The Multifaceted Roles of Pyroptotic Cell Death Pathways in Cancer


1
Institute for Translational Medicine, Medical College of Qingdao University, Dengzhou Road 38, Qingdao 266021, China
2
Key Laboratory of Experimental Marine Biology, Institute of Oceanology, Chinese Academy of Sciences, Qingdao 266071, China
*
Authors to whom correspondence should be addressed.
Cancers 2019, 11(9), 1313; https://doi.org/10.3390/cancers11091313
Submission received: 20 July 2019
/
Revised: 26 August 2019
/
Accepted: 26 August 2019
/
Published: 5 September 2019
(This article belongs to the Special Issue Cell Death in Cancer)
{kind=link}
{kind=link}
{kind=link}
Abstract
:Cancer is a category of diseases involving abnormal cell growth with the potential to invade other parts of the body. Chemotherapy is the most widely used first-line treatment for multiple forms of cancer. Chemotherapeutic agents act via targeting the cellular apoptotic pathway. However, cancer cells usually acquire chemoresistance, leading to poor outcomes in cancer patients. For that reason, it is imperative to discover other cell death pathways for improved cancer intervention. Pyroptosis is a new form of programmed cell death that commonly occurs upon pathogen invasion. Pyroptosis is marked by cell swelling and plasma membrane rupture, which results in the release of cytosolic contents into the extracellular space. Currently, pyroptosis is proposed to be an alternative mode of cell death in cancer treatment. Accumulating evidence shows that the key components of pyroptotic cell death pathways, including inflammasomes, gasdermins and pro-inflammatory cytokines, are involved in the initiation and progression of cancer. Interfering with pyroptotic cell death pathways may represent a promising therapeutic option for cancer management. In this review, we describe the current knowledge regarding the biological significance of pyroptotic cell death pathways in cancer pathogenesis and also discuss their potential therapeutic utility.
1. Introduction
Cell death is a crucial phenomenon in biological activities and serves a pivotal role in maintaining homeostatic balance in vivo [1]. At present, several forms of cell death, such as apoptosis, necroptosis and pyroptosis, have been found [2]. As a form of non-inflammatory programmed cell death, apoptosis can be induced by either intrinsic or extrinsic factors, followed by sequential activation of initiator and executioner caspases [3,4]. Both apoptosis and pyroptosis are executed by caspases. Apoptosis is mediated by caspase-2, -3, -6, -7, -8 and -9 [5]. The term pyroptosis was initially proposed in 2001. Pyroptosis is inherently a type of programmed cell death that is initiated by inflammatory caspases (caspase-1, -4, -5 and -11) upon activation of the canonical or non-canonical inflammasome pathways [6]. The requirement of inflammatory caspases in executing pyroptosis differentiates it from another inflammatory and necrotic form of programmed cell death known as necroptosis [7]. Necroptosis is a form of regulated cell death mediated by receptor-interacting serine/threonine-protein kinase 3 (RIPK3) (all the abbreviations are listed in Table S1) and its downstream substrate mixed lineage kinase domain-like pseudokinase (MLKL) [8]. RIPK3 phosphorylates the necroptosis executioner MLKL, resulting in the formation of MLKL oligomers, which then translocate to the plasma membrane [9]. These events ultimately lead to necrotic plasma membrane permeabilization and cell death associated with loss of cell and organelle integrity [10]. Necroptosis is widely known as a defense mechanism against viral infection and can induce programmed cell death in virus-infected cells.
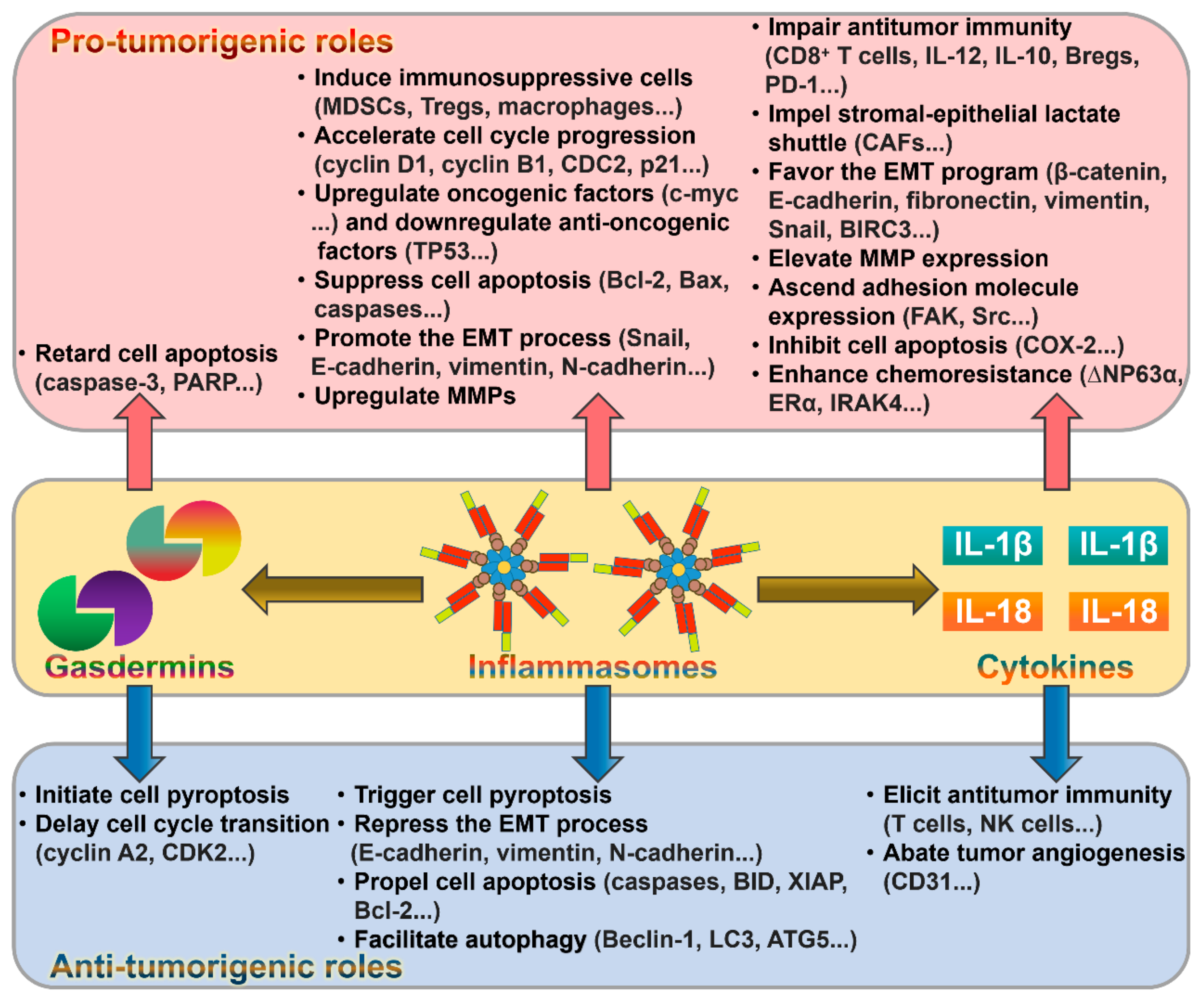
Recently, pyroptosis has become a research hotspot in programmed cell death. The induction of pyroptosis requires the activation of the pore-forming protein gasdermin D (GSDMD) by inflammatory caspases [11]. In the canonical inflammasome pathway, caspase-1 mediates the cleavage of GSDMD and the maturation of pro-inflammatory cytokines, interleukin-1β (IL-1β) and interleukin-18 (IL-18) [12]. GSDMD pores favor the leakage of intracellular components into the extracellular environment. Unlike canonical inflammasomes, the non-canonical inflammasome pathway can be initiated by the direct binding of caspase-4, -5 and -11 to lipopolysaccharide (LPS) from Gram-negative bacteria [13]. These caspases activate GSDMD to induce cell lysis and death. In addition, caspase-1 is activated in the non-classical pyroptosis pathway, leading to the production of IL-1β and IL-18, which are liberated into the extracellular milieu [14]. Pyroptosis serves a vital role in host defense response against pathogens [15]. Pyroptotic cell death, started by pathogen infection, contributes to the release of cytosolic contents from infected cells, hence triggering an inflammatory cascade [16]. Local inflammation results in recruitment and activation of immune cells, ultimately facilitating the clearance of invading pathogens. Of note, recent studies have confirmed that pyroptosis functions in orchestrating cancer cell death [17,18]. Moreover, inflammasomes, gasdermins and pro-inflammatory cytokines can regulate key processes involved in cancer development. Therefore, pyroptotic cell death pathways constitute a novel mechanism contributing to cancer pathogenesis. In this review, we summarize the recent findings related to the role and mechanism of pyroptotic cell death pathways in cancer progression and discuss potential therapeutic values in targeting pyroptosis for cancer therapy.
2. The Characteristics of Pyroptosis
Pyroptosis, a pro-inflammatory form of cell death, is generally induced by intracellular pathogen infection and forms part of the host defense system [19]. Pyroptosis can be induced via two pathways, the canonical and non-canonical inflammasome pathways (Figure 1). Canonical pyroptosis is executed by caspase-1, which is triggered by a number of pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs), while non-canonical pyroptosis is dependent on human caspase-4/-5 or mouse caspase-11 and can be induced by intracellular LPS [20]. The morphological features of caspase-1-dependent pyroptosis and caspase-1-independent pyroptosis are similar. Both are characterized by the loss of cellular membrane integrity, chromatin condensation and DNA fragmentation. Specially, the cellular membrane undergoes rupture, resealing and swelling, and forms a balloon-shaped vesicle around the nucleus [21]. The cellular membrane becomes disrupted, and the cytoplasmic materials, including pro-inflammatory cytokines, endogenous DAMPs and alarmins, are released into the extracellular space [16].
3. The Canonical Pyroptosis Pathway
Inflammasomes are macromolecular protein complexes consisting of an inflammasome sensor, the adaptor protein apoptosis-associated speck-like protein containing a caspase recruitment domain (ASC) and caspase-1 [22]. Based on their structural features, the inflammasome sensors are categorized into nucleotide-binding oligomerization domain (NOD)-like receptors (NLRs), absent in melanoma 2 (AIM2)-like receptors (ALRs) and pyrin [23]. The NLRs belong to host pattern recognition receptors (PRRs) and act as intracellular sensors of PAMPs and DAMPs [24]. The NLRs are composed of three main domains: An N-terminal caspase recruitment domain (CARD) or pyrin domain, a middle nucleotide-binding domain (NBD or NACHT) and a C-terminal leucine-rich repeat (LRR) domain [25]. The NBD domain mediates NLR oligomerization, while the LRR acts as a sensor of PAMPs and DAMPs [26]. Once formed, the N-terminal pyrin or CARD domain of NLR oligomers recruits and seeds ASC or caspase-1. Among NLRs, NLR family pyrin domain-containing 1 (NLRP1), NLRP2, NLRP3, NLRP6, NLRP7, NLRP12 and NLR family CARD domain-containing protein 4 (NLRC4) are regarded as inflammasome-nucleating proteins [27]. The ALRs are a newly characterized class of PRRs that can detect pathogen DNAs in both the cytosol and nucleus [28]. The ALR family member AIM2 consists of an N-terminal pyrin domain, which binds to the pyrin domain of ASC, and a C-terminal hematopoietic interferon (IFN)-inducible nuclear protein containing a 200-amino-acid repeat (HIN-200) domain, which directly interacts with dsDNA [29]. AIM2 can initiate inflammasome assembly upon activation leading to caspase-1-mediated inflammatory responses and cell death [30]. Pyrin is another vital inflammasome-forming protein [31]. Pyrin harbors an N-terminal pyrin domain that is responsible for its combination with ASC and subsequent activation of caspase-1 [32].
Five canonical inflammasomes, NLRP1, NLRP3, NLRC4, AIM2 and pyrin, have been identified [33]. These inflammasomes can be triggered by different stimuli. For instance, the mouse NLRP1b and rat NLRP1 inflammasome sensors can be activated after their cleavage by a lethal factor released by the Gram-positive bacterium Bacillus anthracis [34,35]. NLRP3 mainly recognizes viral dsRNAs, bacterial toxins, reactive oxygen species (ROS) and endogenous damage signals [32]. NLRC4 responds to bacterial protein stimulation, while AIM2 is predominantly responsible for the recognition of cytoplasmic dsDNAs during bacterial or viral infection [36,37]. Pyrin is activated by bacterial toxins that modify RhoA GTPases [38]. The adaptor protein ASC bridges the interaction between the sensor protein and procaspase-1 within the canonical inflammasome [39]. ASC recruits procaspase-1 via a CARD–CARD domain interaction [40]. Remarkably, ASC is indispensable for the pyrin domain-containing sensors (NLRP3, AIM2 and pyrin) to recruit procaspase-1, while the CARD-based sensors (NLRP1b and NLRC4) can directly bind to procaspase-1 [32]. After being recruited to the inflammasome, procaspase-1 forms dimers and activates its own protease capability to generate caspase-1 [15]. Caspase-1-mediated cell death represents the canonical pyroptosis pathway. Activated caspase-1 induces the proteolytic processing of the pro-inflammatory precursor cytokines (pro-IL-1β and pro-IL-18) to release active IL-1β and IL-18 [41]. The pro-pyroptotic factor GSDMD consists of an N-terminal pore-forming domain and a C-terminal repressor domain (RD). The RD domain binds the GSDMD-NT and maintains the protein in an autoinhibitory state [42]. Caspase-1 activated by the canonical inflammasomes induces the cleavage of GSDMD, liberating the N-terminal fragment (GSDMD-NT) [11]. In the canonical pyroptosis pathway, the formation of inflammasomes is required for caspase-1-mediated cleavage of GSDMD. Caspase-1, -4, -5 and -11 cleave GSDMD at an aspartate residue in the linker that connects GSDMD-NT and RD, which leads to the generation of a noncovalent GSDMD-NT-RD complex [43]. Intriguingly, GSDMD-NT has high affinity for specific lipid compositions, such as phosphatidic acid, phosphatidylserine, cardiolipin, mono- and bisphosphorylated phosphoinositols [44]. As phosphatidylserine and phosphoinositols are restricted to the inner leaflet of the plasma membrane, GSDMD-NT can only oligomerize to form pores from the cytosolic face [45]. Upon lipid binding, the N-terminal domain of gasdermin A3 (GSDMA3) underwent significant conformational changes, leading to its separation from the RD domain and oligomerization into a ring-shaped structure [46]. In addition, the conformational changes also facilitated membrane insertion of the ring architecture. Considering the similar structural and biochemical features between GSDMD and GSDMA3, this mechanism could apply to the formation of GSDMD-NT pores. Moreover, cleaved GSDMD exhibits no affinity for the outer leaflet of the cellular membrane, avoiding damage to surrounding cells during pyroptotic cell death [44]. GSDMD-NT-formed pores mediate osmotic cell swelling, plasma membrane rupture and the liberation of intracellular components including IL-1β and IL-18 [47]. Additionally, caspase-1 plays an important role in triggering DNA fragmentation.
GSDMD-NT pores act as the conduit for potassium (K+) efflux that sufficiently triggers the activation of the NLRP3 inflammasome [48,49]. Caspase-11 could activate the canonical NLRP3 inflammasome by boosting GSDMD-induced K+ efflux, demonstrating that canonical and non-canonical inflammasomes functioned synergistically to protect the host against pathogen invasion [50]. The influx of calcium (Ca2+) ions from the extracellular environment also occurs through GSDMD-NT-induced pores [6]. Interestingly, GSDMD-NT pores did not necessarily lead to cell death, since Ca2+ influx served as a signal for cells to initiate membrane repair program. Moreover, the repair mechanism involved recruitment of the endosomal sorting complexes required for transport (ESCRT) machinery to damaged membrane sites. Accordingly, suppression of the ESCRT-III machinery significantly promoted pyroptotic cell death downstream of GSDMD activation. In the pyroptosis pathway, the GSDMD-NT pore serves as a channel for release of IL-1β and IL-18. Notably, these inflammatory cytokines can be released by alternative mechanisms. For instance, activated caspase-1, pro-IL-1β and pro-IL-18 can be encapsulated into secretory lysosomes [51]. Caspase-1 processes pro-IL-1β and pro-IL-18 to generate bioactive cytokines within secretory lysosomes. The mature cytokines are then released into the extracellular milieu via fusion of lysosomes with the plasma membrane. Moreover, caspase-1-mediated IL-1β cleavage triggered its translocation from the cytosol to plasma membrane and was sufficient for GSDMD-independent IL-1β release [52]. In contrast, caspase-1 and GSDMD could accelerate IL-1β secretion. During necroptosis, MLKL activation induced the assembly of the NLRP3 inflammasome and caused plasma membrane rupture [53]. These events resulted in the maturation and release of IL-1β. Thus, IL-1β and IL-18 can be released into the extracellular space through GSDMD-independent mechanisms.
