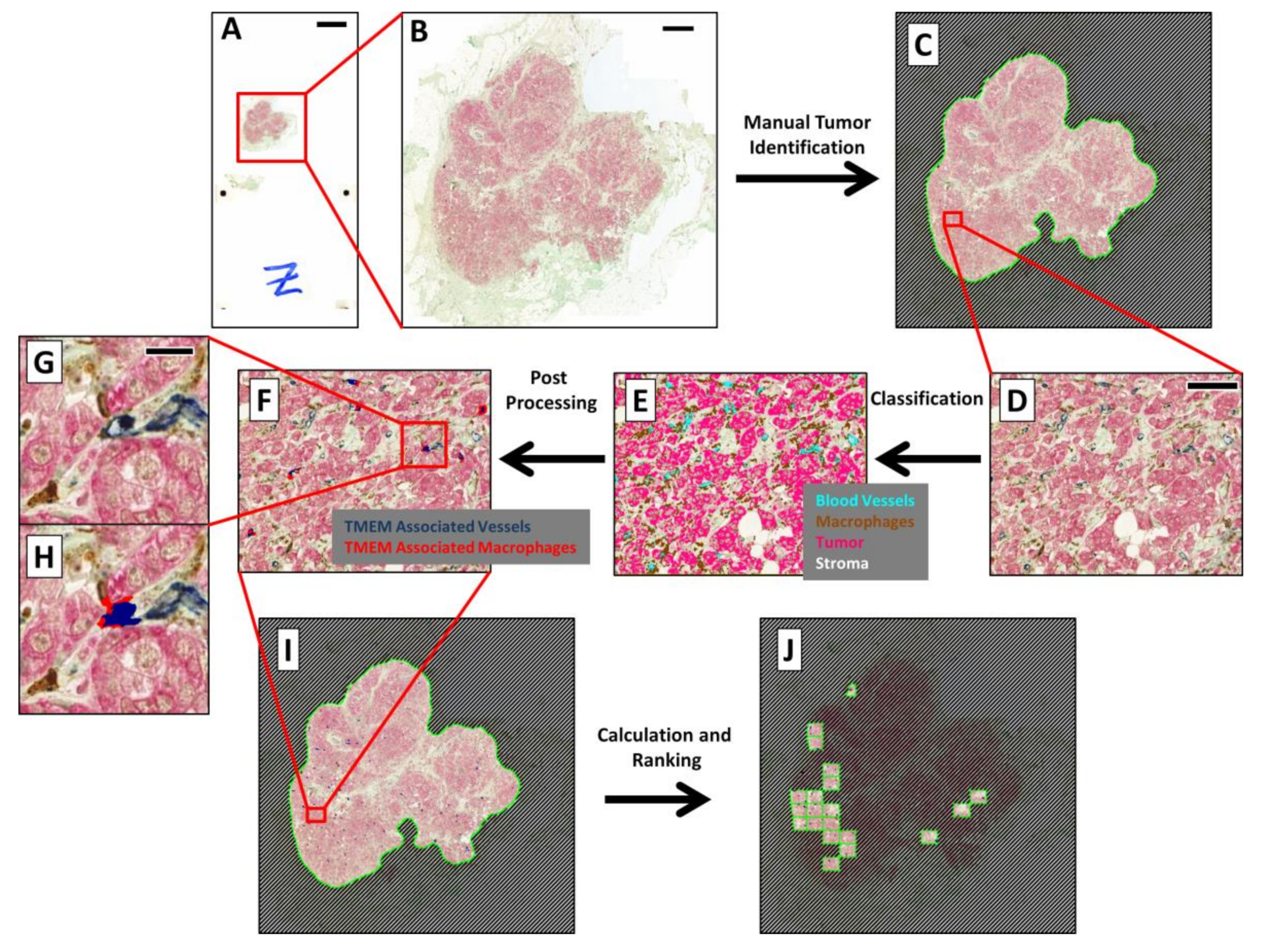
- Preprocessing—RGB images, captured with the slide scanner’s color camera, were split into “Feature Channels”, which optimized the signal contrast for each of the three TMEM stains utilized. A median filter was applied at this stage to aid in the signal separation.
- 2.
