Temporal Characterization of Blood–Brain Barrier Disruption with High-Frequency Electroporation

 , , , and
, , , and 
Abstract
:1. Introduction
2. Results
2.1. High-Frequency Electroporation BBBD Analysis
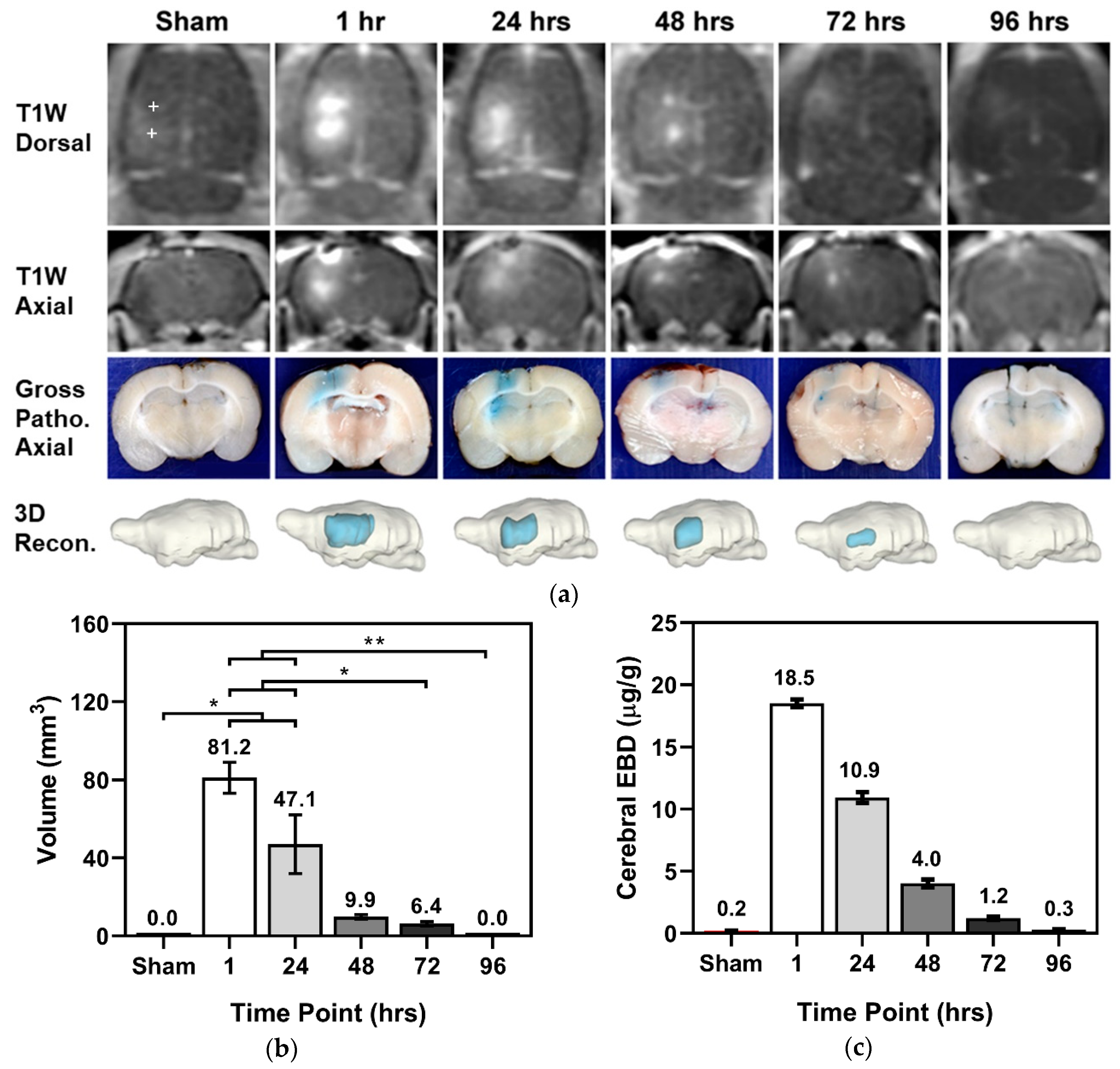
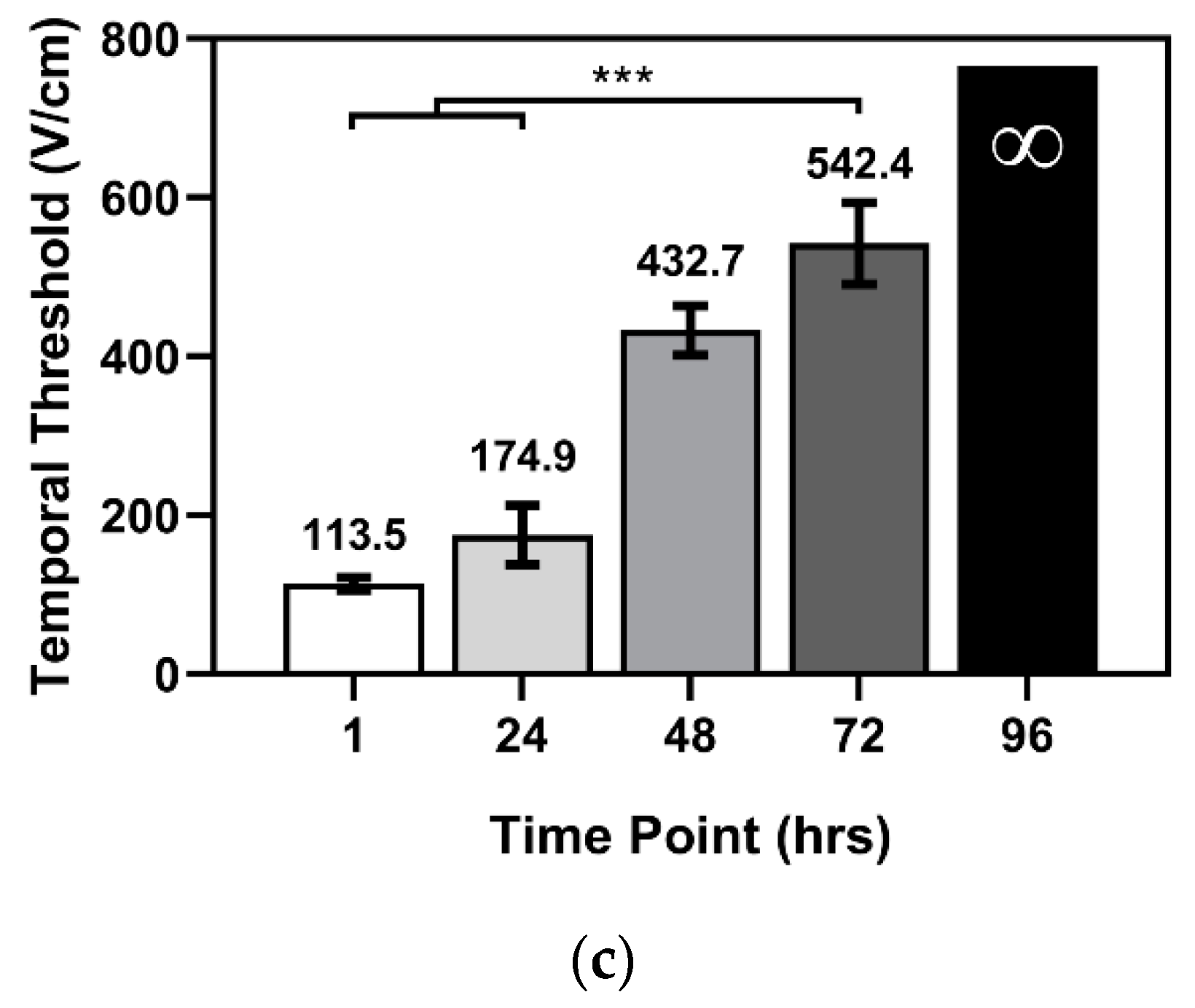
2.1.1. Temporal BBBD Characterization
2.1.2. BBBD with Varied V/d and Burst Number
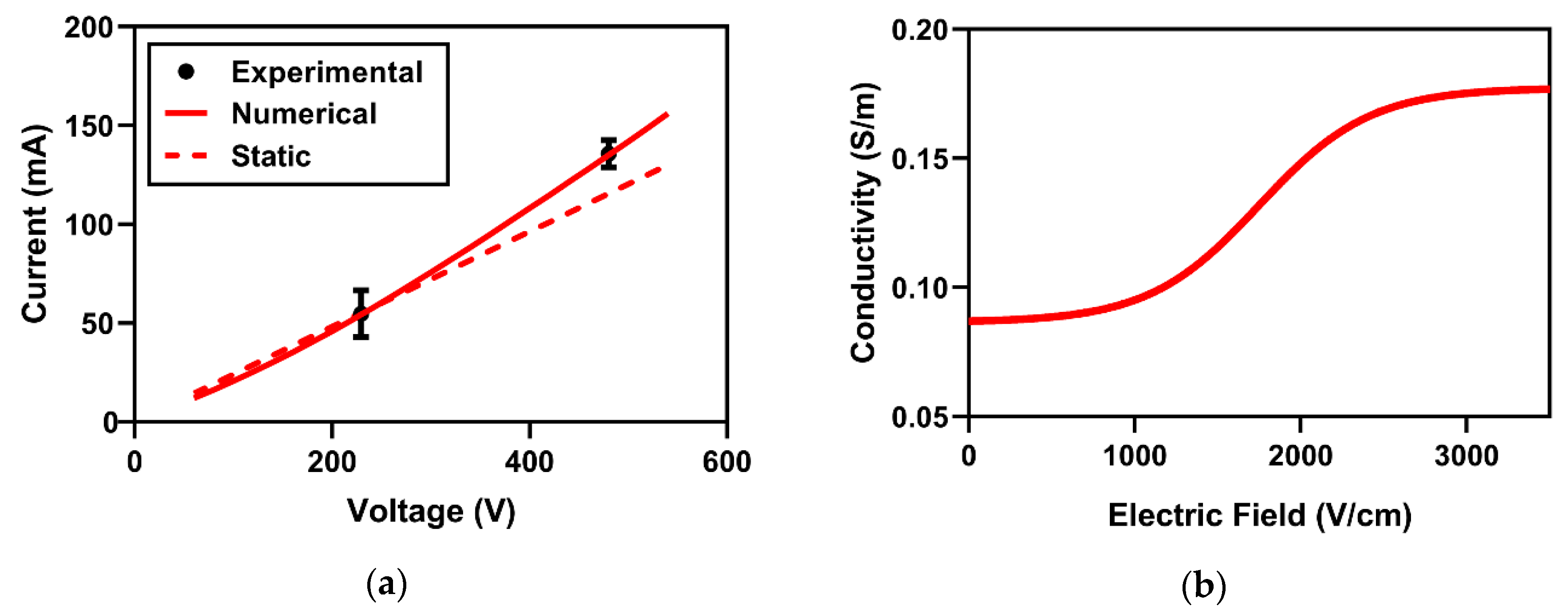
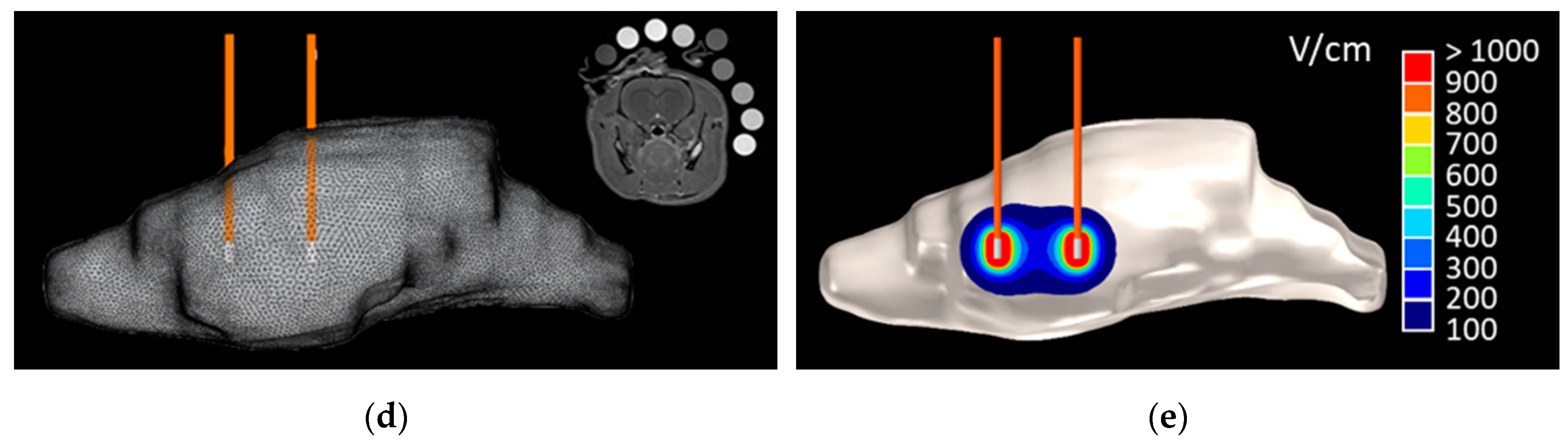
2.2. Numerical BBBD Analysis
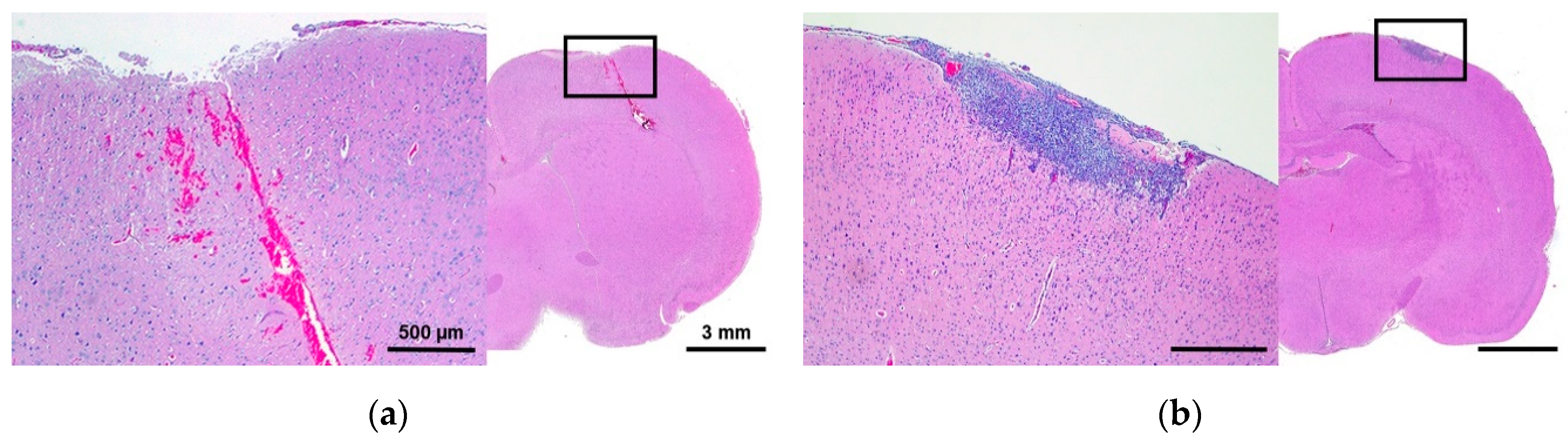
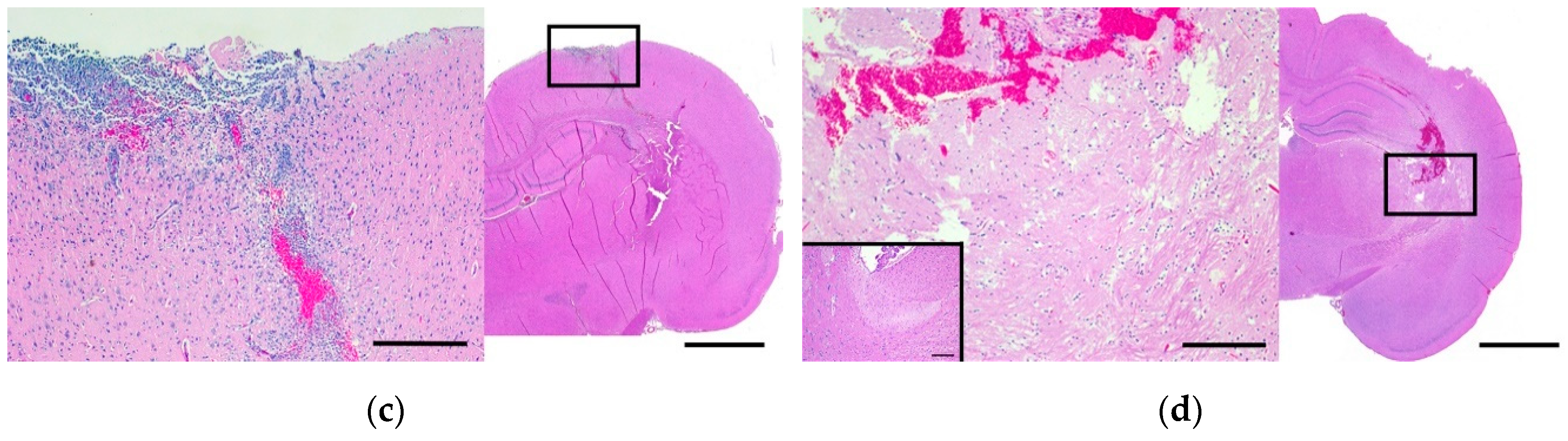
2.3. Histomorphologic Analyses
2.4. Secondary Electrical, Thermal, and Accelerometry Measurements
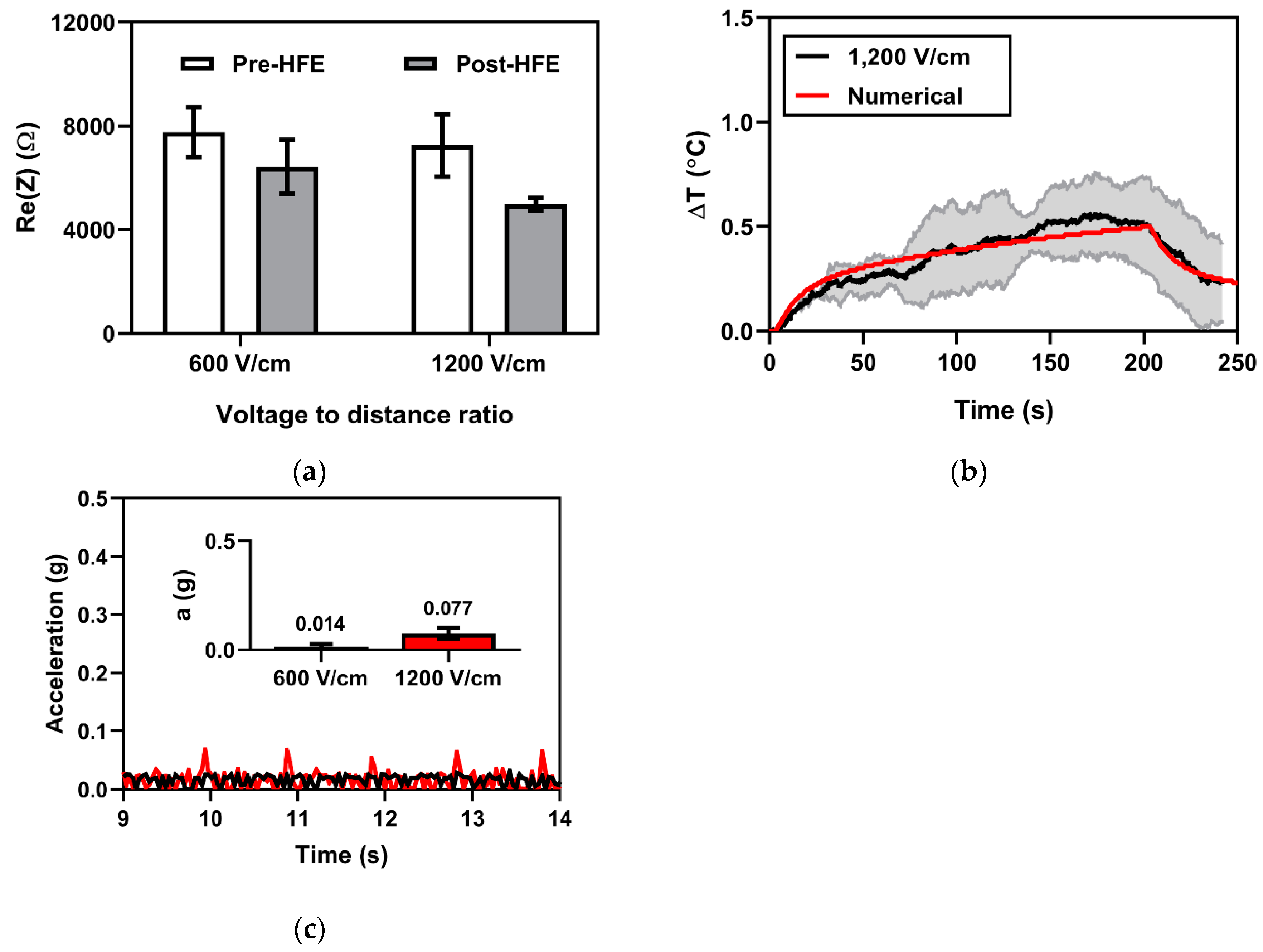
2.4.1. Electrical Impedance Spectroscopy for Monitoring Changes in Tissue Impedance
2.4.2. Fiber Optic Temperature Sensing for Monitoring Joule Heating Effects
2.4.3. Accelerometry Measurements for Muscle Excitation
3. Discussion
4. Materials and Methods
4.1. Assurances and Surgical Procedures
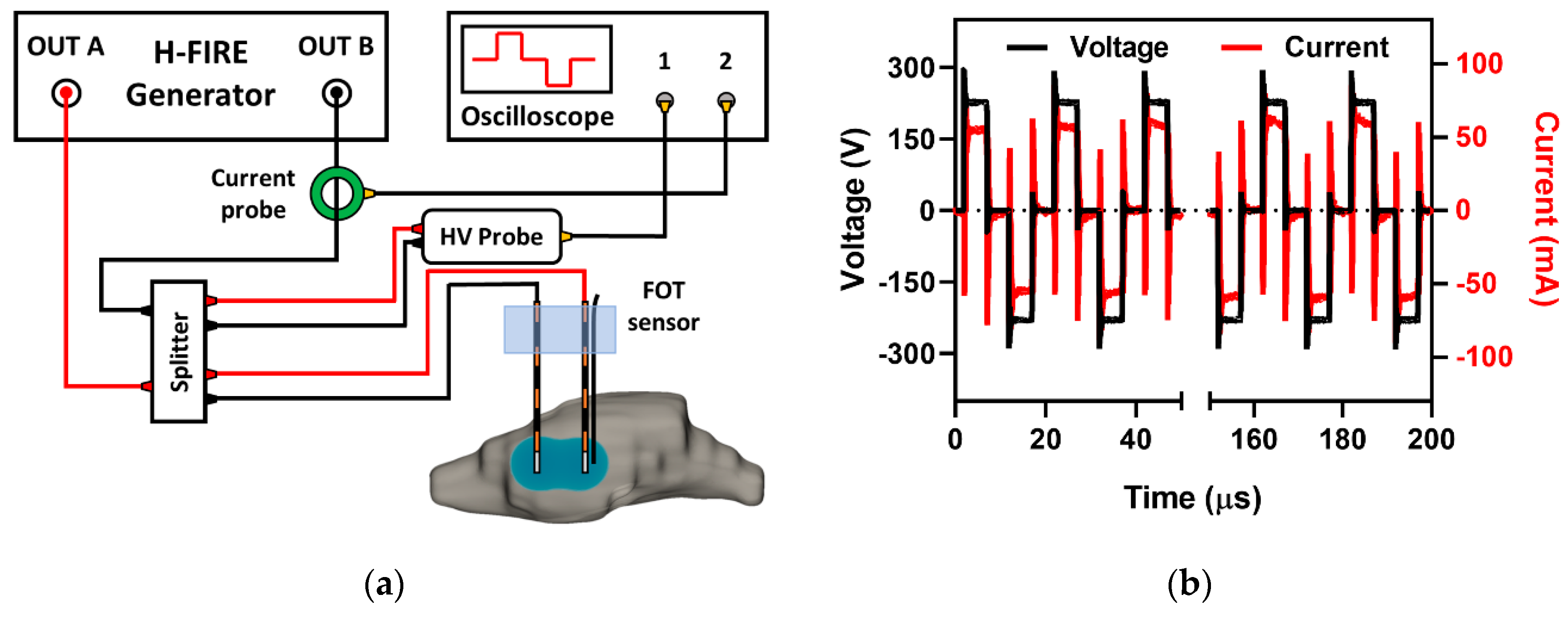
4.2. High-Frequency Electroporation and Parameter Selection
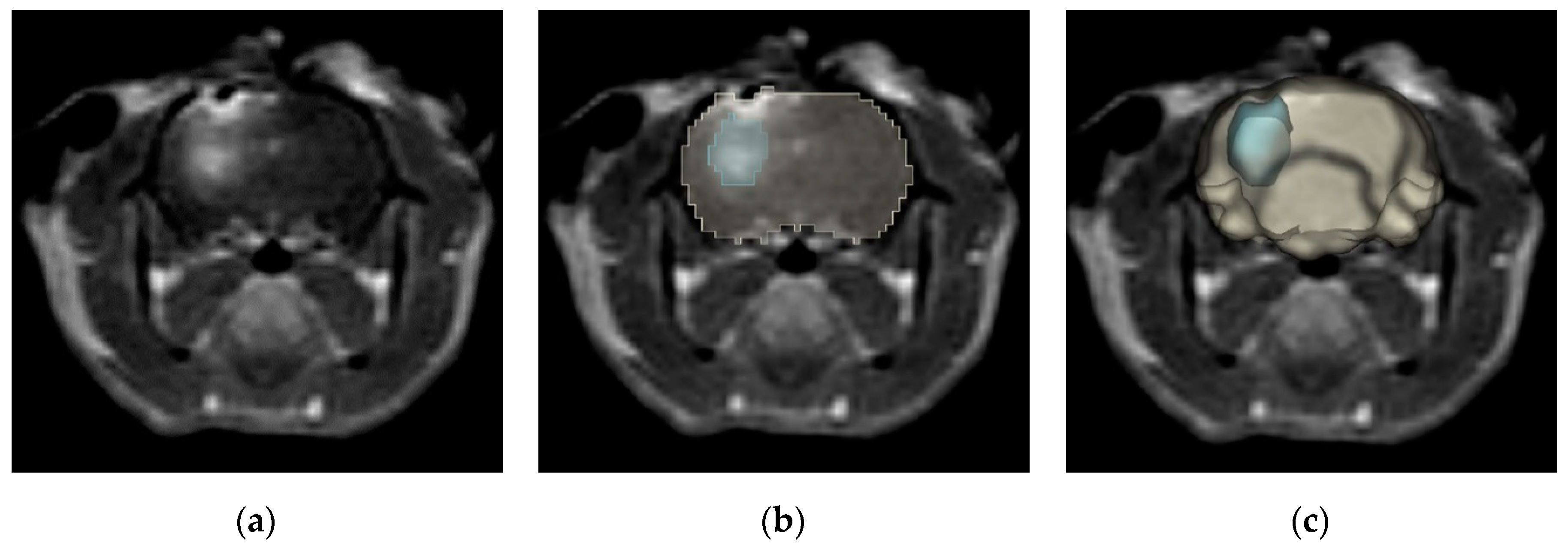
4.3. Magnetic Resonance Imaging and Gd-EBD BBB Disruption Volumetrics
4.4. Histomorphologic Analyses of Gd-EBD Treated Rodents
4.5. Quantification of Evans Blue Dye
4.6. Numerical Determination of BBBD Temporal Thresholds
4.7. Secondary Electrical, Thermal, and Accelerometry Measurements
4.7.1. Electrical Impedance Spectroscopy for Monitoring Changes in Tissue Impedance
4.7.2. Fiber Optic Temperature Sensing for Monitoring Joule Heating Effects
4.7.3. Accelerometry Measurements for Muscle Excitation
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abbott, N.J. Blood-brain barrier structure and function and the challenges for CNS drug delivery. J. Inherit. Metab. Dis. 2013, 36, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Banks, W.A. From blood-brain barrier to blood-brain interface: New opportunities for CNS drug delivery. Nat. Rev. Drug Discov. 2016, 15, 275–292. [Google Scholar] [CrossRef] [PubMed]
- Barar, J.; Rafi, M.A.; Pourseif, M.M.; Omidi, Y. Blood-brain barrier transport machineries and targeted therapy of brain diseases. Bioimpacts 2016, 6, 225–248. [Google Scholar] [CrossRef] [PubMed]
- Régina, A.; Demeule, M.; Laplante, A.; Jodoin, J.; Dagenais, C.; Berthelet, F.; Moghrabi, A.; Béliveau, R. Multidrug resistance in brain tumors: Roles of the blood–brain barrier. Cancer Metastasis Rev. 2001, 20, 13–25. [Google Scholar] [CrossRef]
- Sewing, A.C.P.; Caretti, V.; Lagerweij, T.; Schellen, P.; Jansen, M.H.; van Vuurden, D.G.; Idema, S.; Molthoff, C.F.; Vandertop, W.P.; Kaspers, G.J. Convection enhanced delivery of carmustine to the murine brainstem: A feasibility study. J. Neurosci. Methods 2014, 238, 88–94. [Google Scholar] [CrossRef]
