Personalizing the Prediction of Colorectal Cancer Prognosis by Incorporating Comorbidities and Functional Status into Prognostic Nomograms

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. Inclusion Criteria
2.3. Ascertainment of Comorbidities and Functional Status
2.4. Selection of Variables
2.5. Outcomes
2.6. Model Construction
2.7. Model Validation
2.8. Net Benefit of Adding Comorbidity and Functional Status to the Nomograms
3. Results
3.1. Characteristics of the Study Participants
3.2. Association of Patient and Tumor Characteristics with Survival Outcomes
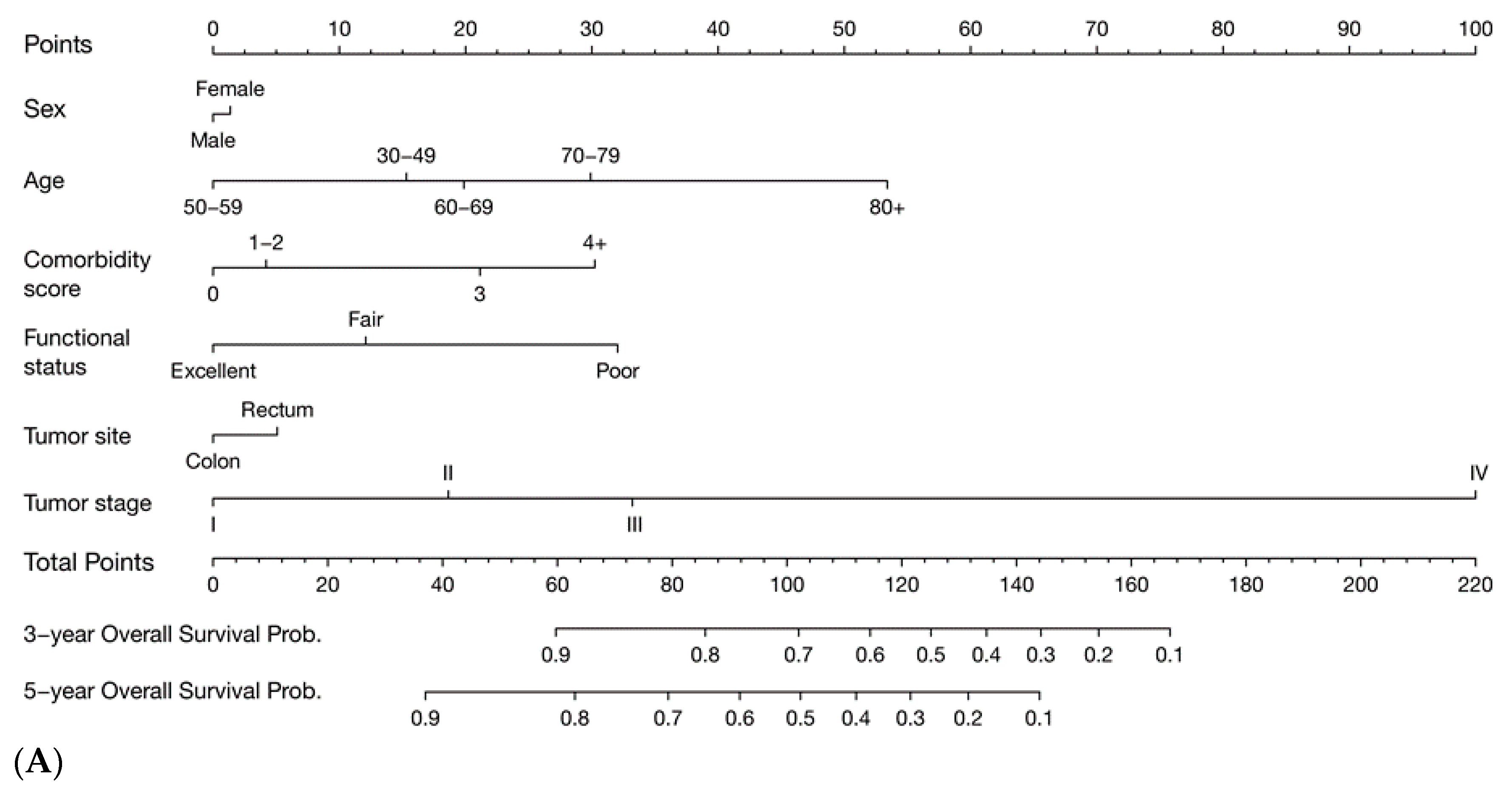
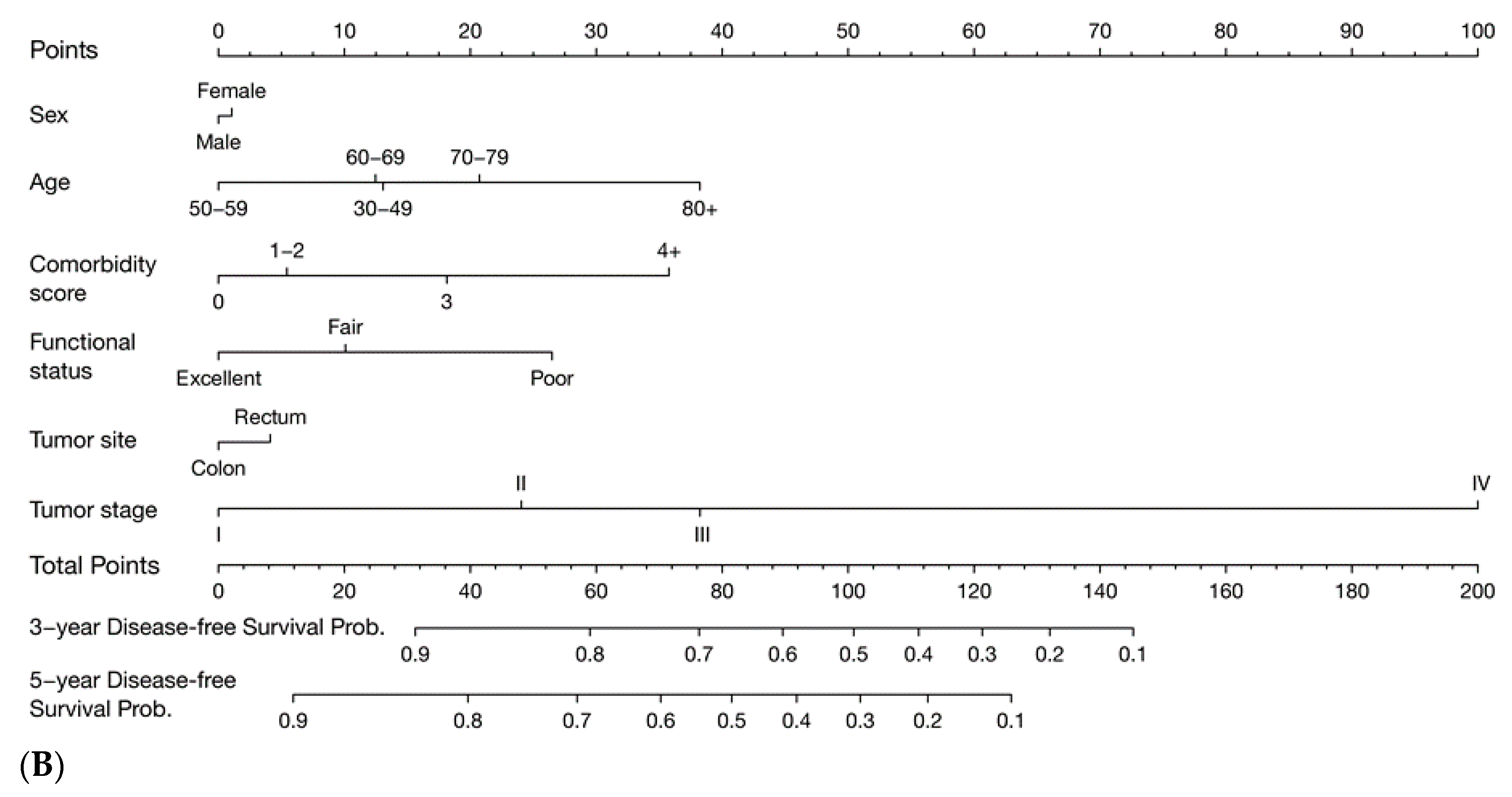
3.3. Prognostic Nomograms
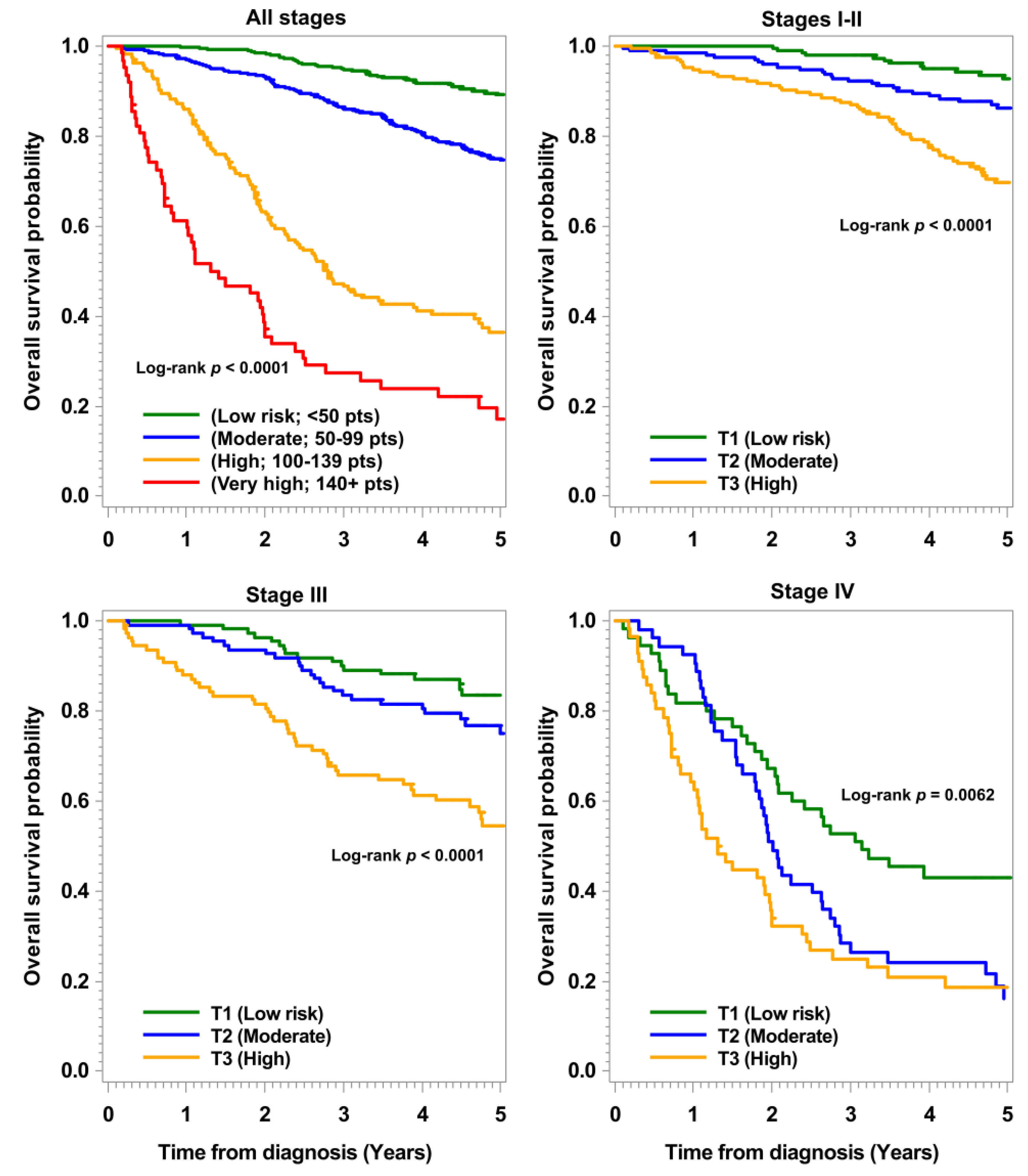
3.4. Validation of Nomograms
3.5. NRI of Adding Comorbidity and Functional Status to the Nomograms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Ouakrim, D.A.; Pizot, C.; Boniol, M.; Malvezzi, M.; Boniol, E.; Negri, M.; Bota, M.; Jenkins, A.; Bleiberg, H.; Autier, P. Trends in Colorectal Cancer Mortality in Europe: Retrospective Analysis of the WHO Mortality Database. BMJ 2015, 351, h4970. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; John Wiley & Sons: West Sussex, UK, 2009. [Google Scholar]
- Weiser, M.R.; Landmann, R.G.; Kattan, M.W.; Gonen, M.; Shia, I.; Chou, J.; Paty, P.B.; Guillem, J.G.; Temple, L.K.; Schrag, D.; et al. Individualized Prediction of Colon Cancer Recurrence Using a Nomogram. J. Clin. Oncol. 2008, 26, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Loprinzi, C.; Kennecke, H.; Grothey, A.; Nelson, G.; Woods, R.; Speers, C.; Alberts, S.R.; Bardia, A.; O’Connell, M.J.; et al. Prognostic Web-Based Models for Stage II and III Colon Cancer: A Population and Clinical Trials-Based Validation of Numeracy and Adjuvant! Online. Cancer 2011, 117, 4155–4165. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.R.; Gönen, M.; Chou, J.F.; Kattan, M.W.; Schrag, D. Predicting Survival after Curative Colectomy for Cancer: Individualizing Colon Cancer Staging. J. Clin. Oncol. 2011, 29, 4796–4802. [Google Scholar] [CrossRef]
