Real-World Data on Cabozantinib in Previously Treated Patients with Metastatic Renal Cell Carcinoma: Focus on Sequences and Prognostic Factors

 , , , , , , ,
, , , , , , ,  , ,
, ,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Overall Population
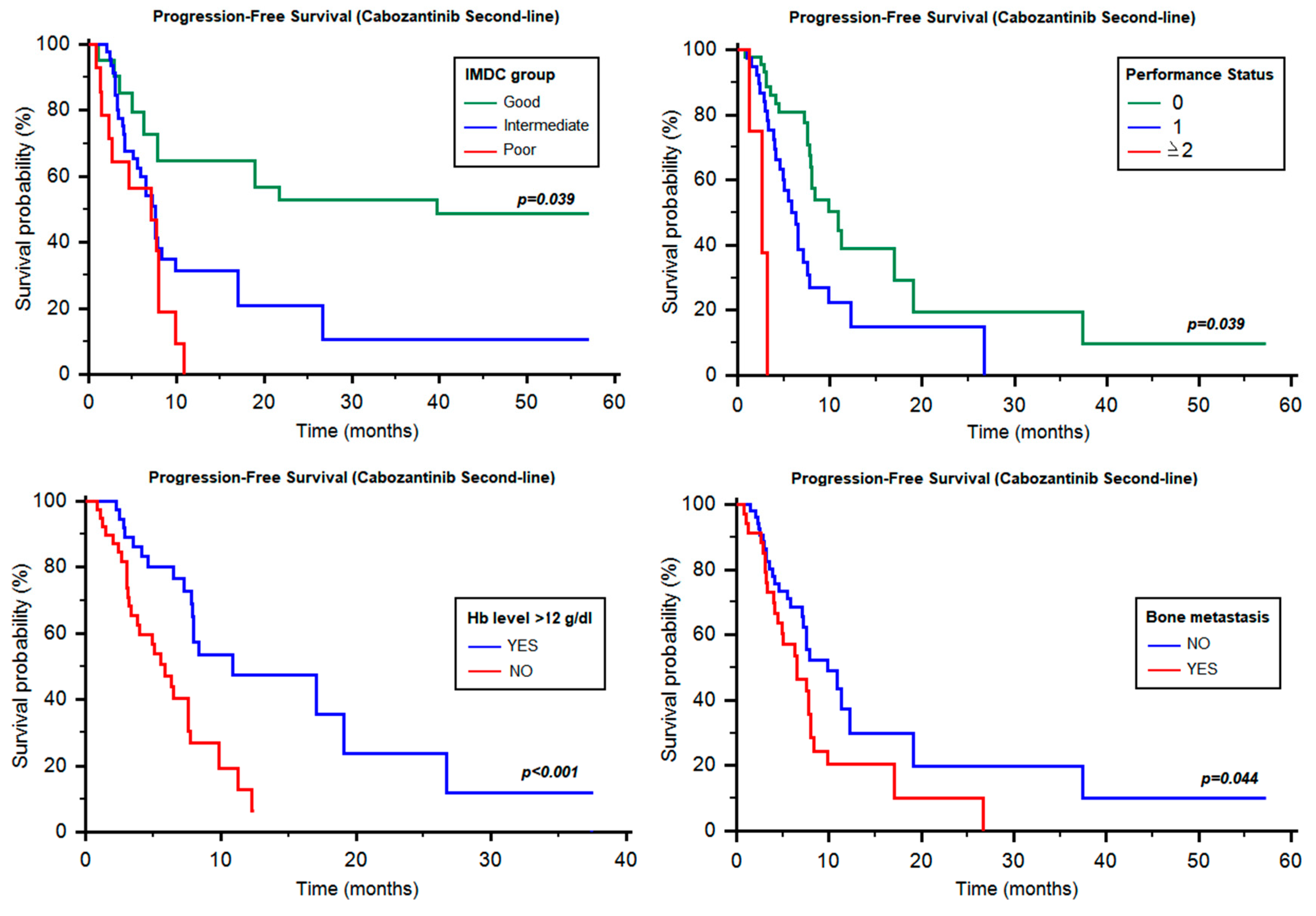
2.2. Progression-Free Survival of Cabozantinib as Second-Line Therapy
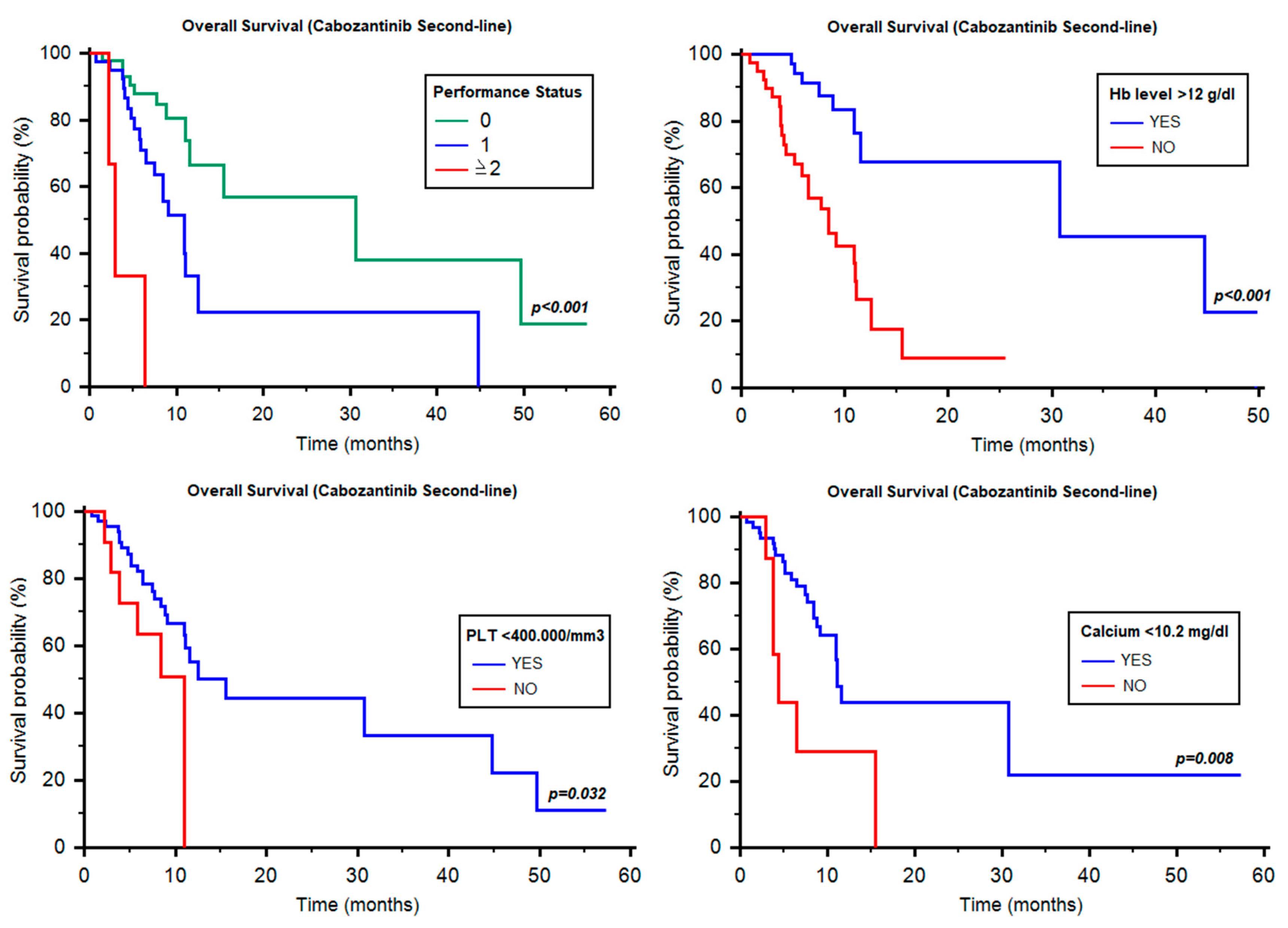
2.3. Overall Survival of Cabozantinib as Second-Line Therapy
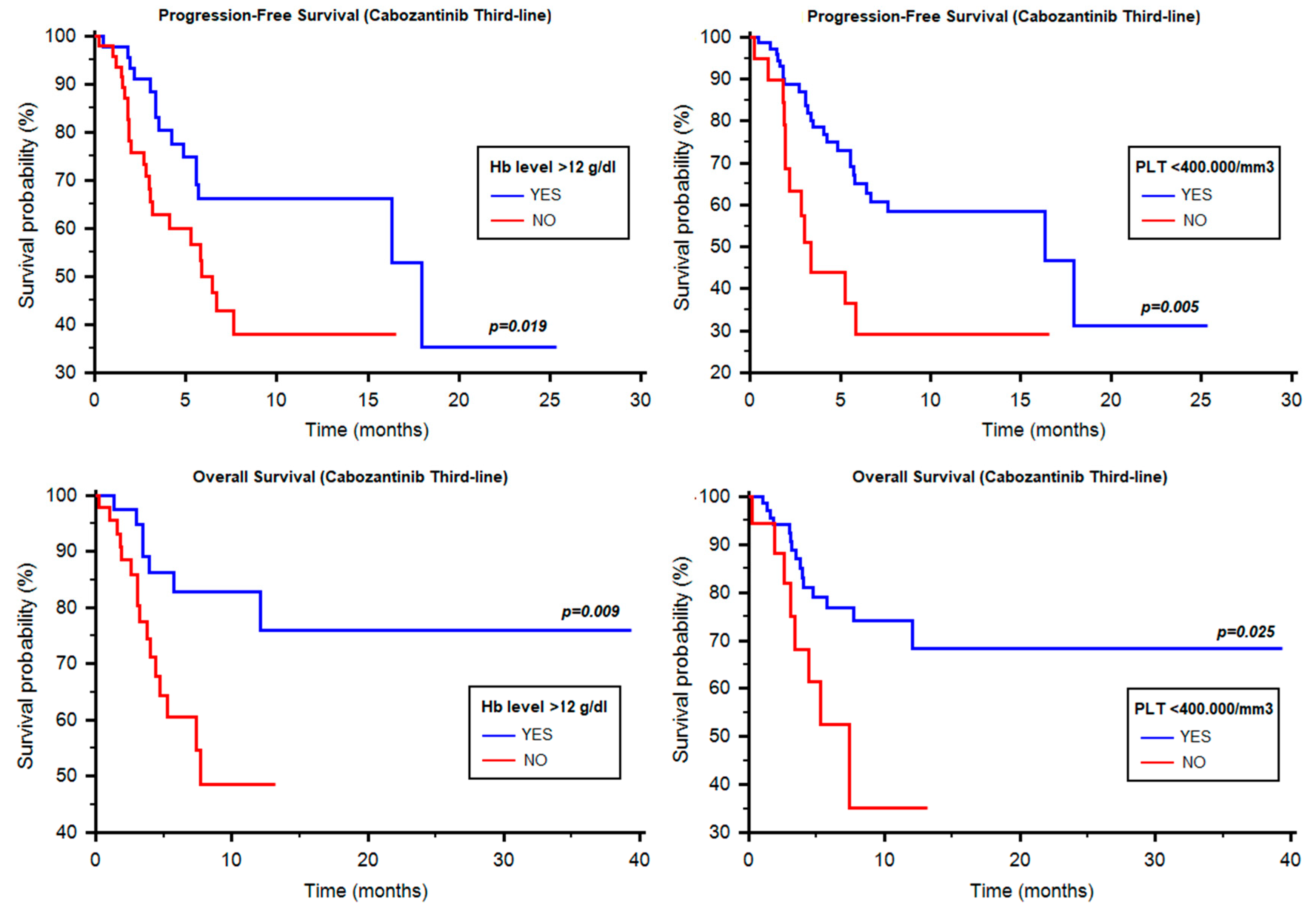
2.4. Progression-Free Survival of Cabozantinib as Third-Line Therapy
2.5. Overall Survival of Cabozantinib as Third-Line Therapy
2.6. Time to Strategy Failure and Sequencing: Cabozantinib vs. Nivolumab
3. Discussion
4. Patients and Methods
4.1. Study Population
4.2. Treatment Regimens and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motzer, R.J.; Escudier, B.; Tomczak, P.; Hutson, T.E.; Michaelson, M.D.; Negrier, S.; Oudard, S.; Gore, M.E.; Tarazi, J.; Hariharan, S.; et al. Axitinib versus sorafenib as second-line treatment for advanced renal cell carcinoma: Overall survival analysis and updated results from a randomized phase 3 trial. Lancet Oncol. 2013, 14, 552–562. [Google Scholar] [CrossRef]
- Escudier, B.; Eisen, T.; Stadler, W.M.; Szczylik, C.; Oudard, S.; Siebels, M.; Negrier, S.; Chevreau, C.; Solska, E.; Desai, A.A.; et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 125–134. [Google Scholar] [CrossRef]
- Escudier, B.; Pluzanska, A.; Koralewski, P.; Ravaud, A.; Bracarda, S.; Szczylik, C.; Chevreau, C.; Filipek, M.; Melichar, B.; Bajetta, E.; et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: Arandomised, double-blind phase III trial. Lancet 2007, 370, 2103–2111. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef]