- Ksendzovsky, A.; Walbridge, S.; Saunders, R.C.; Asthagiri, A.R.; Heiss, J.D.; Lonser, R.R. Convection-enhanced delivery of M13 bacteriophage to the brain. J. Neurosurg. 2012, 117, 197–203. [Google Scholar] [CrossRef]
- Patel, S.J.; Shapiro, W.R.; Laske, D.W.; Jensen, R.L.; Asher, A.L.; Wessels, B.W.; Carpenter, S.P.; Shan, J.S. Safety and feasibility of convection-enhanced delivery of Cotara for the treatment of malignant glioma: Initial experience in 51 patients. Neurosurgery 2005, 56, 1243–1252. [Google Scholar] [CrossRef]
- Lonser, R.R.; Sarntinoranont, M.; Morrison, P.F.; Oldfield, E.H. Convection-enhanced delivery to the central nervous system. J. Neurosurg. 2015, 122, 697–706. [Google Scholar] [CrossRef]
- Sheikov, N.; McDannold, N.; Sharma, S.; Hynynen, K. Effect of focused ultrasound applied with an ultrasound contrast agent on the tight junctional integrity of the brain microvascular endothelium. Ultrasound Med. Biol. 2008, 34, 1093–1104. [Google Scholar] [CrossRef]
- Aryal, M.; Arvanitis, C.D.; Alexander, P.M.; McDannold, N. Ultrasound-mediated blood-brain barrier disruption for targeted drug delivery in the central nervous system. Adv. Drug Deliv. Rev. 2014, 72, 94–109. [Google Scholar] [CrossRef]
- Bhutiani, N.; Philips, P.; Scoggins, C.R.; McMasters, K.M.; Potts, M.H.; Martin, R.C. Evaluation of tolerability and efficacy of irreversible electroporation (IRE) in treatment of Child-Pugh B (7/8) hepatocellular carcinoma (HCC). HPB 2016, 18, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Davalos, R.V.; Mir, I.L.; Rubinsky, B. Tissue ablation with irreversible electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Guenther, E.; Klein, N.; Zapf, S.; Weil, S.; Schlosser, C.; Rubinsky, B.; Stehling, M. Prostate cancer treatment with irreversible electroporation (IRE): Safety, efficacy and clinical experience in 471 treatments. PLoS ONE 2019, 14, e0215093. [Google Scholar] [CrossRef]
- Martin, R.C.G.; Kwon, D.; Chalikonda, S.; Sellers, M.; Kotz, E.; Scoggins, C.; McMasters, K.M.; Watkins, K. Treatment of 200 locally advanced (stage III) pancreatic adenocarcinoma patients with irreversible electroporation: Safety and efficacy. Ann. Surg. 2015, 262, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, G.; Hosein, P.J.; Arora, G.; Barbery, K.J.; Froud, T.; Livingstone, A.S.; Franceschi, D.; Rocha Lima, C.M.; Yrizarry, J. Percutaneous irreversible electroporation for downstaging and control of unresectable pancreatic adenocarcinoma. J. Vasc. Interv. Radiol. 2012, 23, 1613–1621. [Google Scholar] [CrossRef] [PubMed]
