Improvement of Cognitive Function after Continuous Positive Airway Pressure Treatment for Subacute Stroke Patients with Obstructive Sleep Apnea: A Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Ethical Statement
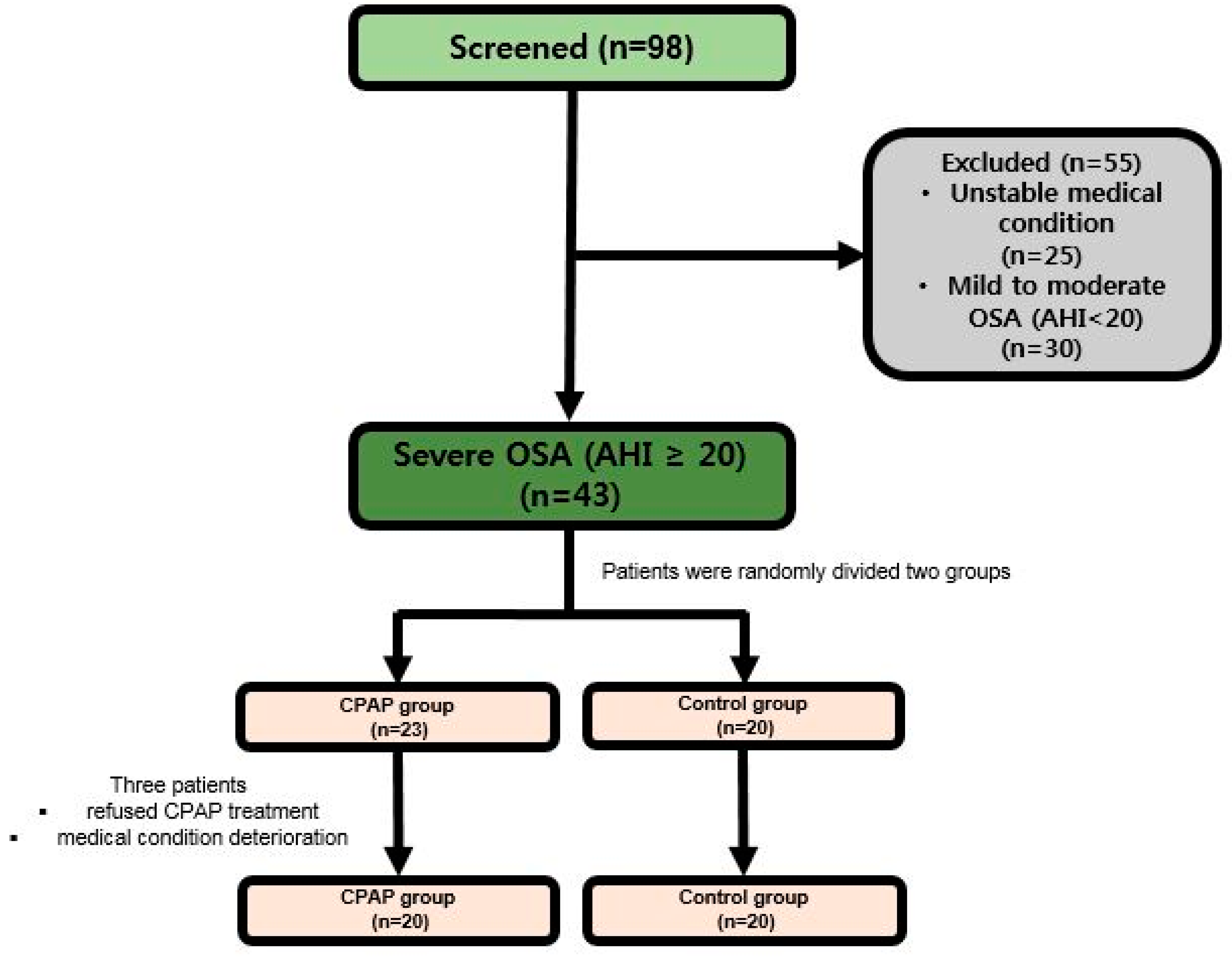
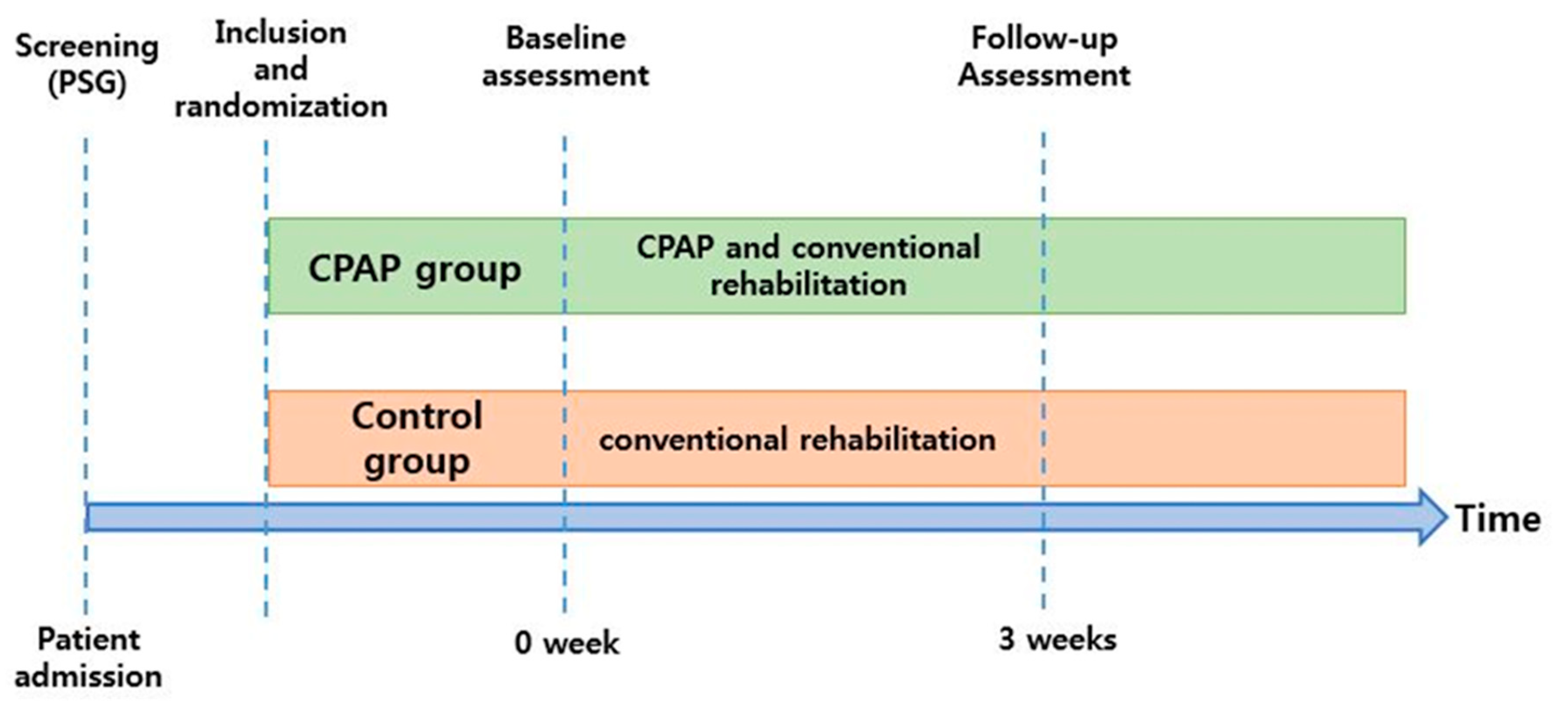
2.2. Study Design
2.3. Patients
2.4. Sleep Examination
2.5. Randomization
2.6. Intervention
2.7. Demographic Data
2.7.1. Primary Outcomes
2.7.2. Secondary Outcome
2.8. Statistical Analysis
3. Results
3.1. Primary Outcome Analysis (Functional and Cognitive Outcomes)
3.2. Secondary Outcome Analysis (Sleep Examination Data)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics—2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Miniño, A.M.; Xu, J.; Kochanek, K. Deaths: Preliminary data for 2008. Natl. Vital Stat. Rep. 2010, 59, 1–52. [Google Scholar] [PubMed]
- Gordon, N.F.; Gulanick, M.; Costa, F.; Fletcher, G.; Franklin, B.A.; Roth, E.J.; Shephard, T. Physical activity and exercise recommendations for stroke survivors: An American Heart Association scientific statement from the Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention; the Council on Cardiovascular Nursing; the Council on Nutrition, Physical Activity, and Metabolism; and the Stroke Council. Stroke 2004, 35, 1230–1240. [Google Scholar] [PubMed]
- De Oliveira, C.B.; De Medeiros, I.R.T.; Frota, N.A.F.; Greters, M.E.; Conforto, A.B. Balance control in hemiparetic stroke patients: Main tools for evaluation. J. Rehabil. Res. Dev. 2008, 45, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Sethi, N.K.; Sacchetti, M.L.; Davis, A.P.; Billings, M.E.; Longstreth, W.T.; Khot, S.P. Early diagnosis and treatment of obstructive sleep apnea after stroke: Are we neglecting a modifiable stroke risk factor? Neurol. Clin. Pract. 2013, 3, 192–201. [Google Scholar] [CrossRef]
- Shahar, E.; Whitney, C.W.; Redline, S.; Lee, E.T.; Newman, A.B.; Javier Nieto, F.; O’Connor, G.T.; Boland, L.L.; Schwartz, J.E.; Samet, J.M. Sleep-disordered breathing and cardiovascular disease: Cross-sectional results of the Sleep Heart Health Study. Am. J. Respir. Crit. Care Med. 2001, 163, 19–25. [Google Scholar] [CrossRef]
- Yaggi, H.K.; Concato, J.; Kernan, W.N.; Lichtman, J.H.; Brass, L.M.; Mohsenin, V. Obstructive Sleep Apnea as a Risk Factor for Stroke and Death. N. Engl. J. Med. 2005, 353, 2034–2041. [Google Scholar] [CrossRef]
