
Prevalence of Major Depressive Disorder and Correlates of Thoughts of Death, Suicidal Behaviour, and Death by Suicide in the Geriatric Population—A General Review of Literature


Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.1.1. Inclusion and Exclusion
2.1.2. Search Strategy
- Prevalence of depression in the geriatric population;
- Prevalence and predictors of thoughts of death by suicide, suicidal behaviors, and death by suicide in geriatric population;
- Methods of suicide.
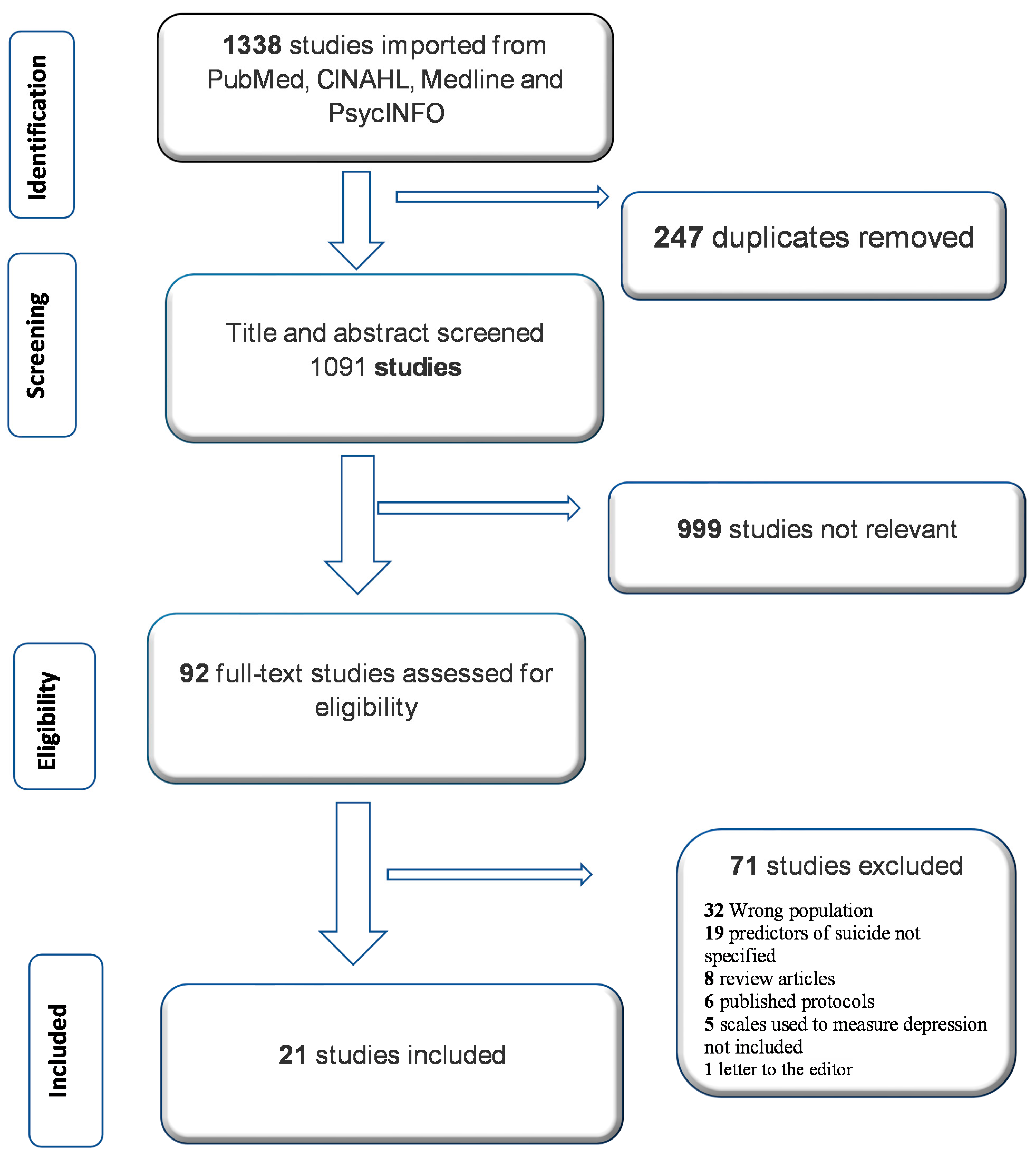
3. Results
4. Discussion
4.1. Demography and Suicide
4.2. Correlates of Death by Suicide in the Elderly
4.3. Mental Illness
4.4. Major Depressive Disorder
4.5. Physical Illness
4.6. Social/Economic Factor
4.7. Substance Use
4.8. Methods of Suicide
4.9. Public Policy and Practice Implications
4.10. Limitations
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perrig-Chiello, P.; Perrig, W.J.; Uebelbacher, A.; Stähelin, H.B. Impact of physical and psychological resources on functional autonomy in old age. Psychol. Health Med. 2006, 11, 470–482. [Google Scholar] [CrossRef]
- Crestani, C.; Masotti, V.; Corradi, N.; Schirripa, M.L.; Cecchi, R. Suicide in the elderly: A 37-years retrospective study. Acta Biomed. 2019, 90, 68–76. [Google Scholar] [CrossRef]
- Fuster, V. Changing Demographics: A New Approach to Global Health Care Due to the Aging Population; American College of Cardiology Foundation: Washington, DC, USA, 2017. [Google Scholar]
- Association, C.M.H. Mental Health and Addiction Issues for Older Adults: Opening the Doors to a Strategic Framework. 2010. Ontario. Available online: http://www.ontario.cmha.ca (accessed on 14 June 2021).