- Neal, R.E., III; Rossmeisl, J.H., Jr.; Garcia, P.A.; Lanz, O.I.; Henao-Guerrero, N.; Davalos, R.V. Successful treatment of a large soft tissue sarcoma with irreversible electroporation. J. Clin. Oncol. 2011, 29, e372–e377. [Google Scholar] [CrossRef]
- Rubinsky, B.; Onik, G.; Mikus, P. Irreversible electroporation: A new ablation modality—Clinical implications. Technol. Cancer Res. Treat. 2007, 6, 37–48. [Google Scholar] [CrossRef]
- Garcia, P.A.; Davalos, R.V.; Miklavcic, D. A numerical investigation of the electric and thermal cell kill distributions in electroporation-based therapies in tissue. PLoS ONE 2014, 9, e103083. [Google Scholar] [CrossRef]
- Kos, B.; Voigt, P.; Miklavcic, D.; Moche, M. Careful treatment planning enables safe ablation of liver tumors adjacent to major blood vessels by percutaneous irreversible electroporation (IRE). Radiol. Oncol. 2015, 49, 234–241. [Google Scholar] [CrossRef]
- Latouche, E.L.; Sano, M.B.; Lorenzo, M.F.; Davalos, R.V.; Martin, R.C.G., 2nd. Irreversible electroporation for the ablation of pancreatic malignancies: A patient-specific methodology. J. Surg. Oncol. 2017, 115, 711–717. [Google Scholar] [CrossRef]
- Li, W.; Fan, Q.; Ji, Z.; Qiu, X.; Li, Z. The effects of irreversible electroporation (IRE) on nerves. PLoS ONE 2011, 6, e18831. [Google Scholar] [CrossRef] [PubMed]
- Maor, E.; Ivorra, A.; Leor, J.; Rubinsky, B. The effect of irreversible electroporation on blood vessels. Technol. Cancer Res. Treat. 2007, 6, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.A.; Rossmeisl, J.H., Jr.; Neal, R.E., II; Ellis, T.L.; Olson, J.D.; Henao-Guerrero, N.; Robertson, J.; Davalos, R.V. Intracranial nonthermal irreversible electroporation: In vivo analysis. J. Membr. Biol. 2010, 236, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.; Pancotto, T.; Rossmeisl, J.H., Jr.; Henao-Guerrero, N.; Gustafson, N.; Daniel, G.; Robertson, J.; Ellis, T.; Davalos, R. Non-thermal irreversible electroporation (N-TIRE) and adjuvant fractionated radiotherapeutic multimodal therapy for intracranial malignant glioma in a canine patient. Technol. Cancer Res. Treat. 2011, 10, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.A.; Kos, B.; Rossmeisl, J.H., Jr.; Pavliha, D.; Miklavcic, D.; Davalos, R.V. Predictive therapeutic planning for irreversible electroporation treatment of spontaneous malignant glioma. Med. Phys. 2017, 44, 4968–4980. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.A.; Rossmeisl, J.H., Jr.; Robertson, J.L.; Olson, J.D.; Johnson, A.J.; Ellis, T.L.; Davalos, R.V. 7.0-T magnetic resonance imaging characterization of acute blood-brain-barrier disruption achieved with intracranial irreversible electroporation. PLoS ONE 2012, 7, e50482. [Google Scholar] [CrossRef]