- Gore, M.E.; Szczylik, C.; Porta, C.; Bracarda, S.; Bjarnason, G.A.; Oudard, S.; Lee, S.H.; Haanen, J.; Castellano, D.; Vrdoljak, E.; et al. Final results from the large sunitinib global expanded-access trial in metastatic renal cell carcinoma. Br. J. Cancer 2015, 113, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Nosov, D.; Eisen, T.; Bondarenko, I.; Lesovoy, V.; Lipatov, O.; Tomczak, P.; Lyulko, O.; Alyasova, A.; Harza, M.; et al. Tivozanib versus sorafenib as initial targeted therapy for patients with metastatic renal cell carcinoma: Results from a phase III trial. J. Clin. Oncol. 2013, 31, 3791–3799. [Google Scholar] [CrossRef]
- Santoni, M.; Massari, F.; Piva, F.; Carrozza, F.; Di Nunno, V.; Cimadamore, A.; Martignetti, A.; Montironi, R.; Battelli, N. Tivozanib for the treatment of renal cell carcinoma. Expert Opin. Pharmacother. 2018, 19, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Di Nunno, V.; Cubelli, M.; Massari, F. The role of the MET/AXL pathway as a new target for multikinase inhibitors in renal cell carcinoma. Expert Rev. Precis. Med. Drug Dev. 2017, 2, 169–175. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Escudier, B.; Powles, T.; Mainwaring, P.N.; Rini, B.I.; Donskov, F.; Hammers, H.; Hutson, T.E.; Lee, J.L.; Peltola, K.; et al. Cabozantinib versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1814–1823. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Escudier, B.; Powles, T.; Tannir, N.M.; Mainwaring, P.N.; Rini, B.I.; Hammers, H.J.; Donskov, F.; Roth, B.J.; Peltola, K.; et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016, 17, 917–927. [Google Scholar] [CrossRef] [Green Version]