- Renfro, L.A.; Grothey, A.; Xue, Y.; Saltz, L.B.; Andre, T.; Twelves, C.; Labianca, R.; Allegra, C.J.; Alberts, S.R.; Loprinzi, C.L.; et al. Accent-Based Web Calculators to Predict Recurrence and Overall Survival in Stage III Colon Cancer. J. Natl. Cancer Inst. 2014, 106, dju333. [Google Scholar] [CrossRef]
- Van Gijn, W.; van Stiphout, R.G.; van de Velde, C.J.; Valentini, V.; Lammering, G.; Gambacorta, M.A.; Pahlman, L.; Bujko, K.; Lambin, P. Nomograms to Predict Survival and the Risk for Developing Local or Distant Recurrence in Patients with Rectal Cancer Treated with Optional Short-Term Radiotherapy. Ann. Oncol. 2015, 26, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W.Y.; Renfro, L.A.; Kerr, D.; de Gramont, A.; Saltz, L.B.; Grothey, A.; Alberts, S.R.; Andre, T.; Guthrie, K.A.; Labianca, R.; et al. Determinants of Early Mortality among 37,568 Patients with Colon Cancer Who Participated in 25 Clinical Trials from the Adjuvant Colon Cancer Endpoints Database. J. Clin. Oncol. 2016, 34, 1182–1189. [Google Scholar] [CrossRef]
- Zhang, Z.; Gao, W.; Luo, Q.; Yin, X.; Basnet, S.; Dai, Z.; Ge, H. A Nomogram Improves AJCC Stages for Colorectal Cancers by Introducing Cea, Modified Lymph Node Ratio and Negative Lymph Node Count. Sci. Rep. 2016, 6, 39028. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Luo, Q.; Yin, X.; Dai, Z.; Basnet, S.; Ge, H. Nomograms to Predict Survival after Colorectal Cancer Resection without Preoperative Therapy. BMC Cancer 2016, 16, 658. [Google Scholar] [CrossRef] [PubMed]