- Sharabi, S.; Last, D.; Guez, D.; Daniels, D.; Hjouj, M.I.; Salomon, S.; Maor, E.; Mardor, Y. Dynamic effects of point source electroporation on the rat brain tissue. Bioelectrochemistry 2014, 99, 30–39. [Google Scholar] [CrossRef]
- Hjouj, M.; Last, D.; Guez, D.; Daniels, D.; Sharabi, S.; Lavee, J.; Rubinsky, B.; Mardor, Y. MRI study on reversible and irreversible electroporation induced blood brain barrier disruption. PLoS ONE 2012, 7, e42817. [Google Scholar] [CrossRef]
- Sharabi, S.; Kos, B.; Last, D.; Guez, D.; Daniels, D.; Harnof, S.; Mardor, Y.; Miklavcic, D. A statistical model describing combined irreversible electroporation and electroporation-induced blood-brain barrier disruption. Radiol. Oncol. 2016, 50, 28–38. [Google Scholar] [CrossRef]
- Bonakdar, M.; Graybill, P.M.; Davalos, R.V. A microfluidic model of the blood-brain barrier to study permeabilization by pulsed electric fields. RSC Adv. 2017, 7, 42811–42818. [Google Scholar] [CrossRef]
- Sharabi, S.; Bresler, Y.; Ravid, O.; Shemesh, C.; Atrakchi, D.; Schnaider-Beeri, M.; Gosselet, F.; Dehouck, L.; Last, D.; Guez, D.; et al. Transient blood-brain barrier disruption is induced by low pulsed electrical fields in vitro: An analysis of permeability and trans-endothelial electric resistivity. Drug Deliv. 2019, 26, 459–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, C.B.; Sano, M.B.; Rossmeisl, J.H., Jr.; Caldwell, J.L.; Garcia, P.A.; Rylander, M.N.; Davalos, R.V. High-frequency irreversible electroporation (H-FIRE) for non-thermal ablation without muscle contraction. Biomed. Eng. Online 2011, 10, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, C.B.; Sano, M.B.; Rylander, M.N.; Davalos, R.V. Theoretical considerations of tissue electroporation with high-frequency bipolar pulses. IEEE Trans. Biomed. Eng. 2011, 58, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, T.J.; Passeri, M.; Lorenzo, M.F.; Sulzer, J.K.; Lyman, W.B.; Swet, J.H.; Vrochides, D.; Baker, E.H.; Iannitti, D.A.; Davalos, R.V.; et al. Experimental high-frequency irreversible electroporation using a single-needle delivery approach for nonthermal pancreatic ablation in vivo. J. Vasc. Interv. Radiol. 2019, 30, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Latouche, E.L.; Arena, C.B.; Ivey, J.W.; Garcia, P.A.; Pancotto, T.E.; Pavlisko, N.; Verbridge, S.S.; Davalos, R.V.; Rossmeisl, J.H. High-frequency irreversible electroporation for intracranial meningioma: A feasibility study in a spontaneous canine tumor model. Technol. Cancer Res. Treat. 2018, 17. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, I.A.; Latouche, E.L.; DeWitt, M.R.; Swet, J.H.; Kirks, R.C.; Baker, E.H.; Iannitti, D.A.; Vrochides, D.; Davalos, R.V.; McKillop, I.H. Induction of rapid, reproducible hepatic ablations using next-generation, high frequency irreversible electroporation (H-FIRE) in vivo. HPB 2016, 18, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Ivey, J.W.; Bonakdar, M.; Kanitkar, A.; Davalos, R.V.; Verbridge, S.S. Improving cancer therapies by targeting the physical and chemical hallmarks of the tumor microenvironment. Cancer Lett. 2016, 380, 330–339. [Google Scholar] [CrossRef] [Green Version]