- Adinkrah, M. Characteristics of Elderly Suicides in Ghana. Omega 2020, 82, 3–24. [Google Scholar] [CrossRef]
- Shah, A.; Bhat, R.; Zarate-Escudero, S.; DeLeo, D.; Erlangsen, A. Suicide rates in five-year age-bands after the age of 60 years: The international landscape. Aging Ment. Health 2016, 20, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.R.; Li, X.; Zhang, Y. Suicide rates in China, 1995–1999. Lancet 2002, 359, 835–840. [Google Scholar] [CrossRef]
- Bergman Levy, T.; Barak, Y.; Sigler, M.; Aizenberg, D. Suicide attempts and burden of physical illness among depressed elderly inpatients. Arch. Gerontol. Geriatr. 2011, 52, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Minayo, M.C.S.; Figueiredo, A.E.B.; Mangas, R.M.D.N. Study of scientific publications (2002–2017) on suicidal ideation, suicide attempts and self-neglect of elderly people hospitalized in Long-Term Care Establishments. Cien. Saude Colet. 2019, 24, 1393–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Mental Health. Transforming the Understanding and Treatment of Mental Illness. Suicide. 2021. Available online: https://www.nimh.nih.gov/health/statistics/suicide (accessed on 6 June 2021).
- Carlson, W.L.; Ong, T.D. Suicide in later life: Failed treatment or rational choice? Clin. Geriatr. Med. 2014, 30, 553–576. [Google Scholar] [CrossRef] [PubMed]
- WHO. Suicide. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 13 June 2021).
- Shah, A.; Bhat, R. Are elderly suicide rates improved by increased provision of mental health service resources? A cross-national study. Int. Psychogeriatr. 2008, 20, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Arboleda-Flórez, J.; Fick, G.H.; Stuart, H.L.; Love, E.J. Association between physical illness and suicide among the elderly. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.M.; Kua, E.H. Ethnicity and elderly suicide in Singapore. Int. Psychogeriatr. 1995, 7, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Schooling, C.M.; Chan, W.M.; Ho, K.S.; Lam, T.H. The association between depressive symptoms and mortality among Chinese elderly: A Hong Kong cohort study. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, S.E.; Burruss, S.K.; Mukherjee, K. Suicide in the elderly: A multidisciplinary approach to prevention. Clin. Geriatr. Med. 2019, 35, 133–145. [Google Scholar] [CrossRef]
- Andrade, E.R.; de Sousa, E.R.; Minayo, M.C.d.S. Self-esteem and quality of life: Essential for the mental health of police officers. Ciência Saúde Coletiva 2009, 14, 275–285. [Google Scholar]
- Minayo, M.C.; Cavalcante, F.G. Suicide in elderly people: A literature review. Rev. Saude Publica 2010, 44, 750–757. [Google Scholar] [CrossRef] [Green Version]
- The American Association of Suicidology. U.S.A. SUICIDE: 2019 OFFICIAL FINAL DATA. 2021. Available online: https://suicidology.org/facts-and-statistics/ (accessed on 6 June 2021).
- WHO. Depression and Other Common Mental Disorders Global Health Estimates. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf?sequence=1&isAllowed=y (accessed on 17 June 2021).
- Edition, F. Diagnostic and statistical manual of mental disorders. Am. Psychiatr. Assoc. 2013, 21, 160. [Google Scholar]
- Gomez, G.E.; Gomez, E.A. Depression in the elderly. J. Psychosoc. Nurs. Ment. Health Serv. 1993, 31, 28–33. [Google Scholar] [CrossRef]
- Tannock, C.; Katona, C. Minor depression in the aged. Concepts, prevalence and optimal management. Drugs Aging 1995, 6, 278–292. [Google Scholar] [CrossRef] [PubMed]
- Babatsikou, F.; Konsolaki, E.; Notara, V.; Kouri, M.; Zyga, S.; Koutis, C. Depression in the elderly: A descriptive study of Urban and Semi-Urban Greek population. Int. J. Caring Sci. 2017, 10, 1286–1295. [Google Scholar]
- Blazer, D.; Hughes, D.C.; George, L.K. The epidemiology of depression in an elderly community population. Gerontologist 1987, 27, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Raue, P.J.; Morales, K.H.; Post, E.P.; Bogner, H.R.; Have, T.T.; Bruce, M.L. The wish to die and 5-year mortality in elderly primary care patients. Am. J. Geriatr. Psychiatry 2010, 18, 341–350. [Google Scholar] [CrossRef] [Green Version]
- Lykouras, L.; Gournellis, R. Depression in the elderly. Ann. Gen. Psychiatry 2008, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Cindy, W.; Helen, F. Depression and suicide in the elderly. Med. Bull. 2011, 9, 13–16. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, J.C.; Pandharipande, P.P.; Girard, T.D.; Brummel, N.E.; Thompson, J.L.; Hughes, C.G.; Pun, B.T.; Vasilevskis, E.E.; Morandi, A.; Shintani, A.K. Depression, post-traumatic stress disorder, and functional disability in survivors of critical illness in the BRAIN-ICU study: A longitudinal cohort study. Lancet Respir. Med. 2014, 2, 369–379. [Google Scholar] [CrossRef] [Green Version]