- Choueiri, T.K.; Halabi, S.; Sanford, B.L.; Hahn, O.; Michaelson, M.D.; Walsh, M.K.; Feldman, D.R.; Olencki, T.; Picus, J.; Small, E.J.; et al. Cabozantinib Versus Sunitinib as initial targeted therapy for patients with metastatic renal cell Carcinoma of poor or intermediate risk: The Alliance A031203 CABOSUN Trial. J. Clin. Oncol. 2017, 35, 591–597. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Hessel, C.; Halabi, S.; Sanford, B.; Michaelson, M.D.; Hahn, O.; Walsh, M.; Olencki, T.; Picus, J.; Small, E.J.; et al. Cabozantinib versus sunitinib as initial therapy for metastatic renal cell carcinoma of intermediate or poor risk (Alliance A031203 CABOSUN randomised trial): Progression-free survival by independent review and overall survival update. Eur. J. Cancer 2018, 94, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Buti, S.; Bersanelli, M. Is Cabozantinib Really Better Than Sunitinib As First-Line Treatment of Metastatic Renal Cell Carcinoma? J. Clin. Oncol. 2017, 35, 1858–1859. [Google Scholar] [CrossRef]
- Debeljak, N.; Solár, P.; Sytkowski, A.J. Erythropoietin and Cancer: The Unintended Consequences of Anemia Correction. Front. Immunol. 2014, 5, 563. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Nolley, R.; Chan, A.M.W.; Rankin, E.B.; Peehl, D.M. Cabozantinib inhibits tumor growth and metastasis of a patient-derived xenograft model of papillary renal cell carcinoma with MET mutation. Cancer Biol. Ther. 2017, 18, 863–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Features | N. of Patients (%) |
|---|---|
| Age | |
| Median | 62.56y |
| Range | 24.55–85.76y |
| Gender | |
| Male | 174 (73.42) |
| Female | 63 (26.58) |
| T-Stage at Diagnosis | |
| T1 | 37 (15.61) |
| T2 | 35 (14.77) |
| T3 | 97 (40.93) |
| T4 | 26 (10.97) |
| Unknown | 42 (17.72) |
| Histology | |
| Clear-cell RCC | 182 (76.79) |
| Non-clear-cell RCC | 55 (23.21) |
| Fuhrman or WHO/ISUP Grade | |
| Grade 1 | 4 (1.69) |
| Grade 2 | 62 (26.16) |
