Multicenter External Validation of the Liverpool Uveal Melanoma Prognosticator Online: An OOG Collaborative Study


 ,
,  , , , , , , , add
Show full author list
, , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Statistical Analyses
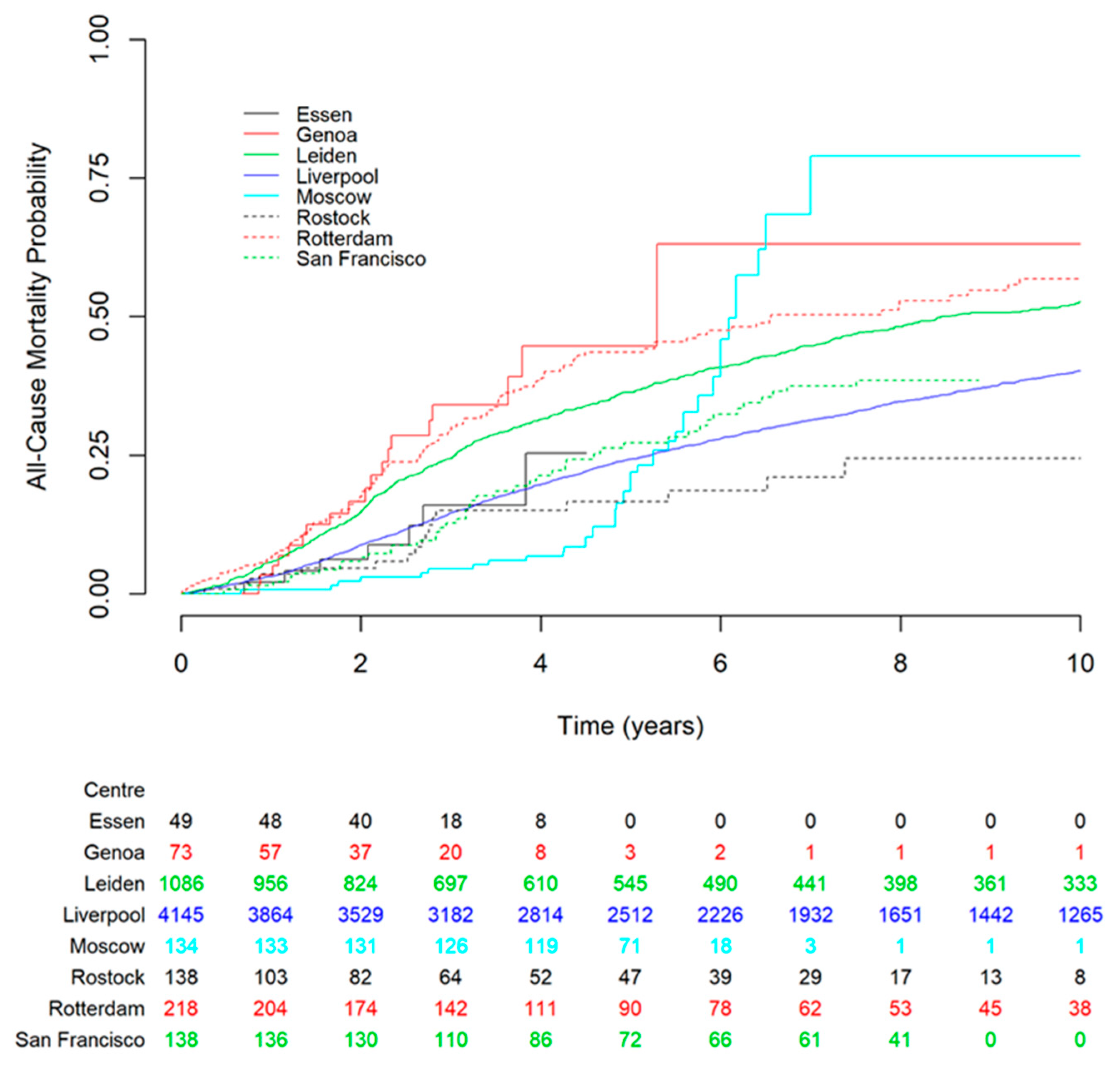
2.2.1. Discrimination
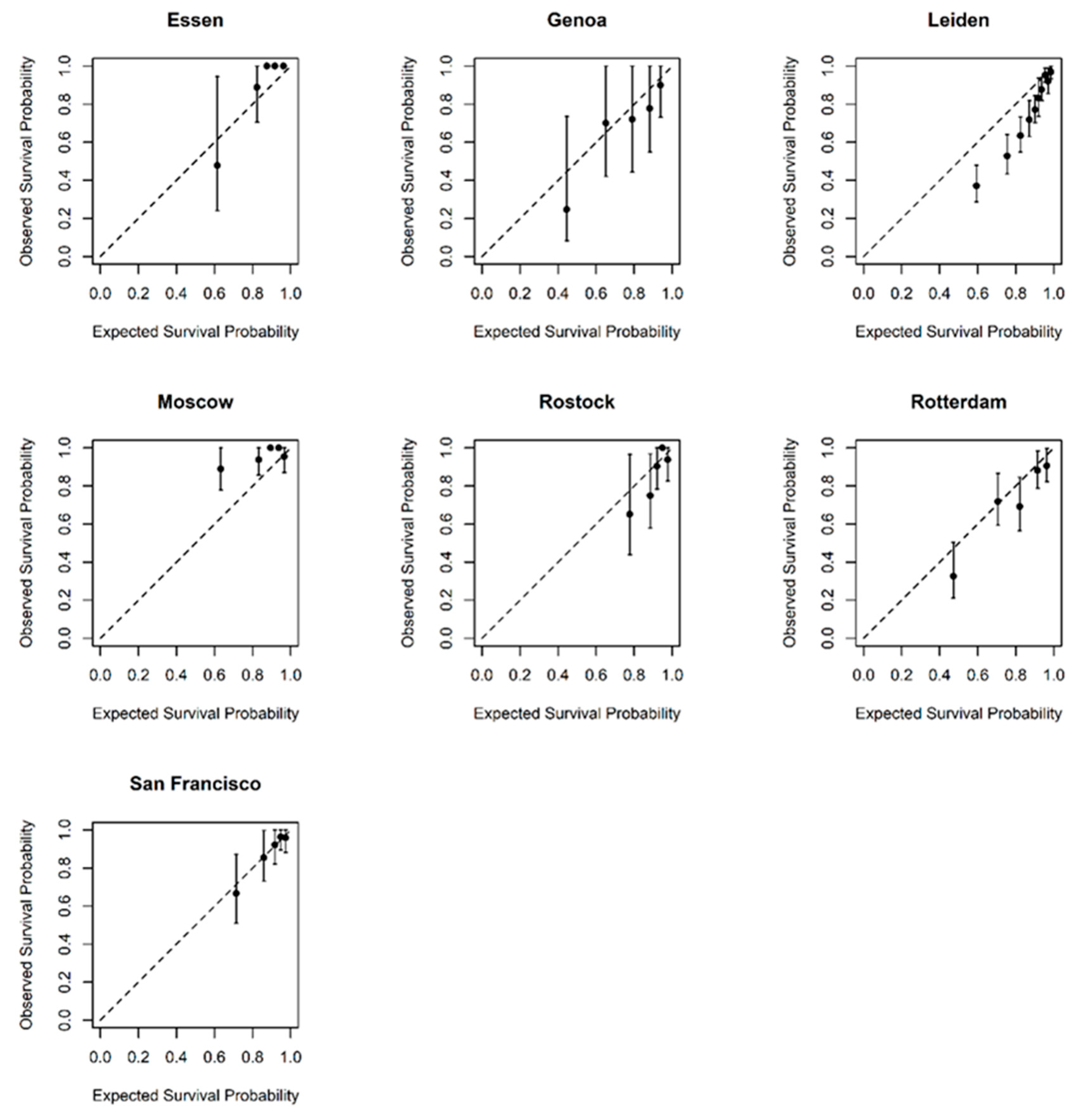
2.2.2. Calibration
3. Discussion
4. Material and Methods
4.1. Ethics
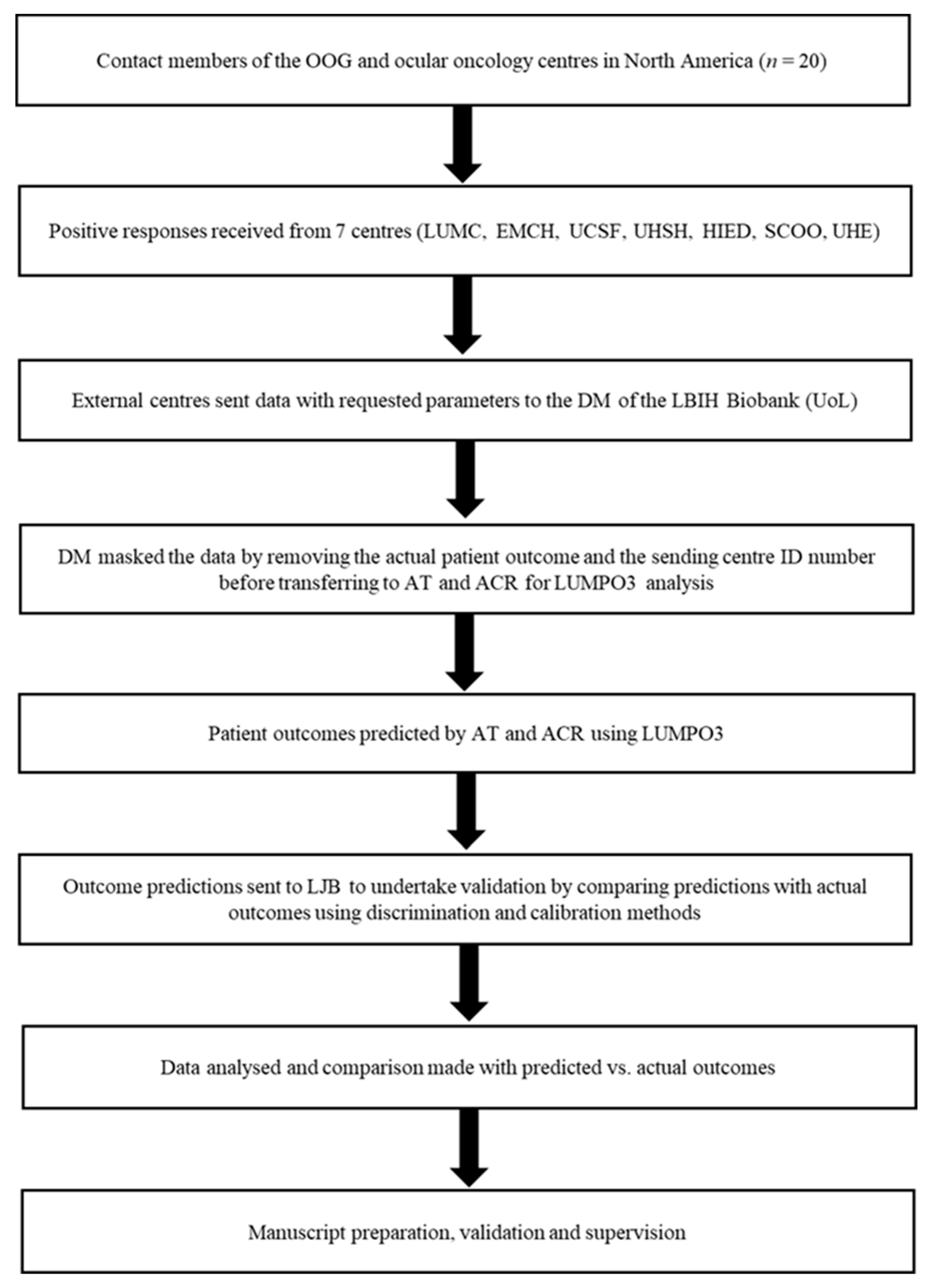
4.2. Data Collection
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singh, N.; Bergman, L.; Seregard, S.; Singh, A.D. Uveal melanoma: Epidemiologic aspects. In Clinical Ophthalmic Oncology: Uveal Tumors; Damato, B., Singh, A.D., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 75–87. [Google Scholar]
- Singh, A.D.; Borden, E.C. Metastatic uveal melanoma. Ophthalmol. Clin. 2005, 18, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Damato, B.; Heimann, H. Personalized treatment of uveal melanoma. Eye 2013, 27, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Cook, S.A.; Damato, B.; Marshall, E.; Salmon, P.J.H.E. Reconciling the principle of patient autonomy with the practice of informed consent: Decision-making about prognostication in uveal melanoma. Health Expect. 2011, 14, 383–396. [Google Scholar] [CrossRef] [Green Version]
- Beran, T.M.; McCannel, T.A.; Stanton, A.L.; Straatsma, B.R.; Burgess, B.L. Reactions to and desire for prognostic testing in choroidal melanoma patients. J. Genet. Couns. 2009, 18, 265–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacco, J.J.; Kalirai, H.; Kenyani, J.; Figueiredo, C.R.; Coulson, J.M.; Coupland, S.E. Recent breakthroughs in metastatic uveal melanoma: A cause for optimism? Future Med. 2018, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eleuteri, A.; Damato, B.; Coupland, S.E.; Taktak, A.F.G. Enhancing survival prognostication in patients with choroidal melanoma by integrating pathologic, clinical and genetic predictors of metastasis. Int. J. Biomed. Eng. Technol. 2012, 1, 18–35. [Google Scholar] [CrossRef]
