Management Recommendations for Merkel Cell Carcinoma—A Danish Perspective

Abstract
:1. Introduction
2. Diagnosis
2.1. Clinical Features
2.2. Pathology
3. Work-Up & Staging
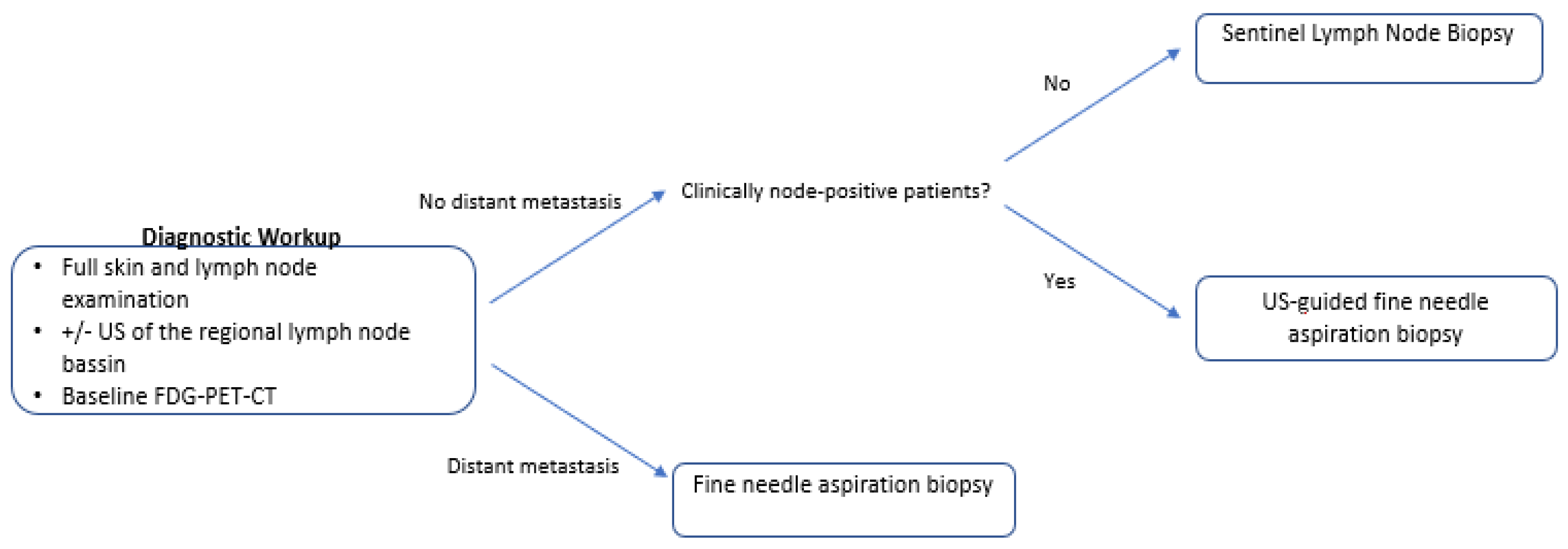
3.1. Work-Up
3.2. Staging
4. Treatment
5. Management of the Primary Tumor
5.1. Surgery
5.2. Adjuvant Radiotherapy
5.3. Definitive Radiotherapy—Nonresectable Disease
6. Management of the Regional Lymph Nodes
6.1. Lymph Node Dissection and Locoregional Radiotherapy
6.2. Definitive Radiotherapy – Nonresectable Disease
6.3. Other Treatment Regimens
7. Management of Distant Metastatic Disease
7.1. Immune Checkpoint Inhibitors
7.2. Avelumab (PD-L1 Antibody)
7.3. Pembrolizumab (PD-1 Antibody)
7.4. Other Immune Checkpoint Inhibitors
7.5. Chemotherapy
8. Follow-Up
9. Registration
10. Methods
11. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Feng, H.; Shuda, M.; Chang, Y.; Moore, P.S. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008, 319, 1096–1100. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, H.L.; Russell, J.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbe, C.; Linette, G.P.; Milella, M.; et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: A multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1374–1385. [Google Scholar] [CrossRef] [Green Version]
- Lyhne, D.; Lock-Andersen, J.; Dahlstrom, K.; Drzewiecki, K.T.; Balslev, E.; Muhic, A.; Krarup-Hansen, A. Rising incidence of Merkel cell carcinoma. J. Plast. Surg. Hand Surg. 2011, 45, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Ezaldein, H.H.; Ventura, A.; DeRuyter, N.P.; Yin, E.S.; Giunta, A. Understanding the influence of patient demographics on disease severity, treatment strategy, and survival outcomes in merkel cell carcinoma: A surveillance, epidemiology, and end-results study. Oncoscience 2017, 4, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.Q.; Waldeck, K.; Vergara, I.A.; Schroder, J.; Madore, J.; Wilmott, J.S.; Colebatch, A.J.; De Paoli-Iseppi, R.; Li, J.; Lupat, R.; et al. UV-associated mutations underlie the etiology of MCV-negative merkel cell carcinomas. Cancer Res. 2015, 75, 5228–5234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moshiri, A.S.; Doumani, R.; Yelistratova, L.; Blom, A.; Lachance, K.; Shinohara, M.M.; Delaney, M.; Chang, O.; McArdle, S.; Thomas, H.; et al. Polyomavirus-Negative merkel cell carcinoma: A more aggressive subtype based on analysis of 282 cases using multimodal tumor virus detection. J. Investig. Dermatol. 2017, 137, 819–827. [Google Scholar] [CrossRef] [Green Version]
- Hasan, S.; Liu, L.; Triplet, J.; Li, Z.; Mansur, D. The role of postoperative radiation and chemoradiation in merkel cell carcinoma: A systematic review of the literature. Front. Oncol. 2013, 3, 276. [Google Scholar] [CrossRef] [Green Version]
- Harms, K.L.; Healy, M.A.; Nghiem, P.; Sober, A.J.; Johnson, T.M.; Bichakjian, C.K.; Wong, S.L. Analysis of prognostic factors from 9387 merkel cell carcinoma cases forms the basis for the new 8th edition ajcc staging system. Ann. Surg. Oncol. 2016, 23, 3564–3571. [Google Scholar] [CrossRef]
- Heath, M.; Jaimes, N.; Lemos, B.; Mostaghimi, A.; Wang, L.C.; Penas, P.F.; Nghiem, P. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: The AEIOU features. J. Am. Acad. Dermatol. 2008, 58, 375–381. [Google Scholar] [CrossRef] [Green Version]