- Parmelee, P.A.; Katz, I.R. Geriatric depression scale. J. Am. Geriatr. Soc. 1990, 38, 1379. [Google Scholar] [CrossRef] [PubMed]
- Mitty, E.; Flores, S. Suicide in late life. Geriatr. Nurs. 2008, 29, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Conwell, Y.; Thompson, C. Suicidal behavior in elders. Psychiatr. Clin. N. Am. 2008, 31, 333–356. [Google Scholar] [CrossRef] [Green Version]
- Williams, V.; Eiseman, E.; Landree, E.; Adamson, D. Demonstrating and Communicating Research Impact. Preparing Niosh Programs for External Review; Rand Corp Santa Monica Ca Inst for Civil Justice: Santa Monica, CA, USA, 2009. [Google Scholar]
- Rossom, R.C.; Simon, G.E.; Coleman, K.J.; Beck, A.; Oliver, M.; Stewart, C.; Ahmedani, B. Are wishes for death or suicidal ideation symptoms of depression in older adults? Aging Ment. Health 2019, 23, 912–918. [Google Scholar] [CrossRef]
- Sarokhani, D.; Parvareh, M.; Dehkordi, A.H.; Sayehmiri, K.; Moghimbeigi, A. Prevalence of Depression among Iranian Elderly: Systematic Review and Meta-Analysis. Iran J. Psychiatry 2018, 13, 55–64. [Google Scholar]
- Shoib, S.; Islam, S.M.S.; Arafat, S.Y.; Hakak, S.A. Depression and suicidal ideation among the geriatric population of Kashmir, India. Int. J. Soc. Psychiatry 2020, 20764020968592. [Google Scholar] [CrossRef]
- Gallo, J.J. Handbook of Geriatric Assessment; Jones & Bartlett Learning: Burlington, MA, USA, 2006. [Google Scholar]
- Pilania, M.; Yadav, V.; Bairwa, M.; Behera, P.; Gupta, S.D.; Khurana, H.; Mohan, V.; Baniya, G.; Poongothai, S. Prevalence of depression among the elderly (60 years and above) population in India, 1997–2016: A systematic review and meta-analysis. BMC Public Health 2019, 19, 832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nations, U. International Day of Older Persons. 2021. Available online: https://www.un.org/en/observances/older-persons-day (accessed on 1 October 2021).
- Park, J.H.; Lee, J.J.; Lee, S.B.; Huh, Y.; Choi, E.A.; Youn, J.C.; Jhoo, J.H.; Kim, J.S.; Woo, J.I.; Kim, K.W. Prevalence of major depressive disorder and minor depressive disorder in an elderly Korean population: Results from the Korean Longitudinal Study on Health and Aging (KLoSHA). J. Affect. Disord. 2010, 125, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Wongpakaran, N.; Wongpakaran, T. Prevalence of major depressive disorders and suicide in long-term care facilities: A report from northern Thailand. Psychogeriatrics 2012, 12, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Padayachey, U.; Ramlall, S.; Chipps, J. Depression in older adults: Prevalence and risk factors in a primary health care sample. S. Afr. Fam. Pract. 2017, 59, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Harwood, D.; Hawton, K.; Hope, T.; Jacoby, R. Psychiatric disorder and personality factors associated with suicide in older people: A descriptive and case-control study. Int. J. Geriatr. Psychiatry 2001, 16, 155–165. [Google Scholar] [CrossRef]
- Conwell, Y.; Duberstein, P.R.; Caine, E.D. Risk factors for suicide in later life. Biol. Psychiatry 2002, 52, 193–204. [Google Scholar] [CrossRef]
- Waern, M.; Runeson, B.S.; Allebeck, P.; Beskow, J.; Rubenowitz, E.; Skoog, I.; Wilhelmsson, K. Mental disorder in elderly suicides: A case-control study. Am. J. Psychiatry 2002, 159, 450–455. [Google Scholar] [CrossRef]
- Booniam, S.; Wongpakaran, T.; Lerttrakarnnon, P.; Jiraniramai, S.; Kuntawong, P.; Wongpakaran, N. Predictors of Passive and Active Suicidal Ideation and Suicide Attempt Among Older People: A Study in Tertiary Care Settings in Thailand. Neuropsychiatr. Dis. Treat. 2020, 16, 3135–3144. [Google Scholar] [CrossRef]
- Altınöz, A.E.; Yenilmez, Ç.; Öner, S.K.; Yıldız, P. Completed suicide rates of older adults in 5-year age bands in Turkey between 2002 and 2013: A retrospective study. Geriatr. Gerontol. Int. 2019, 19, 66–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rurup, M.L.; Deeg, D.J.; Poppelaars, J.L.; Kerkhof, A.J.; Onwuteaka-Philipsen, B.D. Wishes to die in older people: A quantitative study of prevalence and associated factors. Crisis 2011, 32, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Kim, T.H.; Shin, J.; Han, E. Poverty and suicide risk in older adults: A retrospective longitudinal cohort study. Int. J. Geriatr. Psychiatry 2019, 34, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D.; Draper, B.M.; Snowdon, J.; Kõlves, K. Suicides in older adults: A case-control psychological autopsy study in Australia. J. Psychiatr. Res. 2013, 47, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Conejero, I.; Olié, E.; Courtet, P.; Calati, R. Suicide in older adults: Current perspectives. Clin. Interv. Aging 2018, 13, 691–699. [Google Scholar] [CrossRef] [Green Version]