4. The Non-Canonical Pyroptosis Pathway
In addition to the above-described canonical inflammasome pathway, the non-canonical inflammasome was identified [54]. The molecular mechanisms underlying the actions of the non-canonical inflammasome are still being defined. It has been reported that human caspase-4 and -5, the orthologues of mouse caspase-11, serve as receptors for intracellular LPS [13]. Unlike caspase-1, caspase-4, -5 and -11 do not require an upstream signaling pathway to sense LPS, but directly detect LPS [13]. Notably, caspase-11 cannot be activated unless LPS gains access to the cytosol. Specifically, caspase-4, -5 and -11 directly bind to the lipid A moiety of LPS from Gram-negative bacteria in the cytoplasm via their CARD domains. The binding of LPS to caspase-4, -5 and -11 promotes their oligomerization and activation. These activated caspases then cleave GSDMD to generate biologically active GSDMD-NT, contributing to pyroptotic cell death. Thus, in the non-canonical pyroptosis pathway, inflammasome assembly is not necessary for caspase-4, -5 and -11-mediated cleavage of GSDMD. GSDMD-NT causes the activation of caspase-1-dependent NLRP3 inflammasome, resulting in the secretion of IL-1β and IL-18 [55]. Recently, the apoptotic caspase-8 was found to cleave GSDMD, leading to pyroptotic cell death in murine macrophages [56]. However, caspase-8 was less efficient at mediating GSDMD cleavage than caspase-1. Downstream of caspase-8-mediated GSDMD cleavage, the NLRP3 inflammasome was activated, leading to the maturation and secretion of pro-inflammatory cytokines.
5. The Role of Inflammasomes in Cancer
It is well-known that chronic inflammation can propel cancer occurrence. The inflammasome is a multiprotein complex that can modulate innate and adaptive immune responses. Increasing evidence demonstrates that inflammasomes are implicated in cancer growth, invasion and metastasis [57]. Several inflammasomes including NLRP3, NLRP1, NLRC4, pyrin and AIM2 play a vital role in cancer pathogenesis through their regulation of immunity and apoptosis [58]. Among these inflammasome complexes, the NLRP3 inflammasome is the best characterized and can be activated by inflammatory infections and endogenous stimuli, such as pathogens, pore-forming toxins and adenosine triphosphate (ATP) [59]. NLRP3 consists of a pyrin domain, a central NBD and an LRR region. Upon activation, NLRP3 interacts with the pyrin domain of ASC through homophilic interactions [60]. The adaptor ASC in turn recruits procaspase-1 via a CARD–CARD interaction [40].
The roles of NLRP3 in cancer occurrence and progression have been intensively studied. Polymorphisms of the NLRP3 inflammasome were associated with various malignancies including melanoma and colon cancer [61]. The effect of NLRP3 on immune regulation represents a vital mechanism mediating its pro-tumorigenic action. For instance, the NLRP3 inflammasome/IL-1β pathway enhanced immunosuppressive cell accumulation to facilitate the tumorigenesis of head and neck squamous cell carcinoma (HNSCC) [62]. Another study showed that the NLRP3 inflammasome was correlated with the carcinogenesis and development of cancer stem cells (CSCs) in HNSCC [63]. The NLRP3 inflammasome was shown to be engaged in inflammation-related lung carcinogenesis [64]. NLRP3 also promoted lung tumorigenesis induced by benzo(a)pyrene plus LPS in mice [65]. It was reported that inactivation of the NLRP3 inflammasome repressed tumor growth and immunosuppression in breast cancer [66]. Additionally, NLRP3 promoted the expansion of immune-suppressive macrophages in pancreatic ductal adenocarcinoma (PDAC), thus facilitating the generation of tumor-promoting T helper type 2 (Th2) cells and inhibiting the activation of cytotoxic CD8+ T cells [67]. Therefore, the NLRP3 signaling primed macrophage-induced adaptive immune suppression in PDAC. Targeting NLRP3 might be a promising immunotherapeutic strategy for PDAC.
Several literatures have shown that the NLRP3 inflammasome orchestrates cancer pathogenesis by governing cell death pathways. For instance, the NLRP3 inflammasome was involved in leptin-induced growth of breast cancer cells via promotion of cell cycle progression and suppression of cell apoptosis [68]. The NLRP3 inflammasome activation enhanced the proliferation and suppressed the apoptosis of lymphoma cells through upregulation of c-myc and B-cell lymphoma-2 (Bcl-2), and downregulation of tumor protein p53 (TP53) and Bcl-2-associated X protein (Bax) [69]. On the other hand, the NLRP3 inflammasome might suppress cancer progression. 17β-estradiol (E2)-induced activation of the NLRP3 inflammasome triggered pyroptotic cell death and suppressed protective autophagy in hepatocellular carcinoma (HCC) cells [70].
Epithelial-mesenchymal transition (EMT) is a well-orchestrated process by which epithelial cells can convert into cells of the mesenchymal phenotype [71]. It is generally accepted that EMT plays a vital role in tumor invasion and metastasis [72]. The NLRP3 inflammasome controls the EMT program during cancer pathogenesis. A previous study demonstrated that the NLRP3 inflammasome enhanced the migratory and metastatic abilities of colorectal cancer (CRC) cells [73]. In terms of mechanism, NLRP3 promoted the EMT process in CRC cells through modulation of Snail1 [74]. NLRP3 deletion limited the proliferation and EMT-induced invasion of pancreatic cancer (PC) cells [75]. NLRP3 enhanced the proliferation, invasion and migration of oral squamous cell carcinoma (OSCC) cells by modifying the expression of E-cadherin, vimentin and N-cadherin [76]. NLRP3 promoted the proliferation, invasion and migration, as well as suppressed the apoptosis of glioma cells [77]. Mechanistically, NLRP3 regulated glioma progression and metastasis via its effects on the EMT program and the phosphatase and tensin homolog (PTEN)/protein kinase B (Akt) signaling pathway. Activation of the NLRP3 inflammasome antagonized the suppressive effect of polydatin on the proliferation and migration of non-small cell lung cancer (NSCLC) cells [78]. Further mechanistic study indicated that the NLRP3 inflammasome ascended the expression of Snail and lowered the expression of E-cadherin in lung cancer cells [79]. Activation of the NLRP3 inflammasome promoted the metastasis of breast cancer cells [80]. It can be speculated that inactivation of the NLRP3 inflammasome leads to the blockage of cancer progression. As expected, β-hydroxybutyrate inhibited the migration of C6 glioma cells by suppressing the activation of the NLRP3 inflammasome [81]. Consequently, the NLRP3 inflammasome can modify the malignant behaviors of cancer cells.
The NLRP1 inflammasome was the first member of the NLRP family to be discovered and consists of NLRP1, the adaptor protein ASC and caspase-1 [82]. The polymorphism or mutation of the NLRP1 gene was found to be tightly associated with the progression of melanoma [83,84]. NLRP1 facilitated melanoma growth via depressing the apoptotic pathway by inhibiting the activities of caspase-2, -3, -7 and -9 [85]. NLRC4 comprises an N-terminal CARD domain, a central NBD and a C-terminal LRR domain. NLRC4 directly recruits procaspase-1 and is activated by a wide range of bacterial pathogens [86]. NLRC4 plays an important role in limiting cancer progression. NLRC4 and caspase-1 restricted CRC tumorigenesis through regulation of colonic epithelial cell proliferation and death [87]. Pyrin is composed of a pyrin domain, two B-boxes, a coiled-coil domain and a SPRY domain [88]. Pyrin associates with ASC via pyrin–pyrin domain homophilic interactions, which in turn recruits caspase-1 to form an inflammasome complex [89]. The pyrin inflammasome played a crucial role in enhancing intestinal barrier integrity and preventing colonic inflammation to restrict colon tumorigenesis [90].
AIM2 belongs to the pyrin and HIN domain-containing protein (PYHIN) family and can be activated by cytosolic dsDNAs of bacterial or viral origin [91]. The interaction between AIM2 and dsDNA results in AIM2 oligomerization, ultimately leading to inflammasome assembly. Apart from its role in host immune defense, AIM2 also acts as an oncogene in cancer. AIM2 was deregulated in several types of cancer and might represent a potential therapeutic target for cancer [92]. The AIM2 inflammasome boosted liver inflammation and proliferative responses during chemical-induced hepatocarcinogenesis [93]. AIM2 promoted the proliferation of NSCLC cells by upregulating cell cycle-related proteins cyclin B1 and cell division cycle 2 (CDC2) [94]. Consistently, inactivation of the AIM2 inflammasome by luteolin caused decreased expression of p-CDC2 (Tyr15), p21 and cyclin B1, thus inducing cell cycle arrest in NSCLC [95]. AIM2 depletion also restrained the EMT process and cell invasion in NSCLC through downregulation of vimentin and matrix metalloproteinase 9 (MMP9). Similarly, AIM2 could enhance the growth and invasion of cutaneous squamous cell carcinoma (cSCC) cells by upregulating MMP1 and MMP13 [96]. Paradoxically, AIM2 is regarded as a tumor suppressor in various cancers. For instance, AIM2 was capable of inhibiting the proliferation, invasion and migration of renal cell carcinoma (RCC) cells by upregulating autophagy-related genes (Bcl-2, Beclin-1, LC3-II and ATG5) [97]. AIM2 enhanced the apoptosis of CRC cells by inhibiting the phosphoinositide 3-kinase (PI3K)/Akt pathway [98]. AIM2 depressed the proliferation and invasion of HCC cells by blocking the mammalian target of the rapamycin (mTOR)/S6 kinase 1 (S6K1) pathway [99]. The depletion of AIM2 activated the EMT process in HCC cells through regulation of E-cadherin, vimentin and N-cadherin, thereby promoting HCC cell migration and metastasis [100]. The nanoparticles containing AIM2 could inhibit RCC growth and might offer a potential therapeutic approach for RCC treatment [101].
The inflammasome adaptor ASC affects cancer progression by interfering with the apoptotic signaling pathway in cancer cells. ASC was shown to restrain the apoptosis of gastric cancer (GC) cells through an IL-18-mediated inflammation-independent mechanism [102]. As a result, depletion of IL-18 resulted in the suppression of ASC-regulated gastric tumorigenesis. ASC reduced the growth of schwannoma cells by activating caspase-3 and -9 and upregulating Bcl-2 homology domain 3 (BH3)-interacting domain death agonist (BID) [103]. ASC negatively modulated the tumorigenesis of fibrosarcoma by activating caspase-9 and inhibiting the nuclear factor-ĸB (NF-ĸB)-related X-linked inhibitor of apoptosis protein (XIAP) [104]. ASC inhibited the proliferation, motility and invasion of lung cancer cells through downregulation of Bcl-2 and phospho-Src [105]. It has been reported that the apoptosis sponsor caspase-8 also functions as an enhancer of cancer cell migration by phosphorylation via Src [106]. ASC could combine with caspase-8 to impede its accessibility to Src, hence repressing the metastasis of melanoma cells [107]. It is well established that loss of E-cadherin expression, a hallmark of EMT, is a pivotal step impelling metastatic dissemination in multiple cancers [108]. Mechanistically, E-cadherin downregulation contributes to tumor metastasis by inducing transcription factors such as Twist [109]. ASC enhanced the invasion, migration and metastasis of OSCC cells by reducing the expression of E-cadherin [110]. The molecular mechanisms behind the effects of ASC on tumor metastasis remain to be further explored. The biological function of inflammasome components in multiple types of cancer highlights their therapeutic potential as molecular targets for cancer.
Although there are some studies that support the suppressive effects of inflammasome components against cancer, some reports still indicate the pro-tumorigenic functions of inflammasome constituents (Figure 2). The dual roles of the inflammasome pathways may depend on the type of tumors or tissues. Additional exploration is warranted to fully disclose the function of these multiprotein complexes in cancer pathogenesis before targeting them for therapeutic intervention in cancer. The signaling pathways or molecules initiating inflammasome activation during cancer progression should be identified. The detailed mechanisms underlying the involvement of inflammasomes in cancer pathology remain to be studied. Targeting inflammasome components or signaling pathways may provide a new opportunity for development of effective anticancer therapeutics.
Small molecules targeting inflammasome components (e.g., monoclonal antibodies and antagonists) are being developed for use in cancer management [111]. The P2X7 receptor is crucial for the activation of the NLRP3/IL-1 pathway [112]. Avastin (bevacizumab) is a recombinant humanized monoclonal antibody that can suppress angiogenesis by targeting vascular endothelial growth factor A (VEGFA) [113]. It has been approved by the U.S. Food and Drug Administration (FDA) for the treatment of various cancers [114]. Bevacizumab was shown to repress the growth and neoangiogenesis of P2X7-expressing tumors [115]. Accordingly, bevacizumab may be a potent inhibitor of the NLRP3/IL-1 pathway. Moreover, glyburide, also known as glibenclamide, was able to prevent NLRP3 activation and IL-1β production induced by microbial ligands and DAMPs [116]. Of note, accumulating evidence has proven the anticancer property of glibenclamide [117,118,119]. In addition, MCC950 was a specific small-molecule inhibitor of NLRP3 and AIM2 inflammasomes, which might represent a promising therapeutic approach for inflammasome-associated cancers [120]. Intriguingly, non-coding RNAs, including circRNAs and miRNAs, could regulate the activation of the NLRP3 inflammasome [121,122]. Thus, specific inhibitors of the NLRP3 inflammasome hold considerable promise as novel therapeutic agents aimed at treating cancers. Nevertheless, inflammasome-based therapies may cause deleterious side effects including the excessive inhibition of inflammasomes and the development of autoinflammatory or metabolic diseases. The limitation of inflammation-targeted drugs remains to be systematically investigated. Besides, their safety and efficacy must be validated before their clinical translation. A better understanding of the regulatory mechanism and clinical relevance of the inflammasome pathways in cancer will possibly open the way to the translation of small-molecules targeting inflammasomes in clinical cancer therapy.
6. The Contribution of Gasdermins to Cancer Progression
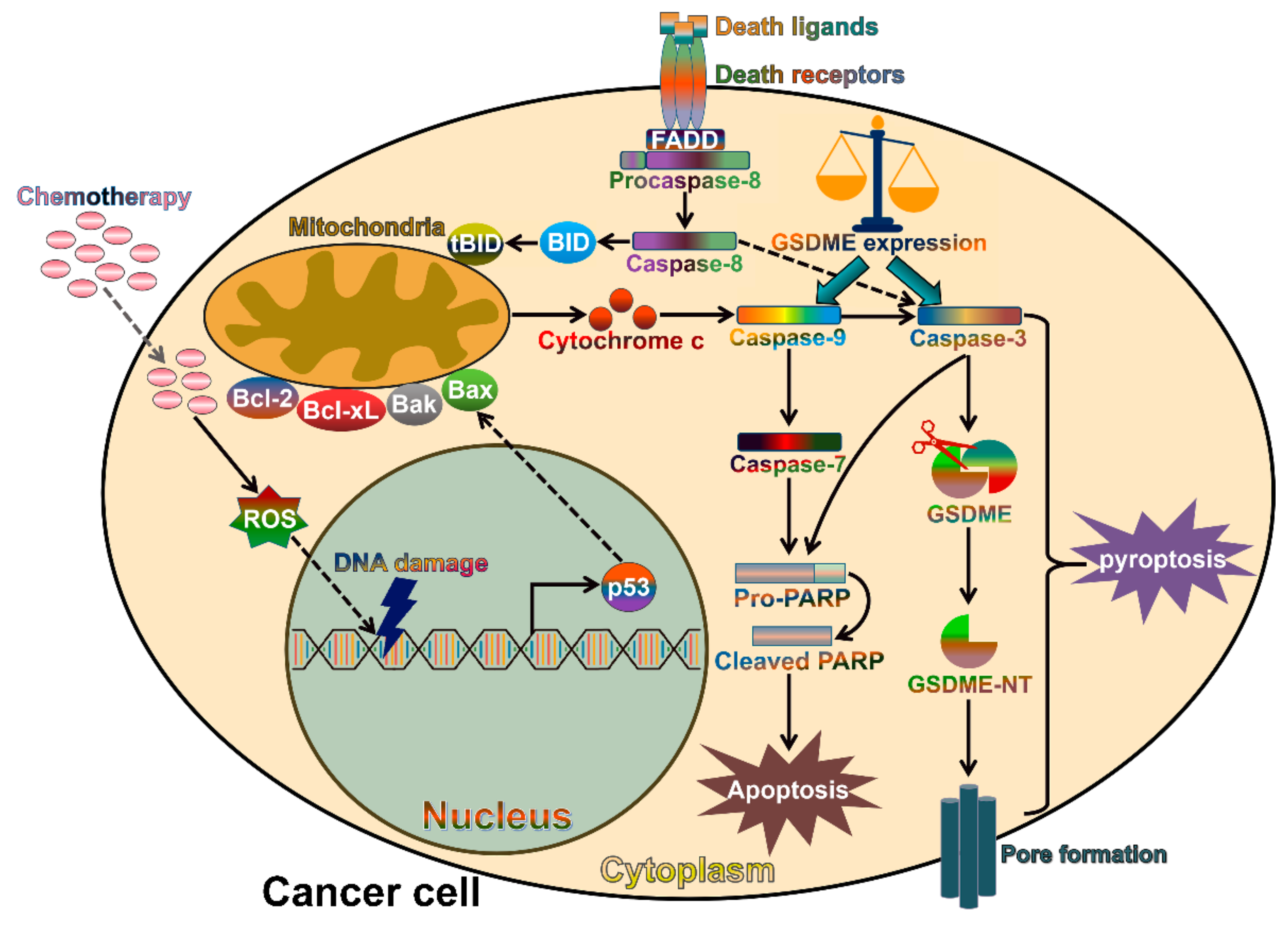
Chemotherapeutic agents are capable of killing tumor cells by activating caspase-3-mediated apoptosis (Figure 3). As cancer cells usually lose their capability to initiate or execute apoptosis, they are resistant to conventional chemotherapeutic agents that target the cellular apoptosis pathway [123]. Therefore, it is necessary to identify alternative cell death pathways for effective cancer management. Notably, a recent study indicated that cleavage of gasdermin E (GSDME) by caspase-3 induced pyroptosis in neuroblastoma and melanoma cells following treatment with chemotherapeutic agents, such as DNA-binding/modifying compounds (doxorubicin, cisplatin and actinomycin-D) and the topoisomerase inhibitors (topotecan, CPT-11, etoposide and mitoxantrone) [17]. Therefore, the activation of caspase-3/GSDME-dependent pyroptosis might be an alternative therapeutic strategy for cancer treatment. Likewise, the chemotherapeutic agent cisplatin initiated the activation of caspase-3 and generation of bioactive GSDME-NT, thus eliciting pyroptosis in lung cancer cells [18]. Another study also showed that the caspase-3/GSDME pathway mediated pyroptotic cell death induced by small-molecule inhibitors in lung cancer cells [124]. Lobaplatin could induce the activation of ROS and the phosphorylation of c-Jun N-terminal kinase (JNK) in CRC cells [125]. This led to the recruitment of Bax to mitochondria and sequential release of cytochrome c, followed by caspase-3/-9 activation and GSDME-mediated pyroptosis. The anticancer agent 5-fluorouracil (5-FU) induced caspase-3-mediated cleavage of GSDME in GC cells, which switched cell apoptosis into pyroptosis [126]. These findings confirmed a vital role of GSDME-mediated pyroptotic cell death in boosting the detrimental effects of chemotherapeutic agents and provide novel insights into improved cancer therapy. Caspase-3 is activated by the apoptotic pathways. Therefore, caspase-3 does not require inflammasome platforms for its activation and subsequent cleavage of GSDME.