- Andea, A.A.; Coit, D.G.; Amin, B.; Busam, K.J. Merkel cell carcinoma: Histologic features and prognosis. Cancer 2008, 113, 2549–2558. [Google Scholar] [CrossRef]
- Llombart, B.; Requena, C.; Cruz, J. Update on merkel cell carcinoma: Epidemiology, etiopathogenesis, clinical features, diagnosis, and staging. Actas Dermo Sifiliogr. 2017, 108, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Tetzlaff, M.T.; Harms, P.W. Danger is only skin deep: Aggressive epidermal carcinomas. An overview of the diagnosis, demographics, molecular-genetics, staging, prognostic biomarkers, and therapeutic advances in Merkel cell carcinoma. Mod. Pathol. 2020, 33, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Lebbe, C.; Becker, J.C.; Grob, J.J.; Malvehy, J.; Del Marmol, V.; Pehamberger, H.; Peris, K.; Saiag, P.; Middleton, M.R.; Bastholt, L.; et al. Diagnosis and treatment of Merkel Cell Carcinoma. European consensus-based interdisciplinary guideline. Eur. J. Cancer 2015, 51, 2396–2403. [Google Scholar] [CrossRef] [PubMed]
- van der Ploeg, A.P.; van Akkooi, A.C.; Schmitz, P.I.; Koljenovic, S.; Verhoef, C.; Eggermont, A.M. EORTC Melanoma Group sentinel node protocol identifies high rate of submicrometastases according to Rotterdam Criteria. Eur. J. Cancer 2010, 46, 2414–2421. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [Green Version]
- Hawryluk, E.B.; O’Regan, K.N.; Sheehy, N.; Guo, Y.; Dorosario, A.; Sakellis, C.G.; Jacene, H.A.; Wang, L.C. Positron emission tomography/computed tomography imaging in Merkel cell carcinoma: A study of 270 scans in 97 patients at the Dana-Farber/Brigham and Women’s Cancer Center. J. Am. Acad. Dermatol. 2013, 68, 592–599. [Google Scholar] [CrossRef]
- Siva, S.; Byrne, K.; Seel, M.; Bressel, M.; Jacobs, D.; Callahan, J.; Laing, J.; Macmanus, M.P.; Hicks, R.J. 18F-FDG PET provides high-impact and powerful prognostic stratification in the staging of Merkel cell carcinoma: A 15-year institutional experience. J. Nucl. Med. 2013, 54, 1223–1229. [Google Scholar] [CrossRef] [Green Version]
- Gunaratne, D.A.; Howle, J.R.; Veness, M.J. Sentinel lymph node biopsy in Merkel cell carcinoma: A 15-year institutional experience and statistical analysis of 721 reported cases. Br. J. Dermatol. 2016, 174, 273–281. [Google Scholar] [CrossRef]
- Frohm, M.L.; Griffith, K.A.; Harms, K.L.; Hayman, J.A.; Fullen, D.R.; Nelson, C.C.; Wong, S.L.; Schwartz, J.L.; Bichakjian, C.K. Recurrence and Survival in patients with merkel cell carcinoma undergoing surgery without adjuvant radiation therapy to the primary site. JAMA Dermatol. 2016, 152, 1001–1007. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.G.; Wang, L.C.; Penas, P.F.; Gellenthin, M.; Lee, S.J.; Nghiem, P. Sentinel lymph node biopsy for evaluation and treatment of patients with Merkel cell carcinoma: The Dana-Farber experience and meta-analysis of the literature. Arch. Dermatol. 2006, 142, 685–690. [Google Scholar] [CrossRef]