- Sjoquist, K.M.; Renfro, L.A.; Simes, R.J.; Tebbutt, N.C.; Clarke, S.; Seymour, M.T.; Adams, R.; Maughan, T.S.; Saltz, L.; Goldberg, R.M.; et al. Personalizing Survival Predictions in Advanced Colorectal Cancer: The Arcad Nomogram Project. J. Natl. Cancer Inst. 2018, 110, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Nozawa, H.; Hata, K.; Kiyomatsu, T.; Tanaka, T.; Nishikawa, T.; Sugihara, K.; Watanabe, T. Nomogram Predicting Survival after Recurrence in Patients with Stage I to III Colon Cancer: A Nationwide Multicenter Study. Dis. Colon Rectum. 2018, 61, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Coupland, C. Development and Validation of Risk Prediction Equations to Estimate Survival in Patients with Colorectal Cancer: Cohort Study. BMJ 2017, 357, j2497. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Chang-Claude, J.; Jansen, L.; Knebel, P.; Stock, C.; Hoffmeister, M. Reduced Risk of Colorectal Cancer up to 10 Years after Screening, Surveillance, or Diagnostic Colonoscopy. Gastroenterology 2014, 146, 709–717. [Google Scholar] [CrossRef]
- Hoffmeister, M.; Jansen, L.; Rudolph, A.; Toth, C.; Kloor, M.; Roth, W.; Blaker, H.; Chang-Claude, J.; Brenner, H. Statin Use and Survival after Colorectal Cancer: The Importance of Comprehensive Confounder Adjustment. J. Natl. Cancer Inst. 2015, 107, djv045. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Owens, W.D.; Felts, J.A.; Spitznagel, E.L., Jr. ASA Physical Status Classifications: A Study of Consistency of Ratings. Anesthesiology 1978, 49, 239–243. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and Response Criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The Use of the Nitrogen Mustards in the Palliative Treatment of Carcinoma. With Particular Reference to Bronchogenic Carcinoma. Cancer 1948, 1, 634–656. [Google Scholar] [CrossRef]
- European Society for Medical Oncology. Performance Scales: Karnofsky & ECOG. Scores. Available online: https://oncologypro.esmo.org/Oncology-in-Practice/Practice-Tools/Performance-Scales (accessed on 28 March 2019).