- Waern, M.; Rubenowitz, E.; Runeson, B.; Skoog, I.; Wilhelmson, K.; Allebeck, P. Burden of illness and suicide in elderly people: Case-control study. BMJ 2002, 324, 1355. [Google Scholar] [CrossRef] [Green Version]
- Razai, D.; Ghadirzadeh, M.R.; Mahdavi, S.A.; Hasani, J.; Hashemi Nazari, S.S. The Suicide Rate in the Elderly Population of Iran between 2008 and 2014. J. Res. Health Sci. 2020, 20, e00471. [Google Scholar] [CrossRef]
- Voaklander, D.C.; Rowe, B.H.; Dryden, D.M.; Pahal, J.; Saar, P.; Kelly, K.D. Medical illness, medication use and suicide in seniors: A population-based case-control study. J. Epidemiol. Community Health 2008, 62, 138–146. [Google Scholar] [CrossRef]
- Kaya, A.; Tosun Tasar, P.; Meral, O.; Sahın, S.; Balkay, M.; Ozgur Aktas, E.; Akcıcek, F. The characteristics of older people suicides by sex and age subgroups. Leg Med. 2020, 46, 101721. [Google Scholar] [CrossRef]
- Liu, B.P.; Qin, P.; Jia, C.X. Behavior Characteristics and Risk Factors for Suicide Among the Elderly in Rural China. J. Nerv. Ment. Dis. 2018, 206, 195–201. [Google Scholar] [CrossRef]
- Shin, K.M.; Cho, S.M.; Hong, C.H.; Park, K.S.; Shin, Y.M.; Lim, K.Y.; Koh, S.H. Suicide among the elderly and associated factors in South Korea. Aging Ment. Health 2013, 17, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Spallek, J.; Reeske, A.; Norredam, M.; Nielsen, S.S.; Lehnhardt, J.; Razum, O. Suicide among immigrants in Europe—A systematic literature review. Eur. J. Public Health 2015, 25, 63–71. [Google Scholar] [CrossRef]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Primers. 2019, 5, 74. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.F.; Chan, S.S.; Lam, L.C. Suicide in the elderly. Curr. Opin. Psychiatry 2001, 14, 395–399. [Google Scholar] [CrossRef]
- Szanto, K.; Galfalvy, H.; Kenneally, L.; Almasi, R.; Dombrovski, A.Y. Predictors of serious suicidal behavior in late-life depression. Eur. Neuropsychopharmacol. 2020, 40, 85–98. [Google Scholar] [CrossRef]
- Tan, L.L.; Wong, H.B. Severity of depression and suicidal ideations among elderly people in Singapore. Int. Psychogeriatr. 2008, 20, 338–346. [Google Scholar] [CrossRef]
- Sharafkhani, R.; Biranvand, A.; Gareaghaji, R. Risk factors for death in suicide attempters-west Azerbaijan province: Case-control study. Stud. Med. Sci. 2013, 23, 655–660. [Google Scholar]
- Shojaei, A.; Moradi, S.; Alaeddini, F.; Khodadoost, M.; Barzegar, A.; Khademi, A. Association between suicide method, and gender, age, and education level in I ran over 2006–2010. Asia-Pac. Psychiatry 2014, 6, 18–22. [Google Scholar] [CrossRef]
- Turvey, C.L.; Conwell, Y.; Jones, M.P.; Phillips, C.; Simonsick, E.; Pearson, J.L.; Wallace, R. Risk factors for late-life suicide: A prospective, community-based study. Am. J. Geriatr. Psychiatry 2002, 10, 398–406. [Google Scholar] [CrossRef]
- Chan, H.L.; Liu, C.Y.; Chau, Y.L.; Chang, C.M. Prevalence and association of suicide ideation among Taiwanese elderly—A population-based cross-sectional study. Chang Gung Med. J. 2011, 34, 197–204. [Google Scholar]
- Zhong, B.L.; Liu, T.B.; Chan, S.S.; Jin, D.; Hu, C.Y.; Dai, J.; Chiu, H.F. Prevalence and correlates of major depressive disorder among rural-to-urban migrant workers in Shenzhen, China. J. Affect. Disord. 2015, 183, 1–9. [Google Scholar] [CrossRef]
- Kessler, R.C.; Warner, C.H.; Ivany, C.; Petukhova, M.V.; Rose, S.; Bromet, E.J.; Brown, M.; Cai, T.; Colpe, L.J.; Cox, K.L.; et al. Predicting suicides after psychiatric hospitalization in US Army soldiers: The Army Study To Assess Risk and rEsilience in Servicemembers (Army STARRS). JAMA Psychiatry 2015, 72, 49–57. [Google Scholar] [CrossRef]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, R. Almost 80. Aged population: Expectations and roles. Int. J. Nurs. Pr. 1999, 5, 51–53. [Google Scholar] [CrossRef]
- Harwood, D.; Hawton, K.; Hope, T.; Jacoby, R. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: A descriptive and case-control study. J. Affect. Disord. 2002, 72, 185–194. [Google Scholar] [CrossRef]
- Raue, P.J.; Ghesquiere, A.R.; Bruce, M.L. Suicide risk in primary care: Identification and management in older adults. Curr. Psychiatry Rep. 2014, 16, 466. [Google Scholar] [CrossRef] [Green Version]
- Draper, B. Suicidal behaviour. Princ. Pract. Geriatr. Psychiatry 2010, 559–564. [Google Scholar] [CrossRef]
- Bickford, D.; Morin, R.T.; Nelson, J.C.; Mackin, R.S. Determinants of Suicide-related Ideation in Late Life Depression: Associations with Perceived Stress. Clin. Gerontol. 2020, 43, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Center for Behavioral Health Statistics and Quality Methodology Report. In DSM-5 Changes: Implications for Child Serious Emotional Disturbance; Substance Abuse and Mental Health Services Administration (US): Rockville, MD, USA, 2016. [Google Scholar]