- Ivey, J.W.; Latouche, E.L.; Sano, M.B.; Rossmeisl, J.H.; Davalos, R.V.; Verbridge, S.S. Targeted cellular ablation based on the morphology of malignant cells. Sci. Rep. 2015, 5, 17157. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Bhonsle, S.; Dong, S.; Lv, Y.; Liu, H.; Safaai-Jazi, A.; Davalos, R.V.; Yao, C. Characterization of conductivity changes during high-frequency irreversible electroporation for treatment planning. IEEE Trans. Biomed. Eng. 2018, 65, 1810–1819. [Google Scholar] [CrossRef]
- Bhonsle, S.; Lorenzo, M.F.; Safaai-Jazi, A.; Davalos, R.V. Characterization of nonlinearity and dispersion in tissue impedance during high-frequency electroporation. IEEE Trans. Biomed. Eng. 2018, 65, 2190–2201. [Google Scholar] [CrossRef]
- Bhonsle, S.P.; Arena, C.B.; Sweeney, D.C.; Davalos, R.V. Mitigation of impedance changes due to electroporation therapy using bursts of high-frequency bipolar pulses. Biomed. Eng. Online 2015, 14, S3. [Google Scholar] [CrossRef] [Green Version]
- Murovec, T.; Sweeney, D.C.; Latouche, E.; Davalos, R.V.; Brosseau, C. Modeling of transmembrane potential in realistic multicellular structures before electroporation. Biophys. J. 2016, 111, 2286–2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, C.B.; Garcia, P.A.; Sano, M.B.; Olson, J.D.; Rogers-Cotrone, T.; Rossmeisl, J.H.; Davalos, R.V. Focal blood-brain-barrier disruption with high-frequency pulsed electric fields. Technology 2014, 2, 206–213. [Google Scholar] [CrossRef]
- Kovacs, Z.I.; Kim, S.; Jikaria, N.; Qureshi, F.; Milo, B.; Lewis, B.K.; Bresler, M.; Burks, S.R.; Frank, J.A. Disrupting the blood-brain barrier by focused ultrasound induces sterile inflammation. Proc. Natl. Acad. Sci. USA 2017, 114, E75–E84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDannold, N.; Vykhodtseva, N.; Jolesz, F.A.; Hynynen, K. MRI investigation of the threshold for thermally induced blood-brain barrier disruption and brain tissue damage in the rabbit brain. Magn. Reason. Med. 2004, 51, 913–923. [Google Scholar] [CrossRef] [PubMed]
- Yung, J.P.; Shetty, A.; Elliott, A.; Weinberg, J.S.; McNichols, R.J.; Gowda, A.; Hazle, J.D.; Stafford, R.J. Quantitative comparison of thermal dose models in normal canine brain. Med. Phys. 2010, 37, 5313–5321. [Google Scholar] [CrossRef] [PubMed]