- Lattimore, J.L.; Wilcox, I.; Skilton, M.; Langenfeld, M.; Celermajer, D.S. Treatment of obstructive sleep apnoea leads to improved microvascular endothelial function in the systemic circulation. Thorax 2006, 61, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Drager, L.F.; Bortolotto, L.A.; Figueiredo, A.C.; Krieger, E.M.; Lorenzi-Filho, G. Effects of Continuous Positive Airway Pressure on Early Signs of Atherosclerosis in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2007, 176, 706–712. [Google Scholar] [CrossRef]
- Minoguchi, K.; Yokoe, T.; Tazaki, T.; Minoguchi, H.; Oda, N.; Tanaka, A.; Yamamoto, M.; Ohta, S.; O’Donnell, C.P.; Adachi, M. Silent brain infarction and platelet activation in obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2007, 175, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Arzt, M.; Young, T.; Finn, L.; Skatrud, J.B.; Bradley, T.D. Association of sleep-disordered breathing and the occurrence of stroke. Am. J. Respir. Crit. Care Med. 2005, 172, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Klobučníková, K.; Šiarnik, P.; Čarnická, Z.; Kollár, B.; Turčáni, P. Causes of Excessive Daytime Sleepiness in Patients with Acute Stroke—A Polysomnographic Study. J. Stroke Cerebrovasc. Dis. 2016, 25, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, J.A.; Van Bennekom, C.A.; Hofman, W.F.; Van Bezeij, T.; Aardweg, J.G.V.D.; Groet, E.; Kylstra, W.A.; Schmand, B. Obstructive Sleep Apnea is Related to Impaired Cognitive and Functional Status after Stroke. Sleep 2015, 38, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohsenin, V.; Valor, R. Sleep apnea in patients with hemispheric stroke. Arch. Phys. Med. Rehabil. 1995, 76, 71–76. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A.; Galiano-Blancart, R.; Soler-Cataluna, J.J.; Cabero-Salt, L.; Roman-Sanchez, P. Improvement in nocturnal disordered breathing after first-ever ischemic stroke: Role of dysphagia. Chest 2006, 129, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Yan-fang, S.; Yu-ping, W. Sleep-disordered breathing: Impact on functional outcome of ischemic stroke patients. Sleep Med. 2009, 10, 717–719. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, C.L.; Milanova, M.; Gugger, M. Sleep-disordered breathing and acute ischemic stroke: Diagnosis, risk factors, treatment, evolution, and long-term clinical outcome. Stroke 2006, 37, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Camilo, M.R.; Schnitman, S.V.; Sander, H.H.; Eckeli, A.L.; Fernandes, R.M.; Leite, J.P.; Bassetti, C.L.; Pontes-Neto, O.M. Sleep-disordered breathing among acute ischemic stroke patients in Brazil. Sleep Med. 2016, 19, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Hermann, D.M.; Bassetti, C.L. Sleep-related breathing and sleep-wake disturbances in ischemic stroke. Neurology 2009, 73, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Dyken, M.E.; Somers, V.K.; Yamada, T.; Ren, Z.Y.; Zimmerman, M.B. Investigating the relationship between stroke and obstructive sleep apnea. Stroke 1996, 27, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Joo, B.E.; Seok, H.Y.; Yu, S.W.; Kim, B.J.; Park, K.W.; Lee, D.H.; Jung, K.Y. Prevalence of sleep-disordered breathing in acute ischemic stroke as determined using a portable sleep apnea monitoring device in Korean subjects. Sleep Breath. 2011, 15, 77–82. [Google Scholar] [CrossRef]
- Jeon, H.; Sohn, M.K.; Jeon, M.; Jee, S. Clinical Characteristics of Sleep-Disordered Breathing in Subacute Phase of Stroke. Ann. Rehabil. Med. 2017, 41, 556–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iranzo, A.; Santamaria, J.; Berenguer, J.; Sánchez, M.; Chamorro, A. Prevalence and clinical importance of sleep apnea in the first night after cerebral infarction. Neurology 2002, 58, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Nopmaneejumruslers, C.; Kaneko, Y.; Hajek, V.; Zivanovic, V.; Bradley, T.D. Cheyne-Stokes respiration in stroke: Relationship to hypocapnianand occult cardiac dysfunction. Am. J. Respir. Crit. Care Med. 2005, 171, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.A.; Soler-Cataluña, J.J.; Ejarque-Martínez, L.; Soriano, Y.; Román-Sánchez, P.; Illa, F.B.; Canal, J.M.; Durán-Cantolla, J. Continuous positive airway pressure treatment reduces mortality in patients with ischemic stroke and obstructive sleep apnea: A 5-year follow-up study. Am. J. Respir. Crit. Care Med. 2009, 180, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Parra, O.; Arboix, A.; Montserrat, J.; Quintó, L.; Bechich, S.; García-Eroles, L. Sleep-related breathing disorders: Impact on mortality of cerebrovascular disease. Eur. Respir. J. 2004, 24, 267–272. [Google Scholar] [CrossRef]