- Boakye, D.; Rillmann, B.; Walter, V.; Jansen, L.; Hoffmeister, M.; Brenner, H. Impact of Comorbidity and Frailty on Prognosis in Colorectal Cancer Patients: A Systematic Review and Meta-Analysis. Cancer Treat. Rev. 2018, 64, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, S.R.; Jordhoy, M.S.; Nesbakken, A.; Skovlund, E.; Bakka, A.; Johannessen, H.O.; Wyller, T.B. Which Elements of a Comprehensive Geriatric Assessment (CGA) Predict Post-Operative Complications and Early Mortality after Colorectal Cancer Surgery? J. Geriatr. Oncol. 2010, 1, 57–65. [Google Scholar] [CrossRef]
- Parakh, S.; Wong, H.L.; Rai, R.; Ali, S.; Field, K.; Shapiro, J.; Wong, R.; Nott, L.; Gibbs, P.; Yip, D. Patterns of Care and Outcomes for Elderly Patients with Metastatic Colorectal Cancer in Australia. J. Geriatr. Oncol. 2015, 6, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in Oncology: More Than Meets the Eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to Build and Interpret a Nomogram for Cancer Prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the Added Predictive Ability of a New Marker: From Area under the ROC Curve to Reclassification and Beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Leening, M.J.; Vedder, M.M.; Witteman, J.C.; Pencina, M.J.; Steyerberg, E.W. Net Reclassification Improvement: Computation, Interpretation, and Controversies: A Literature Review and Clinician’s Guide. Ann. Intern. Med. 2014, 160, 122–131. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Hari, D.M.; Leung, A.M.; Lee, J.H.; Sim, M.S.; Vuong, B.; Chiu, C.G.; Bilchik, A.J. AJCC Cancer Staging Manual 7th Edition Criteria for Colon Cancer: Do the Complex Modifications Improve Prognostic Assessment? J. Am. Coll. Surg. 2013, 217, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.X.; Song, W.; Chen, Z.H.; Wei, J.H.; Liao, Y.J.; Lei, J.; Hu, M.; Chen, G.Z.; Liao, B.; Lu, J.; et al. Prognostic and Predictive Value of a Microrna Signature in Stage II Colon Cancer: A Microrna Expression Analysis. Lancet Oncol. 2013, 14, 1295–1306. [Google Scholar] [CrossRef]