- Classification—A linear Bayesian classifier algorithm [23] was trained to identify and classify each pixel into one of five categories (macrophages, darkly stained tumor cells, lightly stained tumor cells, blood vessels, and stroma) by pathologist-guided identification of each of the stains within fields of view extracted from 6 different slides. Two categories were utilized for the tumor cells to accommodate variations in staining. Training was performed during the development of the algorithm and remained unchanged thereafter. The classifier algorithm was then applied to the slide one high-power field at a time. This is demonstrated in Figure 1D, which shows the IHC staining in a single high-power field of view, and in Figure 1E, which shows the same field with each pixel pseudo-colored by its classification.
- 3.
- Postprocessing—Contiguous groupings of pixels in each classification were treated as separate objects, and image analysis steps were next applied to manipulate and redefine these classified objects based upon size, morphometry, and spatial relations to other objects, ultimately resulting in the identification of TMEM objects (Figure 1H and Figure 2). After identification of TMEM objects, the entire digital slide was globally scored (Figure 1I) and ranked (Figure 1J) as described below.
- 4.
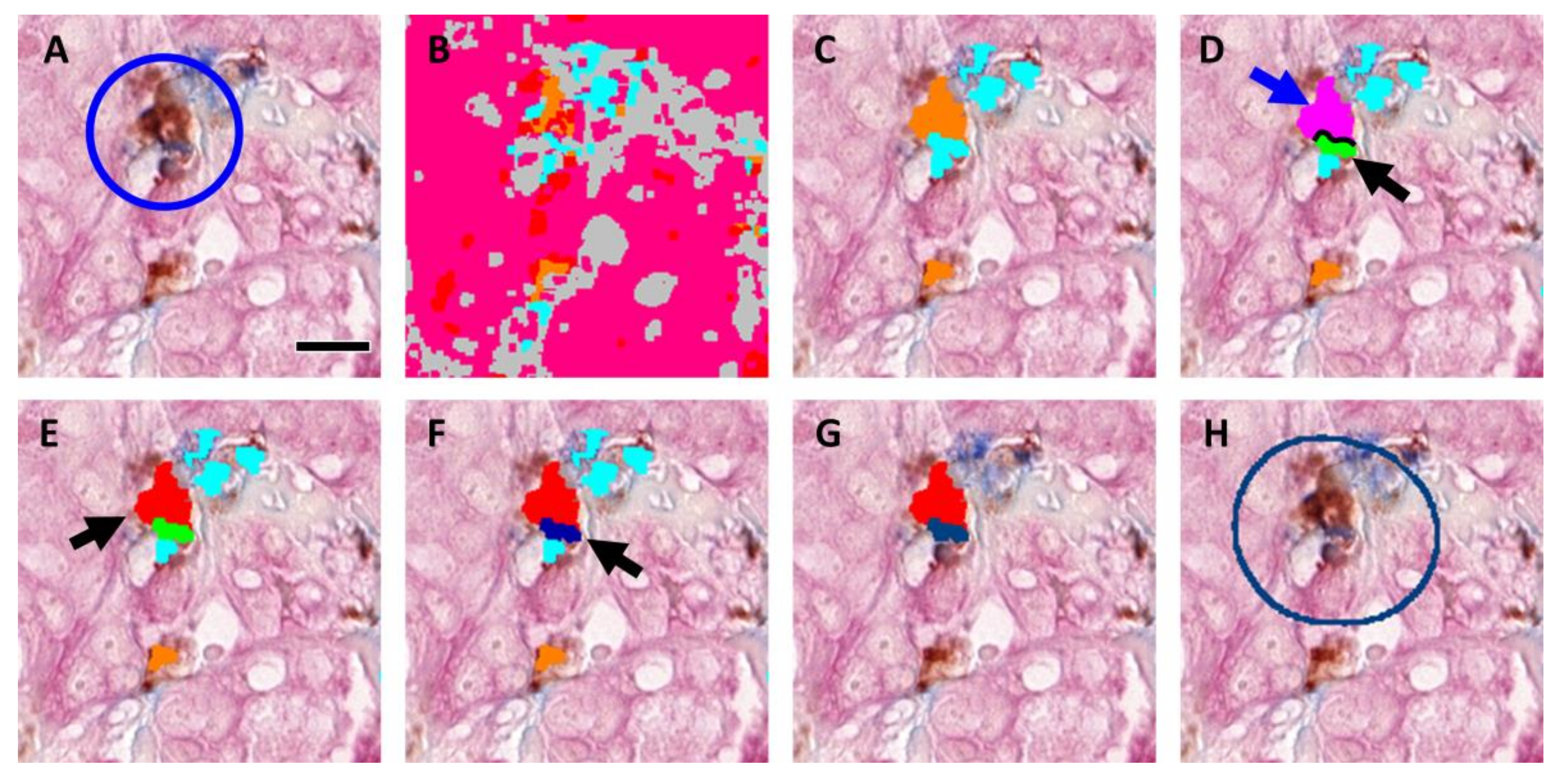
- The steps for identification of TMEM objects are demonstrated in Figure 2 using a field of view containing a single TMEM doorway (Figure 2A) (manually identified and marked by a circle). Figure 2B shows the same field of view after pixel classification by the trained algorithm. Next, the two classifications of tumor (pink and red) were merged and the boundaries of all objects (tumor, stroma (gray), vessels (cyan), and macrophages (orange)) were smoothed by enlarging (dilating) and subsequently shrinking (eroding) each object. In addition, large vessels and macrophage aggregates (>800 µm2) were also removed along with small fragments of tumor tissue (<10 µm2), stroma (<400 µm2), particles resembling macrophages (<5 µm2), and particles resembling vessels (<5 µm2). Figure 2C shows the macrophages (orange) and vessels (cyan) that were identified using this procedure. Objects were redefined based on cell–cell contacts as follows:
- a.
- b.
- Macrophages that are in contact with vessels that have been identified as vessel–macrophage complexes were labeled as separate objects called “macrophage–vessel complexes” (Figure 2D, magenta object, blue arrow).
- c.
- Macrophages that have been identified as macrophage–vessel complexes were evaluated for their amount of contact with Mena+ tumor cells and vessels depending upon their size. These contacts were defined as follows:
- Large macrophage–vessel complexes (≥40 µm2) that have at least 8% of their perimeter in contact with tumor cells and at least 20% of their perimeter in contact with vessels were labeled as “large TMEM-associated macrophages” (Figure 2E, red object, black arrow),
- Small macrophage–vessel complexes (<40 µm2) that have at least 10% of their perimeter in contact with tumor tissue and at least 10% of their perimeter in contact with vessels were labeled as “small TMEM-associated macrophages” (label not shown in figure),
- d.
- Vessels that have at least 20% of their perimeter in contact with tumor cells and at least 20% of their perimeter in contact with small and large TMEM-associated macrophages were labeled as “TMEM-associated vessels” (Figure 2F, dark blue object, black arrow),
- e.
- All objects other than small and large TMEM-associated macrophages and TMEM-associated vessels were removed (Figure 2G).
- 5.
- Calculation—Metrics were applied to the final classified pixel clusters to quantify the objects (e.g., object counts, object areas, and interface lengths).
- 6.
- Ranking—The entire tissue within pathologist’s defined region of interest (ROI) was divided into areas equivalent to a pathologist’s microscope high-power field (~300 × 400 µm, Figure 1I), and each area was individually analyzed. The TMEM doorway count for each area was calculated by summing the number of identified TMEM objects within the area. The counts for all of the areas were then compared and ranked, and the highest scoring areas were finally presented to the pathologist for review (Figure 1J). The final TMEM doorway score for the entire patient sample was determined as the sum of the counts of the TMEM objects within the top 10 ranked fields of view.