- Sahlin, C.; Sandberg, O.; Gustafson, Y.; Bucht, G.; Carlberg, B.; Stenlund, H.; Franklin, K.A. Obstructive sleep apnea is a risk factor for death in patients with stroke: A 10-year follow-up. Arch. Intern. Med. 2008, 168, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.M.; Bayley, M.; Green, R.; Murray, B.J.; Bradley, T.D. Influence of continuous positive airway pressure on outcomes of rehabilitation in stroke patients with obstructive sleep apnea. Stroke 2011, 42, 1062–1067. [Google Scholar] [CrossRef]
- Turkington, P.; Bamford, J.; Wanklyn, P.; Elliott, M. Prevalence and predictors of upper airway obstruction in the first 24 hours after acute stroke. Stroke 2002, 33, 2037–2042. [Google Scholar] [CrossRef]
- Broadley, S.A.; Jørgensen, L.; Cheek, A.; Salonikis, S.; Taylor, J.; Thompson, P.D.; Antic, R. Early investigation and treatment of obstructive sleep apnoea after acute stroke. J. Clin. Neurosci. 2007, 14, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.G.; Johnson, D.C. Frequency of Sleep Apnea in Stroke and TIA Patients: A Meta-analysis. J. Clin. Sleep Med. 2010, 6, 131–137. [Google Scholar] [PubMed]
- Lisabeth, L.D.; Sánchez, B.N.; Chervin, R.D.; Morgenstern, L.B.; Zahuranec, D.B.; Tower, S.D.; Brown, D.L. High prevalence of poststroke sleep-disordered breathing in Mexican Americans. Sleep Med. 2017, 33, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Rola, R.; Wierzbicka, A.; Wichniak, A.; Jernajczyk, W.; Richter, P.; Ryglewicz, D. Sleep related breathing disorders in patients with ischemic stroke and transient ischemic attacks: Respiratory and clinical correlations. J. Physiol. Pharmacol. 2007, 58 (Suppl. S5), 575–582. [Google Scholar] [PubMed]
- Sullivan, C.; Berthon-Jones, M.; Issa, F.; Eves, L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef]
- Montserrat, J.M.; Ferrer, M.; Hernandez, L.; Farré, R.; Vilagut, G.; Navajas, D.; Badia, J.R.; Carrasco, E.V.A.; De Pablo, J.U.; Ballester, E.; et al. Effectiveness of CPAP treatment in daytime function in sleep apnea syndrome: A randomized controlled study with an optimized placebo. Am. J. Respir. Crit. Care Med. 2001, 164, 608–613. [Google Scholar] [CrossRef]
- Sutherland, B.A.; Minnerup, J.; Balami, J.S.; Arba, F.; Buchan, A.M.; Kleinschnitz, C. Neuroprotection for Ischaemic Stroke: Translation from the Bench to the Bedside. Int. J. Stroke 2012, 7, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Parra, O.; Sánchez-Armengol, A.; Bonnin, M.; Arboix, A.; Campos-Rodríguez, F.; Pérez-Ronchel, J.; Durán-Cantolla, J.; de la Torre, G.; Marcos, J.G.; de la Peña, M.; et al. Early treatment of obstructive apnoea and stroke outcome: A randomised controlled trial. Eur. Respir. J. 2011, 37, 1128–1136. [Google Scholar] [CrossRef]