- Dogrusöz, M.; Jager, M.J. Genetic prognostication in uveal melanoma. Acta Ophthalmol. 2018, 96, 331–347. [Google Scholar] [CrossRef]
- Damato, B. Progress in the management of patients with uveal melanoma. The 2012 ashton lecture. Eye 2012, 26, 1157–1172. [Google Scholar] [CrossRef] [Green Version]
- Rospond-Kubiak, I.; Wroblewska-Zierhoffer, M.; Twardosz-Pawlik, H.; Kociecki, J. The liverpool uveal melanoma prognosticator online (lumpo) for prognosing metastasis free survival in the absence of cytogenetic data after ruthenium brachytherapy for uveal melanoma. Acta Ophthalmol. 2015, 93. [Google Scholar] [CrossRef]
- DeParis, S.W.; Taktak, A.; Eleuteri, A.; Enanoria, W.; Heimann, H.; Coupland, S.E.; Damato, B. External validation of the liverpool uveal melanoma prognosticator online. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6116–6122. [Google Scholar] [CrossRef] [Green Version]
- Eleuteri, A.; Taktak, A.F.G.; Coupland, S.E.; Heimann, H.; Kalirai, H.; Damato, B. Prognostication of metastatic death in uveal melanoma patients: A markov multi-state model. Comput. Biol. Med. 2018, 102, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B. Overall c as a measure of discrimination in survival analysis: Model specific population value and confidence interval estimation. Stat. Med. 2004, 23, 2109–2123. [Google Scholar] [CrossRef] [PubMed]
- McGrath, S.; Zhao, X.; Qin, Z.Z.; Steele, R.; Benedetti, A. One-sample aggregate data meta-analysis of medians. Stat. Med. 2019, 38, 969–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taktak, A.; Antolini, L.; Aung, M.; Boracchi, P.; Campbell, I.; Damato, B.; Ifeachor, E.; Lama, N.; Lisboa, P.; Setzkorn, C.; et al. Double-blind evaluation and benchmarking of survival models in a multi-centre study. Comput. Biol. Med. 2007, 37, 1108–1120. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L.; Shields, J.A. Uveal melanoma: Estimating prognosis. Indian J. Ophthalmol. 2015, 63, 93–102. [Google Scholar] [CrossRef]