- Stuart, B.C.; Davidoff, A.J.; Erten, M.Z. Changes in Medication Management after a Diagnosis of Cancer among Medicare Beneficiaries with Diabetes. J. Oncol. Pract. 2015, 11, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Chen, W.T.; Kung, P.T.; Chiu, C.F.; Wang, Y.H.; Shieh, S.H.; Tsai, W.C. Characteristics, Survival, and Related Factors of Newly Diagnosed Colorectal Cancer Patients Refusing Cancer Treatments under a Universal Health Insurance Program. BMC Cancer 2014, 14, 446. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Training Set | Validation Set | |||
|---|---|---|---|---|---|---|
| n = 2679 | n = 1608 | n = 1071 | ||||
| n | % | n | % | n | % | |
| Sex | ||||||
| Women | 1051 | 39.2 | 639 | 39.7 | 412 | 38.5 |
| Men | 1628 | 60.8 | 969 | 60.3 | 659 | 61.5 |
| Age (years) | ||||||
| Median (Range) | 70 (30–96) | 70 (32–96) | 70 (30–94) | |||
| 30–49 | 159 | 5.9 | 98 | 6.1 | 61 | 5.7 |
| 50–59 | 413 | 15.4 | 240 | 14.9 | 173 | 16.2 |
| 60–69 | 714 | 26.7 | 448 | 27.9 | 266 | 24.8 |
| 70–79 | 935 | 34.9 | 536 | 33.3 | 399 | 37.2 |
| 80+ | 458 | 17.1 | 286 | 17.8 | 172 | 16.1 |
| Comorbidity score | ||||||
| Median (Range) | 0 (0–7) | 0 (0–7) | 0 (0–7) | |||
| CCI 0 | 1451 | 54.2 | 871 | 54.2 | 580 | 54.2 |
| CCI 1–2 | 901 | 33.6 | 531 | 33.0 | 370 | 34.5 |
| CCI 3 | 179 | 6.7 | 107 | 6.6 | 72 | 6.7 |
| CCI 4+ | 148 | 5.5 | 99 | 6.2 | 49 | 4.6 |
| Functional status | ||||||
| Excellent 1 | 1410 | 52.6 | 864 | 53.7 | 546 | 51.0 |
| Fair 2 | 1131 | 42.2 | 662 | 41.2 | 469 | 43.8 |
| Poor 3 | 138 | 5.2 | 82 | 5.1 | 56 | 5.2 |
| Tumor location | ||||||
| Colon | 1685 | 62.9 | 1010 | 62.8 | 675 | 63.0 |
| Rectum and rectosigmoid | 994 | 37.1 | 598 | 37.2 | 396 | 37.0 |
| Tumor stage, UICC | ||||||
| I | 594 | 22.2 | 361 | 22.4 | 233 | 21.8 |
| II | 832 | 31.0 | 485 | 30.2 | 347 | 32.4 |
| III | 862 | 32.2 | 535 | 33.3 | 327 | 30.5 |