- Iyer, J.G.; Storer, B.E.; Paulson, K.G.; Lemos, B.; Phillips, J.L.; Bichakjian, C.K.; Zeitouni, N.; Gershenwald, J.E.; Sondak, V.; Otley, C.C.; et al. Relationships among primary tumor size, number of involved nodes, and survival for 8044 cases of Merkel cell carcinoma. J. Am. Acad. Dermatol. 2014, 70, 637–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeller, U.; Mueller, T.; Schubert, T.; Budach, V.; Ghadjar, P.; Brenner, W.; Kiecker, F.; Schicke, B.; Haase, O. Regional nodal relapse in surgically staged Merkel cell carcinoma. Strahlenther. Onkol. Organ Dtsch. Rontgenges. 2015, 191, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Lemos, B.D.; Storer, B.E.; Iyer, J.G.; Phillips, J.L.; Bichakjian, C.K.; Fang, L.C.; Johnson, T.M.; Liegeois-Kwon, N.J.; Otley, C.C.; Paulson, K.G.; et al. Pathologic nodal evaluation improves prognostic accuracy in Merkel cell carcinoma: Analysis of 5823 cases as the basis of the first consensus staging system. J. Am. Acad. Dermatol. 2010, 63, 751–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiengpruksawan, A.; Coit, D.G.; Thaler, H.T.; Urmacher, C.; Knapper, W.K. Merkel cell carcinoma. Prognosis and management. Arch. Surg. 1991, 126, 1514–1519. [Google Scholar] [CrossRef]
- Ott, M.J.; Tanabe, K.K.; Gadd, M.A.; Stark, P.; Smith, B.L.; Finkelstein, D.M.; Souba, W.W. Multimodality management of Merkel cell carcinoma. Arch. Surg. 1999, 134, 388–392, discussion 392–383. [Google Scholar] [CrossRef]
- Sattler, E.; Geimer, T.; Sick, I.; Flaig, M.J.; Ruzicka, T.; Berking, C.; Kunte, C. Sentinel lymph node in Merkel cell carcinoma: To biopsy or not to biopsy? J. Dermatol. 2013, 40, 374–379. [Google Scholar] [CrossRef]
- Perez, M.C.; de Pinho, F.R.; Holstein, A.; Oliver, D.E.; Naqvi, S.M.H.; Kim, Y.; Messina, J.L.; Burke, E.; Gonzalez, R.J.; Sarnaik, A.A.; et al. Resection Margins in merkel cell carcinoma: Is a 1-cm margin wide enough? Ann. Surg. Oncol. 2018, 25, 3334–3340. [Google Scholar] [CrossRef]
- Bhatia, S.; Storer, B.E.; Iyer, J.G.; Moshiri, A.; Parvathaneni, U.; Byrd, D.; Sober, A.J.; Sondak, V.K.; Gershenwald, J.E.; Nghiem, P. Adjuvant Radiation therapy and chemotherapy in merkel cell carcinoma: Survival analyses of 6908 cases from the national cancer data base. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.M.; Roman, S.A.; Sosa, J.A.; Judson, B.L. The role of adjuvant therapy in the management of head and neck merkel cell carcinoma: An analysis of 4815 patients. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Petrelli, F.; Ghidini, A.; Torchio, M.; Prinzi, N.; Trevisan, F.; Dallera, P.; De Stefani, A.; Russo, A.; Vitali, E.; Bruschieri, L.; et al. Adjuvant radiotherapy for Merkel cell carcinoma: A systematic review and meta-analysis. Radiother. Oncol. 2019, 134, 211–219. [Google Scholar] [CrossRef]
- Patel, S.A.; Qureshi, M.M.; Sahni, D.; Truong, M.T. Identifying an optimal adjuvant radiotherapy dose for extremity and trunk merkel cell carcinoma following resection: An analysis of the national cancer database. JAMA Dermatol. 2017, 153, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.A.; Qureshi, M.M.; Mak, K.S.; Sahni, D.; Giacalone, N.J.; Ezzat, W.; Jalisi, S.; Truong, M.T. Impact of total radiotherapy dose on survival for head and neck Merkel cell carcinoma after resection. Head neck 2017, 39, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, M.; Gaskins, J.; Wall, W.; Tennant, P.; Bumpous, J.; Dunlap, N. Optimal adjuvant radiotherapy dose for stage I, II or III Merkel cell carcinoma: An analysis of the National Cancer Database. Jpn. J. Clin. Oncol. 