- Rogers, W.R.; Merritt, J.H.; Comeaux, J.A.; Kuhnel, C.T.; Moreland, D.F.; Teltschik, D.G.; Lucas, J.H.; Murphy, M.R. Strength-duration curve for an electrically excitable tissue extended down to near 1 nanosecond. IEEE Trans. Plasma Sci. 2004, 32, 1587–1599. [Google Scholar] [CrossRef]
- Sano, M.B.; Arena, C.B.; Bittleman, K.R.; DeWitt, M.R.; Cho, H.J.; Szot, C.S.; Saur, D.; Cissell, J.M.; Robertson, J.; Lee, Y.W.; et al. Bursts of Bipolar Microsecond Pulses Inhibit Tumor Growth. Sci Rep. 2015, 5, 14999. [Google Scholar] [CrossRef] [Green Version]
- Ivey, J.W.; Wasson, E.M.; Alinezhadbalalami, N.; Kanitkar, A.; Debinski, W.; Sheng, Z.; Davalos, R.V.; Verbridge, S.S. Characterization of ablation thresholds for 3D-cultured patient-derived glioma stem cells in response to high-frequency irreversible electroporation. Research 2019, 2019, 8081315. [Google Scholar] [CrossRef] [Green Version]
- Sano, M.B.; Arena, C.B.; DeWitt, M.R.; Saur, D.; Davalos, R.V. In-vitro bipolar nano- and microsecond electro-pulse bursts for irreversible electroporation therapies. Bioelectrochemistry 2014, 100, 69–79. [Google Scholar] [CrossRef]
- Mercadal, B.; Arena, C.B.; Davalos, R.V.; Ivorra, A. Avoiding nerve stimulation in irreversible electroporation: A numerical modeling study. Phys. Med. Biol. 2017, 62, 8060–8079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golberg, A.; Rubinsky, B. Towards electroporation based treatment planning considering electric field induced muscle contractions. Technol. Cancer Res. Treat. 2012, 11, 189–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toda, N.; Tanaka, T.; Ayajiki, K.; Okamura, T. Cerebral vasodilatation induced by stimulation of the pterygopalatine ganglion and greater petrosal nerve in anesthetized monkeys. Neuroscience 2000, 96, 393–398. [Google Scholar] [CrossRef]
- Dunki-Jacobs, E.M.; Philips, P.; Martin II, R.C. Evaluation of resistance as a measure of successful tumor ablation during irreversible electroporation of the pancreas. J. Am. Coll. Surg. 2014, 218, 179–187. [Google Scholar] [CrossRef]
- Ivorra, A.; Al-Sakere, B.; Rubinsky, B.; Mir, L.M. In vivo electrical conductivity measurements during and after tumor electroporation: Conductivity changes reflect the treatment outcome. Phys. Med. Biol. 2009, 54, 5949–5963. [Google Scholar] [CrossRef]
- Wasson, E.M.; Alinezhadbalalami, N.; Brock, R.M.; Allen, I.C.; Verbridge, S.S.; Davalos, R.V. Understanding the role of calcium-mediated cell death in high-frequency irreversible electroporation. Bioelectrochemistry 2020, 131, 107369. [Google Scholar] [CrossRef]