- Snowdon, J.; Baume, P. A study of suicides of older people in Sydney. Int. J. Geriatr. Psychiatry 2002, 17, 261–269. [Google Scholar] [CrossRef]
- Benazzi, F. Late-life depression in private practice depressed outpatients: A 203-case study. Int. J. Geriatr. Psychiatry 1998, 13, 145–148. [Google Scholar] [CrossRef]
- Butters, M.A.; Whyte, E.M.; Nebes, R.D.; Begley, A.E.; Dew, M.A.; Mulsant, B.H.; Zmuda, M.D.; Bhalla, R.; Meltzer, C.C.; Pollock, B.G.; et al. The nature and determinants of neuropsychological functioning in late-life depression. Arch. Gen. Psychiatry 2004, 61, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Rapp, M.A.; Dahlman, K.; Sano, M.; Grossman, H.T.; Haroutunian, V.; Gorman, J.M. Neuropsychological differences between late-onset and recurrent geriatric major depression. Am. J. Psychiatry 2005, 162, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.D. Depression in the elderly. N. Engl. J. Med. 2014, 371, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Conwell, Y.; Olsen, K.; Caine, E.D.; Flannery, C. Suicide in later life: Psychological autopsy findings. Int. Psychogeriatr. 1991, 3, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, M.M.; Marttunen, M.J.; Isometsä, E.T.; Heikkinen, M.E.; Aro, H.M.; Kuoppasalmi, K.I.; Lönnqvist, J.K. Mental disorders in elderly suicide. Int. Psychogeriatr. 1995, 7, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Szigethy, E.; Conwell, Y.; Forbes, N.T.; Cox, C.; Caine, E.D. Adrenal weight and morphology in victims of completed suicide. Biol. Psychiatry 1994, 36, 374–380. [Google Scholar] [CrossRef]
- Roca, M.; Del Amo, A.R.; Riera-Serra, P.; Pérez-Ara, M.A.; Castro, A.; Roman Juan, J.; García-Toro, M.; García-Pazo, P.; Gili, M. Suicidal risk and executive functions in major depressive disorder: A study protocol. BMC Psychiatry 2019, 19, 253. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.P.; Qin, P.; Liu, Y.Y.; Yuan, L.; Gu, L.X.; Jia, C.X. Mental disorders and suicide attempt in rural China. Psychiatry Res. 2018, 261, 190–196. [Google Scholar] [CrossRef]
- O’Neil, M. Depression in the elderly. J. Contin. Educ. Nurs. 2007, 38, 14–15. [Google Scholar] [CrossRef]
- Pratt, C.C.; Schmall, V.L.; Wilson, W.; Benthin, A. A model community education program on depression and suicide in later life. Gerontologist 1991, 31, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Forsell, Y.; Jorm, A.F.; Winblad, B. Suicidal thoughts and associated factors in an elderly population. Acta Psychiatr. Scand. 1997, 95, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Cattell, H. Suicide in the elderly. Adv. Psychiatr. Treat. 2000, 6, 102–108. [Google Scholar] [CrossRef]
- Conwell, Y.; Duberstein, P.R.; Cox, C.; Herrmann, J.H.; Forbes, N.T.; Caine, E.D. Relationships of age and axis I diagnoses in victims of completed suicide: A psychological autopsy study. Am. J. Psychiatry 1996, 153, 1001–1008. [Google Scholar] [CrossRef]
- Handley, T.; Rich, J.; Davies, K.; Lewin, T.; Kelly, B. The Challenges of Predicting Suicidal Thoughts and Behaviours in a Sample of Rural Australians with Depression. Int. J. Environ. Res. Public Health 2018, 15, 928. [Google Scholar] [CrossRef] [Green Version]
- Lapierre, S.; Erlangsen, A.; Waern, M.; De Leo, D.; Oyama, H.; Scocco, P.; Gallo, J.; Szanto, K.; Conwell, Y.; Draper, B.; et al. A systematic review of elderly suicide prevention programs. Crisis 2011, 32, 88–98. [Google Scholar] [CrossRef]
- Yip, P.S.; Chi, I.; Chiu, H.; Chi Wai, K.; Conwell, Y.; Caine, E. A prevalence study of suicide ideation among older adults in Hong Kong SAR. Int. J. Geriatr. Psychiatry 2003, 18, 1056–1062. [Google Scholar] [CrossRef]
- Abou El-Magd, R.M.; Obuobi-Donkor, G.; Adu, M.K.; Lachowski, C.; Duddumpudi, S.; Lawal, M.A.; Sapara, A.O.; Achor, M.; Kouzehgaran, M.; Hegde, R.; et al. Repetitive Transcranial Magnetic Stimulation with and without Internet-Delivered Cognitive-Behavioral Therapy for the Treatment of Resistant Depression: Protocol for Patient-Centered Randomized Controlled Pilot Trial. JMIR Res. Protoc. 2020, 9, e18843. [Google Scholar] [CrossRef]
- Carney, S.S.; Rich, C.L.; Burke, P.A.; Fowler, R.C. Suicide over 60: The San Diego study. J. Am. Geriatr. Soc. 1994, 42, 174–180. [Google Scholar] [CrossRef]
- Conwell, Y.; Rotenberg, M.; Caine, E.D. Completed suicide at age 50 and over. J. Am. Geriatr. Soc. 1990, 38, 640–644. [Google Scholar] [CrossRef]
- Brown, J.H.; Henteleff, P.; Barakat, S.; Rowe, C.J. Is it normal for terminally ill patients to desire death? Am. J. Psychiatry 1986, 143, 208–211. [Google Scholar] [CrossRef]
- Conwell, Y.; Caine, E.D.; Olsen, K. Suicide and cancer in late life. Hosp. Community Psychiatry 1990, 41, 1334–1339. [Google Scholar] [CrossRef]
