Endovascular Thrombectomy Following Acute Ischemic Stroke: A Single-Center Case Series and Critical Review of the Literature

Abstract
:1. Introduction
1.1. Intra-Venous Thrombolysis
1.2. Intra-Arterial Fibrinolysis
1.3. Endovascular Thrombectomy
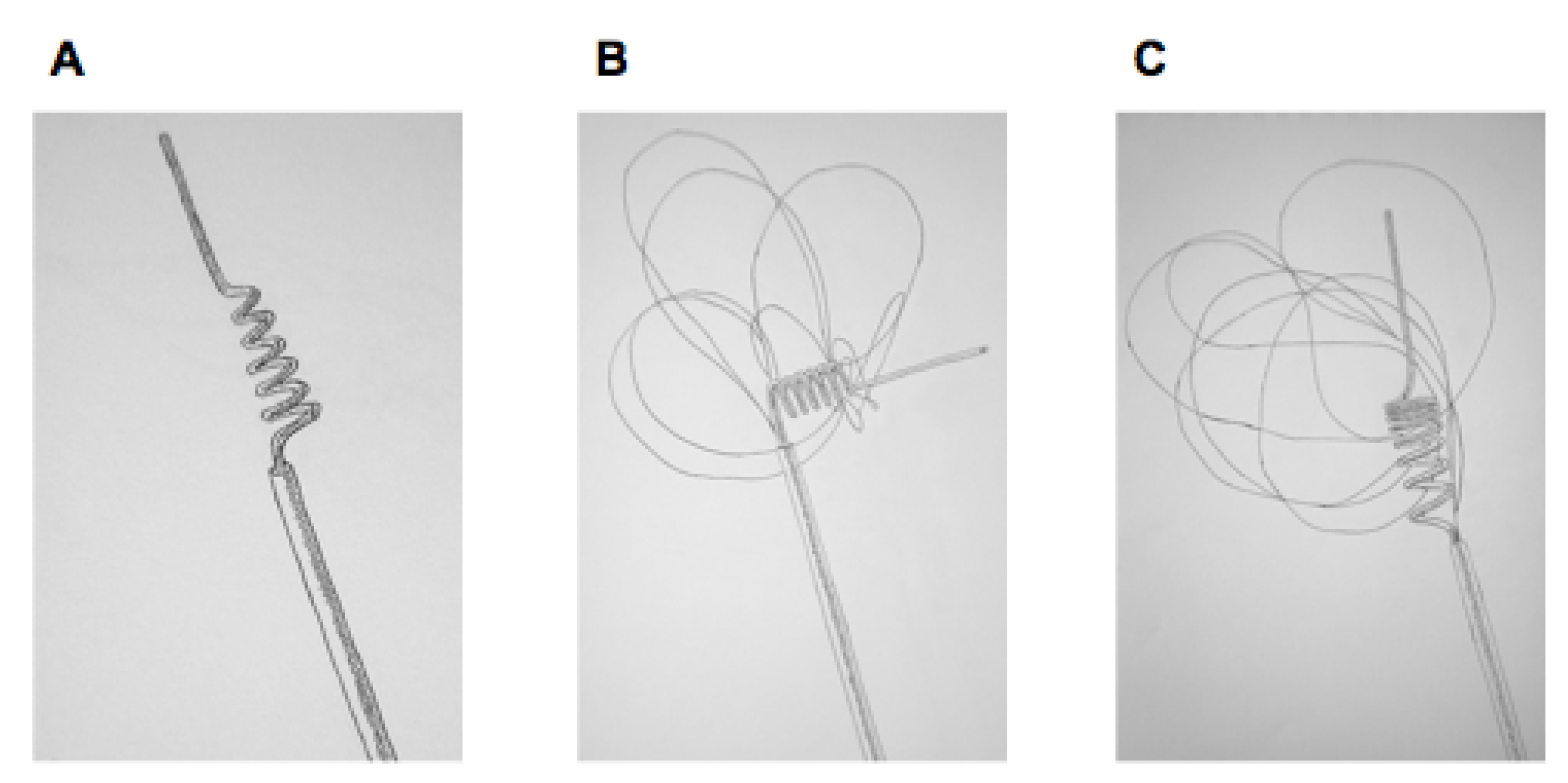
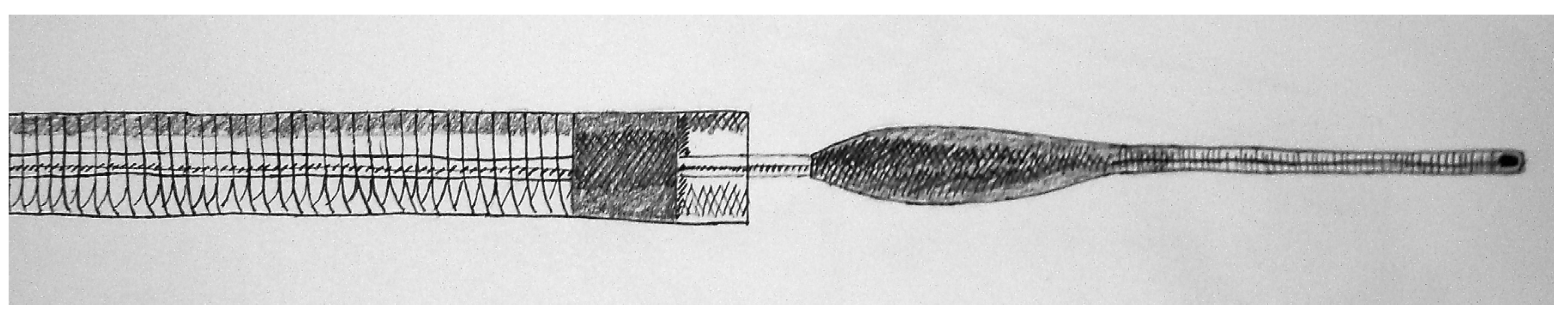
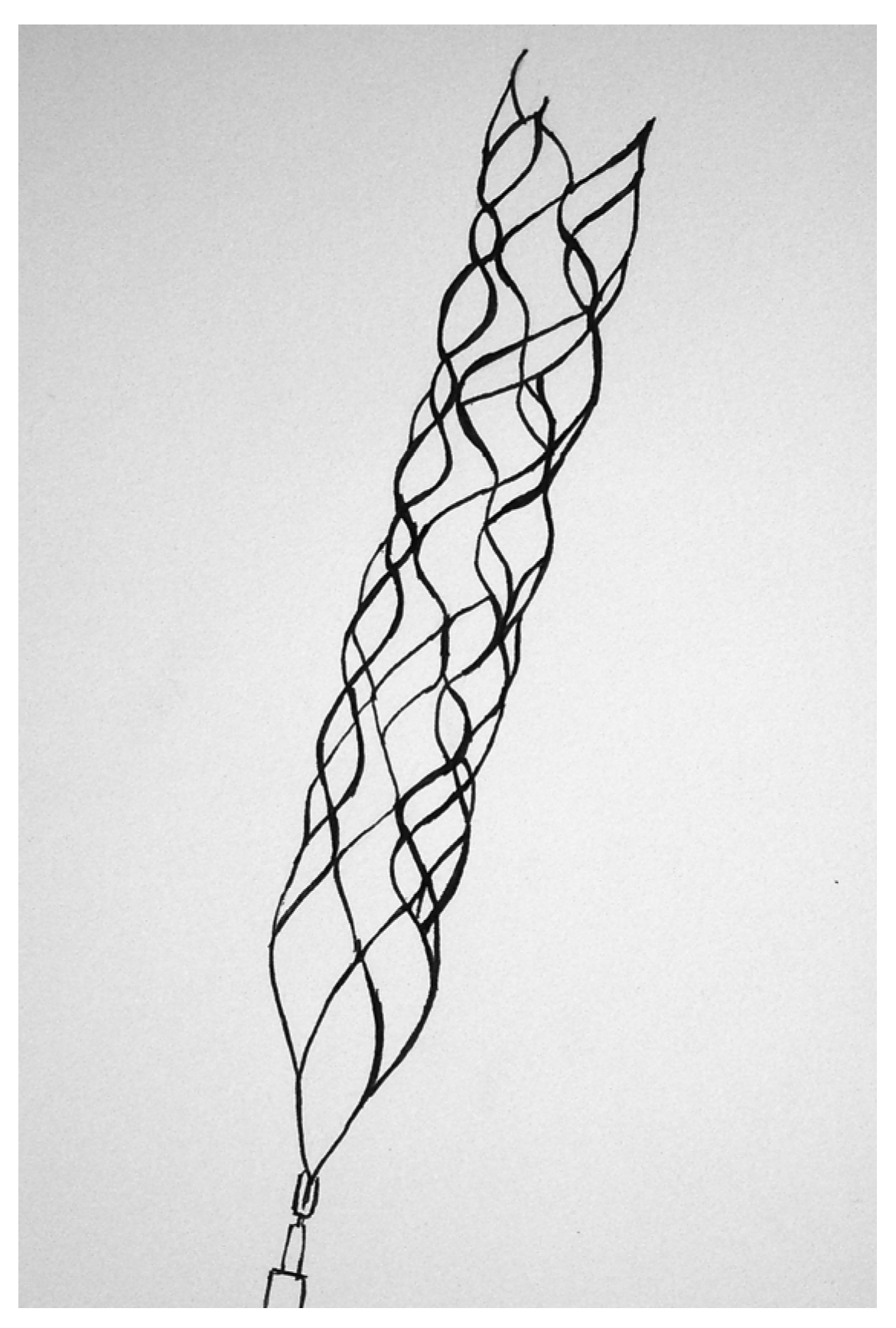
1.3.1. Distally Deployed Devices

1.3.2. Proximally Deployed Devices

1.3.3. Intra-Clot Deployed Devices

1.4. Combined Approaches
2. Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | TICI Recanalization | Degree of Recanalization |
|---|---|---|
| 0 | No perfusion distal to the occlusion | Incomplete |
| 1 | Perfusion past the site of occlusion, but no significant distal branch filling | |
| 2a | Incomplete (<50%) distal branch filling | Partial |
| 2b | Incomplete (>50%) distal branch filling | Complete or nearly complete |
| 3 | Full perfusion with filling of all distal branches |
3. Results
3.1. Pre-Procedural Data
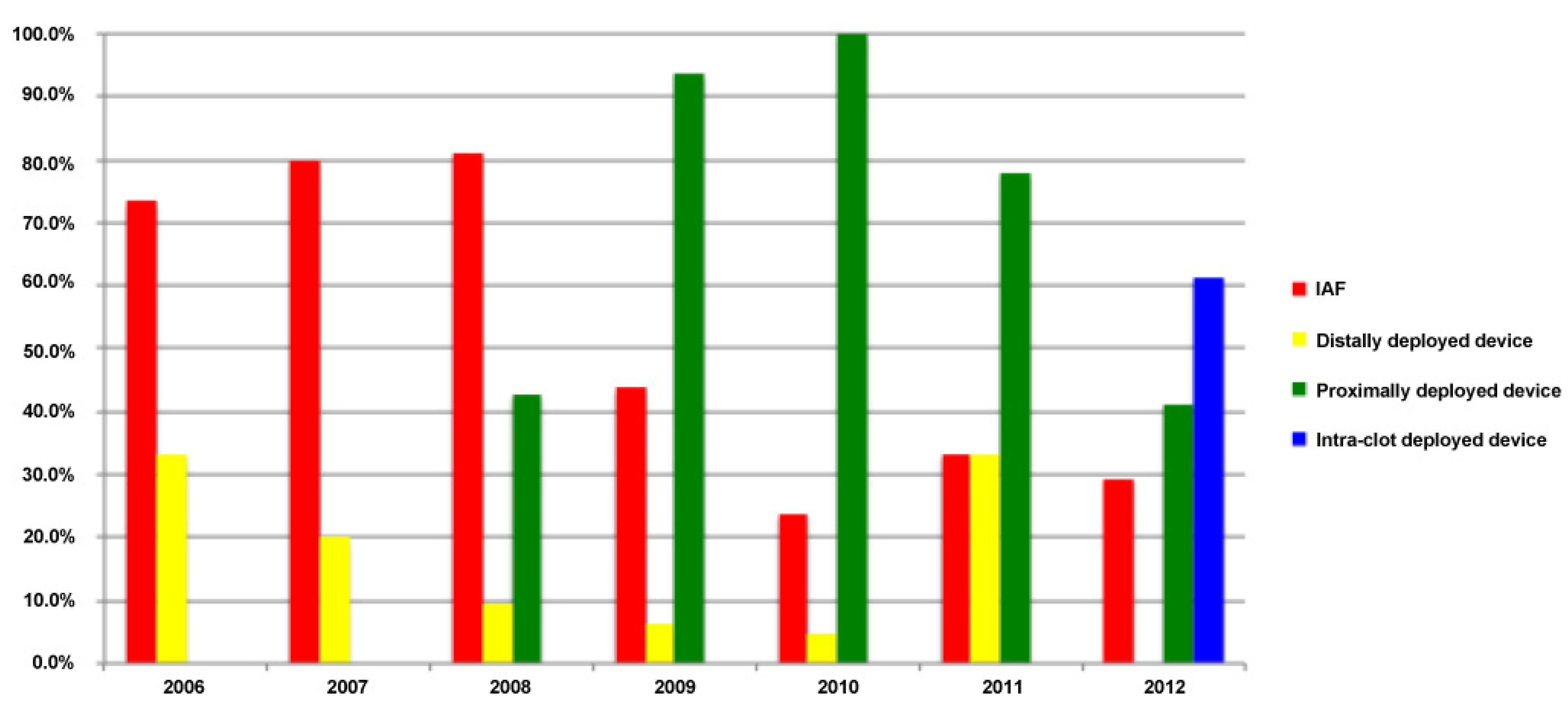