- Brill, A.K.; Horvath, T.; Seiler, A.; Camilo, M.; Haynes, A.G.; Ott, S.R.; Egger, M.; Bassetti, C.L. CPAP as treatment of sleep apnea after stroke: A meta-analysis of randomized trials. Neurology 2018, 90, e1222–e1230. [Google Scholar] [CrossRef]
- Parra, O.; Sánchez-Armengol, Á.; Capote, F.; Bonnin, M.; Arboix, A.; Campos-Rodríguez, F.; Pérez-Ronchel, J.; Durán-Cantolla, J.; Martínez-Null, C.; de la Peña, M.; et al. Efficacy of continuous positive airway pressure treatment on 5-year survival in patients with ischaemic stroke and obstructive sleep apnea: A randomized controlled trial. J. Sleep Res. 2015, 24, 47–53. [Google Scholar] [CrossRef]
- Sandberg, O.; Franklin, K.; Bucht, G.; Eriksson, S.; Gustafson, Y. Nasal continuous positive airway pressure in stroke patients with sleep apnoea: A randomized treatment study. Eur. Respir. J. 2001, 18, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical Guideline for the Evaluation, Management and Long-term Care of Obstructive Sleep Apnea in Adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar] [PubMed]
- Collop, N.A.; Anderson, W.M.; Boehlecke, B.; Claman, D.; Goldberg, R.; Gottlieb, D.J.; Hudgel, D.; Sateia, M.; Schwab, R. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients: Portable Monitoring Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2007, 3, 737–747. [Google Scholar] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. Sleepiness in different situations measured by the Epworth Sleepiness Scale. Sleep 1994, 17, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.W.; Lee, J.H.; Son, H.K.; Lee, S.H.; Shin, C.; Johns, M.W. The reliability and validity of the Korean version of the Epworth sleepiness scale. Sleep Breath. 2011, 15, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Han, N.E.; Kim, D.Y.; Lee, S.-A. Validity of Korean Version of Functional Outcomes of Sleep Questionnaire in Patients with Simple Snoring and Obstructive Sleep Apnea. Sleep Med. Res. 2014, 5, 5–14. [Google Scholar] [CrossRef]
- Tombaugh, T.N.; McIntyre, N.J. The Mini-Mental State Examination: A Comprehensive Review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef]
- Kylstra, W.A.; Aaronson, J.A.; Hofman, W.F.; Schmand, B.A. Neuropsychological functioning after CPAP treatment in obstructive sleep apnea: A meta-analysis. Sleep Med. Rev. 2013, 17, 341–347. [Google Scholar] [CrossRef]