2019, 50, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Finnigan, R.; Hruby, G.; Wratten, C.; Keller, J.; Tripcony, L.; Dickie, G.; Rischin, D.; Poulsen, M. The impact of preradiation residual disease volume on time to locoregional failure in cutaneous Merkel cell carcinoma--a TROG substudy. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Tsang, G.; O’Brien, P.; Robertson, R.; Hamilton, C.; Wratten, C.; Denham, J. All delays before radiotherapy risk progression of Merkel cell carcinoma. Australas. Radiol. 2004, 48, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Fields, R.C.; Busam, K.J.; Chou, J.F.; Panageas, K.S.; Pulitzer, M.P.; Allen, P.J.; Kraus, D.H.; Brady, M.S.; Coit, D.G. Recurrence after complete resection and selective use of adjuvant therapy for stage I through III Merkel cell carcinoma. Cancer 2012, 118, 3311–3320. [Google Scholar] [CrossRef] [PubMed]
- Takagishi, S.R.; Marx, T.E.; Lewis, C.; Tarabadkar, E.S.; Juhlin, I.D.; Blom, A.; Iyer, J.G.; Liao, J.J.; Tseng, Y.D.; Fu, T.; et al. Postoperative radiation therapy is associated with a reduced risk of local recurrence among low risk Merkel cell carcinomas of the head and neck. Adv. Radiat. Oncol. 2016, 1, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Grotz, T.E.; Joseph, R.W.; Pockaj, B.A.; Foote, R.L.; Otley, C.C.; Bagaria, S.P.; Weaver, A.L.; Jakub, J.W. Negative sentinel lymph node biopsy in merkel cell carcinoma is associated with a low risk of same-nodal-basin recurrences. Ann. Surg. Oncol. 2015, 22, 4060–4066. [Google Scholar] [CrossRef]
- Gunaratne, D.A.; Howle, J.R.; Veness, M.J. Definitive radiotherapy for Merkel cell carcinoma confers clinically meaningful in-field locoregional control: A review and analysis of the literature. J. Am. Acad. Dermatol. 2017, 77, 142–148. [Google Scholar] [CrossRef]
- Pape, E.; Rezvoy, N.; Penel, N.; Salleron, J.; Martinot, V.; Guerreschi, P.; Dziwniel, V.; Darras, S.; Mirabel, X.; Mortier, L. Radiotherapy alone for Merkel cell carcinoma: A comparative and retrospective study of 25 patients. J. Am. Acad. Dermatol. 2011, 65, 983–990. [Google Scholar] [CrossRef]
- Perez, M.C.; Oliver, D.E.; Weitman, E.S.; Boulware, D.; Messina, J.L.; Torres-Roca, J.; Cruse, C.W.; Gonzalez, R.J.; Sarnaik, A.A.; Sondak, V.K.; et al. Management of sentinel lymph node metastasis in merkel cell carcinoma: Completion lymphadenectomy, radiation, or both? Ann. Surg. Oncol. 2019, 26, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Durham, A.B.; Bichakjian, C.K.; Harms, P.W.; Hayman, J.A.; McLean, S.A.; Harms, K.L.; Burns, W.R. Completion lymph node dissection or radiation therapy for sentinel node metastasis in merkel cell carcinoma. Ann. Surg. Oncol. 2019, 26, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Mehrany, K.; Otley, C.C.; Weenig, R.H.; Phillips, P.K.; Roenigk, R.K.; Nguyen, T.H. A meta-analysis of the prognostic significance of sentinel lymph node status in Merkel cell carcinoma. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2002, 28, 113–117, discussion 117. [Google Scholar] [CrossRef]
- Fang, L.C.; Lemos, B.; Douglas, J.; Iyer, J.; Nghiem, P. Radiation monotherapy as regional treatment for lymph node-positive Merkel cell carcinoma. Cancer 2010, 116, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Adjuvant Avelumab in MCC (ADAM). Available online: https://clinicaltrials.gov/ct2/show/NCT03271372 (accessed on 11 March 2019).