2.2. Determination of Appropriate Metric for Automated Algorithm
2.3. Evaluation of Algorithm Performance
Pathologist Inter- and Intra-Observer Validation
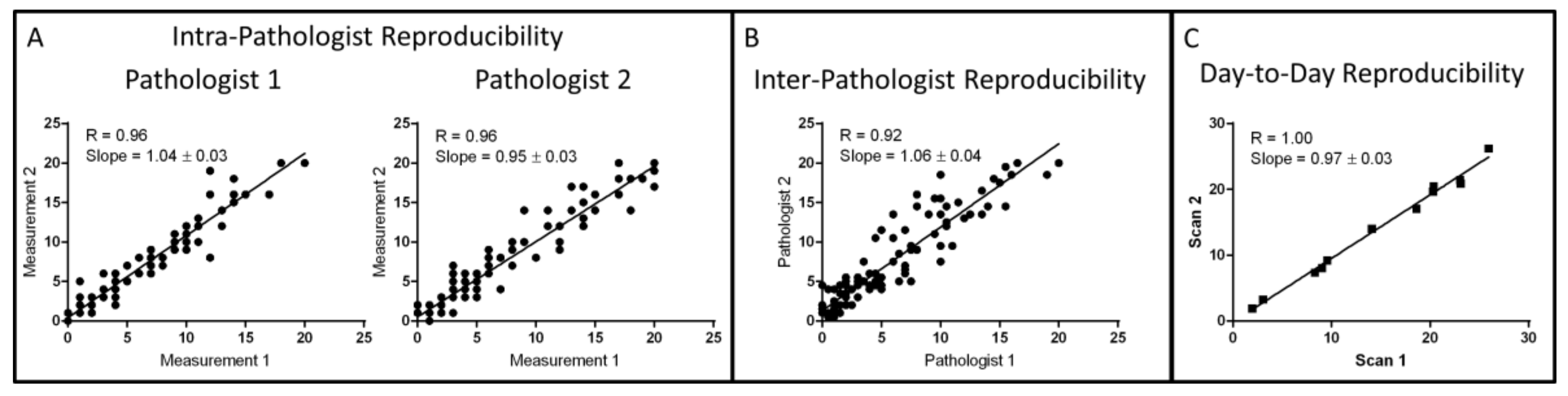
2.4. Algorithm Reproducibility
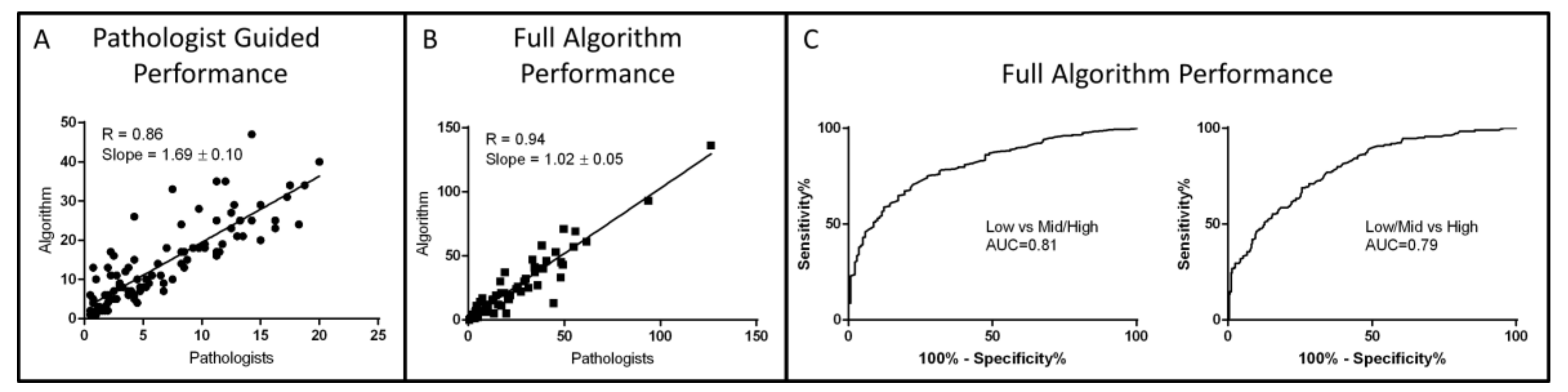
2.5. Algorithm Performance
3. Discussion
4. Materials and Methods
4.1. Cohort
4.2. IHC Triple Staining
- Endothelial cells—CD-31 (clone JC70A; 1:800 dilution; DAKO, Santa Clara, CA, USA) with Bond Epitope Retrieval Solution 2 and Vector Blue chromogen,
- Macrophages—CD-68 (clone PG-M1; 1:300 dilution; DAKO) with antigen retrieval using Bond Epitope Retrieval Solution 1 and 3,3’-Diaminobenzidine (DAB) chromogen,
- Tumor cells—anti-pan-Mena antibody (P/N: 610692, BD Biosciences, San Jose, CA, USA) that stain all isoforms of Mena, macrophages with Fast Red chromogen (Bond Polymer Refine Red Detection, Leica Biosystems, Buffalo Grove, IL, USA).