- Duberstein, P.R.; Conwell, Y.; Conner, K.R.; Eberly, S.; Caine, E.D. Suicide at 50 years of age and older: Perceived physical illness, family discord and financial strain. Psychol. Med. 2004, 34, 137–146. [Google Scholar] [CrossRef]
- Fässberg, M.M.; van Orden, K.A.; Duberstein, P.; Erlangsen, A.; Lapierre, S.; Bodner, E.; Canetto, S.S.; De Leo, D.; Szanto, K.; Waern, M. A systematic review of social factors and suicidal behavior in older adulthood. Int. J. Environ. Res. Public Health 2012, 9, 722–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uncapher, H.; Gallagher-Thompson, D.; Osgood, N.J.; Bongar, B. Hopelessness and suicidal ideation in older adults. Gerontologist 1998, 38, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Rowe, J.L.; Conwell, Y.; Schulberg, H.C.; Bruce, M.L. Social support and suicidal ideation in older adults using home healthcare services. Am. J. Geriatr. Psychiatry 2006, 14, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Purcell, D.; Thrush, C.R.; Blanchette, P.L. Suicide among the elderly in Honolulu County: A multiethnic comparative study (1987–1992). Int. Psychogeriatr. 1999, 11, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Zilberman, M.L.; Tavares, H.; Blume, S.B.; el-Guebaly, N. Substance use disorders: Sex differences and psychiatric comorbidities. Can. J. Psychiatry 2003, 48, 5–13. [Google Scholar] [CrossRef]
- Szanto, K.; Prigerson, H.G.; Reynolds, C.F., III. Suicide in the elderly. Clin. Neurosci. Res. 2001, 1, 366–376. [Google Scholar] [CrossRef]
- Draper, B. Suicidal behaviour in the elderly. Int. J. Geriatr. Psychiatry 1994, 9, 655–661. [Google Scholar] [CrossRef]
- Li, M.; Katikireddi, S.V. Urban-rural inequalities in suicide among elderly people in China: A systematic review and meta-analysis. Int. J. Equity Health 2019, 18, 2. [Google Scholar] [CrossRef]
- Phillips, M.R.; Yang, G.; Zhang, Y.; Wang, L.; Ji, H.; Zhou, M. Risk factors for suicide in China: A national case-control psychological autopsy study. Lancet 2002, 360, 1728–1736. [Google Scholar] [CrossRef]
- Ji, J.; Kleinman, A.; Becker, A.E. Suicide in contemporary China: A review of China’s distinctive suicide demographics in their sociocultural context. Harv. Rev. Psychiatry 2001, 9, 1–12. [Google Scholar] [CrossRef]
- Reddy, M. Suicide Incidence and Epidemiology; SAGE Publications Sage India: New Delhi, India, 2010. [Google Scholar]
- Li, X.; Xiao, Z.; Xiao, S. Suicide among the elderly in mainland China. Psychogeriatrics 2009, 9, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Conwell, Y. Management of suicidal behavior in the elderly. Psychiatr. Clin. N. Am. 1997, 20, 667–683. [Google Scholar] [CrossRef]
- Kim, K.H.; Jeong, K.Y.; Lee, J.S.; Choi, H.S.; Hong, H.P.; Ko, Y.G. The characteristics of elderly patients with suicide attempts: A comparative study with non-elderly patients. Ann. Geriatr. Med. Res. 2016, 20, 209–220. [Google Scholar] [CrossRef]
- Lebowitz, B.D.; Pearson, J.L.; Schneider, L.S.; Reynolds, C.F., 3rd; Alexopoulos, G.S.; Bruce, M.L.; Conwell, Y.; Katz, I.R.; Meyers, B.S.; Morrison, M.F.; et al. Diagnosis and treatment of depression in late life. Consensus statement update. JAMA 1997, 278, 1186–1190. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Shalaby, R.; Hrabok, M.; Vuong, W.; Noble, J.M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; et al. Mental Health Outreach via Supportive Text Messages during the COVID-19 Pandemic: Improved Mental Health and Reduced Suicidal Ideation after Six Weeks in Subscribers of Text4Hope Compared to a Control Population. Int. J. Environ. Res. Public Health 2021, 18, 2157. [Google Scholar] [CrossRef]
- Office of the Surgeon General; National Action Alliance for Suicide Prevention. Publications and Reports of the Surgeon General. In 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action: A Report of the U.S. Surgeon General and of the National Action Alliance for Suicide Prevention; US Department of Health & Human Services (US): Washington, DC, USA, 2012. [Google Scholar]
- Mojtabai, R. Diagnosing depression in older adults in primary care. N. Engl. J. Med. 2014, 370, 1180–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author and Year | Country | Sample Size | Scale Used | Prevalence of MDD |
|---|---|---|---|---|
| Park J.H. et al. (2010) | Korea | 1118 | Geriatric Depression Scale (GDS)-Korea | 5.37% |
| Wongpakaran N. et al. (2012) | Thailand | 113 | Geriatric Depression Scale | 23.5% |
| Booniam S. et al. (2020) | Thailand | 803 | DSM-IV and Thai Geriatric Depression Scale | 18.64% |
| Padayachey U. et al. (2017) | South Africa | 300 | Geriatric Depression Scale | 40% |
| Shoib S. et al. (2020) | India | 200 | Beck’s Depression Inventory | 56% |
| Wærn M. et al. (2002) | Scandinavia | 100 | DSM-IV | 38% |