In humans and mice, caspase-3 specially cleaves GSDME at the tetrapeptide motif 267DMPD270 [17], while caspase-1, -4, -5, -8 and -11 cleave GSDMD after the 272FLTD275 sequence [42,127]. The cleavage of GSDMD and GSDME by caspases results in the liberation of the N-terminal domains (GSDMD-NT and GSDME-NT) that induce pyroptosis via their pore-forming activity. Caspases-1, -3, -4, -5, -8 and -11 are able to target multiple substrates [128]. Although each caspase possesses its preferred substrate cohort, caspase-1, -4, -5, -8 and -11 could cleave the same substrate GSDMD. The cleavage of GSDMD by caspases is triggered by different stimuli. For instance, caspase-1-mediated cleavage of GSDMD occurs in response to microbial infection or danger signals, while caspase-4, -5 and -11 are activated upon sensing of intracellular LPS to cleave GSDMD. The cleavage of GSDMD by diverse caspases enables cells to initiate pyroptosis under distinct circumstances. Caspase-8 and -3 play a crucial role in initiating cell apoptosis. Reportedly, the Yersinia effector YopJ served as a strong activator of caspase-8 via RIPK1 [129]. Yersinia infection triggered caspase-8-mediated GSDMD cleavage and subsequent pyroptotic cell death, whereas the apoptotic pathway was restrained [127]. Depletion of GSDMD caused the shift from caspase-8-dependent pyroptosis to apoptosis. Several Yersinia effectors were found to repress caspase-1 cleavage [130,131]. This may contribute to the restriction of caspase-1-dependent GSDMD cleavage during Yersinia infection. Overexpression of GSDME in cancer cells switched caspase-3-mediated apoptosis triggered by tumor necrosis factor (TNF) or chemotherapeutic agents to pyroptosis [17]. Thus, caspase activity and the abundance of its substrates may lead to the switch from apoptosis to pyroptosis. In addition, several signaling cascades, such as the type I IFN and toll-like receptor (TLR)-induced signaling pathways, might be involved in shifting from apoptosis to pyroptosis during pathogen infection [132,133]. Interestingly, caspase-3 was reported to promote apoptosis via preventing pyroptosis by inactivating GSDMD [134]. It was proposed that the apoptotic activators could dampen pyroptosis. The inhibition of GSDMD by caspase-3 may act as a negative regulatory feedback mechanism to counteract pyroptosis. Several cell death pathways may exist upon stimulation, and the pyroptotic and apoptotic processes do not act exclusively. Further studies are required to explore the complex interplay between caspase-mediated cell death pathways. Moreover, the dual roles of caspase-3 in pyroptosis await thorough investigation.
Another member of the gasdermin protein family, GSDMD, plays multifaceted roles in cancer pathogenesis. GSDMD promoted the proliferation of NSCLC cells via inhibiting apoptosis by limiting the activation of caspase-3 and poly (ADP-ribose) polymerase (PARP) [135]. However, GSDMD functions oppositely in other types of cancer. For instance, downregulation of GSDMD significantly enhanced the proliferation of GC cells by raising the expression of cell cycle-related proteins, cyclin A2 and cyclin-dependent kinase 2 (CDK2) [136]. The extracellular signal-regulated kinase (ERK), signal transducer and activator of transcription 3 (STAT3) and PI3K/Akt signaling pathways also mediated the anti-proliferative effect of GSDMD. Moreover, adeno-associated virus-mediated delivery of GSDMD caused decreased growth of schwannoma cells [137]. This strategy might be a potential therapeutic approach for clinical treatment of schwannomas.
Pyroptosis has attracted lots of attention, as it may offer potential beneficial effects on therapeutic interventions in cancer. Both GSDMD and GSDME serve an important role in executing pyroptosis. Further studies on these gasdermin family members would be fundamental to adequately dissect the molecular events underlying pyroptotic cell death in cancer. More investigations are required to disclose the precise mechanisms behind GSDMD- and GSDME-mediated pyroptotic pathways, which would provide clues for cancer chemotherapy. GSDMD shows pro-tumorigenic or anti-tumorigenic abilities in different forms of cancer. Thus, it is critical to determine the molecular mechanisms contributing to the distinct impacts of GSDMD on cancer progression. Remarkably, GSDME-mediated pyroptosis may lead to the cytotoxicity of chemotherapy in normal tissues. It is likely that blocking GSDME expression in normal tissues could attenuate the adverse effects of chemotherapeutic drugs. However, further research is warranted to support the clinical utility of GSDME-targeted therapeutics in cancer patients.
7. The Emerging Role of Inflammasome-Dependent Cytokines in Cancer Pathogenesis
IL-1β and IL-18 are stored as inactive proforms that reside in the cytoplasm of naive immune cells [138]. Caspase-1-mediated cleavage of pro-IL-1β and pro-IL-18 occurs during the activation of the inflammasome pathways [139]. However, aberrantly expressed IL-1β and IL-18 contribute to cancer pathology [140]. These two cytokines have emerged as pivotal regulators of tumorigenic processes that may either inhibit or promote tumor occurrence, growth, invasion and metastasis according to the tumor stage, type and microenvironment.
7.1. IL-1β and Cancer
The IL-1 signaling cascade is activated upon the binding of IL-1α or IL-1β to the IL-1 receptor type 1 (IL-1R1), recruiting the IL-1R accessory protein (IL-1RAcP) and the myeloid differentiation primary response protein 88 (MyD88) to the receptor complex [141]. This is followed by the phosphorylation of various kinases and the translocation of NF-ĸB to the nucleus, eventually leading to the activation of inflammatory responses [142]. IL-1 is a key mediator of innate and adaptive immune responses and plays a critical role in sensing microbial invasion and activating lymphoid cell function [143]. More importantly, the pro-inflammatory cytokine IL-1β has significant effects on tumor growth, invasiveness and metastasis. For instance, IL-1β was found to be a master cytokine in the development of breast cancer [144]. Blockage of IL-1β could induce antitumor immunity and resulted in breast cancer regression by activating CD8+ lymphocytes. OSCC-derived IL-1β favored stromal glycolysis and induced a lactate shuttle to cancer cells, which facilitated the proliferation of OSCC cells [145]. IL-1β enhanced the proliferation of osteosarcoma (OS) cells by modifying the NF-ĸB/miR-506/Jagged1 (JAG1) pathway [146]. Reportedly, IL-1β promoted OS cell growth through modulation of the miR-376c/transforming growth factor-α (TGFA) axis [147]. These studies implied that multiple signaling pathways mediated the pro-tumorigenic activity of IL-1β in OS cells.
IL-1β can adjust the malignant characteristics of cancer cells. IL-1β enhanced the stem-like properties of GC cells by promoting the nuclear translocation of metastasis-promoting S100 calcium-binding protein A4 (S100A4) [148]. Consistently, blockage of the IL-1β signaling repressed the EMT process in GC cells by upregulating β-catenin and E-cadherin, and downregulating fibronectin, vimentin, Snail, MMP2 and MMP9 [149]. IL-1β also favored the EMT program in CRC cells by downregulating E-cadherin and upregulating vimentin [150]. The roles of IL-1β in the invasion of breast cancer were extensively explored. The IL-1β response driven by breast cancer prevented the differentiation of metastasis-initiating cancer cells (MICs) into highly proliferative E-cadherin-positive progeny [151]. Conversely, abolishment of the pro-inflammatory response led to metastatic colonization of breast cancer. Another study showed that IL-1β induced the EMT process and promoted the malignancy of breast cancer cells by activating the IL-1β/IL-1R1/β-catenin pathway [152]. Macrophage-derived IL-1β enhanced the migration of breast cancer cells and their adhesion to lymphatic endothelial cells [153]. IL-1β enhanced the invasion of breast cancer cells via upregulating MMP-9 by activating focal adhesion kinase (FAK) and proto-oncogene tyrosine-protein kinase Src [154]. IL-1β could enhance the invasion and migration of esophageal squamous cell carcinoma (ESCC) cells by promoting EMT and inducing the NF-ĸB signaling [155]. IL-1β promoted EMT and metastasis of HCC cells by upregulating hypoxia inducible factor-1α (HIF-1α) [156]. Similarly, IL-1β induced the nuclear import of NF-ĸB as well as enhanced MMP transcription, thus promoting OSCC invasion and progression [157]. IL-1β increased the expression of fascin and promoted extracellular matrix degradation and infiltration into the collagen matrix, hence facilitating OSCC cell invasion [158]. Additionally, IL-1β could increase the expression of glutaredoxin 1 (Grx1) in OSCC cells, thus facilitating the malignant transformation process [159].
The inflammatory environment is essential for the induction of chemoresistance in cancer cells. The molecular mechanisms underlying the role of the IL-1β signaling pathway in cancer chemoresistance have been disclosed. It was found that IL-1β was able to upregulate the chemoresistance-associated gene, the tumor protein 63 (TP63) isoform ∆NP63α, contributing to the acquisition of cisplatin resistance in breast cancer cells [160]. IL-1β conferred doxorubicin resistance to breast cancer cells by elevating the expression of the baculoviral inhibitor of apoptosis repeat-containing 3 (BIRC3), known as an EMT marker [161]. Thus, IL-1β-induced chemoresistance in cancer cells might be attributed to its regulation of the EMT program. IL-1β was able to enhance tamoxifen resistance in breast cancer cells by downregulating the estrogen receptor α (ERα) [152]. Abrogation of IL-1β enabled PDAC cells to regain gemcitabine sensitivity by targeting IL-1R-associated kinase 4 (IRAK4) [162]. Altogether, these studies raise the possibility that the IL-1β signaling could be therapeutically disrupted to improve chemotherapeutic efficacy in cancer patients.
7.2. Therapeutic Potential of IL-1 Neutralization in Cancer
IL-1β is considered as an attractive target in cancer treatment. Three IL-1 blockers, including anakinra, canakinumab and rilonacept, have been approved [163]. The IL-1R antagonist (IL-1Ra) is a natural inhibitor of IL-1β in vivo, where it acts via occupying the IL-1R [164]. Anakinra is molecularly identical to native IL-1Ra [165]. IL-1Ra was able to block the IL-1 signaling in chronic myelogenous leukemia (CML) and inhibited the growth of leukemia stem cells (LSCs) [166]. This study provided a solid basis for further investigation of anti-IL-1 strategies to promote LSC elimination in CML. A randomized phase III trial indicated that the IL-1Ra levels had a significant association with bermekimab responsiveness in patients with advanced CRC [167]. Anakinra overcame erlotinib resistance in HNSCC xenografts but had no effect on the anticancer activity of erlotinib in HNSCC cells [168]. The effectiveness of 5-FU plus bevacizumab and anakinra was assessed in patients with metastatic colorectal cancer (mCRC) [169]. This therapeutic regimen showed good tolerance in mCRC and exhibited efficacy with long-lasting tumor stabilization. Moreover, this combination had a manageable safety profile and might be a promising treatment option for CRC patients. Anakinra plus gemcitabine attenuated the proliferation, invasion and migration of PDAC cells [170]. Combined treatment with anakinra and gemcitabine also obviously reduced the tumor burden in vivo. Therefore, anakinra in combination with gemcitabine might be an effective therapeutic approach for PDAC.
Canakinumab is a human monoclonal antibody targeting IL-1β [171]. Reportedly, anakinra or canakinumab repressed breast cancer cell metastasis, and also blocked cancer cells shed into the circulation in vivo [172]. Anakinra plus canakinumab completely controlled disease activity and inhibited neoplastic recurrence in the patient with refractory Behcet disease uveitis and concomitant bladder papillary carcinoma [173]. The therapeutic potential of canakinumab in lung cancer patients was previously investigated. A significant decline in the incidence of lung cancer was observed in patients that received 150 or 300 mg of canakinumab as compared to the placebo group [174]. Lung cancer mortality was remarkably less frequent in patients assigned to canakinumab than that in patients who received the placebo, with the effect being more prominent in the higher dose (300 mg) group [175]. Rilonacept is a soluble decoy receptor that mainly neutralizes IL-1β [176]. As expected, rilonacept could maintain inflammatory remission in patients enrolled in a clinical trial [177]. Specially, rilonacept treatment caused a rapid and sustained decrease in the severity of inflammatory syndromes [178]. Further clinical studies are demanded to assess the therapeutic effectiveness of rilonacept in cancer.
7.3. IL-18 and Cancer
IL-18 belongs to the IL-1 cytokine family and is constitutively expressed by most cell types including epithelial cells, fibroblasts, macrophages and natural killer (NK) cells [179]. Like IL-1β, IL-18 is activated when cleaved by caspase-1 following inflammasome activation [180]. The pro-inflammatory activity of IL-18 is tuned by its physiological inhibitor IL-18 binding protein (IL-18BP) [181]. IL-18 is involved in the carcinogenesis of multiple cancers. Accumulating evidence indicated that the IL-18 promoter genotype was correlated with the risk of PC, nasopharyngeal carcinoma (NPC), HCC and NSCLC [182,183,184,185]. Moreover, genetic polymorphisms of IL-18 were linked with the prognosis and survival of patients with acute myeloid leukemia (AML) [186]. Upregulation of IL-18 was correlated with poor overall survival in patients with multiple myeloma (MM) [187]. The mechanisms by which this pro-inflammatory cytokine controls cancer progression have been explored. IL-18 restrained the apoptosis of AML cells by elevating the expression of cyclooxygenase-2 (COX-2) [188]. IL-18 mediated estrogen-related receptor α (ERRα)-regulated proliferation and migration of CRC cells [189]. IL-18 promoted OSCC cell invasion and metastasis by reinforcing the EMT process via the Wnt/β-catenin signaling pathway [190]. These studies demonstrated that IL-18 functioned to modify the malignant behaviors of cancer cells. In addition, serum IL-18 levels were evidently lower in patients with pancreatic adenocarcinoma (PA) who had response to gemcitabine-based chemotherapy compared with chemotherapy-unresponsive patients [191]. Serum IL-18 levels might be used to predict the response to gemcitabine-based chemotherapy in PA patients.
It is well-known that IL-18 acts as a critical participant in initiating antitumor immune responses [192]. IL-18 modulates innate and adaptive immune responses through the recruitment or differentiation of immune cells, such as NK cells, T cells and monocytes [179]. Moreover, IL-18 augments IFN-γ production and cytotoxicity of NK cells, T cells and neutrophils [193]. The previous study demonstrated that IL-18 favored the IFN-γ production by CD8+ T cells and NK cells, thereby eliciting antitumor immunity during ESCC carcinogenesis [194]. Accordingly, IL-18 significantly depressed the proliferation and metastasis of ESCC cells [195]. Likewise, IL-18 facilitated the expansion of NK cells and altered their phenotypes in lung cancer [196]. IL-18-induced NK cells might be useful for cancer immunotherapy. Adoptive transfer of T cells engineered with a melanoma-specific T cell receptor (TCR) and inducible IL-18 resulted in enhanced antitumor T cell responses, hence suppressing melanoma growth in vivo [197]. Thus, IL-18 improved the anticancer activity of dacarbazine in malignant melanoma [198]. IL-18 served a suppressive role in HCC progression by enhancing the differentiation, activity and survival of tumor-infiltrating T cells [199]. Furthermore, IL-18 inhibited HCC growth by priming NK cells trafficked to the liver [200]. Mesenchymal stem cells-expressing IL-18 inhibited the proliferation and metastasis of breast cancer cells by activating immunocytes and immune cytokines, downregulating the proliferation marker Ki-67 and suppressing tumor angiogenesis [201]. Collectively, IL-18-based immunotherapy might be a promising therapeutic strategy for cancer.
On the contrary, IL-18 can compromise host immune responses in favor of cancer evasion. PC cell-derived IL-18 boosted the differentiation of naive B cells into regulatory B cells (Bregs) and ascended expression of programmed cell death-ligand 1 (PD-L1) in Bregs, which led to PC immune tolerance [202]. Paradoxically, IL-18 enhanced the cytotoxic activity of NK cells and T cells in PC-transplanted mice [203]. However, IL-18 enhanced the proliferation and invasion of PC cells through the NF-ĸB signaling pathway. When combined with the NF-ĸB inhibitor, IL-18 exhibited a therapeutic effect on PC. It seemed that multiple pathways simultaneously participated in IL-18-regulated PC progression. The complex interplay among these pathways might determine the final effects of IL-18 on cancer pathogenesis. Breast cancer-derived IL-18 triggered programmed cell death-1 (PD-1) expression on immunosuppressive NK cells and was associated with poor prognosis in patients with triple-negative breast cancer [204]. As expected, IL-18 was implicated in leptin-enhanced breast cancer cell invasion and migration [205]. Thus, IL-18 could drive breast cancer progression by inducing PD-1-dependent immunosuppression.