4.3. Manual TMEM Quantification
4.4. Digital Whole Slide Imaging
4.5. Statistical Analysis
5. Conclusions
6. Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Vijver, M.J.; He, Y.D.; van’t Veer, L.J.; Dai, H.; Hart, A.A.; Voskuil, D.W.; Schreiber, G.J.; Peterse, J.L.; Roberts, C.; Marton, M.J.; et al. A gene-expression signature as a predictor of survival in breast cancer. N Engl J. Med. 2002, 347, 1999–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, B.D.; Sica, G.L.; Liu, Y.F.; Rohan, T.E.; Gertler, F.B.; Condeelis, J.S.; Jones, J.G. Tumor microenvironment of metastasis in human breast carcinoma: A potential prognostic marker linked to hematogenous dissemination. Clin. Cancer Res. 2009, 15, 2433–2441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparano, J.A.; Gray, R.; Oktay, M.H.; Entenberg, D.; Rohan, T.; Xue, X.; Donovan, M.; Peterson, M.; Shuber, A.; Hamilton, D.A.; et al. A metastasis biomarker (MetaSite Breast Score) is associated with distant recurrence in hormone receptor-positive, HER2-negative early-stage breast cancer. Nature PJ Breast Cancer 2017, 3, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuzick, J.; Dowsett, M.; Pineda, S.; Wale, C.; Salter, J.; Quinn, E.; Zabaglo, L.; Mallon, E.; Green, A.R.; Ellis, I.O.; et al. Prognostic value of a combined estrogen receptor, progesterone receptor, Ki-67, and human epidermal growth factor receptor 2 immunohistochemical score and comparison with the Genomic Health recurrence score in early breast cancer. J. Clin. Oncol 2011, 29, 4273–4278. [Google Scholar] [CrossRef] [Green Version]
- Rohan, T.E.; Xue, X.; Lin, H.M.; D’Alfonso, T.M.; Ginter, P.S.; Oktay, M.H.; Robinson, B.D.; Ginsberg, M.; Gertler, F.B.; Glass, A.G.; et al. Tumor microenvironment of metastasis and risk of distant metastasis of breast cancer. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [Green Version]
- Wyckoff, J.; Wang, W.; Lin, E.Y.; Wang, Y.; Pixley, F.; Stanley, E.R.; Graf, T.; Pollard, J.W.; Segall, J.; Condeelis, J. A paracrine loop between tumor cells and macrophages is required for tumor cell migration in mammary tumors. Cancer Res. 2004, 64, 7022–7029. [Google Scholar] [CrossRef] [Green Version]
- Wyckoff, J.B.; Wang, Y.; Lin, E.Y.; Li, J.F.; Goswami, S.; Stanley, E.R.; Segall, J.E.; Pollard, J.W.; Condeelis, J. Direct visualization of macrophage-assisted tumor cell intravasation in mammary tumors. Cancer Res. 2007, 67, 2649–2656. [Google Scholar] [CrossRef] [Green Version]
- Patsialou, A.; Bravo-Cordero, J.J.; Wang, Y.; Entenberg, D.; Liu, H.; Clarke, M.; Condeelis, J.S. Intravital multiphoton imaging reveals multicellular streaming as a crucial component of in vivo cell migration in human breast tumors. Intravital 2013, 2, e25294. [Google Scholar] [CrossRef] [Green Version]
- Harney, A.S.; Arwert, E.N.; Entenberg, D.; Wang, Y.; Guo, P.; Qian, B.Z.; Oktay, M.H.; Pollard, J.W.; Jones, J.G.; Condeelis, J.S. Real-Time Imaging Reveals Local, Transient Vascular Permeability, and Tumor Cell Intravasation Stimulated by TIE2hi Macrophage-Derived VEGFA. Cancer Discov. 2015, 5, 932–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karagiannis, G.S.; Goswami, S.; Jones, J.G.; Oktay, M.H.; Condeelis, J.S. Signatures of breast cancer metastasis at a glance. J. Cell Sci. 2016, 129, 1751–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roh-Johnson, M.; Bravo-Cordero, J.J.; Patsialou, A.; Sharma, V.P.; Guo, P.; Liu, H.; Hodgson, L.; Condeelis, J. Macrophage contact induces RhoA GTPase signaling to trigger tumor cell intravasation. Oncogene 2014, 33, 4203–4212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harney, A.S.; Karagiannis, G.S.; Pignatelli, J.; Smith, B.D.; Kadioglu, E.; Wise, S.C.; Hood, M.M.; Kaufman, M.D.; Leary, C.B.; Lu, W.P.; et al. The Selective Tie2 Inhibitor Rebastinib Blocks Recruitment and Function of Tie2(Hi) Macrophages in Breast Cancer and Pancreatic Neuroendocrine Tumors. Mol. Cancer Ther. 2017, 16, 2486–2501. [Google Scholar] [CrossRef] [Green Version]