- Cornejo, C.; Miller, C.J. Merkel cell carcinoma: Updates on staging and management. Dermatol. Clin. 2019, 37, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.G.; Tan, D.; Yu, S.S. Recent advances in Merkel cell carcinoma. F1000Res 2019, 8. [Google Scholar] [CrossRef] [Green Version]
- Nghiem, P.; Kaufman, H.L.; Bharmal, M.; Mahnke, L.; Phatak, H.; Becker, J.C. Systematic literature review of efficacy, safety and tolerability outcomes of chemotherapy regimens in patients with metastatic Merkel cell carcinoma. Future Oncol. 2017, 13, 1263–1279. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, H.; Lambert, J.; Barbosa, C.D.; Guillemin, I.; Mahnke, L.; Bharmal, M. Patient experiences with avelumab vs. chemotherapy for treating MCC: Results from protocol-specified qualitative research. J. Clin. Oncol. 2017, 2017, e21065. [Google Scholar] [CrossRef]
- Nghiem, P.T.; Bhatia, S.; Lipson, E.J.; Kudchadkar, R.R.; Miller, N.J.; Annamalai, L.; Berry, S.; Chartash, E.K.; Daud, A.; Fling, S.P.; et al. PD-1 blockade with pembrolizumab in advanced merkel-cell carcinoma. N. Engl. J. Med. 2016, 374, 2542–2552. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Russell, J.; Lebbe, C.; Chmielowski, B.; Gambichler, T.; Grob, J.J.; Kiecker, F.; Rabinowits, G.; Terheyden, P.; Zwiener, I.; et al. Efficacy and safety of first-line avelumab treatment in patients with stage iv metastatic merkel cell carcinoma: A preplanned interim analysis of a clinical trial. JAMA Oncol. 2018, 4, e180077. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, H.L.; Russell, J.S.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbe, C.; Milella, M.; Brownell, I.; et al. Updated efficacy of avelumab in patients with previously treated metastatic Merkel cell carcinoma after >/=1 year of follow-up: JAVELIN Merkel 200, a phase 2 clinical trial. J. Immunother. Cancer 2018, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Food and Drug Administration (FDA). Approval Of Avelumab. Available online: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm548278.htm (accessed on 29 January 2019).
- Nghiem, P.; Bhatia, S.; Lipson, E.J.; Sharfman, W.H.; Kudchadkar, R.R.; Brohl, A.S.; Friedlander, P.A.; Daud, A.; Kluger, H.M.; Reddy, S.A.; et al. Durable tumor regression and overall survival in patients with advanced merkel cell carcinoma receiving pembrolizumab as first-line therapy. J. Clin. Oncol. 2019, 37, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Walocko, F.M.; Scheier, B.Y.; Harms, P.W.; Fecher, L.A.; Lao, C.D. Metastatic Merkel cell carcinoma response to nivolumab. J. Immunother. Cancer 2016, 4, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabol, A.J.; Markovic, S.; Otley, C. Benefit of chemotherapy in patients with Merkel cell carcinoma with distant metastases and visceral organ involvement. J. Clin. Oncol. 2016. [Google Scholar] [CrossRef]
- Iyer, J.G.; Blom, A.; Doumani, R.; Lewis, C.; Tarabadkar, E.S.; Anderson, A.; Ma, C.; Bestick, A.; Parvathaneni, U.; Bhatia, S.; et al. Response rates and durability of chemotherapy among 62 patients with metastatic Merkel cell carcinoma. Cancer Med. 2016, 5, 2294–2301. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network (NCCN). Guidelines-Merkel Cell Carcinoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/mcc.pdf (accessed on 16 September 2019).