7.4. Potential Efficacy of Anti-IL-18 in Cancer Therapy
IL-18 shows anticancer activity in different pre-clinical models of cancer immunotherapy through the activation of NK and/or T cell responses [206]. Clinical studies have been conducted to assess the therapeutic efficacy of IL-18 in cancer patients. Ten melanoma patients and nine RCC patients were enrolled in a previous study and were assigned to different doses (100, 500, 1000 or 2000 μg/kg) of IL-18 [207]. No dose-limiting toxicity was observed. Notably, IL-18 exhibited immune regulatory activity in these patients. In a phase I clinical trial, twenty-one RCC patients, six melanoma patients and one patient with Hodgkin lymphoma were given IL-18 in doses ranging from 3 to 1000 μg/kg [208]. Only one patient administrated with 100 μg/kg IL-18 experienced transient hypotension and bradycardia during the first infusion. No other dose-limiting toxicity was observed. IL-18 administration could effectively activate immune cells (lymphocytes and monocytes). Moreover, the serum levels of IFN-γ, granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-18BP and soluble Fas ligand (FasL) were elevated in these patients. Thus, IL-18 had biological effects on the immune system and might be effective in treating cancer. In a phase 2 randomized study, IL-18 was well tolerated and exhibited low toxicity in 64 patients with metastatic melanoma [209].
However, IL-18 had limited therapeutic efficacy as a single agent in cancer patients. Previously, nineteen patients with non-Hodgkin lymphoma were given rituximab in combination with IL-18 at doses of 1, 3, 10, 20, 30 and 100 μg/kg [210]. This combination elevated the expression of IFN-γ, GM-CSF, and chemokines. Moreover, objective tumor responses could be observed in five patients. IL-18 (3 μg/kg) plus pegylated liposomal doxorubicin (PLD) was safe and biologically active in sixteen patients with recurrent ovarian cancer [211]. IL-18 may be used as an immune-stimulatory molecule in combined therapy with conventional chemotherapeutic agents. Intriguingly, IL-18 plays a pro-carcinogenic role in several types of cancer. Under the condition that IL-18 is harmful, the utilization of IL-18BP to neutralize IL-18 may be a potential therapeutic approach for certain types of cancer. A previous study showed that the IL-18BP-Fc therapy restrained the lung metastasis of breast cancer cells by blocking tumor-released IL-18 [212]. IL-18BP may be an alternative treatment option for cancer patients. These promising results may propel further investigation of the clinical utility of IL-18-based therapy in cancer intervention.
8. Conclusions
Pyroptosis, a lytic form of programmed cell death, is widely accepted as a crucial host defense mechanism against pathogen invasion. The biological functions of the pyroptotic pathways in cancer pathogenesis have gained increasing attention in recent years. Inflammasomes, gasdermins and inflammasome-dependent cytokines play a critical role in the carcinogenesis, growth, invasion, metastasis and chemoresistance of cancer cells. The broad and complicated impacts of pyroptotic cell death pathways on cancer development are mainly attributed to their regulatory effects on apoptosis-, EMT- or immune-related signaling cascades. To systematically understand the pivotal roles of pyroptosis in cancer, numerous questions must be addressed. The complex signaling mechanisms responsible for the regulation of pyroptosis in cancer cells has yet to be fully deciphered. Therefore, a deeper investigation into this mode of cell death is urgently required, either alone or alongside other cell death processes including necrosis and apoptosis. Further studies are warranted to disclose the underlying mechanisms of pyroptosis as well as its exact functions in cancer pathogenesis. The inflammasomes and pro-inflammatory cytokines act as a double-edged sword in cancer occurrence and development. It is likely that the functions of these critical components of the pyroptotic pathways in carcinogenesis differ depending on various factors, such as cell or tissue type, and tumor stage. Therefore, it is essential to disclose the pro-carcinogenic and anti-carcinogenic mechanisms by which the pyroptotic pathways orchestrate different stages of cancer development. In addition, various inflammasomes are present in cancer cells. Further studies are required to figure out how specific inflammasomes are activated or how they interact with each other during cancer progression. Furthermore, the influences of each inflammasome on host antitumor immunity and cancer immunotherapy are awaiting elucidation.
A growing number of studies have proven the regulatory roles of inflammasome-dependent cytokines (IL-1β and IL-18) in cancer development. Both IL-1β and IL-18 possess the ability to govern the antitumor immunity. Nevertheless, the detailed mechanisms by which these cytokines affect antitumor immunity and remodel the tumor microenvironment merit further investigation. Multiple types of cell, including tumor cells and stromal cells, can produce and release IL-1β and IL-18 into the tumor microenvironment. The precise function of the two cytokines secreted by diverse cells in modifying the inflammatory milieu should be characterized in further studies. The regulatory mechanisms underlying the maturation and secretion of IL-1β and IL-18 into the tumor microenvironment require profound elucidation. It is well established that the pyroptotic pathways can drive the maturation and secretion of IL-1β and IL-18. However, the significance of pyroptosis in the production of IL-1β and IL-18 remains to be further explored. In addition, the molecular mechanisms mediating the pro- or anti-carcinogenic roles of IL-1β and IL-18 deserve systematical investigation. Conventional chemotherapeutic agents are able to trigger caspase-3-induced pyroptosis in cancer cells. The regulation of pyroptotic cell death pathways in combined with chemotherapeutic drugs would be a promising therapeutic strategy for cancer. At present, only a few literatures have addressed the activation of pyroptosis by chemotherapy. The molecular mechanisms behind the activation of pyroptosis in chemotherapy-treated cancer cells await thorough elucidation. In particular, the signaling pathways that control the transition from chemotherapy-induced apoptosis to pyroptosis still need to be fully deciphered. Additional efforts should focus on comprehensively delineating the mechanisms of action for the induction of pyroptotic cell death in cancer intervention. Both GSDMD and GSDME are responsible for executing pyroptosis via their pore-forming activity. More work is demanded to explore how GSDMD- or GSDME-mediated pyroptotic pathways are selectively activated by different stimuli. It is intriguing whether GSDMD-induced pyroptosis occurs in cancer cells. The factors accounting for the switch between the two pyroptotic pathways should also be identified. Collectively, a better understanding of the molecular mechanisms underlying pyroptotic cell death will be conducive to the development of alternative therapeutic strategies for cancer treatment.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6694/11/9/1313/s1, Table S1: List of abbreviations used in this review.
Author Contributions
M.W. and K.W. conceived and designed the study; M.W. drafted the manuscript; M.W., S.J. and Y.Z. prepared the figures; and P.L. and K.W. revised the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China (81701991) and Applied Basic Research Programs of Qingdao, China (17-1-1-59-jch).
Acknowledgments
The authors would like to thank the editor and three anonymous reviewers for their constructive and insightful comments that greatly improved this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bergsbaken, T.; Fink, S.L.; Cookson, B.T. Pyroptosis: Host Cell Death and Inflammation. Nat. Rev. Microbiol. 2009, 7, 99–109. [Google Scholar] [CrossRef]
- D’Arcy, M.S. Cell Death: A Review of the Major Forms of Apoptosis, Necrosis and Autophagy. Cell Biol. Int. 2019, 43, 582–592. [Google Scholar] [CrossRef]
- He, Y.; Amer, A.O. Microbial Modulation of Host Apoptosis and Pyroptosis. Front. Cell Infect. Microbiol. 2014, 4, 83. [Google Scholar] [CrossRef]
- Sharma, D.; Kanneganti, T.D. Inflammatory Cell Death in Intestinal Pathologies. Immunol. Rev. 2017, 280, 57–73. [Google Scholar] [CrossRef]
- Fearnhead, H.O.; Rodriguez, J.; Govek, E.E.; Guo, W.; Kobayashi, R.; Hannon, G.; Lazebnik, Y.A. Oncogene-dependent Apoptosis is Mediated by Caspase-9. Proc. Natl. Acad. Sci. USA 1998, 95, 13664–13669. [Google Scholar] [CrossRef]
- Ruhl, S.; Shkarina, K.; Demarco, B.; Heilig, R.; Santos, J.C.; Broz, P. ESCRT-dependent Membrane Repair Negatively Regulates Pyroptosis Downstream of GSDMD Activation. Science 2018, 362, 956–960. [Google Scholar] [CrossRef]
- Weinlich, R.; Oberst, A.; Beere, H.M.; Green, D.R. Necroptosis in Development, Inflammation and Disease. Nat. Rev. Mol. Cell Biol. 2017, 18, 127–136. [Google Scholar] [CrossRef]
- Dhuriya, Y.K.; Sharma, D. Necroptosis: A Regulated Inflammatory Mode of Cell Death. J. Neuroinflamm. 2018, 15, 199. [Google Scholar] [CrossRef]
- Gong, Y.N.; Guy, C.; Crawford, J.C.; Green, D.R. Biological Events and Molecular Signaling following MLKL Activation during Necroptosis. Cell Cycle 2017, 16, 1748–1760. [Google Scholar] [CrossRef]
- Grootjans, S.; Vanden Berghe, T.; Vandenabeele, P. Initiation and Execution Mechanisms of Necroptosis: An Overview. Cell Death Differ. 2017, 24, 1184–1195. [Google Scholar] [CrossRef]
- Gaidt, M.M.; Hornung, V. Pore Formation by GSDMD is the Effector Mechanism of Pyroptosis. EMBO J. 2016, 35, 2167–2169. [Google Scholar] [CrossRef]
- Man, S.M.; Kanneganti, T.D. Gasdermin D: The Long-awaited Executioner of Pyroptosis. Cell Res. 2015, 25, 1183–1184. [Google Scholar] [CrossRef]
- Shi, J.; Zhao, Y.; Wang, Y.; Gao, W.; Ding, J.; Li, P.; Hu, L.; Shao, F. Inflammatory caspases are innate immune receptors for intracellular LPS. Nature 2014, 514, 187–192. [Google Scholar] [CrossRef]
- Kayagaki, N.; Stowe, I.B.; Lee, B.L.; O’Rourke, K.; Anderson, K.; Warming, S.; Cuellar, T.; Haley, B.; Roose-Girma, M.; Phung, Q.T.; et al. Caspase-11 cleaves gasdermin D for non-canonical inflammasome signalling. Nature 2015, 526, 666–671. [Google Scholar] [CrossRef]
- Xia, X.; Wang, X.; Zheng, Y.; Jiang, J.; Hu, J. What role does pyroptosis play in microbial infection? J. Cell. Physiol. 2019, 234, 7885–7892. [Google Scholar] [CrossRef]
- Man, S.M.; Karki, R.; Kanneganti, T.D. Molecular mechanisms and functions of pyroptosis, inflammatory caspases and inflammasomes in infectious diseases. Immunol. Rev. 2017, 277, 61–75. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Gao, W.; Shi, X.; Ding, J.; Liu, W.; He, H.; Wang, K.; Shao, F. Chemotherapy drugs induce pyroptosis through caspase-3 cleavage of a gasdermin. Nature 2017, 547, 99–103. [Google Scholar] [CrossRef]
- Zhang, C.C.; Li, C.G.; Wang, Y.F.; Xu, L.H.; He, X.H.; Zeng, Q.Z.; Zeng, C.Y.; Mai, F.Y.; Hu, B.; Ouyang, D.Y. Chemotherapeutic paclitaxel and cisplatin differentially induce pyroptosis in A549 lung cancer cells via caspase-3/GSDME activation. Apoptosis 2019, 24, 312–325. [Google Scholar] [CrossRef]
- Bauernfeind, F.; Hornung, V. Of inflammasomes and pathogens—Sensing of microbes by the inflammasome. EMBO Mol. Med. 2013, 5, 814–826. [Google Scholar] [CrossRef]
- Stowe, I.; Lee, B.; Kayagaki, N. Caspase-11: Arming the guards against bacterial infection. Immunol. Rev. 2015, 265, 75–84. [Google Scholar] [CrossRef]
- Fernandes-Alnemri, T.; Wu, J.; Yu, J.W.; Datta, P.; Miller, B.; Jankowski, W.; Rosenberg, S.; Zhang, J.; Alnemri, E.S. The pyroptosome: a supramolecular assembly of ASC dimers mediating inflammatory cell death via caspase-1 activation. Cell Death Differ. 2007, 14, 1590–1604. [Google Scholar] [CrossRef]
- Schroder, K.; Tschopp, J. The inflammasomes. Cell 2010, 140, 821–832. [Google Scholar] [CrossRef]
- Sharma, D.; Kanneganti, T.D. The cell biology of inflammasomes: Mechanisms of inflammasome activation and regulation. J. Cell Biol. 2016, 213, 617–629. [Google Scholar] [CrossRef] [Green Version]
- Rubartelli, A.; Lotze, M.T. Inside, outside, upside down: damage-associated molecular-pattern molecules (DAMPs) and redox. Trends Immunol. 2007, 28, 429–436. [Google Scholar] [CrossRef]
- Davis, B.K.; Wen, H.; Ting, J.P. The inflammasome NLRs in immunity, inflammation, and associated diseases. Annu. Rev. Immunol. 2011, 29, 707–735. [Google Scholar] [CrossRef]
- Sharma, N.; Jha, S. NLR-regulated pathways in cancer: Opportunities and obstacles for therapeutic interventions. Cell. Mol. Life Sci. CMLS 2016, 73, 1741–1764. [Google Scholar] [CrossRef]
- Awad, F.; Assrawi, E.; Jumeau, C.; Georgin-Lavialle, S.; Cobret, L.; Duquesnoy, P.; Piterboth, W.; Thomas, L.; Stankovic-Stojanovic, K.; Louvrier, C.; et al. Impact of human monocyte and macrophage polarization on NLR expression and NLRP3 inflammasome activation. PLoS ONE 2017, 12, e0175336. [Google Scholar] [CrossRef]
- Caneparo, V.; Landolfo, S.; Gariglio, M.; De Andrea, M. The Absent in Melanoma 2-Like Receptor IFN-Inducible Protein 16 as an Inflammasome Regulator in Systemic Lupus Erythematosus: The Dark Side of Sensing Microbes. Front. Immunol. 2018, 9, 1180. [Google Scholar] [CrossRef]
- Man, S.M.; Karki, R.; Kanneganti, T.D. AIM2 inflammasome in infection, cancer, and autoimmunity: Role in DNA sensing, inflammation, and innate immunity. Eur. J. Immunol. 2016, 46, 269–280. [Google Scholar] [CrossRef]
- Lee, J.; Li, L.; Gretz, N.; Gebert, J.; Dihlmann, S. Absent in Melanoma 2 (AIM2) is an important mediator of interferon-dependent and -independent HLA-DRA and HLA-DRB gene expression in colorectal cancers. Oncogene 2012, 31, 1242–1253. [Google Scholar] [CrossRef]
- Yu, J.W.; Wu, J.; Zhang, Z.; Datta, P.; Ibrahimi, I.; Taniguchi, S.; Sagara, J.; Fernandes-Alnemri, T.; Alnemri, E.S. Cryopyrin and pyrin activate caspase-1, but not NF-kappaB, via ASC oligomerization. Cell Death Differ. 2006, 13, 236–249. [Google Scholar] [CrossRef]