- Shao, Q.; O’Flanagan, S.; Lam, T.; Roy, P.; Pelaez, F.; Burbach, B.J.; Azarin, S.M.; Shimizu, Y.; Bischof, J.C. Engineering T cell response to cancer antigens by choice of focal therapeutic conditions. Int. J. Hyperth. 2019, 36, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Ringel-Scaia, V.M.; Beitel-White, N.; Lorenzo, M.F.; Brock, R.M.; Huie, K.E.; Coutermarsh-Ott, S.; Eden, K.; McDaniel, D.K.; Verbridge, S.S.; Rossmeisl Jr, J.H.; et al. High-frequency irreversible electroporation is an effective tumor ablation strategy that induces immunologic cell death and promotes systemic anti-tumor immunity. EBioMedicine 2019, 44, 112–125. [Google Scholar] [CrossRef] [Green Version]
- Redondo, L.M.; Zahyka, M.; Kandratsyeu, A. Solid-state generation of high-frequency burst of bipolar pulses for medical applications. IEEE Trans. Plasma Sci. 2019, 47, 4091–4095. [Google Scholar] [CrossRef]
- Butt, M.T. Morphologic changes associated with intrathecal catheters for direct delivery to the central nervous system in preclinical studies. Toxicol. Pathol. 2011, 39, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Uyama, O.; Okamura, N.; Yanase, M.; Narita, M.; Kawabata, K.; Sugita, M. Quantitative evaluation of vascular permeability in the gerbil brain after transient ischemia using Evans blue fluorescence. J. Cereb. Blood Flow Metab. 1988, 8, 282–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the quantitative imaging network. Magn. Reason. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sel, D.; Cukjati, D.; Batiuskaite, D.; Slivnik, T.; Mir, L.M.; Miklavcic, D. Sequential finite element model of tissue electropermeabilization. IEEE Trans. Biomed. Eng. 2005, 52, 816–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Temporal (h) | Pathological BBBDV (mm3) | MRI BBBDV (mm3) | Cerebral [EBD] (µg/g) | Serum [EBD] (µg/g) | BBBD Temporal Threshold (V/cm) |
|---|---|---|---|---|---|
| sham | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.2 ± 0.0 | 1494.0 ± 0.0 | ∞ |
| 1 | 81.2 ± 7.9 * | 84.1 ± 8.7 * | 18.5 ± 0.29 | 1318.3 ± 66.8 | 113.5 ± 8.2 |
| 24 | 47.1 ± 15.1 * | 40.9 ± 5.4 | 10.9 ± 0.45 | 1393.8 ± 122.0 | 174.9 ± 37.1 |
| 48 | 9.9 ± 1.1 | 10.4 ± 1.1 | 4.0 ± 0.31 | 1404.0 ± 115.1 | 432.7 ± 30.8 |
| 72 | 6.4 ± 1.1 | 5.8 ± 1.0 | 1.2 ± 0.13 | 1403.3 ± 145.1 | 542.5 ± 51.5 |
| 96 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.3 ± 0.04 | 1400.5 ± 107.5 | ∞ |
| Category | Survival (h) | Grade 1 | Grade 2 | Grade 2a | Grade 2b | Grade 3a | Grade 4 |
|---|---|---|---|---|---|---|---|
| sham | sham, n = 2 | 2 | 0 | 0 | 0 | 0 | 0 |
| Immediate response | Burst100, n = 2 | 2 | 0 | 0 | 0 | 0 | 0 |
| 1, n = 2 | 2 | 0 | 0 | 0 | 0 | 0 | |
| 24, n = 4 | 4 | 0 | 0 | 0 | 0 | 0 | |
| 48, n = 4 | 4 | 0 | 0 | 0 | 0 | 0 | |
| Delayed response | 72, n = 4 | 1 | 1 | 2 | 0 | 0 | 0 |
| 96, n = 4 | 0 | 0 | 2 | 2 | 0 | 0 | |
| H-FIRE | H-FIRE, n = 2 | 0 | 0 | 0 | 0 | 1 | 1 |
| Group | Time-Point (h) | Voltage/Distance Ratio (V/cm) | Number of Bursts |