- Gilbertson, J.R.; Ho, J.; Anthony, L.; Jukic, D.M.; Yagi, Y.; Parwani, A.V. Primary histologic diagnosis using automated whole slide imaging: A validation study. BMC Clin. Pathol 2006, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Braun, M.W.; Kearns, K.D. Improved learning efficiency and increased student collaboration through use of virtual microscopy in the teaching of human pathology. Anat. Sci. Educ. 2008, 1, 240–246. [Google Scholar] [CrossRef]
- McShane, L.M.; Aamodt, R.; Cordon-Cardo, C.; Cote, R.; Faraggi, D.; Fradet, Y.; Grossman, H.B.; Peng, A.; Taube, S.E.; Waldman, F.M. Reproducibility of p53 immunohistochemistry in bladder tumors. National Cancer Institute, Bladder Tumor Marker Network. Clin. Cancer Res. 2000, 6, 1854–1864. [Google Scholar]
- Rhodes, A.; Jasani, B.; Balaton, A.J.; Barnes, D.M.; Anderson, E.; Bobrow, L.G.; Miller, K.D. Study of interlaboratory reliability and reproducibility of estrogen and progesterone receptor assays in Europe. Documentation of poor reliability and identification of insufficient microwave antigen retrieval time as a major contributory element of unreliable assays. Am. J. Clin. Pathol. 2001, 115, 44–58. [Google Scholar] [CrossRef] [Green Version]
- Gancberg, D.; Jarvinen, T.; di Leo, A.; Rouas, G.; Cardoso, F.; Paesmans, M.; Verhest, A.; Piccart, M.J.; Isola, J.; Larsimont, D. Evaluation of HER-2/NEU protein expression in breast cancer by immunohistochemistry: An interlaboratory study assessing the reproducibility of HER-2/NEU testing. Breast Cancer Res. Treat. 2002, 74, 113–120. [Google Scholar] [CrossRef]
- Al-Janabi, S.; Huisman, A.; Vink, A.; Leguit, R.J.; Offerhaus, G.J.; Ten Kate, F.J.; van Dijk, M.R.; van Diest, P.J. Whole slide images for primary diagnostics in dermatopathology: A feasibility study. J. Clin. Pathol 2012, 65, 152–158. [Google Scholar] [CrossRef]
- Nielsen, P.S.; Lindebjerg, J.; Rasmussen, J.; Starklint, H.; Waldstrom, M.; Nielsen, B. Virtual microscopy: An evaluation of its validity and diagnostic performance in routine histologic diagnosis of skin tumors. Human Pathol. 2010, 41, 1770–1776. [Google Scholar] [CrossRef]
- Al Habeeb, A.; Evans, A.; Ghazarian, D. Virtual microscopy using whole-slide imaging as an enabler for teledermatopathology: A paired consultant validation study. J. Pathol. Inform. 2012, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Izenman, A.J. Linear discriminant analysis. In Modern Multivariate Statistical Techniques; Springer: New York, NY, USA, 2013; pp. 237–280. [Google Scholar]
- Katz, S.J.; Morrow, M. Addressing overtreatment in breast cancer: The doctors’ dilemma. Cancer 2013, 119, 3584–3588. [Google Scholar] [CrossRef] [PubMed]
- Entenberg, D.; Kedrin, D.; Wyckoff, J.; Sahai, E.; Condeelis, J.; Segall, J.E. Imaging tumor cell movement in vivo. Curr. Protoc. Cell Biol. 2013. Chapter 19:Unit19.7. [Google Scholar] [CrossRef] [PubMed]