| IV | 391 | 14.6 | 227 | 14.1 | 164 | 15.3 |
| Follow up period (years) | ||||||
| Median (IQR) | 4.7 (3.3–5.3) | 4.7 (3.3–5.3) | 4.7 (3.3–5.3) | |||
| Variables | Primary Outcomes | Secondary Outcomes | |||
|---|---|---|---|---|---|
| OS | DFS † | DSS | RFS † | nDSS | |
| HR * (95% CI) | HR * (95% CI) | HR * (95% CI) | HR * (95% CI) | HR * (95% CI) | |
| Sex | |||||
| Women | Ref | Ref | Ref | Ref | Ref |
| Men | 0.96 (0.81–1.14) | 0.97 (0.83–1.14) | 0.74 (0.59–0.92) | 0.80 (0.65–0.97) | 1.47 (1.12–1.92) |
| Age | |||||
| 30–49 | 1.56 (0.98–2.48) | 1.42 (0.93–2.18) | 1.31 (0.80–2.14) | 1.32 (0.86–2.03) | 1.58 (0.29–8.62) |
| 50–59 | Ref | Ref | Ref | Ref | Ref |
| 60–69 | 1.77 (1.26–2.49) | 1.40 (1.04–1.89) | 1.34 (0.92–1.96) | 1.16 (0.84–1.60) | 5.73 (2.06–15.95) |
| 70–79 | 2.37 (1.70–3.30) | 1.75 (1.31–2.35) | 1.83 (1.26–2.64) | 1.37 (0.99–1.88) | 7.86 (2.85–21.66) |
| 80+ | 4.66 (3.27–6.63) | 2.81 (2.05–3.85) | 2.61 (1.71–3.99) | 1.60 (1.11–2.32) | 19.68 (7.10–54.59) |
| Comorbidity score | |||||
| CCI 0 | Ref | Ref | Ref | Ref | Ref |
| CCI 1–2 | 1.13 (0.93–1.36) | 1.16 (0.97–1.39) | 0.99 (0.77–1.27) | 1.03 (0.82–1.29) | 1.37 (1.02–1.86) |
| CCI 3 | 1.84 (1.36–2.49) | 1.63 (1.21–2.21) | 1.75 (1.15–2.66) | 1.28 (0.85–1.94) | 2.03 (1.30–3.17) |
| CCI 4+ | 2.39 (1.78–3.21) | 2.63 (1.97–3.51) | 1.54 (0.97–2.46) | 1.80 (1.20–2.70) | 3.81 (2.55–5.70) |
| Functional status | |||||
| Excellent | Ref | Ref | Ref | Ref | Ref |
| Fair | 1.42 (1.17–1.72) | 1.31 (1.10–1.57) | 1.38 (1.09–1.76) | 1.25 (1.01–1.56) | 1.44 (1.06–1.97) |
| Poor | 2.52 (1.82–3.48) | 2.05 (1.49–2.82) | 1.84 (1.14–2.97) | 1.67 (1.09–2.56) | 3.20 (2.02–5.05) |
| Tumor location | |||||
| Colon | Ref | Ref | Ref | Ref | Ref |
| Rectum | 1.16 (0.98–1.37) | 1.12 (0.95–1.32) | 1.10 (0.88–1.38) | 1.06 (0.87–1.29) | 1.10 (0.84–1.43) |
| Tumor stage | |||||
| I | Ref | Ref | Ref | Ref | Ref |