- Olaithe, M.; Bucks, R.S. Executive dysfunction in OSA before and after treatment: A meta-analysis. Sleep 2013, 36, 1297–1305. [Google Scholar] [CrossRef]
- Duss, S.B.; Seiler, A.; Schmidt, M.H.; Pace, M.; Adamantidis, A.; Müri, R.M.; Bassetti, C.L. The role of sleep in recovery following ischemic stroke: A review of human and animal data. Neurobiol. Sleep Circadian Rhythms 2017, 2, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Parra, O.; Arboix, A.; Bechich, S.; García-Eroles, L.; Montserrat, J.M.; López, J.A.; Ballester, E.; Guerra, J.M.; Sopeña, J.J. Time Course of Sleep-related Breathing Disorders in First-Ever Stroke or Transient Ischemic Attack. Am. J. Respir. Crit. Care Med. 2000, 161, 375–380. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CPAP (n = 20) | Control (n = 20) | p-Value | |
|---|---|---|---|
| Sex, n (men/women) | 13/7 (65.0/35.0%) | 16/4 (80.0/20.0%) | 0.429 |
| Age (years) | 63.3 ± 13.1 | 66.9 ± 12.3 | 0.369 |
| Type of stroke, n (ischemic/hemorrhagic) | 14/6 (70.0/30.0%) | 16/4 (80.0/20.0%) | 0.602 |
| Lesion type, n (Supratentorial/Infratentorial) | 14/6 (70.0/30.0%) | 11/9 (55.0/45.0%) | 0.429 |
| Ischemic group primary treatment, n (Thrombolysis/Thrombectomy) | 2/4 (10.0/20.0%) | 2/3 (10.0/15.0%) | 0.000 |
| Hemorrhagic group primary treatment, n (observation/hemorrhage removal) | 3/3 (50.0/50.0%) | 2/2 (50.0/50.0%) | 0.000 |
| BMI | 23.3 ± 3.7 | 24.4 ± 3.9 | 0.370 |
| LOS | 38.6 ± 11.4 | 37.8 ± 14.8 | 0.849 |
| NIHSS | 6.7 ± 3.5 | 6.5 ± 5.7 | 0.869 |
| K-MMSE | 18.6 ± 7.7 | 17.5 ± 9.1 | 0.668 |
| FAC | 1.3 ± 1.5 | 1.7 ± 2.0 | 0.474 |
| MRS | 3.9 ± 1.0 | 3.5 ± 1.2 | 0.207 |
| BBS | 15.5 ± 17.1 | 22.9 ± 22.9 | 0.251 |
| K-MBI | 43.1 ± 26.5 | 45.8 ± 31.6 | 0.775 |
| HTN (+/−) | 13/7 (65.0/35.0%) | 15/5 (75.0/25.0%) | 0.602 |
| DM (+/−) | 4/16 (20.0/80.0%) | 7/13 (35.0/65.0%) | 0.429 |
| EQ-5D | 0.3 ± 0.3 | 0.3 ± 1.3 | 0.612 |
| ESS | 6.0 ± 5.4 | 6.7 ± 5.2 | 0.677 |
| Central apnea | 5.5 ± 13.2 | 4.4 ± 14.0 | 0.796 |
| Obstructive apnea | 26.5 ± 17.5 | 15.2 ±13.4 | 0.028 * |
| Mixed apnea | 3.3 ± 6.9 | 5.2 ± 10.3 | 0.503 |
| Hypopnea | 9.1 ± 8.9 | 10.1 ± 7.4 | 0.699 |
| AHI | 44.4 ± 16.8 | 34.9 ± 17.2 | 0.085 |
| Snore flag index | 62.6 ± 76.3 | 42.0 ± 63.9 | 0.359 |
| Desaturation index | 43.3 ± 18.4 | 34.4 ± 20.2 | 0.156 |
| CPAP (n = 20) | Control (n = 20) | p-Value | |
|---|---|---|---|