- Harney, A.S.; Wang, Y.; Condeelis, J.S.; Entenberg, D. Extended Time-lapse Intravital Imaging of Real-time Multicellular Dynamics in the Tumor Microenvironment. J. Vis. Exp. JoVE 2016, e54042. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, G.S.; Pastoriza, J.M.; Wang, Y.; Harney, A.S.; Entenberg, D.; Pignatelli, J.; Sharma, V.P.; Xue, E.A.; Cheng, E.; D’Alfonso, T.M.; et al. Neoadjuvant chemotherapy induces breast cancer metastasis through a TMEM-mediated mechanism. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgibbons, P.L.; Bradley, L.A.; Fatheree, L.A.; Alsabeh, R.; Fulton, R.S.; Goldsmith, J.D.; Haas, T.S.; Karabakhtsian, R.G.; Loykasek, P.A.; Marolt, M.J. Principles of analytic validation of immunohistochemical assays: Guideline from the College of American Pathologists Pathology and Laboratory Quality Center. Arch. Pathol. Lab. Med. 2014, 138, 1432–1443. [Google Scholar] [CrossRef] [Green Version]
- Linde, N.; Casanova-Acebes, M.; Sosa, M.S.; Mortha, A.; Rahman, A.; Farias, E.; Harper, K.; Tardio, E.; Reyes Torres, I.; Jones, J.; et al. Macrophages orchestrate breast cancer early dissemination and metastasis. Nat. Commun 2018, 9, 21. [Google Scholar] [CrossRef]
- Entenberg, D.; Voiculescu, S.; Guo, P.; Borriello, L.; Wang, Y.; Karagiannis, G.S.; Jones, J.; Baccay, F.; Oktay, M.; Condeelis, J. A permanent window for the murine lung enables high-resolution imaging of cancer metastasis. Nat. Methods 2018, 15, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Ginter, P.S.; Karagiannis, G.S.; Entenberg, D.; Lin, Y.; Condeelis, J.; Jones, J.G.; Oktay, M.H. Tumor Microenvironment of Metastasis (TMEM) Doorways Are Restricted to the Blood Vessel Endothelium in Both Primary Breast Cancers and Their Lymph Node Metastases. Cancers 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.; Gertler, F.B.; Balsamo, M.; Condeelis, J.S.; Camp, R.L.; Xue, X.; Lin, J.; Rohan, T.E.; Rimm, D.L. Quantitative assessment of invasive mena isoforms (Menacalc) as an independent prognostic marker in breast cancer. Breast Cancer Res.: BCR 2012, 14, R124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forse, C.L.; Agarwal, S.; Pinnaduwage, D.; Gertler, F.; Condeelis, J.S.; Lin, J.; Xue, X.; Johung, K.; Mulligan, A.M.; Rohan, T.E.; et al. Menacalc, a quantitative method of metastasis assessment, as a prognostic marker for axillary node-negative breast cancer. BMC Cancer 2015, 15, 483. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method of TMEM Quantification | Sum of TMEM-Associated Vessels | Sum of TMEM-Associated Macrophages | Total Interface Length between TMEM-Associated Vessels and TMEM-Associated Macrophages |
|---|---|---|---|
| Sum of TMEM-Associated Vessels | 1.00 | 0.98 p < 0.0001 | 0.96 p < 0.0001 |
| Sum of TMEM-Associated Macrophages | 0.98 p < 0.0001 | 1.00 | 0.97 p < 0.0001 |
| Total Interface Length between TMEM-Associated Vessels and TMEM-Associated Macrophages | 0.96 p < 0.0001 | 0.97 p < 0.0001 | 1.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Entenberg, D.; Oktay, M.H.; D’Alfonso, T.; Ginter, P.S.; Robinson, B.D.; Xue, X.; Rohan, T.E.; Sparano, J.A.; Jones, J.G.; Condeelis, J.S. Validation of an Automated Quantitative Digital Pathology Approach for Scoring TMEM: A Prognostic Biomarker for Metastasis. Cancers 2020, 12, 846. https://doi.org/10.3390/cancers12040846
Entenberg D, Oktay MH, D’Alfonso T, Ginter PS, Robinson BD, Xue X, Rohan TE, Sparano JA, Jones JG, Condeelis JS. Validation of an Automated Quantitative Digital Pathology Approach for Scoring TMEM: A Prognostic Biomarker for Metastasis. Cancers. 2020; 12(4):846. https://doi.org/10.3390/cancers12040846
Chicago/Turabian StyleEntenberg, David, Maja H. Oktay, Timothy D’Alfonso, Paula S. Ginter, Brian D. Robinson, Xiaonan Xue, Thomas E. Rohan, Joseph A. Sparano, Joan G. Jones, and John S. Condeelis. 2020. "Validation of an Automated Quantitative Digital Pathology Approach for Scoring TMEM: A Prognostic Biomarker for Metastasis" Cancers 12, no. 4: 846. https://doi.org/10.3390/cancers12040846