| Name of Author and Year | Country of Origin | Study Design | Targeted Group | Sample Size | Reason for Suicide | Findings |
|---|---|---|---|---|---|---|
| Crestani C. et al. (2019) | Italy | A retrospective study (autopsy/police report) | 60 years and above | 538 | Mental illness | The highest risk of suicide is observed in the age between 70 and 79 years. Pathological factors were revealed in 427 cases. Mental illness was related significantly to suicidal risk. |
| Bogers I.C.H.M. et al. (2013) | Netherlands | A prospective study | 60 years and above | 378 | Depression and physical injury | Patients reporting thoughts of death but no suicidal ideation were older and more severely depressed, whereas patients with suicidal ideation were also more severely depressed but not older. |
| Rurup M.L. et al. (2011) | Netherlands | A longitudinal cohort study | 58–98 years | 1794 | Psychiatric comorbidity; dysthymia and panic attack. | Of those who wished to die, 67% had depressive symptoms, and 20% suffered from a depressive disorder. |
| Altınöz A.E. et al. (2019) | Turkey | A retrospective study | 65 years and above | 978 | Mental illness and financial difficulties. | The most common cause of suicide was financial difficulty for men and marital conflict for women. The most frequent suicide method among older adults of both sexes was hanging. In all age groups, firearms use was more common among men and jumping from a high place was more common among women. |
| Conejero I. et al. (2018) | Korea | A prospective longitudinal study | 60 years and above | 1548 | Physical illness | Independent relationship between physical health status and suicidal behavior in the elderly. High correlation with the history of suicide attempts in the elderly, and there is independence between depression factors and suicide. |
| Bogers I.C. et al. (2013) | Netherlands | A prospective multi-site naturalistic study | 60 years and above | 378 | Depression | In depressed older persons, thoughts of death and suicide differ in relevant demographic, social, and clinical characteristics, suggesting that the risks and consequences of the two conditions differ. |
| Bickford D. et al. (2020) | San Francisco | A retrospective study | 65 years and above | 225 | Perceived stress | Perceived stress was found to be a risk for suicidal activity in depressed older adults. |
| Booniam S. et al. (2020) | Thailand | A retrospective study | mean age of 69 years | 803 | Major Depressive Disorder (MDD) | MDD was the main predictor for suicidal ideation; however, agoraphobia and poor perceived social support increases suicide risk. |
| Razai D. et al. (2020) | Iran | A cross-sectional descriptive-analytic study | 65 years and above | 1601 | Physical and mental illnesses | Successful suicides have been rising, from 3.7 in 2008 to 4.37 per 100,000 people in 2014. |
| Rossom B.C. et al. (2019) | US | Cross-sectional cohort study | 65 years and above | 203,668 | Depression | Depression severity was by far the strongest predictor of suicidal ideation in older adult patients. Older patients with suicidal ideation should be screened for depression. |
| Shin K.M. et al. (2013) | Korea | A prospective study | 60 years and above | 1548 | Anxiety, depression and stroke | This study suggests that there is an independent relationship between physical health status and suicide behavior in the case of elders. |
| Shoib S. et al. (2020) | India | A cross-sectional study | 65 years and above | 200 | Depression | Depression had a positive correlation with suicidal ideation. Hopelessness and suicidal intent had a more significant positive correlation. |
| Bergman L.T. et al. (2011) | Israel | A retrospective study | 65 years and above | 78 | Physical illness | Suicidal patients scored higher in the vascular and respiratory section of the cumulative illness rating scale; higher rates of illness among suicidal elderly patients. |
| Liu B.P. et al. (2018) | China | A paired case-controlled | 60 years and above | 190 | Not living with a spouse, depressive symptoms | The influence of negative life events increases the risk of suicide in the elderly. |
| Sun W. et al. (2010) | China | A cohort Study | 65 years and above | 56,088 | Depression and physical illness | Depressive symptoms were associated with all-cause mortality in men and with suicide in both sexes. |
| Kaya A. et al. (2020) | Turkey | A retrospective study(autopsy) | 60 years and above | 17,942 | Asphyxia, CNS injury and physical illness | In the summer, June and July, the suicides occurred more frequently in the 65–74 age subgroup. |
| Adinkrah M. et al. (2020) | Ghana | A descriptive study | 60 years to 65 years | 40 | Lack of finance, indebtedness, cuckoldry, sexual dysfunction, grief or marital breakdown. | Elderly persons who died by suicide were male, aged 60 to 65 years old, and of low income. |