| Grade 3 | 86 (36.39) |
| Grade 4 | 32 (13.50) |
| Unknown | 59 (22.36) |
| N. of Metastatic Sites at Recurrence | |
| 1 site | 77 (32.49) |
| ≥2 sites | 160 (67.51) |
| Site of Metastasis | |
| Lung | 154 (64.98) |
| Lymph nodes | 133 (56.12) |
| Bone | 80 (34.04) |
| Liver | 53 (22.36) |
| Brain | 20 (8.44) |
| IMDC Risk Group | |
| Good | 57 (24.05) |
| Intermediate | 146 (61.60) |
| Poor | 34 (14.35) |
| First-Line Therapy | |
| Sunitinib | 141 (59.49) |
| Pazopanib | 81 (34.18) |
| Immunotherapy combinations | 9 (3.80) |
| Other | 6 (2.53) |
| Second-Line Therapy | 237 (100) |
| Cabozantinib | 112 (47.26) |
| Nivolumab | 89 (37.55) |
| Axitinib | 19 (8.01) |
| Everolimus | 14 (5.91) |
| Other | 3 (1.27) |
| Third-Line Therapy | 178 (100) |
| Cabozantinib | 125 (70.22) |
| Nivolumab | 29 (16.29) |
| Other | 24 (13.49) |
| IMDC Criteria | N of Patients (%) |
|---|---|
| <1 y from Diagnosis to Systemic Therapy | |
| Yes | 120 (50.63) |
| No | 117 (49.37) |
| Performance Status < 80% (Karnofsky) | |
| Yes | 19 (8.02) |
| No | 214 (91.98) |
| Hb Level < LLN | |
| Yes | 88 (37.13) |
| No | 149 (62.87) |
| Calcium Level > ULN | |
| Yes | 21 (8.86) |
| No | 216 (91.14) |
| Neutrophil > ULN | |
| Yes | 29 (12.24) |
| No | 208 (87.76) |
| Platelets > ULN | |
| Yes | 31 (13.08) |
| No | 206 (86.92) |
| Groups | Second-Line Cabozantinib | Third-Line Cabozantinib | ||
|---|---|---|---|---|
| All Patients | PFS [Median (95% CI)] | OS [Median (95% CI)] | PFS [Median (95% CI)] | OS [Median (95% CI)] |
| 7.76 (6.51–10.88) | 11.57 (10.90–NR) | 11.38 (5.79–NR) | NR (11.5–NR) | |
| Second-line Cabozantinib (29 patients, 25.9%) | Third-line Cabozantinib (28 patients, 22.4%) | |||
| Favourable Group | PFS [Median (95% CI)] | OS [Median (95% CI)] | PFS [Median (95% CI)] | OS [Median (95% CI)] |