- De Torre-Minguela, C.; Mesa Del Castillo, P.; Pelegrin, P. The NLRP3 and Pyrin Inflammasomes: Implications in the Pathophysiology of Autoinflammatory Diseases. Front. Immunol. 2017, 8, 43. [Google Scholar] [CrossRef] [Green Version]
- Garib, F.Y.; Rizopulu, A.P.; Kuchmiy, A.A.; Garib, V.F. Inactivation of Inflammasomes by Pathogens Regulates Inflammation. Biochem. Biokhimiia 2016, 81, 1326–1339. [Google Scholar] [CrossRef]
- Levinsohn, J.L.; Newman, Z.L.; Hellmich, K.A.; Fattah, R.; Getz, M.A.; Liu, S.; Sastalla, I.; Leppla, S.H.; Moayeri, M. Anthrax lethal factor cleavage of Nlrp1 is required for activation of the inflammasome. PLoS Pathog. 2012, 8, e1002638. [Google Scholar] [CrossRef]
- Hellmich, K.A.; Levinsohn, J.L.; Fattah, R.; Newman, Z.L.; Maier, N.; Sastalla, I.; Liu, S.; Leppla, S.H.; Moayeri, M. Anthrax lethal factor cleaves mouse nlrp1b in both toxin-sensitive and toxin-resistant macrophages. PLoS ONE 2012, 7, e49741. [Google Scholar] [CrossRef]
- Qu, Y.; Misaghi, S.; Izrael-Tomasevic, A.; Newton, K.; Gilmour, L.L.; Lamkanfi, M.; Louie, S.; Kayagaki, N.; Liu, J.; Komuves, L.; et al. Phosphorylation of NLRC4 is critical for inflammasome activation. Nature 2012, 490, 539–542. [Google Scholar] [CrossRef]
- Morrone, S.R.; Matyszewski, M.; Yu, X.; Delannoy, M.; Egelman, E.H.; Sohn, J. Assembly-driven activation of the AIM2 foreign-dsDNA sensor provides a polymerization template for downstream ASC. Nat. Commun. 2015, 6, 7827. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Magnotti, F.; Belot, A.; Henry, T. The pyrin inflammasome: from sensing RhoA GTPases-inhibiting toxins to triggering autoinflammatory syndromes. Pathog. Dis. 2018, 76, fty020. [Google Scholar] [CrossRef]
- Lu, A.; Magupalli, V.G.; Ruan, J.; Yin, Q.; Atianand, M.K.; Vos, M.R.; Schroder, G.F.; Fitzgerald, K.A.; Wu, H.; Egelman, E.H. Unified polymerization mechanism for the assembly of ASC-dependent inflammasomes. Cell 2014, 156, 1193–1206. [Google Scholar] [CrossRef]
- Srinivasula, S.M.; Poyet, J.L.; Razmara, M.; Datta, P.; Zhang, Z.; Alnemri, E.S. The PYRIN-CARD protein ASC is an activating adaptor for caspase-1. J. Biol. Chem. 2002, 277, 21119–21122. [Google Scholar] [CrossRef]
- Malik, A.; Kanneganti, T.D. Inflammasome activation and assembly at a glance. J. Cell Sci. 2017, 130, 3955–3963. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Zhao, Y.; Wang, K.; Shi, X.; Wang, Y.; Huang, H.; Zhuang, Y.; Cai, T.; Wang, F.; Shao, F. Cleavage of GSDMD by inflammatory caspases determines pyroptotic cell death. Nature 2015, 526, 660–665. [Google Scholar] [CrossRef]
- Ding, J.; Wang, K.; Liu, W.; She, Y.; Sun, Q.; Shi, J.; Sun, H.; Wang, D.C.; Shao, F. Pore-forming activity and structural autoinhibition of the gasdermin family. Nature 2016, 535, 111–116. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Z.; Ruan, J.; Pan, Y.; Magupalli, V.G.; Wu, H.; Lieberman, J. Inflammasome-activated gasdermin D causes pyroptosis by forming membrane pores. Nature 2016, 535, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, S.B.; Miao, E.A. Gasdermins: Effectors of Pyroptosis. Trends Cell Biol. 2017, 27, 673–684. [Google Scholar] [CrossRef]
- Ruan, J.; Xia, S.; Liu, X.; Lieberman, J.; Wu, H. Cryo-EM structure of the gasdermin A3 membrane pore. Nature 2018, 557, 62–67. [Google Scholar] [CrossRef]
- Kepp, O.; Galluzzi, L.; Zitvogel, L.; Kroemer, G. Pyroptosis—A cell death modality of its kind? Eur. J. Immunol. 2010, 40, 627–630. [Google Scholar] [CrossRef]
- Banerjee, I.; Behl, B.; Mendonca, M.; Shrivastava, G.; Russo, A.J.; Menoret, A.; Ghosh, A.; Vella, A.T.; Vanaja, S.K.; Sarkar, S.N.; et al. Gasdermin D Restrains Type I Interferon Response to Cytosolic DNA by Disrupting Ionic Homeostasis. Immunity 2018, 49, 413–426.e5. [Google Scholar] [CrossRef] [Green Version]
- Munoz-Planillo, R.; Kuffa, P.; Martinez-Colon, G.; Smith, B.L.; Rajendiran, T.M.; Nunez, G. K(+) efflux is the common trigger of NLRP3 inflammasome activation by bacterial toxins and particulate matter. Immunity 2013, 38, 1142–1153. [Google Scholar] [CrossRef]
- Ruhl, S.; Broz, P. Caspase-11 activates a canonical NLRP3 inflammasome by promoting K(+) efflux. Eur. J. Immunol. 2015, 45, 2927–2936. [Google Scholar] [CrossRef]
- Monteleone, M.; Stow, J.L.; Schroder, K. Mechanisms of unconventional secretion of IL-1 family cytokines. Cytokine 2015, 74, 213–218. [Google Scholar] [CrossRef]
- Monteleone, M.; Stanley, A.C.; Chen, K.W.; Brown, D.L.; Bezbradica, J.S.; von Pein, J.B.; Holley, C.L.; Boucher, D.; Shakespear, M.R.; Kapetanovic, R.; et al. Interleukin-1beta Maturation Triggers Its Relocation to the Plasma Membrane for Gasdermin-D-Dependent and -Independent Secretion. Cell Rep. 2018, 24, 1425–1433. [Google Scholar] [CrossRef]
- Gutierrez, K.D.; Davis, M.A.; Daniels, B.P.; Olsen, T.M.; Ralli-Jain, P.; Tait, S.W.; Gale, M., Jr.; Oberst, A. MLKL Activation Triggers NLRP3-Mediated Processing and Release of IL-1beta Independently of Gasdermin-D. J. Immunol. 2017, 198, 2156–2164. [Google Scholar] [CrossRef]
- Kayagaki, N.; Warming, S.; Lamkanfi, M.; Vande Walle, L.; Louie, S.; Dong, J.; Newton, K.; Qu, Y.; Liu, J.; Heldens, S.; et al. Non-canonical inflammasome activation targets caspase-11. Nature 2011, 479, 117–121. [Google Scholar] [CrossRef]
- He, W.T.; Wan, H.; Hu, L.; Chen, P.; Wang, X.; Huang, Z.; Yang, Z.H.; Zhong, C.Q.; Han, J. Gasdermin D is an executor of pyroptosis and required for interleukin-1beta secretion. Cell Res. 2015, 25, 1285–1298. [Google Scholar] [CrossRef]
- Sarhan, J.; Liu, B.C.; Muendlein, H.I.; Li, P.; Nilson, R.; Tang, A.Y.; Rongvaux, A.; Bunnell, S.C.; Shao, F.; Green, D.R.; et al. Caspase-8 induces cleavage of gasdermin D to elicit pyroptosis during Yersinia infection. Proc. Natl. Acad. Sci. USA 2018, 115, E10888–E10897. [Google Scholar] [CrossRef]
- Kolb, R.; Liu, G.H.; Janowski, A.M.; Sutterwala, F.S.; Zhang, W. Inflammasomes in cancer: A double-edged sword. Protein Cell 2014, 5, 12–20. [Google Scholar] [CrossRef]
- Di Virgilio, F. The therapeutic potential of modifying inflammasomes and NOD-like receptors. Pharmacol. Rev. 2013, 65, 872–905. [Google Scholar] [CrossRef]
- Jo, E.K.; Kim, J.K.; Shin, D.M.; Sasakawa, C. Molecular mechanisms regulating NLRP3 inflammasome activation. Cell. Mol. Immunol. 2016, 13, 148–159. [Google Scholar] [CrossRef]
- Chen, M.; Wang, H.; Chen, W.; Meng, G. Regulation of adaptive immunity by the NLRP3 inflammasome. Int. Immunopharmacol. 2011, 11, 549–554. [Google Scholar] [CrossRef]
- Moossavi, M.; Parsamanesh, N.; Bahrami, A.; Atkin, S.L.; Sahebkar, A. Role of the NLRP3 inflammasome in cancer. Mol. Cancer 2018, 17, 158. [Google Scholar] [CrossRef]
- Chen, L.; Huang, C.F.; Li, Y.C.; Deng, W.W.; Mao, L.; Wu, L.; Zhang, W.F.; Zhang, L.; Sun, Z.J. Blockage of the NLRP3 inflammasome by MCC950 improves anti-tumor immune responses in head and neck squamous cell carcinoma. Cell. Mol. Life Sci. CMLS 2018, 75, 2045–2058. [Google Scholar] [CrossRef]
- Huang, C.F.; Chen, L.; Li, Y.C.; Wu, L.; Yu, G.T.; Zhang, W.F.; Sun, Z.J. NLRP3 inflammasome activation promotes inflammation-induced carcinogenesis in head and neck squamous cell carcinoma. J. Exp. Clin. Cancer Res. 2017, 36, 116. [Google Scholar] [CrossRef]
- Duan, S.; Wang, N.; Huang, L.; Shao, H.; Zhang, P.; Wang, W.; Wu, Y.; Wang, J.; Liu, H.; Zhang, Q.; et al. NLRP3 inflammasome activation involved in LPS and coal tar pitch extract-induced malignant transformation of human bronchial epithelial cells. Environ. Toxicol. 2019, 34, 585–593. [Google Scholar] [CrossRef]
- Huang, L.; Duan, S.; Shao, H.; Zhang, A.; Chen, S.; Zhang, P.; Wang, N.; Wang, W.; Wu, Y.; Wang, J.; et al. NLRP3 deletion inhibits inflammation-driven mouse lung tumorigenesis induced by benzo(a)pyrene and lipopolysaccharide. Respir. Res. 2019, 20, 20. [Google Scholar] [CrossRef]
- Zhang, L.; Li, H.; Zang, Y.; Wang, F. NLRP3 inflammasome inactivation driven by miR2233p reduces tumor growth and increases anticancer immunity in breast cancer. Mol. Med. Rep. 2019, 19, 2180–2188. [Google Scholar] [CrossRef]
- Daley, D.; Mani, V.R.; Mohan, N.; Akkad, N.; Pandian, G.; Savadkar, S.; Lee, K.B.; Torres-Hernandez, A.; Aykut, B.; Diskin, B.; et al. NLRP3 signaling drives macrophage-induced adaptive immune suppression in pancreatic carcinoma. J. Exp. Med. 2017, 214, 1711–1724. [Google Scholar] [CrossRef] [Green Version]
- Raut, P.K.; Kim, S.H.; Choi, D.Y.; Jeong, G.S.; Park, P.H. Growth of breast cancer cells by leptin is mediated via activation of the inflammasome: Critical roles of estrogen receptor signaling and reactive oxygen species production. Biochem. Pharmacol. 2019, 161, 73–88. [Google Scholar] [CrossRef]
- Zhao, X.; Zhang, C.; Hua, M.; Wang, R.; Zhong, C.; Yu, J.; Han, F.; He, N.; Zhao, Y.; Liu, G.; et al. NLRP3 inflammasome activation plays a carcinogenic role through effector cytokine IL-18 in lymphoma. Oncotarget 2017, 8, 108571–108583. [Google Scholar] [CrossRef] [Green Version]
- Wei, Q.; Zhu, R.; Zhu, J.; Zhao, R.; Li, M. E2-induced activation of the NLRP3 inflammasome triggers pyroptosis and inhibits autophagy in HCC cells. Oncol. Res. 2019, 27, 827–834. [Google Scholar] [CrossRef]
- Pastushenko, I.; Blanpain, C. EMT Transition States during Tumor Progression and Metastasis. Trends Cell Biol. 2019, 29, 212–226. [Google Scholar] [CrossRef]
- Yeung, K.T.; Yang, J. Epithelial-mesenchymal transition in tumor metastasis. Mol. Oncol. 2017, 11, 28–39. [Google Scholar] [CrossRef]
- Deng, Q.; Geng, Y.; Zhao, L.; Li, R.; Zhang, Z.; Li, K.; Liang, R.; Shao, X.; Huang, M.; Zuo, D.; et al. NLRP3 inflammasomes in macrophages drive colorectal cancer metastasis to the liver. Cancer Lett. 2019, 442, 21–30. [Google Scholar] [CrossRef]
- Wang, H.; Wang, Y.; Du, Q.; Lu, P.; Fan, H.; Lu, J.; Hu, R. Inflammasome-independent NLRP3 is required for epithelial-mesenchymal transition in colon cancer cells. Exp. Cell Res. 2016, 342, 184–192. [Google Scholar] [CrossRef]
- Hu, H.; Wang, Y.; Ding, X.; He, Y.; Lu, Z.; Wu, P.; Tian, L.; Yuan, H.; Liu, D.; Shi, G.; et al. Long non-coding RNA XLOC_000647 suppresses progression of pancreatic cancer and decreases epithelial-mesenchymal transition-induced cell invasion by down-regulating NLRP3. Mol. Cancer 2018, 17, 18. [Google Scholar] [CrossRef]
- Wang, H.; Luo, Q.; Feng, X.; Zhang, R.; Li, J.; Chen, F. NLRP3 promotes tumor growth and metastasis in human oral squamous cell carcinoma. BMC Cancer 2018, 18, 500. [Google Scholar] [CrossRef]
- Yin, X.F.; Zhang, Q.; Chen, Z.Y.; Wang, H.F.; Li, X.; Wang, H.X.; Li, H.X.; Kang, C.M.; Chu, S.; Li, K.F.; et al. NLRP3 in human glioma is correlated with increased WHO grade, and regulates cellular proliferation, apoptosis and metastasis via epithelial-mesenchymal transition and the PTEN/AKT signaling pathway. Int. J. Oncol. 2018, 53, 973–986. [Google Scholar] [CrossRef] [Green Version]
- Zou, J.; Yang, Y.; Yang, Y.; Liu, X. Polydatin suppresses proliferation and metastasis of non-small cell lung cancer cells by inhibiting NLRP3 inflammasome activation via NF-kappaB pathway. Biomed. Pharmacother. 2018, 108, 130–136. [Google Scholar] [CrossRef]
- Wang, Y.; Kong, H.; Zeng, X.; Liu, W.; Wang, Z.; Yan, X.; Wang, H.; Xie, W. Activation of NLRP3 inflammasome enhances the proliferation and migration of A549 lung cancer cells. Oncol. Rep. 2016, 35, 2053–2064. [Google Scholar] [CrossRef] [Green Version]
- Hu, Q.; Zhao, F.; Guo, F.; Wang, C.; Fu, Z. Polymeric Nanoparticles Induce NLRP3 Inflammasome Activation and Promote Breast Cancer Metastasis. Macromol. Biosci. 2017, 17, 1700273. [Google Scholar] [CrossRef]
- Shang, S.; Wang, L.; Zhang, Y.; Lu, H.; Lu, X. The Beta-Hydroxybutyrate Suppresses the Migration of Glioma Cells by Inhibition of NLRP3 Inflammasome. Cell. Mol. Neurobiol. 2018, 38, 1479–1489. [Google Scholar] [CrossRef]
- Wang, Y.C.; Li, W.Z.; Wu, Y.; Yin, Y.Y.; Dong, L.Y.; Chen, Z.W.; Wu, W.N. Acid-sensing ion channel 1a contributes to the effect of extracellular acidosis on NLRP1 inflammasome activation in cortical neurons. J. Neuroinflamm. 2015, 12, 246. [Google Scholar] [CrossRef]
- Verma, D.; Bivik, C.; Farahani, E.; Synnerstad, I.; Fredrikson, M.; Enerback, C.; Rosdahl, I.; Soderkvist, P. Inflammasome polymorphisms confer susceptibility to sporadic malignant melanoma. Pigment Cell Melanoma Res. 2012, 25, 506–513. [Google Scholar] [CrossRef] [Green Version]
- Zhong, F.L.; Mamai, O.; Sborgi, L.; Boussofara, L.; Hopkins, R.; Robinson, K.; Szeverenyi, I.; Takeichi, T.; Balaji, R.; Lau, A.; et al. Germline NLRP1 Mutations Cause Skin Inflammatory and Cancer Susceptibility Syndromes via Inflammasome Activation. Cell 2016, 167, 187–202.e17. [Google Scholar] [CrossRef] [Green Version]
- Zhai, Z.; Liu, W.; Kaur, M.; Luo, Y.; Domenico, J.; Samson, J.M.; Shellman, Y.G.; Norris, D.A.; Dinarello, C.A.; Spritz, R.A.; et al. NLRP1 promotes tumor growth by enhancing inflammasome activation and suppressing apoptosis in metastatic melanoma. Oncogene 2017, 36, 3820–3830. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.L.; Mirrashidi, K.M.; Stowe, I.B.; Kummerfeld, S.K.; Watanabe, C.; Haley, B.; Cuellar, T.L.; Reichelt, M.; Kayagaki, N. ASC- and caspase-8-dependent apoptotic pathway diverges from the NLRC4 inflammasome in macrophages. Sci. Rep. 2018, 8, 3788. [Google Scholar] [CrossRef]
- Hu, B.; Elinav, E.; Flavell, R.A. Inflammasome-mediated suppression of inflammation-induced colorectal cancer progression is mediated by direct regulation of epithelial cell proliferation. Cell Cycle 2011, 10, 1936–1939. [Google Scholar] [CrossRef] [Green Version]
- Papin, S.; Cuenin, S.; Agostini, L.; Martinon, F.; Werner, S.; Beer, H.D.; Grutter, C.; Grutter, M.; Tschopp, J. The SPRY domain of Pyrin, mutated in familial Mediterranean fever patients, interacts with inflammasome components and inhibits proIL-1beta processing. Cell Death Differ. 2007, 14, 1457–1466. [Google Scholar] [CrossRef]
- Richards, N.; Schaner, P.; Diaz, A.; Stuckey, J.; Shelden, E.; Wadhwa, A.; Gumucio, D.L. Interaction between pyrin and the apoptotic speck protein (ASC) modulates ASC-induced apoptosis. J. Biol. Chem. 2001, 276, 39320–39329. [Google Scholar] [CrossRef]