- Marshall, E.; Romaniuk, C.; Ghaneh, P.; Wong, H.; McKay, M.; Chopra, M.; Coupland, S.E.; Damato, B.E. Mri in the detection of hepatic metastases from high-risk uveal melanoma: A prospective study in 188 patients. Br. J. Ophthalmol. 2013, 97, 159–163. [Google Scholar] [CrossRef]
- Gomez, D.; Wetherill, C.; Cheong, J.; Jones, L.; Marshall, E.; Damato, B.; Coupland, S.E.; Ghaneh, P.; Poston, G.J.; Malik, H.Z.; et al. The liverpool uveal melanoma liver metastases pathway: Outcome following liver resection. J. Surg. Oncol. 2014, 109, 542–547. [Google Scholar] [CrossRef]
- Amin, M.B.; American Joint Committee on Cancer; American Cancer Society. AJCC Cancer Staging Manual, 8th ed.; Springer: Chicago, IL, USA, 2017; 1024p. [Google Scholar]
- Dogrusoz, M.; Bagger, M.; van Duinen, S.G.; Kroes, W.G.; Ruivenkamp, C.A.L.; Bohringer, S.; Andersen, K.K.; Luyten, G.P.M.; Kiilgaard, J.F.; Jager, M.J. The prognostic value of ajcc staging in uveal melanoma is enhanced by adding chromosome 3 and 8q status. Investig. Ophthalmol. Vis. Sci. 2017, 58, 969–984. [Google Scholar] [CrossRef] [Green Version]
- Bagger, M.M. Intraocular biopsy of uveal melanoma risk assessment and identification of genetic prognostic markers. Acta Ophthalmol. 2018, 96, 6–28. [Google Scholar] [CrossRef] [Green Version]
- Walter, S.D.; Chao, D.L.; Feuer, W.; Schiffman, J.; Char, D.H.; Harbour, J.W. Prognostic implications of tumor diameter in association with gene expression profile for uveal melanoma. JAMA Ophthalmol. 2016, 134, 734–740. [Google Scholar] [CrossRef] [Green Version]
- Vaquero-Garcia, J.; Lalonde, E.; Ewens, K.G.; Ebrahimzadeh, J.; Richard-Yutz, J.; Shields, C.L.; Barrera, A.; Green, C.J.; Barashal, Y.; Ganguly, A. Primeum: A model for predicting risk of metastasis in uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2017, 58, 4096–4105. [Google Scholar] [CrossRef] [PubMed]