| 11.28 (7.89–NR) | 12.53 (11.57–NR) | 11.38 (4.24–NR) | NR (7.40–NR) | |
| Second-line Cabozantinib (64 patients, 57.1%) | Third-line Cabozantinib (78 patients, 68.4%) | |||
| Intermediate Group | PFS [Median (95% CI)] | OS [Median (95% CI)] | PFS [Median (95% CI)] | OS [Median (95% CI)] |
| 7.59 (5.52–NR) | 10.95 (9.11–NR) | 7.63 (5.56–NR) | NR (11.51–NR) | |
| Second-line Cabozantinib (19 patients, 17.0%) | Third-line Cabozantinib (19 patients, 9.2%) | |||
| Poor-Risk Group | PFS [Median (95% CI)] | OS [Median (95% CI)] | PFS [Median (95% CI)] | OS [Median (95% CI)] |
| 7.13 (2.66–NR) | 11.05 (7.46–NR) | 5.75 (3.19–NR) | NR (4.01–NR) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoni, M.; Heng, D.Y.; Bracarda, S.; Procopio, G.; Milella, M.; Porta, C.; Matrana, M.R.; Cartenì, G.; Crabb, S.J.; De Giorgi, U.; et al. Real-World Data on Cabozantinib in Previously Treated Patients with Metastatic Renal Cell Carcinoma: Focus on Sequences and Prognostic Factors. Cancers 2020, 12, 84. https://doi.org/10.3390/cancers12010084
Santoni M, Heng DY, Bracarda S, Procopio G, Milella M, Porta C, Matrana MR, Cartenì G, Crabb SJ, De Giorgi U, et al. Real-World Data on Cabozantinib in Previously Treated Patients with Metastatic Renal Cell Carcinoma: Focus on Sequences and Prognostic Factors. Cancers. 2020; 12(1):84. https://doi.org/10.3390/cancers12010084
Chicago/Turabian StyleSantoni, Matteo, Daniel Y. Heng, Sergio Bracarda, Giuseppe Procopio, Michele Milella, Camillo Porta, Marc R. Matrana, Giacomo Cartenì, Simon J. Crabb, Ugo De Giorgi, and et al. 2020. "Real-World Data on Cabozantinib in Previously Treated Patients with Metastatic Renal Cell Carcinoma: Focus on Sequences and Prognostic Factors" Cancers 12, no. 1: 84. https://doi.org/10.3390/cancers12010084