- Sharma, D.; Malik, A.; Guy, C.S.; Karki, R.; Vogel, P.; Kanneganti, T.D. Pyrin Inflammasome Regulates Tight Junction Integrity to Restrict Colitis and Tumorigenesis. Gastroenterology 2018, 154, 948–964.e8. [Google Scholar] [CrossRef]
- Hornung, V.; Ablasser, A.; Charrel-Dennis, M.; Bauernfeind, F.; Horvath, G.; Caffrey, D.R.; Latz, E.; Fitzgerald, K.A. AIM2 recognizes cytosolic dsDNA and forms a caspase-1-activating inflammasome with ASC. Nature 2009, 458, 514–518. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Dong, X.; Yang, X.; Wan, D.; Sun, L.; Gu, M.; Li, M.; Zhu, Z.; Wang, J.; Shang, Z.; et al. Expression and clinical significance of absent in melanoma 2 in colorectal cancer. Biomed. Pharmacother. 2017, 94, 843–849. [Google Scholar] [CrossRef]
- Martinez-Cardona, C.; Lozano-Ruiz, B.; Bachiller, V.; Peiro, G.; Algaba-Chueca, F.; Gomez-Hurtado, I.; Such, J.; Zapater, P.; Frances, R.; Gonzalez-Navajas, J.M. AIM2 deficiency reduces the development of hepatocellular carcinoma in mice. Int. J. Cancer 2018, 143, 2997–3007. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Jin, C.; Yang, Y.; Wang, K.; Zhou, Y.; Zhou, Y.; Wang, R.; Li, T.; Hu, R. AIM2 promotes non-small-cell lung cancer cell growth through inflammasome-dependent pathway. J. Cell. Physiol. 2019, 234, 20161–20173. [Google Scholar] [CrossRef]
- Yu, Q.; Zhang, M.; Ying, Q.; Xie, X.; Yue, S.; Tong, B.; Wei, Q.; Bai, Z.; Ma, L. Decrease of AIM2 mediated by luteolin contributes to non-small cell lung cancer treatment. Cell Death Dis. 2019, 10, 218. [Google Scholar] [CrossRef]
- Farshchian, M.; Nissinen, L.; Siljamaki, E.; Riihila, P.; Piipponen, M.; Kivisaari, A.; Kallajoki, M.; Grenman, R.; Peltonen, J.; Peltonen, S.; et al. Tumor cell-specific AIM2 regulates growth and invasion of cutaneous squamous cell carcinoma. Oncotarget 2017, 8, 45825–45836. [Google Scholar] [CrossRef]
- Chai, D.; Shan, H.; Wang, G.; Li, H.; Fang, L.; Song, J.; Zhang, Q.; Bai, J.; Zheng, J. AIM2 is a potential therapeutic target in human renal carcinoma and suppresses its invasion and metastasis via enhancing autophagy induction. Exp. Cell Res. 2018, 370, 561–570. [Google Scholar] [CrossRef]
- Chen, J.; Wang, Z.; Yu, S. AIM2 regulates viability and apoptosis in human colorectal cancer cells via the PI3K/Akt pathway. OncoTargets Ther. 2017, 10, 811–817. [Google Scholar] [CrossRef]
- Ma, X.; Guo, P.; Qiu, Y.; Mu, K.; Zhu, L.; Zhao, W.; Li, T.; Han, L. Loss of AIM2 expression promotes hepatocarcinoma progression through activation of mTOR-S6K1 pathway. Oncotarget 2016, 7, 36185–36197. [Google Scholar] [CrossRef]
- Chen, S.L.; Liu, L.L.; Lu, S.X.; Luo, R.Z.; Wang, C.H.; Wang, H.; Cai, S.H.; Yang, X.; Xie, D.; Zhang, C.Z.; et al. HBx-mediated decrease of AIM2 contributes to hepatocellular carcinoma metastasis. Mol. Oncol. 2017, 11, 1225–1240. [Google Scholar] [CrossRef]
- Chai, D.; Liu, N.; Li, H.; Wang, G.; Song, J.; Fang, L.; Lu, Z.; Yao, H.; Zheng, J. H1/pAIM2 nanoparticles exert anti-tumour effects that is associated with the inflammasome activation in renal carcinoma. J. Cell. Mol. Med. 2018, 22, 5670–5681. [Google Scholar] [CrossRef]
- Deswaerte, V.; Nguyen, P.; West, A.; Browning, A.F.; Yu, L.; Ruwanpura, S.M.; Balic, J.; Livis, T.; Girard, C.; Preaudet, A.; et al. Inflammasome Adaptor ASC Suppresses Apoptosis of Gastric Cancer Cells by an IL18-Mediated Inflammation-Independent Mechanism. Cancer Res. 2018, 78, 1293–1307. [Google Scholar] [CrossRef]
- Ahmed, S.G.; Ahmed, A.; Maguire, C.A.; Doha, M.; Sagers, J.; Lewis, R.M.; Muzikansky, A.; Giovannini, M.; Stemmer-Rachamimov, A.; Stankovic, K.M.; et al. Gene therapy with apoptosis-associated speck-like protein (ASC), a newly described schwannoma tumor suppressor, inhibits schwannoma growth in vivo. Neuro Oncol. 2019. [Google Scholar] [CrossRef]
- Kitazawa, M.; Hida, S.; Fujii, C.; Taniguchi, S.; Ito, K.; Matsumura, T.; Okada, N.; Sakaizawa, T.; Kobayashi, A.; Takeoka, M.; et al. ASC Induces Apoptosis via Activation of Caspase-9 by Enhancing Gap Junction-Mediated Intercellular Communication. PLoS ONE 2017, 12, e0169340. [Google Scholar] [CrossRef]
- Sakaizawa, T.; Matsumura, T.; Fujii, C.; Hida, S.; Toishi, M.; Shiina, T.; Yoshida, K.; Hamanaka, K.; Ito, K.I.; Taniguchi, S. Potential Role of ASC, a Proapoptotic Protein, for Determining the Cisplatin Susceptibility of Lung Cancer Cells. Tohoku J. Exp. Med. 2018, 244, 133–144. [Google Scholar] [CrossRef] [Green Version]
- Graf, R.P.; Keller, N.; Barbero, S.; Stupack, D. Caspase-8 as a regulator of tumor cell motility. Curr. Mol. Med. 2014, 14, 246–254. [Google Scholar] [CrossRef]
- Okada, N.; Fujii, C.; Matsumura, T.; Kitazawa, M.; Okuyama, R.; Taniguchi, S.; Hida, S. Novel role of ASC as a regulator of metastatic phenotype. Cancer Med. 2016, 5, 2487–2500. [Google Scholar] [CrossRef]
- Kang, Y.; Massague, J. Epithelial-mesenchymal transitions: Twist in development and metastasis. Cell 2004, 118, 277–279. [Google Scholar] [CrossRef]
- Onder, T.T.; Gupta, P.B.; Mani, S.A.; Yang, J.; Lander, E.S.; Weinberg, R.A. Loss of E-cadherin promotes metastasis via multiple downstream transcriptional pathways. Cancer Res. 2008, 68, 3645–3654. [Google Scholar] [CrossRef]
- Wu, C.S.; Chang, K.P.; OuYang, C.N.; Kao, H.K.; Hsueh, C.; Chen, L.C.; Cheng, H.Y.; Liang, Y.; Liou, W.; Liang, C.L.; et al. ASC contributes to metastasis of oral cavity squamous cell carcinoma. Oncotarget 2016, 7, 50074–50085. [Google Scholar] [CrossRef]
- Baldwin, A.G.; Brough, D.; Freeman, S. Inhibiting the Inflammasome: A Chemical Perspective. J. Med. Chem. 2016, 59, 1691–1710. [Google Scholar] [CrossRef]
- Ferrari, D.; Pizzirani, C.; Adinolfi, E.; Lemoli, R.M.; Curti, A.; Idzko, M.; Panther, E.; Di Virgilio, F. The P2X7 receptor: A key player in IL-1 processing and release. J. Immunol. 2006, 176, 3877–3883. [Google Scholar] [CrossRef]
- Ferrara, N.; Hillan, K.J.; Gerber, H.P.; Novotny, W. Discovery and development of bevacizumab, an anti-VEGF antibody for treating cancer. Nat. Rev. Drug Discov. 2004, 3, 391–400. [Google Scholar] [CrossRef]
- Thi, H.T.H.; Hong, S. Inflammasome as a Therapeutic Target for Cancer Prevention and Treatment. J. Cancer Prev. 2017, 22, 62–73. [Google Scholar] [CrossRef] [Green Version]
- Adinolfi, E.; Raffaghello, L.; Giuliani, A.L.; Cavazzini, L.; Capece, M.; Chiozzi, P.; Bianchi, G.; Kroemer, G.; Pistoia, V.; Di Virgilio, F. Expression of P2X7 receptor increases in vivo tumor growth. Cancer Res. 2012, 72, 2957–2969. [Google Scholar] [CrossRef]
- Lamkanfi, M.; Mueller, J.L.; Vitari, A.C.; Misaghi, S.; Fedorova, A.; Deshayes, K.; Lee, W.P.; Hoffman, H.M.; Dixit, V.M. Glyburide inhibits the Cryopyrin/Nalp3 inflammasome. J. Cell Biol. 2009, 187, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Subramaniyam, N.; Arumugam, S.; Ezthupurakkal, P.B.; Ariraman, S.; Biswas, I.; Muthuvel, S.K.; Balakrishnan, A.; Alshammari, G.M.; Chinnasamy, T. Unveiling anticancer potential of glibenclamide: Its synergistic cytotoxicity with doxorubicin on cancer cells. J. Pharm. Biomed. Anal. 2018, 154, 294–301. [Google Scholar] [CrossRef]
- Yan, B.; Peng, Z.; Xing, X.; Du, C. Glibenclamide induces apoptosis by activating reactive oxygen species dependent JNK pathway in hepatocellular carcinoma cells. Biosci. Rep. 2017, 37, BSR20170685. [Google Scholar] [CrossRef]
- Yasukagawa, T.; Niwa, Y.; Simizu, S.; Umezawa, K. Suppression of cellular invasion by glybenclamide through inhibited secretion of platelet-derived growth factor in ovarian clear cell carcinoma ES-2 cells. FEBS Lett. 2012, 586, 1504–1509. [Google Scholar] [CrossRef] [Green Version]
- Perera, A.P.; Fernando, R.; Shinde, T.; Gundamaraju, R.; Southam, B.; Sohal, S.S.; Robertson, A.A.B.; Schroder, K.; Kunde, D.; Eri, R. MCC950, a specific small molecule inhibitor of NLRP3 inflammasome attenuates colonic inflammation in spontaneous colitis mice. Sci. Rep. 2018, 8, 8618. [Google Scholar] [CrossRef]
- Cheng, J.; Liu, Q.; Hu, N.; Zheng, F.; Zhang, X.; Ni, Y.; Liu, J. Downregulation of hsa_circ_0068087 ameliorates TLR4/NF-kappaB/NLRP3 inflammasome-mediated inflammation and endothelial cell dysfunction in high glucose conditioned by sponging miR-197. Gene 2019, 709, 1–7. [Google Scholar] [CrossRef]
- Song, J.; Yang, S.; Yin, R.; Xiao, Q.; Ma, A.; Pan, X. MicroRNA-181a regulates the activation of the NLRP3 inflammatory pathway by targeting MEK1 in THP-1 macrophages stimulated by ox-LDL. J. Cell. Biochem. 2019, 120, 13640–13650. [Google Scholar] [CrossRef]
- Schmitt, C.A.; Fridman, J.S.; Yang, M.; Baranov, E.; Hoffman, R.M.; Lowe, S.W. Dissecting p53 tumor suppressor functions in vivo. Cancer Cell 2002, 1, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.; Zhang, S.; Wu, J.; Chen, M.; Cai, M.C.; Fu, Y.; Li, W.; Wang, J.; Zhao, X.; Yu, Z.; et al. Molecular Targeted Therapies Elicit Concurrent Apoptotic and GSDME-Dependent Pyroptotic Tumor Cell Death. Clin. Cancer Res. 2018, 24, 6066–6077. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Li, S.; Qi, J.; Chen, Z.; Wu, Y.; Guo, J.; Wang, K.; Sun, X.; Zheng, J. Cleavage of GSDME by caspase-3 determines lobaplatin-induced pyroptosis in colon cancer cells. Cell Death Dis. 2019, 10, 193. [Google Scholar] [CrossRef]
- Wang, Y.; Yin, B.; Li, D.; Wang, G.; Han, X.; Sun, X. GSDME mediates caspase-3-dependent pyroptosis in gastric cancer. Biochem. Biophys. Res. Commun. 2018, 495, 1418–1425. [Google Scholar] [CrossRef]
- Orning, P.; Weng, D.; Starheim, K.; Ratner, D.; Best, Z.; Lee, B.; Brooks, A.; Xia, S.; Wu, H.; Kelliher, M.A.; et al. Pathogen blockade of TAK1 triggers caspase-8-dependent cleavage of gasdermin D and cell death. Science 2018, 362, 1064–1069. [Google Scholar] [CrossRef]
- Julien, O.; Wells, J.A. Caspases and their substrates. Cell Death Differ. 2017, 24, 1380–1389. [Google Scholar] [CrossRef]
- Weng, D.; Marty-Roix, R.; Ganesan, S.; Proulx, M.K.; Vladimer, G.I.; Kaiser, W.J.; Mocarski, E.S.; Pouliot, K.; Chan, F.K.; Kelliher, M.A.; et al. Caspase-8 and RIP kinases regulate bacteria-induced innate immune responses and cell death. Proc. Natl. Acad. Sci. USA 2014, 111, 7391–7396. [Google Scholar] [CrossRef] [Green Version]
- Ratner, D.; Orning, M.P.; Proulx, M.K.; Wang, D.; Gavrilin, M.A.; Wewers, M.D.; Alnemri, E.S.; Johnson, P.F.; Lee, B.; Mecsas, J.; et al. The Yersinia pestis Effector YopM Inhibits Pyrin Inflammasome Activation. PLoS Pathog. 2016, 12, e1006035. [Google Scholar] [CrossRef]
- Ratner, D.; Orning, M.P.; Lien, E. Bacterial secretion systems and regulation of inflammasome activation. J. Leukoc. Biol. 2017, 101, 165–181. [Google Scholar] [CrossRef]
- Lee, S.; Hirohama, M.; Noguchi, M.; Nagata, K.; Kawaguchi, A. Influenza A Virus Infection Triggers Pyroptosis and Apoptosis of Respiratory Epithelial Cells through the Type I Interferon Signaling Pathway in a Mutually Exclusive Manner. J. Virol. 2018, 92. [Google Scholar] [CrossRef]
- Bergsbaken, T.; Cookson, B.T. Macrophage activation redirects yersinia-infected host cell death from apoptosis to caspase-1-dependent pyroptosis. PLoS Pathog. 2007, 3, e161. [Google Scholar] [CrossRef]
- Chen, K.W.; Demarco, B.; Heilig, R.; Shkarina, K.; Boettcher, A.; Farady, C.J.; Pelczar, P.; Broz, P. Extrinsic and intrinsic apoptosis activate pannexin-1 to drive NLRP3 inflammasome assembly. EMBO J. 2019, 38, e101638. [Google Scholar] [CrossRef]
- Gao, J.; Qiu, X.; Xi, G.; Liu, H.; Zhang, F.; Lv, T.; Song, Y. Downregulation of GSDMD attenuates tumor proliferation via the intrinsic mitochondrial apoptotic pathway and inhibition of EGFR/Akt signaling and predicts a good prognosis in nonsmall cell lung cancer. Oncol. Rep. 2018, 40, 1971–1984. [Google Scholar] [CrossRef]
- Wang, W.J.; Chen, D.; Jiang, M.Z.; Xu, B.; Li, X.W.; Chu, Y.; Zhang, Y.J.; Mao, R.; Liang, J.; Fan, D.M. Downregulation of gasdermin D promotes gastric cancer proliferation by regulating cell cycle-related proteins. J. Dig. Dis. 2018, 19, 74–83. [Google Scholar] [CrossRef]
- Ahmed, S.G.; Abdelanabi, A.; Doha, M.; Brenner, G.J. Schwannoma gene therapy by adeno-associated virus delivery of the pore-forming protein Gasdermin-D. Cancer Gene Ther. 2019. [Google Scholar] [CrossRef]
- Lage, S.L.; Dominical, V.M.; Wong, C.S.; Sereti, I. Evaluation of Canonical Inflammasome Activation in Human Monocytes by Imaging Flow Cytometry. Front. Immunol. 2019, 10, 1284. [Google Scholar] [CrossRef]
- Vande Walle, L.; Lamkanfi, M. Pyroptosis. Curr. Biol. CB 2016, 26, R568–R572. [Google Scholar] [CrossRef] [Green Version]
- Van Gorp, H.; Lamkanfi, M. The emerging roles of inflammasome-dependent cytokines in cancer development. EMBO Rep. 2019, 20. [Google Scholar] [CrossRef]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 2011, 117, 3720–3732. [Google Scholar] [CrossRef] [Green Version]
- Boraschi, D.; Italiani, P.; Weil, S.; Martin, M.U. The family of the interleukin-1 receptors. Immunol. Rev. 2018, 281, 197–232. [Google Scholar] [CrossRef]
- Munoz-Wolf, N.; Lavelle, E.C. A Guide to IL-1 family cytokines in adjuvanticity. FEBS J. 2018, 285, 2377–2401. [Google Scholar] [CrossRef]
- Kaplanov, I.; Carmi, Y.; Kornetsky, R.; Shemesh, A.; Shurin, G.V.; Shurin, M.R.; Dinarello, C.A.; Voronov, E.; Apte, R.N. Blocking IL-1beta reverses the immunosuppression in mouse breast cancer and synergizes with anti-PD-1 for tumor abrogation. Proc. Natl. Acad. Sci. USA 2019, 116, 1361–1369. [Google Scholar] [CrossRef]
- Wu, J.; Hong, Y.; Wu, T.; Wang, J.; Chen, X.; Wang, Z.; Cheng, B.; Xia, J. Stromal-epithelial lactate shuttle induced by tumorderived interleukin1beta promotes cell proliferation in oral squamous cell carcinoma. Int. J. Mol. Med. 2018, 41, 687–696. [Google Scholar] [CrossRef]
- Hu, M.; Yuan, X.; Liu, Y.; Tang, S.; Miao, J.; Zhou, Q.; Chen, S. IL-1beta-induced NF-kappaB activation down-regulates miR-506 expression to promotes osteosarcoma cell growth through JAG1. Biomed. Pharmacother. 2017, 95, 1147–1155. [Google Scholar] [CrossRef]
- Liu, B.; Zhou, Y.; Chen, X.; Peng, D. IL-1beta-mediated NF-kappaB signaling augments the osteosarcoma cell growth through modulating miR-376c/TGFA axis. Die Pharm. 2017, 72, 419–424. [Google Scholar] [CrossRef]