- Becker, J.C.; Lorenz, E.; Ugurel, S.; Eigentler, T.K.; Kiecker, F.; Pfohler, C.; Kellner, I.; Meier, F.; Kahler, K.; Mohr, P.; et al. Evaluation of real-world treatment outcomes in patients with distant metastatic Merkel cell carcinoma following second-line chemotherapy in Europe. Oncotarget 2017, 8, 79731–79741. [Google Scholar] [CrossRef] [Green Version]
- Cowey, C.L.; Mahnke, L.; Espirito, J.; Helwig, C.; Oksen, D.; Bharmal, M. Real-world treatment outcomes in patients with metastatic Merkel cell carcinoma treated with chemotherapy in the USA. Future Oncol. 2017, 13, 1699–1710. [Google Scholar] [CrossRef] [Green Version]
- Allen, P.J.; Bowne, W.B.; Jaques, D.P.; Brennan, M.F.; Busam, K.; Coit, D.G. Merkel cell carcinoma: Prognosis and treatment of patients from a single institution. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 2300–2309. [Google Scholar] [CrossRef] [Green Version]
- Nivolumab Treatment for Virus-Associated Cancers (CheckMate 358). Available online: https://clinicaltrials.gov/ct2/show/NCT02488759 (accessed on 18 February 2020).



{kind=link}
{kind=link}
| Cancer Type | CK (AE1/AE3) | CK20 | CK7 | TTF-1 | CD56 | LCA | S-100 | CD-99 | Chromogranin A | Synaptophysin |
|---|---|---|---|---|---|---|---|---|---|---|
| Merkel cell carcinoma | + | + | − | − | + | − | − | + | + | + |
| Small cell lung cancer | + | − | + | + | + | − | − | + | + | + |
| Lymphoma | − | − | − | − | − | + | − | − | − | − |
| Melanoma | −/(+) | − | − | − | + | − | + | − | − | − |
| Ewing’s sarcoma | −/(+) | − | − | − | + | − | - | + | −/(+) | −/(+) |
| Stage | Patients Upstaged by PET/CT | Patients Upstaged by PET/CT (%) |
|---|---|---|
| IA | 0/12 | 0% |
| IB | 0/5 | 0% |
| IIA | 0/3 | 0% |
| IIB | 0/5 | 0% |
| IIIA | 1/22 | 4.5% |
| IIIB | 4/8 | 50% |
| IV | 5/5 | 100% |
| Stage | Clinical Staging (95% CI) | Pathological Staging (95% CI) |
|---|---|---|
| I | 45.0% (41.9–48.1%) | 62.8% (59.6–65.8%) |
| IIA | 30.9% (27.0–34.9%) | 54.6% (49.3–59.7%) |
| IIB | 27.3% (16.0–39.9%) | 34.8% (25.6–44.1%) |
| IIIA | Data lacking | 40.3% (37.5–43.0%) |
| IIIB | Data lacking | 26.8% (23.4–30.4%) |
| IV | Data lacking | 13.5% (11.0–16.3%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naseri, S.; Steiniche, T.; Ladekarl, M.; Bønnelykke-Behrndtz, M.L.; Hölmich, L.R.; Langer, S.W.; Venzo, A.; Tabaksblat, E.; Klausen, S.; Skaarup Larsen, M.; et al. Management Recommendations for Merkel Cell Carcinoma—A Danish Perspective. Cancers 2020, 12, 554. https://doi.org/10.3390/cancers12030554
Naseri S, Steiniche T, Ladekarl M, Bønnelykke-Behrndtz ML, Hölmich LR, Langer SW, Venzo A, Tabaksblat E, Klausen S, Skaarup Larsen M, et al. Management Recommendations for Merkel Cell Carcinoma—A Danish Perspective. Cancers. 2020; 12(3):554. https://doi.org/10.3390/cancers12030554
Chicago/Turabian StyleNaseri, Simon, Torben Steiniche, Morten Ladekarl, Marie Louise Bønnelykke-Behrndtz, Lisbet R. Hölmich, Seppo W. Langer, Alessandro Venzo, Elizaveta Tabaksblat, Siri Klausen, Mathilde Skaarup Larsen, and et al. 2020. "Management Recommendations for Merkel Cell Carcinoma—A Danish Perspective" Cancers 12, no. 3: 554. https://doi.org/10.3390/cancers12030554