- Kaiserman, I.; Rosner, M.; Pe’er, J. Forecasting the prognosis of choroidal melanoma with an artificial neural network. Ophthalmology 2005, 112, 1608–1611. [Google Scholar] [CrossRef]
- Onken, M.D.; Worley, L.A.; Char, D.H.; Augsburger, J.J.; Correa, Z.M.; Nudleman, E.; Aaberg, T.M.; Altaweel, M.M.; Bardenstein, D.S.; Finger, P.T.; et al. Collaborative ocular oncology group report number 1: Prospective validation of a multi-gene prognostic assay in uveal melanoma. Ophthalmology 2012, 119, 1596–1603. [Google Scholar] [CrossRef] [Green Version]
- Plasseraud, K.M.; Cook, R.W.; Tsai, T.; Shildkrot, Y.; Middlebrook, B.; Maetzold, D.; Wilkinson, J.; Stone, J.; Johnson, C.; Oelschlager, K.; et al. Clinical performance and management outcomes with the decisiondx-um gene expression profile test in a prospective multicenter study. J. Oncol. 2016, 2016, 5325762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caines, R.; Eleuteri, A.; Kalirai, H.; Fisher, A.C.; Heimann, H.; Damato, B.E.; Coupland, S.E.; Taktak, A.F.G. Cluster analysis of multiplex ligation-dependent probe amplification data in choroidal melanoma. Mol. Vis. 2015, 21, 1–11. [Google Scholar] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for some traditional and novel measures. Epidemiol. (Camb. Mass.) 2010, 21, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Snell, K.I.E.; Hua, H.; Debray, T.P.A.; Ensor, J.; Look, M.P.; Moons, K.G.M.; Riley, R.D. Multivariate meta-analysis of individual participant data helped externally validate the performance and implementation of a prediction model. J. Clin. Epidemiol. 2016, 69, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Robertson, A.G.; Shih, J.; Yau, C.; Gibb, E.A.; Oba, J.; Mungall, K.L.; Hess, J.M.; Uzunangelov, V.; Walter, V.; Danilova, L.; et al. Integrative analysis identifies four molecular and clinical subsets in uveal melanoma. Cancer Cell 2017, 32, 204–220. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics, n (%) Unless Otherwise Stated | Liverpool (n = 4145) | Leiden (n = 1086) | Rotterdam (n = 218) | San Francisco (n = 138) | Rostock (n = 138) | Moscow (n = 134) | Genoa (n = 73) | Essen (n = 49) | Pooled Estimates |