| De Leo D. et al. (2013) | Australia | A case-control study | 60 years and above | 261 | Psychiatric diagnosis, hopelessness, past suicidal attempts and living alone | Older adult suicides showed a significantly lower prevalence of psychiatric diagnoses (62%) when compared to middle-aged suicide cases (80%). In both age groups, subjects who died by suicide were significantly more likely to present a psychiatric diagnosis. |
| Chan H.L. et al. (2011) | Taiwan | A Cross-sectional Study | 65 years and above | 3853 | Physical illness and depressive symptoms | The point prevalence of elderly suicidal ideation was 6.1%. Female gender, age over 85 years, low level of education, single status, unemployment, no income, disability, current smoking, self-perceived bad to very bad health, depressive symptoms, various physical disorders, and pain symptoms were strongly associated with suicide ideation. |
| Conwell Y. et al. (2002) | Monroe (US) | A case-control study (psychological autopsies) | 60 years and above | 238 | Depressive illness | Completed suicides had a more depressive illness, physical illness burden and functional limitations. They were more likely to be prescribed antidepressants, anxiolytic agents and narcotic analgesics. Among depressed subjects, affective symptom severity and emotional dysfunction distinguished suicide completers. |
| Wærn M. et al. (2002) | Scandinavia | A case-control study (psychological autopsies) | 65 years and above | 100 | Depressive disorder | Ninety-seven percent of the suicide victims fulfilled the criteria for at least one DSM-IV axis I diagnosis, compared with 18% of the living comparison subjects. Recurrent major depressive disorder was a very strong risk factor for suicide, as was substance use disorder. |
| Turvey C.L. et al. (2002) | US | A longitudinal cohort study | 66 years and above | 14,456 | Depressive symptoms, perceived health status, sleep quality, and absence of loved one | This study provided additional information about the context of late-life depression that also contributes to suicidal behavior: poor perceived health, poor sleep quality, and limited presence of a relative or friend to confide in. |
| Wongpakaran N. et al. (2012) | Thailand | A cross-sectional descriptive study | 63 years- 94years | 113 | Major Depressive Disorder | 23.5% met the criteria for current major depressive episodes and suicide risk was reported for one-third of the elderly. |
| Harwood D. et al. (2001) | UK | A descriptive and case-control study | 60 years and above | 154 | Depression, personality disorder, and personality trait | 77% of the suicide sample had a psychiatric disorder at the time of death, most often depression (63%). |
| Voaklander D.C. et al. (2008) | British Columbia | A case-control studies | 66 years and above | 602 | Lower socioeconomic status, depression and physical illness. | The annual rate of suicide is 13.2 per 100,000. Firearms were the most common mechanism (28%), followed by hanging/suffocation (25%), self-poisoning (21%), and jumping from height (7%). There was an elevated risk for those prescribed inappropriate benzodiazepines and those using strong narcotic pain killer. |
| Author and Year | Methods of Suicide |
|---|---|
| Crestani C. et al. (2019) | Hanging Fall from height Firearm |
| Altınöz A.E. et al. (2019) | Hanging Firearm Jump from height |
| Razai D. et al. (2020) | Hanging Poisoning |
| Kim K.H. et al. (2016) | Drug overdoses Pesticide or caustics |
| Rossom B.C. et al. (2019) | Hanging |
| Shin K.M. et al. (2013) | Hanging |
| Adinkrah M. et al. (2020) | Hanging and firearm |
| Kaya A. et al. (2020) | Hanging |
| Voaklander D.C. et al. (2008) | Medication overdose (benzodiazepine) Firearm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obuobi-Donkor, G.; Nkire, N.; Agyapong, V.I.O. Prevalence of Major Depressive Disorder and Correlates of Thoughts of Death, Suicidal Behaviour, and Death by Suicide in the Geriatric Population—A General Review of Literature. Behav. Sci. 2021, 11, 142. https://doi.org/10.3390/bs11110142
Obuobi-Donkor G, Nkire N, Agyapong VIO. Prevalence of Major Depressive Disorder and Correlates of Thoughts of Death, Suicidal Behaviour, and Death by Suicide in the Geriatric Population—A General Review of Literature. Behavioral Sciences. 2021; 11(11):142. https://doi.org/10.3390/bs11110142
Chicago/Turabian StyleObuobi-Donkor, Gloria, Nnamdi Nkire, and Vincent I. O. Agyapong. 2021. "Prevalence of Major Depressive Disorder and Correlates of Thoughts of Death, Suicidal Behaviour, and Death by Suicide in the Geriatric Population—A General Review of Literature" Behavioral Sciences 11, no. 11: 142. https://doi.org/10.3390/bs11110142