- Yu, A.; Wang, Y.; Bian, Y.; Chen, L.; Guo, J.; Shen, W.; Chen, D.; Liu, S.; Sun, X. IL-1beta promotes the nuclear translocaiton of S100A4 protein in gastric cancer cells MGC803 and the cell’s stem-like properties through PI3K pathway. J. Cell. Biochem. 2018, 119, 8163–8173. [Google Scholar] [CrossRef]
- Wang, X.; Wang, B.; Xie, J.; Hou, D.; Zhang, H.; Huang, H. Melatonin inhibits epithelialtomesenchymal transition in gastric cancer cells via attenuation of IL1beta/NFkappaB/MMP2/MMP9 signaling. Int. J. Mol. Med. 2018, 42, 2221–2228. [Google Scholar] [CrossRef]
- Li, T.; Zhu, J.; Zuo, S.; Chen, S.; Ma, J.; Ma, Y.; Guo, S.; Wang, P.; Liu, Y. 1,25(OH)2D3 attenuates IL-1beta-induced epithelial to mesenchymal transition through inhibiting the expression of lncTCF7. Oncol. Res. 2018, 27, 739–750. [Google Scholar] [CrossRef]
- Castano, Z.; San Juan, B.P.; Spiegel, A.; Pant, A.; DeCristo, M.J.; Laszewski, T.; Ubellacker, J.M.; Janssen, S.R.; Dongre, A.; Reinhardt, F.; et al. IL-1beta inflammatory response driven by primary breast cancer prevents metastasis-initiating cell colonization. Nat. Cell Biol. 2018, 20, 1084–1097. [Google Scholar] [CrossRef]
- Jimenez-Garduno, A.M.; Mendoza-Rodriguez, M.G.; Urrutia-Cabrera, D.; Dominguez-Robles, M.C.; Perez-Yepez, E.A.; Ayala-Sumuano, J.T.; Meza, I. IL-1beta induced methylation of the estrogen receptor ERalpha gene correlates with EMT and chemoresistance in breast cancer cells. Biochem. Biophys. Res. Commun. 2017, 490, 780–785. [Google Scholar] [CrossRef]
- Storr, S.J.; Safuan, S.; Ahmad, N.; El-Refaee, M.; Jackson, A.M.; Martin, S.G. Macrophage-derived interleukin-1beta promotes human breast cancer cell migration and lymphatic adhesion in vitro. Cancer Immunol. Immunother. CII 2017, 66, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- Mon, N.N.; Senga, T.; Ito, S. Interleukin-1beta activates focal adhesion kinase and Src to induce matrix metalloproteinase-9 production and invasion of MCF-7 breast cancer cells. Oncol. Lett. 2017, 13, 955–960. [Google Scholar] [CrossRef]
- Zhou, J.; Zheng, S.; Liu, T.; Liu, Q.; Chen, Y.; Tan, D.; Ma, R.; Lu, X. IL-1beta from M2 macrophages promotes migration and invasion of ESCC cells enhancing epithelial-mesenchymal transition and activating NF-kappaB signaling pathway. J. Cell. Biochem. 2018, 119, 7040–7052. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, Q.; Lou, Y.; Fu, Q.; Chen, Q.; Wei, T.; Yang, J.; Tang, J.; Wang, J.; Chen, Y.; et al. Hypoxia-inducible factor-1alpha/interleukin-1beta signaling enhances hepatoma epithelial-mesenchymal transition through macrophages in a hypoxic-inflammatory microenvironment. Hepatology 2018, 67, 1872–1889. [Google Scholar] [CrossRef]
- Wang, C.I.; Yu, C.J.; Huang, Y.; Yi, J.S.; Cheng, H.W.; Kao, H.K.; Lao, W.W.; Chang, K.P. Association of overexpressed karyopherin alpha 2 with poor survival and its contribution to interleukin-1beta-induced matrix metalloproteinase expression in oral cancer. Head Neck 2018, 40, 1719–1733. [Google Scholar] [CrossRef]
- Lee, M.K.; Park, J.H.; Gi, S.H.; Hwang, Y.S. IL-1beta Induces Fascin Expression and Increases Cancer Invasion. Anticancer Res. 2018, 38, 6127–6132. [Google Scholar] [CrossRef]
- Chen, X.; Lv, Q.; Hong, Y.; Chen, X.; Cheng, B.; Wu, T. IL-1beta maintains the redox balance by regulating glutaredoxin 1 expression during oral carcinogenesis. J. Oral Pathol. Med. 2017, 46, 332–339. [Google Scholar] [CrossRef]
- Mendoza-Rodriguez, M.G.; Ayala-Sumuano, J.T.; Garcia-Morales, L.; Zamudio-Meza, H.; Perez-Yepez, E.A.; Meza, I. IL-1beta Inflammatory Cytokine-Induced TP63 Isoform NP63alpha Signaling Cascade Contributes to Cisplatin Resistance in Human Breast Cancer Cells. Int. J. Mol. Sci. 2019, 20, 270. [Google Scholar] [CrossRef]
- Mendoza-Rodriguez, M.; Arevalo Romero, H.; Fuentes-Panana, E.M.; Ayala-Sumuano, J.T.; Meza, I. IL-1beta induces up-regulation of BIRC3, a gene involved in chemoresistance to doxorubicin in breast cancer cells. Cancer Lett. 2017, 390, 39–44. [Google Scholar] [CrossRef]
- Zhang, D.; Li, L.; Jiang, H.; Li, Q.; Wang-Gillam, A.; Yu, J.; Head, R.; Liu, J.; Ruzinova, M.B.; Lim, K.H. Tumor-Stroma IL1beta-IRAK4 Feedforward Circuitry Drives Tumor Fibrosis, Chemoresistance, and Poor Prognosis in Pancreatic Cancer. Cancer Res. 2018, 78, 1700–1712. [Google Scholar] [CrossRef]
- Dinarello, C.A. An expanding role for interleukin-1 blockade from gout to cancer. Mol. Med. 2014, 20 (Suppl. 1), S43–S58. [Google Scholar] [CrossRef]
- Braddock, M.; Quinn, A. Targeting IL-1 in inflammatory disease: New opportunities for therapeutic intervention. Nat. Rev. Drug Discov. 2004, 3, 330–339. [Google Scholar] [CrossRef]
- Fleischmann, R.; Stern, R.; Iqbal, I. Anakinra: an inhibitor of IL-1 for the treatment of rheumatoid arthritis. Expert Opin. Biol. Ther. 2004, 4, 1333–1344. [Google Scholar] [CrossRef]
- Zhang, B.; Chu, S.; Agarwal, P.; Campbell, V.L.; Hopcroft, L.; Jorgensen, H.G.; Lin, A.; Gaal, K.; Holyoake, T.L.; Bhatia, R. Inhibition of interleukin-1 signaling enhances elimination of tyrosine kinase inhibitor-treated CML stem cells. Blood 2016, 128, 2671–2682. [Google Scholar] [CrossRef]
- Kurzrock, R.; Hickish, T.; Wyrwicz, L.; Saunders, M.; Wu, Q.; Stecher, M.; Mohanty, P.; Dinarello, C.A.; Simard, J. Interleukin-1 receptor antagonist levels predict favorable outcome after bermekimab, a first-in-class true human interleukin-1alpha antibody, in a phase III randomized study of advanced colorectal cancer. Oncoimmunology 2019, 8, 1551651. [Google Scholar] [CrossRef]
- Stanam, A.; Gibson-Corley, K.N.; Love-Homan, L.; Ihejirika, N.; Simons, A.L. Interleukin-1 blockade overcomes erlotinib resistance in head and neck squamous cell carcinoma. Oncotarget 2016, 7, 76087–76100. [Google Scholar] [CrossRef] [Green Version]
- Isambert, N.; Hervieu, A.; Rebe, C.; Hennequin, A.; Borg, C.; Zanetta, S.; Chevriaux, A.; Richard, C.; Derangere, V.; Limagne, E.; et al. Fluorouracil and bevacizumab plus anakinra for patients with metastatic colorectal cancer refractory to standard therapies (IRAFU): A single-arm phase 2 study. Oncoimmunology 2018, 7, e1474319. [Google Scholar] [CrossRef]
- Zhuang, Z.; Ju, H.Q.; Aguilar, M.; Gocho, T.; Li, H.; Iida, T.; Lee, H.; Fan, X.; Zhou, H.; Ling, J.; et al. IL1 Receptor Antagonist Inhibits Pancreatic Cancer Growth by Abrogating NF-kappaB Activation. Clin. Cancer Res. 2016, 22, 1432–1444. [Google Scholar] [CrossRef]
- Church, L.D.; McDermott, M.F. Canakinumab, a fully-human mAb against IL-1beta for the potential treatment of inflammatory disorders. Curr. Opin. Mol. Ther. 2009, 11, 81–89. [Google Scholar]
- Tulotta, C.; Lefley, D.V.; Freeman, K.; Gregory, W.M.; Hanby, A.M.; Heath, P.R.; Nutter, F.; Wilkinson, J.M.; Spicer-Hadlington, A.R.; Liu, X.; et al. Endogenous Production of IL1B by Breast Cancer Cells Drives Metastasis and Colonization of the Bone Microenvironment. Clin. Cancer Res. 2019, 25, 2769–2782. [Google Scholar] [CrossRef]
- Orlando, I.; Vitale, A.; Rigante, D.; Lopalco, G.; Fabiani, C.; Cantarini, L. Long-term efficacy and safety of the interleukin-1 inhibitors anakinra and canakinumab in refractory Behcet disease uveitis and concomitant bladder papillary carcinoma. Intern. Med. J. 2017, 47, 1086–1088. [Google Scholar] [CrossRef]
- Thompson, P.L.; Nidorf, S.M. Anti-inflammatory therapy with canakinumab for atherosclerotic disease: Lessons from the CANTOS trial. J. Thorac. Dis. 2018, 10, 695–698. [Google Scholar] [CrossRef]
- Ridker, P.M.; MacFadyen, J.G.; Thuren, T.; Everett, B.M.; Libby, P.; Glynn, R.J.; Group, C.T. Effect of interleukin-1beta inhibition with canakinumab on incident lung cancer in patients with atherosclerosis: Exploratory results from a randomised, double-blind, placebo-controlled trial. Lancet 2017, 390, 1833–1842. [Google Scholar] [CrossRef]
- Dinarello, C.A.; Simon, A.; van der Meer, J.W. Treating inflammation by blocking interleukin-1 in a broad spectrum of diseases. Nat. Rev. Drug Discov. 2012, 11, 633–652. [Google Scholar] [CrossRef] [Green Version]
- Garg, M.; de Jesus, A.A.; Chapelle, D.; Dancey, P.; Herzog, R.; Rivas-Chacon, R.; Muskardin, T.L.W.; Reed, A.; Reynolds, J.C.; Goldbach-Mansky, R.; et al. Rilonacept maintains long-term inflammatory remission in patients with deficiency of the IL-1 receptor antagonist. JCI Insight 2017, 2, e94838. [Google Scholar] [CrossRef]
- Dinarello, C.A.; van der Meer, J.W. Treating inflammation by blocking interleukin-1 in humans. Semin. Immunol. 2013, 25, 469–484. [Google Scholar] [CrossRef] [Green Version]
- Wawrocki, S.; Druszczynska, M.; Kowalewicz-Kulbat, M.; Rudnicka, W. Interleukin 18 (IL-18) as a target for immune intervention. Acta Biochim. Pol. 2016, 63, 59–63. [Google Scholar] [CrossRef]
- Enoksson, S.L.; Grasset, E.K.; Hagglof, T.; Mattsson, N.; Kaiser, Y.; Gabrielsson, S.; McGaha, T.L.; Scheynius, A.; Karlsson, M.C. The inflammatory cytokine IL-18 induces self-reactive innate antibody responses regulated by natural killer T cells. Proc. Natl. Acad. Sci. USA 2011, 108, E1399–E1407. [Google Scholar] [CrossRef]
- Sedimbi, S.K.; Hagglof, T.; Karlsson, M.C. IL-18 in inflammatory and autoimmune disease. Cell. Mol. Life Sci. CMLS 2013, 70, 4795–4808. [Google Scholar] [CrossRef]
- Jurecekova, J.; Babusikova, E.; Kmetova Sivonova, M.; Drobkova, H.; Petras, M.; Kliment, J.; Halasova, E. Association between interleukin-18 variants and prostate cancer in Slovak population. Neoplasma 2017, 64, 148–155. [Google Scholar] [CrossRef]
- Huang, C.Y.; Chang, W.S.; Tsai, C.W.; Hsia, T.C.; Shen, T.C.; Bau, D.T.; Shui, H.A. Interleukin-18 promoter genotype is associated with the risk of nasopharyngeal carcinoma in Taiwan. Cancer Manag. Res. 2018, 10, 5199–5207. [Google Scholar] [CrossRef]
- Bakr, N.M.; Awad, A.; Moustafa, E.A. Association of genetic variants in the interleukin-18 gene promoter with risk of hepatocellular carcinoma and metastasis in patients with hepatitis C virus infection. IUBMB Life 2018, 70, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Gan, W.Y.; Li, H.M.; Zhang, Y.G.; Li, C.M.; Wang, Y. Association between IL18-607C/A and -137G/C polymorphisms and susceptibility to non-small cell lung cancer in a Chinese population. Genet. Mol. Res. GMR 2016, 15, gmr15048822. [Google Scholar] [CrossRef]
- Wang, H.; Hua, M.; Wang, S.; Yu, J.; Chen, C.; Zhao, X.; Zhang, C.; Zhong, C.; Wang, R.; He, N.; et al. Genetic polymorphisms of IL-18 rs1946518 and IL-1beta rs16944 are associated with prognosis and survival of acute myeloid leukemia. Inflamm. Res. 2017, 66, 249–258. [Google Scholar] [CrossRef]
- Nakamura, K.; Kassem, S.; Cleynen, A.; Chretien, M.L.; Guillerey, C.; Putz, E.M.; Bald, T.; Forster, I.; Vuckovic, S.; Hill, G.R.; et al. Dysregulated IL-18 Is a Key Driver of Immunosuppression and a Possible Therapeutic Target in the Multiple Myeloma Microenvironment. Cancer Cell 2018, 33, 634–648.e5. [Google Scholar] [CrossRef] [Green Version]
- Ko, C.Y.; Wang, W.L.; Li, C.F.; Jeng, Y.M.; Chu, Y.Y.; Wang, H.Y.; Tseng, J.T.; Wang, J.M. IL-18-induced interaction between IMP3 and HuR contributes to COX-2 mRNA stabilization in acute myeloid leukemia. J. Leukoc. Biol. 2016, 99, 131–141. [Google Scholar] [CrossRef]
- Ding, S.; Tang, Z.; Jiang, Y.; Huang, H.; Luo, P.; Qing, B.; Zhang, S.; Tang, R. IL-8 Is Involved in Estrogen-Related Receptor alpha-Regulated Proliferation and Migration of Colorectal Cancer Cells. Dig. Dis. Sci. 2017, 62, 3438–3446. [Google Scholar] [CrossRef]
- Li, Y.; Xu, Z.; Li, J.; Ban, S.; Duan, C.; Liu, W. Interleukin-18 expression in oral squamous cell carcinoma: its role in tumor cell migration and invasion, and growth of tumor cell xenografts. FEBS Open Bio 2018, 8, 1953–1963. [Google Scholar] [CrossRef]
- Usul Afsar, C.; Karabulut, M.; Karabulut, S.; Alis, H.; Gonenc, M.; Dagoglu, N.; Serilmez, M.; Tas, F. Circulating interleukin-18 (IL-18) is a predictor of response to gemcitabine based chemotherapy in patients with pancreatic adenocarcinoma. J. Infect. Chemother. 2017, 23, 196–200. [Google Scholar] [CrossRef]
- Fabbi, M.; Carbotti, G.; Ferrini, S. Context-dependent role of IL-18 in cancer biology and counter-regulation by IL-18BP. J. Leukoc. Biol. 2015, 97, 665–675. [Google Scholar] [CrossRef]
- Kaplanski, G. Interleukin-18: Biological properties and role in disease pathogenesis. Immunol. Rev. 2018, 281, 138–153. [Google Scholar] [CrossRef]
- Li, J.; Qiu, G.; Fang, B.; Dai, X.; Cai, J. Deficiency of IL-18 Aggravates Esophageal Carcinoma Through Inhibiting IFN-gamma Production by CD8(+)T Cells and NK Cells. Inflammation 2018, 41, 667–676. [Google Scholar] [CrossRef]
- Xu, X.; Song, C.; Chen, Z.; Yu, C.; Wang, Y.; Tang, Y.; Luo, J. Downregulation of HuR Inhibits the Progression of Esophageal Cancer through Interleukin-18. Cancer Res. Treat. 2018, 50, 71–87. [Google Scholar] [CrossRef] [Green Version]
- Senju, H.; Kumagai, A.; Nakamura, Y.; Yamaguchi, H.; Nakatomi, K.; Fukami, S.; Shiraishi, K.; Harada, Y.; Nakamura, M.; Okamura, H.; et al. Effect of IL-18 on the Expansion and Phenotype of Human Natural Killer Cells: Application to Cancer Immunotherapy. Int. J. Biol. Sci. 2018, 14, 331–340. [Google Scholar] [CrossRef] [Green Version]
- Kunert, A.; Chmielewski, M.; Wijers, R.; Berrevoets, C.; Abken, H.; Debets, R. Intra-tumoral production of IL18, but not IL12, by TCR-engineered T cells is non-toxic and counteracts immune evasion of solid tumors. Oncoimmunology 2017, 7, e1378842. [Google Scholar] [CrossRef]
- Yang, C.; Cao, H.; Liu, N.; Xu, K.; Ding, M.; Mao, L.J. Oncolytic adenovirus expressing interleukin-18 improves antitumor activity of dacarbazine for malignant melanoma. Drug Des. Dev. Ther. 2016, 10, 3755–3761. [Google Scholar] [CrossRef]
- Markowitz, G.J.; Yang, P.; Fu, J.; Michelotti, G.A.; Chen, R.; Sui, J.; Yang, B.; Qin, W.H.; Zhang, Z.; Wang, F.S.; et al. Inflammation-Dependent IL18 Signaling Restricts Hepatocellular Carcinoma Growth by Enhancing the Accumulation and Activity of Tumor-Infiltrating Lymphocytes. Cancer Res. 2016, 76, 2394–2405. [Google Scholar] [CrossRef]
- Zhuang, L.; Fulton, R.J.; Rettman, P.; Sayan, A.E.; Coad, J.; Al-Shamkhani, A.; Khakoo, S.I. Activity of IL-12/15/18 primed natural killer cells against hepatocellular carcinoma. Hepatol. Int. 2019, 13, 75–83. [Google Scholar] [CrossRef]