|---|---|---|---|---|---|---|---|---|---|
| Age at treatment (years), mean (SD) | 61.4 (14.1) | 60.7 (14.4) | 62.0 (14.3) | 60.0 (13.1) | 64.8 (13.8) | 53.0 (13.7) | 62.0 (16.2) | 63.8 (14.7) | 61.2 (14.2) |
| Sex | |||||||||
| Female | 2010 (48) | 498 (46) | 111 (51) | 67 (49) | 80 (58) | 84 (63) | 26 (36) | 27 (55) | 2903 (48) |
| Male | 2135 (52) | 588 (54) | 107 (49) | 71 (51) | 58 (42) | 50 (37) | 47 (64) | 22 (45) | 3078 (52) |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Largest Ultrasound Diameter (mm), mean (SD) | 12.4 (3.8) | 11.2 (3.7) | 12.9 (3.6) | 11.2 (3.3) | 11.3 (3.5) | 15.4 (3.3) | 15.5 (3.3) | 13.8 (3.7) | 12.3 (3.7) |
| Missing | 110 | 0 | 4 | 4 | 0 | 0 | 0 | 0 | 118 |
| Ultrasound tumour Height (mm), mean (SD) | 5.3 (3.4) | 5.6 (3.3) | 7.38 (3.5) | 5.3 (2.1) | 5.2 (2.9) | 9.1 (2.9) | 10.8 (3.5) | 8.6 (3.5) | 5.6 (3.3) |
| Missing | 98 | 1 | 6 | 0 | 0 | 0 | 1 | 0 | 106 |
| Ciliary Body Involvement | |||||||||
| No | 3046 (73) | 803 (74) | 154 (71) | 32 (84) | 130 (94) | 93 (69) | 63 (86) | 33 (69) | 4354 (74) |
| Yes | 1098 (27) | 283 (26) | 64 (29) | 6 (16) | 8 (6) | 41 (31) | 10 (14) | 15 (31) | 1525 (26) |
| Missing | 1 | 0 | 0 | 100 | 0 | 0 | 0 | 1 | 102 |
| Extraocular Melanoma | |||||||||
| No | 3872 (93) | 848 (79) | 191 (88) | 134 (99) | 130 (96) | 119 (89) | 73 (100) | 35 (92) | 5402 (90) |
| Yes | 273 (7) | 228 (21) | 27 (12) | 1 (1) | 5 (4) | 15 (11) | 0 (0) | 3 (8) | 552 (10) |
| Missing | 0 | 10 | 0 | 0 | 3 | 0 | 0 | 11 | 24 |
| Epithelioid cells present | |||||||||
| No | 915 (42) | 351 (33) | 74 (34) | 38 (55) | 31 (97) | 61 (46) | 0 (0) | - | 1470 (39) |
| Yes | 1268 (58) | 720 (67) | 144 (66) | 31 (45) | 1 (3) | 71 (53) | 56 (100) | - | 2291 (61) |
| Missing | 1962 | 15 | 0 | 0 | 106 | 2 | 17 | 49 | 2151 |