| ΔNIHSS | −1.5 ± 1.3 | −1.1 ± 1.5 | 0.157 |
| ΔMMSE | 4.0 ± 3.4 | 2.2 ± 1.9 | 0.045 * |
| ΔFAC | 0.8 ± 1.0 | 0.9 ± 1.0 | 0.862 |
| ΔMRS | −0.8 ± 0.8 | −0.4 ± 0.6 | 0.142 |
| ΔBBS | 10.0 ± 10.3 | 8.7 ± 10.7 | 0.583 |
| ΔK-MBI | 14.0 ± 9.8 | 13.5 ± 9.9 | 0.873 |
| ΔEQ-5D | 0.2 ± 0.2 | 0.2 ± 0.3 | 0.282 |
| CPAP (n = 20) | Control (n = 20) | p-Value | |
|---|---|---|---|
| ΔOrientation to time (5) | 0.7 ± 1.0 | 0.1 ± 1.4 | 0.055 |
| ΔOrientation to place (5) | 1.0 ± 1.1 | 0.6 ± 0.9 | 0.155 |
| ΔRegistration (3) | 0.1 ± 0.4 | 0.2 ± 0.7 | 0.554 |
| ΔAttention and calculation (5) | 1.4 ± 0.8 | 0.3 ± 1.3 | 0.001 * |
| ΔRecall (3) | 0.3 ± 1.1 | 0.4 ± 0.6 | 0.558 |
| ΔLanguage (8) | 0.5 ± 0.9 | 0.8 ± 1.1 | 0.501 |
| ΔDrawing (1) | 0.1 ± 0.4 | 0.1 ± 0.6 | 0.710 |
| ΔTotal (30) | 4.0 ± 3.4 | 2.2 ± 1.9 | 0.045 * |
| CPAP (n = 20) | Control (n = 20) | p-Value | |
|---|---|---|---|
| ΔESS | −2.3 ± 2.3 | 0.6 ± 3.3 | 0.003 * |
| ΔCentral apnea | −2.7 ± 10.2 | −0.2 ± 2.9 | 0.449 |
| ΔObstructive apnea | −13.0 ± 14.1 | 1.6 ± 10.6 | 0.001 * |
| ΔMixed apnea | −0.5 ± 7.1 | −0.8 ± 11.3 | 0.715 |
| ΔHypopnea | −1.8 ± 8.1 | −3.7 ± 5.0 | 0.378 |
| ΔAHI | −17.9 ± 12.8 | −3.0 ± 9.7 | 0.001 * |
| ΔSnore flag index | −23.5 ± 54.8 | 0.7 ± 70.3 | 0.441 |
| ΔDesaturation index | −16.2 ± 14.9 | −7.7 ± 19.6 | 0.133 |
| β | Adjusted R2 | p-Value | |
|---|---|---|---|
| ΔAHI | |||
| ΔMMSE | 0.071 | 0.114 | 0.033 * |
| ΔESS | 0.109 | 0.220 | 0.002 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Im, S.; Park, J.i.; Kim, Y.; Sohn, M.K.; Jee, S. Improvement of Cognitive Function after Continuous Positive Airway Pressure Treatment for Subacute Stroke Patients with Obstructive Sleep Apnea: A Randomized Controlled Trial. Brain Sci. 2019, 9, 252. https://doi.org/10.3390/brainsci9100252
Kim H, Im S, Park Ji, Kim Y, Sohn MK, Jee S. Improvement of Cognitive Function after Continuous Positive Airway Pressure Treatment for Subacute Stroke Patients with Obstructive Sleep Apnea: A Randomized Controlled Trial. Brain Sciences. 2019; 9(10):252. https://doi.org/10.3390/brainsci9100252
Chicago/Turabian StyleKim, Howook, Soobin Im, Jun il Park, Yeongwook Kim, Min Kyun Sohn, and Sungju Jee. 2019. "Improvement of Cognitive Function after Continuous Positive Airway Pressure Treatment for Subacute Stroke Patients with Obstructive Sleep Apnea: A Randomized Controlled Trial" Brain Sciences 9, no. 10: 252. https://doi.org/10.3390/brainsci9100252