|---|---|---|---|
| sham § | 1 | 0 | 0 |
| 1 * | 1 | 600 | 200 |
| 2 † | 24 | 600 | 200 |
| 3 † | 48 | 600 | 200 |
| 4 † | 72 | 600 | 200 |
| 5 * | 96 | 600 | 200 |
| 6, H-FIRE * | 1 | 1200 | 200 |
| 7, Burst100 * | 1 | 600 | 100 |
| Score | Criteria: Brain Parenchyma Changes |
|---|---|
| 0 | No lesions apparent |
| 1 | Superficial cerebral contusion, edema, electrode tracks, +/- hemorrhage; lesions limited to electrode tracks |
| 2 | Superficial cerebral contusion, edema, electrode tracks, +/- hemorrhage, inflammation; lesions limited to electrode tracks |
| 3 | Parenchymal hemorrhagic necrosis/ablation localized to electrode tracks/tips |
| 4 | Regional parenchymal hemorrhagic necrosis/ablation (necrosis around and remote from needle tracks) |
| Criteria: Meningeal Changes * | |
| a | Mild meningeal inflammatory infiltrates; limited locally to electrode insertion areas |
| b | Moderate meningeal inflammatory infiltrates; meningeal involvement throughout surgical site |
| c | Severe meningeal inflammatory infiltrates; diffuse meningitis extending beyond surgical field |
| Material | Parameter | Value | Units |
|---|---|---|---|
| Brain tissue | Density, ρ | 1046 | kg/m3 |
| Specific heat, c | 3630 | J/(kg∙K) | |
| Thermal conductivity, k | 0.51 | W/(m∙K) | |
| Blood perfusion coefficient, ω | 1.75 × 10−3 | 1/s | |
| Insulation | Density, ρ | 1190 | kg/m3 |
| Specific heat, c | 1470 | J/(kg∙K) | |
| Thermal conductivity, k | 0.18 | W/(m∙K) | |
| Electrical conductivity, σ | 2.5 × 1014 | S/m | |
| Stainless steel | Density, ρ | 7850 | kg/m3 |
| Specific heat, c | 475 | J/(kg∙K) | |
| Thermal conductivity, k | 44.5 | W/(m∙K) | |
| Electrical conductivity, σ | 4.0 × 1014 | S/m |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenzo, M.F.; Thomas, S.C.; Kani, Y.; Hinckley, J.; Lee, M.; Adler, J.; Verbridge, S.S.; Hsu, F.-C.; Robertson, J.L.; Davalos, R.V.; et al. Temporal Characterization of Blood–Brain Barrier Disruption with High-Frequency Electroporation. Cancers 2019, 11, 1850. https://doi.org/10.3390/cancers11121850
Lorenzo MF, Thomas SC, Kani Y, Hinckley J, Lee M, Adler J, Verbridge SS, Hsu F-C, Robertson JL, Davalos RV, et al. Temporal Characterization of Blood–Brain Barrier Disruption with High-Frequency Electroporation. Cancers. 2019; 11(12):1850. https://doi.org/10.3390/cancers11121850
Chicago/Turabian StyleLorenzo, Melvin F., Sean C. Thomas, Yukitaka Kani, Jonathan Hinckley, Matthew Lee, Joy Adler, Scott S. Verbridge, Fang-Chi Hsu, John L. Robertson, Rafael V. Davalos, and et al. 2019. "Temporal Characterization of Blood–Brain Barrier Disruption with High-Frequency Electroporation" Cancers 11, no. 12: 1850. https://doi.org/10.3390/cancers11121850