- Liu, X.; Hu, J.; Li, Y.; Cao, W.; Wang, Y.; Ma, Z.; Li, F. Mesenchymal stem cells expressing interleukin-18 inhibit breast cancer in a mouse model. Oncol. Lett. 2018, 15, 6265–6274. [Google Scholar] [CrossRef]
- Zhao, Y.; Shen, M.; Feng, Y.; He, R.; Xu, X.; Xie, Y.; Shi, X.; Zhou, M.; Pan, S.; Wang, M.; et al. Regulatory B cells induced by pancreatic cancer cell-derived interleukin-18 promote immune tolerance via the PD-1/PD-L1 pathway. Oncotarget 2018, 9, 14803–14814. [Google Scholar] [CrossRef]
- Guo, X.; Zheng, L.; Jiang, J.; Zhao, Y.; Wang, X.; Shen, M.; Zhu, F.; Tian, R.; Shi, C.; Xu, M.; et al. Blocking NF-kappaB Is Essential for the Immunotherapeutic Effect of Recombinant IL18 in Pancreatic Cancer. Clin. Cancer Res. 2016, 22, 5939–5950. [Google Scholar] [CrossRef]
- Park, I.H.; Yang, H.N.; Lee, K.J.; Kim, T.S.; Lee, E.S.; Jung, S.Y.; Kwon, Y.; Kong, S.Y. Tumor-derived IL-18 induces PD-1 expression on immunosuppressive NK cells in triple-negative breast cancer. Oncotarget 2017, 8, 32722–32730. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Wei, L.; Huang, Y.; Wu, Y.; Su, M.; Pang, X.; Wang, N.; Ji, F.; Zhong, C.; Chen, T. Leptin promotes breast cancer cell migration and invasion via IL-18 expression and secretion. Int. J. Oncol. 2016, 48, 2479–2487. [Google Scholar] [CrossRef] [Green Version]
- Ma, Z.; Li, W.; Yoshiya, S.; Xu, Y.; Hata, M.; El-Darawish, Y.; Markova, T.; Yamanishi, K.; Yamanishi, H.; Tahara, H.; et al. Augmentation of Immune Checkpoint Cancer Immunotherapy with IL18. Clin. Cancer Res. 2016, 22, 2969–2980. [Google Scholar] [CrossRef]
- Robertson, M.J.; Kirkwood, J.M.; Logan, T.F.; Koch, K.M.; Kathman, S.; Kirby, L.C.; Bell, W.N.; Thurmond, L.M.; Weisenbach, J.; Dar, M.M. A dose-escalation study of recombinant human interleukin-18 using two different schedules of administration in patients with cancer. Clin. Cancer Res. 2008, 14, 3462–3469. [Google Scholar] [CrossRef]
- Robertson, M.J.; Mier, J.W.; Logan, T.; Atkins, M.; Koon, H.; Koch, K.M.; Kathman, S.; Pandite, L.N.; Oei, C.; Kirby, L.C.; et al. Clinical and biological effects of recombinant human interleukin-18 administered by intravenous infusion to patients with advanced cancer. Clin. Cancer Res. 2006, 12, 4265–4273. [Google Scholar] [CrossRef]
- Tarhini, A.A.; Millward, M.; Mainwaring, P.; Kefford, R.; Logan, T.; Pavlick, A.; Kathman, S.J.; Laubscher, K.H.; Dar, M.M.; Kirkwood, J.M. A phase 2, randomized study of SB-485232, rhIL-18, in patients with previously untreated metastatic melanoma. Cancer 2009, 115, 859–868. [Google Scholar] [CrossRef]
- Robertson, M.J.; Kline, J.; Struemper, H.; Koch, K.M.; Bauman, J.W.; Gardner, O.S.; Murray, S.C.; Germaschewski, F.; Weisenbach, J.; Jonak, Z.; et al. A dose-escalation study of recombinant human interleukin-18 in combination with rituximab in patients with non-Hodgkin lymphoma. J. Immunother. 2013, 36, 331–341. [Google Scholar] [CrossRef]
- Simpkins, F.; Flores, A.; Chu, C.; Berek, J.S.; Lucci, J., 3rd; Murray, S.; Bauman, J.; Struemper, H.; Germaschewski, F.; Jonak, Z.; et al. Chemoimmunotherapy using pegylated liposomal Doxorubicin and interleukin-18 in recurrent ovarian cancer: a phase I dose-escalation study. Cancer Immunol. Res. 2013, 1, 168–178. [Google Scholar] [CrossRef]
- Cao, Q.; Cai, W.; Niu, G.; He, L.; Chen, X. Multimodality imaging of IL-18–binding protein-Fc therapy of experimental lung metastasis. Clin. Cancer Res. 2008, 14, 6137–6145. [Google Scholar] [CrossRef]
Figure 1.
Molecular mechanisms involved in inflammasome activation. Activation of the canonical inflammasomes usually requires two steps. As the first priming step, PAMPs or DAMPs combine with TLRs on the plasma membrane to trigger NF-ĸB-dependent transcription of inflammasome components and their downstream targets, including NLRP3, pro-IL-1β and pro-IL-18. The second step involves the recognition of PAMPs or DAMPs by the inflammasome sensors AIM2, pyrin, NLRC4, NLRP1 and NLRP3. These sensors recruit the adaptor protein ASC and procaspase-1 to form diverse inflammasomes. Once assembled, the inflammasomes act as activating platforms for procaspase-1. Catalytically active caspase-1 converts the inactive pro-IL-1β and pro-IL-18 into their biologically active forms (IL-1β and IL-18). On the other hand, caspase-1 cleaves GSDMD to release an N-terminal pore-forming domain (GSDMD-NT), which migrates toward the plasma membrane and forms membrane pores. The pores facilitate the release of the active IL-1β and IL-18 into the extracellular environment. In addition, caspase-1 activation leads to the cleavage of chromosomal DNA by nuclease activity. The non-canonical inflammasome pathway is specifically activated by Gram-negative bacteria. IFN-γ-induced GBP causes the lysis of Gram-negative bacteria-containing vacuoles, allowing the release of LPS into the cytoplasm. Intracellular bacterial LPS can directly activate caspase-4 and -5 in humans and caspase-11 in mice. These caspases cleave GSDMD to drive pyroptotic cell death. GSDMD-NT activates the NLRP3 inflammasome to promote caspase-1-dependent cytokine maturation. TLR, toll-like receptor; PAMPs, pathogen-associated molecular patterns; DAMPs, damage-associated molecular patterns; IFN-γ, interferon-γ; IFNR, interferon receptor; NF-ĸB, nuclear factor-ĸB; GBP, guanylate-binding protein; ASC, apoptosis-associated speck-like protein containing a caspase recruitment domain; LPS, lipopolysaccharide; GSDMD, gasdermin D; GSDMD-NT, the N-terminal fragment of GSDMD; IL-1β, interleukin-1β; IL-18, interleukin-18.
Figure 1.
Molecular mechanisms involved in inflammasome activation. Activation of the canonical inflammasomes usually requires two steps. As the first priming step, PAMPs or DAMPs combine with TLRs on the plasma membrane to trigger NF-ĸB-dependent transcription of inflammasome components and their downstream targets, including NLRP3, pro-IL-1β and pro-IL-18. The second step involves the recognition of PAMPs or DAMPs by the inflammasome sensors AIM2, pyrin, NLRC4, NLRP1 and NLRP3. These sensors recruit the adaptor protein ASC and procaspase-1 to form diverse inflammasomes. Once assembled, the inflammasomes act as activating platforms for procaspase-1. Catalytically active caspase-1 converts the inactive pro-IL-1β and pro-IL-18 into their biologically active forms (IL-1β and IL-18). On the other hand, caspase-1 cleaves GSDMD to release an N-terminal pore-forming domain (GSDMD-NT), which migrates toward the plasma membrane and forms membrane pores. The pores facilitate the release of the active IL-1β and IL-18 into the extracellular environment. In addition, caspase-1 activation leads to the cleavage of chromosomal DNA by nuclease activity. The non-canonical inflammasome pathway is specifically activated by Gram-negative bacteria. IFN-γ-induced GBP causes the lysis of Gram-negative bacteria-containing vacuoles, allowing the release of LPS into the cytoplasm. Intracellular bacterial LPS can directly activate caspase-4 and -5 in humans and caspase-11 in mice. These caspases cleave GSDMD to drive pyroptotic cell death. GSDMD-NT activates the NLRP3 inflammasome to promote caspase-1-dependent cytokine maturation. TLR, toll-like receptor; PAMPs, pathogen-associated molecular patterns; DAMPs, damage-associated molecular patterns; IFN-γ, interferon-γ; IFNR, interferon receptor; NF-ĸB, nuclear factor-ĸB; GBP, guanylate-binding protein; ASC, apoptosis-associated speck-like protein containing a caspase recruitment domain; LPS, lipopolysaccharide; GSDMD, gasdermin D; GSDMD-NT, the N-terminal fragment of GSDMD; IL-1β, interleukin-1β; IL-18, interleukin-18.

Figure 2.
Overview of the roles of the pyroptotic pathways in cancer. The major components (inflammasomes, gasdermins and inflammatory cytokines) involved in pyroptotic cell death pathways can either promote or restrain cancer progression. Their pro-tumorigenic mechanisms primarily include induction of immunosuppressive cells, impairment of antitumor immunity, suppression of cell apoptosis, and promotion of the EMT program. Promotion of cell death, repression of the EMT process and induction of antitumor immunity represent pivotal mechanisms mediating the anti-tumorigenic roles of the pyroptotic pathways. PARP, poly (ADP-ribose) polymerase; MDSCs, myeloid-derived suppressor cells; Tregs, regulatory T cells; CDC2, cell division cycle 2; TP53, tumor protein p53; Bcl-2, B-cell lymphoma-2; Bax, Bcl-2-associated X protein; EMT, epithelial-mesenchymal transition; MMPs, matrix metalloproteinases; IL-12, interleukin-12; IL-10, interleukin-10; Bregs, regulatory B cells; PD-1, programmed cell death-1; CAFs, cancer-associated fibroblasts; BIRC3, baculoviral inhibitor of apoptosis repeat-containing 3; FAK, focal adhesion kinase; COX-2, cyclooxygenase-2; ∆NP63α, tumor protein 63 (TP63) isoform; ERα, estrogen receptor α; IRAK4, interleukin-1 receptor-associated kinase 4; CDK2, cyclin-dependent kinase 2; BID, Bcl-2 homology domain 3 (BH3)-interacting domain death agonist; XIAP, X-linked inhibitor of apoptosis protein; LC3, microtubule-associated protein light chain 3; ATG5, autophagy-related gene 5; NK cells, natural killer cells.
Figure 2.
Overview of the roles of the pyroptotic pathways in cancer. The major components (inflammasomes, gasdermins and inflammatory cytokines) involved in pyroptotic cell death pathways can either promote or restrain cancer progression. Their pro-tumorigenic mechanisms primarily include induction of immunosuppressive cells, impairment of antitumor immunity, suppression of cell apoptosis, and promotion of the EMT program. Promotion of cell death, repression of the EMT process and induction of antitumor immunity represent pivotal mechanisms mediating the anti-tumorigenic roles of the pyroptotic pathways. PARP, poly (ADP-ribose) polymerase; MDSCs, myeloid-derived suppressor cells; Tregs, regulatory T cells; CDC2, cell division cycle 2; TP53, tumor protein p53; Bcl-2, B-cell lymphoma-2; Bax, Bcl-2-associated X protein; EMT, epithelial-mesenchymal transition; MMPs, matrix metalloproteinases; IL-12, interleukin-12; IL-10, interleukin-10; Bregs, regulatory B cells; PD-1, programmed cell death-1; CAFs, cancer-associated fibroblasts; BIRC3, baculoviral inhibitor of apoptosis repeat-containing 3; FAK, focal adhesion kinase; COX-2, cyclooxygenase-2; ∆NP63α, tumor protein 63 (TP63) isoform; ERα, estrogen receptor α; IRAK4, interleukin-1 receptor-associated kinase 4; CDK2, cyclin-dependent kinase 2; BID, Bcl-2 homology domain 3 (BH3)-interacting domain death agonist; XIAP, X-linked inhibitor of apoptosis protein; LC3, microtubule-associated protein light chain 3; ATG5, autophagy-related gene 5; NK cells, natural killer cells.

Figure 3.
Schematic representation of chemotherapy-induced apoptosis and pyroptosis in cancer cell. Apoptosis is induced via the intrinsic or extrinsic death signaling pathway. Chemotherapy induces DNA damage and activates p53, which interacts with Bax in mitochondria and triggers the mitochondria-dependent (intrinsic) apoptotic pathway. Detailedly, Bax promotes the release of cytochrome c and initiates the capase-9/caspase-3 cascade, resulting in cell apoptosis. In contrast, the extrinsic apoptosis pathway involves the binding of death ligands (e.g., Fas and TNF) to their receptors. This event gives rise to the activation of caspase-8. The latter evokes cell apoptosis by cleaving BID and directly activating caspase-3. In certain GSDME-expressing cancer cells, GSDME is able to switch chemotherapy-induced apoptosis to pyroptosis. Caspase-3 cleaves GSDME to generate the N-terminal fragment (GSDME-NT), which perforates the plasma membrane to execute pyroptosis. Bcl-2, B-cell lymphoma-2; Bcl-xL, B-cell lymphoma-extra large; Bak, Bcl-2 homologous antagonist/killer; Bax, Bcl-2-associated X protein; BID, Bcl-2 homology domain 3 (BH3)-interacting domain death agonist; tBID, truncated BID; FADD, Fas-associated death domain protein; ROS, reactive oxygen species; PARP, poly (ADP-ribose) polymerase; GSDME, gasdermin E; GSDME-NT, the N-terminal fragment of GSDME.
Figure 3.
Schematic representation of chemotherapy-induced apoptosis and pyroptosis in cancer cell. Apoptosis is induced via the intrinsic or extrinsic death signaling pathway. Chemotherapy induces DNA damage and activates p53, which interacts with Bax in mitochondria and triggers the mitochondria-dependent (intrinsic) apoptotic pathway. Detailedly, Bax promotes the release of cytochrome c and initiates the capase-9/caspase-3 cascade, resulting in cell apoptosis. In contrast, the extrinsic apoptosis pathway involves the binding of death ligands (e.g., Fas and TNF) to their receptors. This event gives rise to the activation of caspase-8. The latter evokes cell apoptosis by cleaving BID and directly activating caspase-3. In certain GSDME-expressing cancer cells, GSDME is able to switch chemotherapy-induced apoptosis to pyroptosis. Caspase-3 cleaves GSDME to generate the N-terminal fragment (GSDME-NT), which perforates the plasma membrane to execute pyroptosis. Bcl-2, B-cell lymphoma-2; Bcl-xL, B-cell lymphoma-extra large; Bak, Bcl-2 homologous antagonist/killer; Bax, Bcl-2-associated X protein; BID, Bcl-2 homology domain 3 (BH3)-interacting domain death agonist; tBID, truncated BID; FADD, Fas-associated death domain protein; ROS, reactive oxygen species; PARP, poly (ADP-ribose) polymerase; GSDME, gasdermin E; GSDME-NT, the N-terminal fragment of GSDME.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wang, M.; Jiang, S.; Zhang, Y.; Li, P.; Wang, K. The Multifaceted Roles of Pyroptotic Cell Death Pathways in Cancer. Cancers 2019, 11, 1313. https://doi.org/10.3390/cancers11091313
AMA Style
Wang M, Jiang S, Zhang Y, Li P, Wang K. The Multifaceted Roles of Pyroptotic Cell Death Pathways in Cancer. Cancers. 2019; 11(9):1313. https://doi.org/10.3390/cancers11091313
Chicago/Turabian StyleWang, Man, Shuai Jiang, Yinfeng Zhang, Peifeng Li, and Kun Wang. 2019. "The Multifaceted Roles of Pyroptotic Cell Death Pathways in Cancer" Cancers 11, no. 9: 1313. https://doi.org/10.3390/cancers11091313
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.