| Closed PAS+ Loops | |||||||||
| No | 600 (50) | 230 (40) | 124 (58) | - | - | - | - | - | 954 (48) |
| Yes | 597 (50) | 346 (60) | 88 (42) | - | - | - | - | - | 1031 (52) |
| Missing | 2948 | 510 | 0 | 138 | 138 | 134 | 73 | 49 | 3990 |
| MITOC (n, %) | |||||||||
| 0 | 673 (38) | 173 (17) | 14 (8) | 1 (20) | 32 (100) | - | - | - | 893 (30) |
| 1 | 414 (23) | 282 (28) | 27 (16) | 0 (0) | 0 (0) | - | - | - | 723 (24) |
| 2 | 366 (21) | 291 (29) | 45 (27) | 4 (80) | 0 (0) | - | - | - | 706 (24) |
| 3 | 307 (17) | 264 (26) | 81 (49) | 0 (0) | 0 (0) | - | - | - | 652 (22) |
| Missing | 2385 | 76 | 51 | 133 | 106 | 134 | 73 | 49 | 3007 |
| Chromosome 3 loss | |||||||||
| No | 333 (55) | 201 (50) | 100 (46) | 22 (58) | - | 77 (57) | 27 (39) | 37 (76) | 797 (53) |
| Yes | 269 (45) | 202 (50) | 117 (54) | 16 (42) | - | 57 (43) | 43 (61) | 12 (24) | 716 (47) |
| Missing | 3543 | 683 | 1 | 100 | 138 | 0 | 3 | 0 | 4468 |
| Chromosome 8 gain | |||||||||
| No | 330 (55) | 186 (53) | 82 (38) | 21 (55) | - | 97 (72) | 23 (34) | - | 739 (52) |
| Yes | 272 (45) | 162 (47) | 136 (62) | 17 (45) | - | 37 (28) | 45 (66) | - | 669 (48) |
| Missing | 3543 | 738 | 0 | 100 | 138 | 0 | 5 | 49 | 4573 |
| Follow-up time (years), median | 6.5 | 5.2 | 4.0 | 0.7 | 2.7 | 5.0 | 2.0 | 2.7 | 6.5 |
| (IQR) | (3.2–11.7) | (4.3–5.9) | (2.3–8.0) | (0.5–2.1) | (1.0–6.5) | (4.5–5.7) | (1.1–3.0) | (2.1–3.3) | (3.2–11.7) |
| Outcome | |||||||||
| Alive | 2480 (60) | 440 (41) | 98 (45) | 94 (68) | 121 (88) | 92 (69) | 54 (74) | 42 (86) | 3421 (57) |
| Dead | 1665 (40) | 646 (59) | 120 (55) | 44 (32) | 17 (12) | 42 (31) | 19 (26) | 7 (14) | 2560 (43) |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Cause of Death | |||||||||
| Other | 770 (46) | 291 (45) | 36 (30) | - | 4 (27) | 5 (12) | 2 (11) | 2 (33) | 1110 (43) |
| Possible UM metastasis | 0 (0) | 0 (0) | 0 (0) | - | 6 (40) | 10 (24) | 2 (11) | 1 (17) | 19 (2) |
| Definite UM metastasis | 893 (54) | 355 (55) | 78 (70) | - | 5 (33) | 27 (64) | 16 (84) | 3 (50) | 1377 (55) |