| II | 1.71 (1.27–2.31) | 1.92 (1.44–2.55) | 3.11 (1.50–6.46) | 3.83 (2.16–6.82) | 1.45 (1.04–2.02) |
| III | 2.60 (1.96–3.46) | 2.81 (2.13–3.71) | 11.54 (5.87–22.72) | 9.39 (5.43–16.24) | 1.08 (0.76–1.54) |
| IV | 17.84 (13.20–24.12) | 14.94 (11.15–20.04) | 92.15 (46.69–181.9) | 50.30 (28.99–87.29) | 1.99 (1.08–3.66) |
| Survival Outcomes | Training Set | Validation Set | ||||
|---|---|---|---|---|---|---|
| Harrell’s C-Index | Harrell’s C-Index | |||||
| Stage Only | Model 2 † | Nomogram ‡ | Stage Only | Model 2 † | Nomogram ‡ | |
| All patients | ||||||
| Overall survival | 0.7121 | 0.7745 | 0.7929 | 0.7071 | 0.7489 | 0.7680 |
| Disease-free survival | 0.7027 | 0.7333 | 0.7506 | 0.7014 | 0.7179 | 0.7369 |
| Disease-specific | 0.8199 | 0.8446 | 0.8498 | 0.8063 | 0.8229 | 0.8302 |
| Recurrence-free survival | 0.7749 | 0.7878 | 0.7920 | 0.7591 | 0.7678 | 0.7720 |
| Non-disease-specific | 0.5542 | 0.7504 | 0.7965 | 0.5240 | 0.7087 | 0.7503 |
| Stages I–III | ||||||
| Overall survival | 0.6315 | 0.7254 | 0.7546 | 0.6124 | 0.6716 | 0.7062 |
| Disease-free survival | 0.6409 | 0.6836 | 0.7089 | 0.6215 | 0.6463 | 0.6713 |
| Disease-specific | 0.7557 | 0.7867 | 0.7988 | 0.7278 | 0.7478 | 0.7627 |
| Recurrence-free survival | 0.7297 | 0.7361 | 0.7445 | 0.6869 | 0.6946 | 0.7044 |
| Non-disease-specific | 0.5669 | 0.7554 | 0.8005 | 0.5246 | 0.7103 | 0.7492 |
| Stage IV | ||||||
| Overall survival | - | 0.6207 | 0.6325 | - | 0.6018 | 0.6166 |
| Disease-free survival | - | 0.5982 | 0.6067 | - | 0.5822 | 0.5957 |
| Disease-specific | - | 0.6234 | 0.6377 | - | 0.5963 | 0.6136 |
| Recurrence-free survival | - | 0.6060 | 0.6113 | - | 0.5767 | 0.5947 |
| Non-disease-specific | - | 0.7983 | 0.8182 | - | 0.5573* | 0.6193 * |
| Outcomes | Validation Set | ||
|---|---|---|---|
| NRIe | NRIne | NRI >0 (95% CI) * | |
| All patients | |||
| Overall survival | −0.263 | 0.415 | 0.152 (0.020–0.497) |
| Disease-free survival | −0.297 | 0.513 | 0.216 (0.070–0.336) |