| Missing | 2 | 0 | 6 | 44 | 2 | 0 | 0 | 1 | 55 |
| Dataset | 1 year | 2 year | 3 year | 4 year |
|---|---|---|---|---|
| Essen | 0.85 (0.72, 0.98) | 0.87 (0.77, 0.98) | 0.89 (0.80, 0.98) | 0.89 (0.80, 0.98) |
| Genoa | 0.78 (0.68, 0.88) | 0.78 (0.68, 0.88) | 0.78 (0.69, 0.88) | 0.78 (0.69, 0.88) |
| Leiden | 0.72 (0.70, 0.74) | 0.73 (0.71, 0.75) | 0.73 (0.71, 0.75) | 0.73 (0.71, 0.75) |
| Moscow | 0.65 (0.56, 0.74) | 0.64 (0.54, 0.75) | 0.65 (0.54, 0.75) | 0.65 (0.54, 0.75) |
| Rostock | 0.70 (0.57, 0.84) | 0.72 (0.59, 0.84) | 0.71 (0.57, 0.84) | 0.71 (0.58, 0.84) |
| Rotterdam | 0.73 (0.69, 0.78) | 0.74 (0.69, 0.78) | 0.74 (0.69, 0.78) | 0.74 (0.69, 0.78) |
| San Francisco | 0.64 (0.56, 0.72) | 0.66 (0.58, 0.74) | 0.66 (0.58, 0.74) | 0.66 (0.58, 0.74) |
| Pooled estimate | 0.72 (0.68, 0.75) | 0.73 (0.70, 0.77) | 0.73 (0.70, 0.77) | 0.73 (0.70, 0.77) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cunha Rola, A.; Taktak, A.; Eleuteri, A.; Kalirai, H.; Heimann, H.; Hussain, R.; Bonnett, L.J.; Hill, C.J.; Traynor, M.; Jager, M.J.; et al. Multicenter External Validation of the Liverpool Uveal Melanoma Prognosticator Online: An OOG Collaborative Study. Cancers 2020, 12, 477. https://doi.org/10.3390/cancers12020477
Cunha Rola A, Taktak A, Eleuteri A, Kalirai H, Heimann H, Hussain R, Bonnett LJ, Hill CJ, Traynor M, Jager MJ, et al. Multicenter External Validation of the Liverpool Uveal Melanoma Prognosticator Online: An OOG Collaborative Study. Cancers. 2020; 12(2):477. https://doi.org/10.3390/cancers12020477
Chicago/Turabian StyleCunha Rola, Alda, Azzam Taktak, Antonio Eleuteri, Helen Kalirai, Heinrich Heimann, Rumana Hussain, Laura J. Bonnett, Christopher J. Hill, Matthew Traynor, Martine J. Jager, and et al. 2020. "Multicenter External Validation of the Liverpool Uveal Melanoma Prognosticator Online: An OOG Collaborative Study" Cancers 12, no. 2: 477. https://doi.org/10.3390/cancers12020477