| Disease specific survival | −0.338 | 0.588 | 0.250 (0.122–0.395) |
| Recurrence-free survival | −0.580 | 0.657 | 0.077 (−0.031–0.293) |
| Non-disease-specific survival | −0.287 | 0.489 | 0.202 (−0.209–0.689) |
| Stages I–III | |||
| Overall survival | 0.248 | 0.386 | 0.634 (0.224–0.787) |
| Disease-free survival | −0.160 | 0.487 | 0.327 (0.163–0.578) |
| Disease specific survival | −0.320 | 0.544 | 0.224 (−0.423–0.607) |
| Recurrence-free survival | −0.116 | 0.563 | 0.447 (0.082–0.691) |
| Non-disease-specific survival | −0.350 | 0.618 | 0.222 (−0.066–0.932) |
| Stage IV | |||
| Overall survival | 0.284 | 0.101 | 0.386 (0.012–0.738) |
| Disease-free survival | −0.117 | 0.569 | 0.452 (−0.196–0.719) |
| Disease specific survival | −0.151 | 0.566 | 0.415 (−0.335–0.631) |
| Recurrence-free survival | −0.016 | 0.236 | 0.220 (−0.164–0.588) |
| Non-disease-specific survival | 0.220 | 0.353 | 0.573 (−1.124; 1.803) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boakye, D.; Jansen, L.; Schneider, M.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Personalizing the Prediction of Colorectal Cancer Prognosis by Incorporating Comorbidities and Functional Status into Prognostic Nomograms. Cancers 2019, 11, 1435. https://doi.org/10.3390/cancers11101435
Boakye D, Jansen L, Schneider M, Chang-Claude J, Hoffmeister M, Brenner H. Personalizing the Prediction of Colorectal Cancer Prognosis by Incorporating Comorbidities and Functional Status into Prognostic Nomograms. Cancers. 2019; 11(10):1435. https://doi.org/10.3390/cancers11101435
Chicago/Turabian StyleBoakye, Daniel, Lina Jansen, Martin Schneider, Jenny Chang-Claude, Michael Hoffmeister, and Hermann Brenner. 2019. "Personalizing the Prediction of Colorectal Cancer Prognosis by Incorporating Comorbidities and Functional Status into Prognostic Nomograms" Cancers 11, no. 10: 1435. https://doi.org/10.3390/cancers11101435