3.2. Procedural Data

| Degree of Recanalization | Number | Percentage | |
|---|---|---|---|
| Distally deployed device (n = 9) | |||
| Incomplete | 5/9 | 55.6% | |
| Partial | 4/9 | 44.4% | |
| Complete/nearly complete | 0/9 | 0.0% | |
| Proximally deployed device (n = 57) | |||
| Incomplete | 18/57 | 31.6% | |
| Partial | 16/57 | 28.1% | |
| Complete/nearly complete | 23/57 | 40.4% | |
| Combined proximally & distally deployed devices (n = 7) | |||
| Incomplete | 3/7 | 42.9% | |
| Partial | 2/7 | 28.6% | |
| Complete/nearly complete | 2/7 | 28.6% | |
| Intra-clot deployed device (n = 11) | |||
| Incomplete | 2/11 | 18.2% | |
| Partial | 0/11 | 0.0% | |
| Complete/nearly complete | 9/11 | 81.8% | |
3.3. Post-Procedural Data
| Total Reperfusion Hemorrhage | Symptomatic Reperfusion Hemorrhage | |||
|---|---|---|---|---|
| Total | 44/84 | 52.4% | 13/84 | 15.5% |
| With IVT | 18/31 | 58.1% | 7/31 | 22.6% |
| Without IVT | 26/53 | 49.1% | 6/53 | 11.3% |
| With IAF | 14/27 | 51.9% | 5/27 | 18.5% |
| Without IAF | 30/57 | 52.6% | 8/57 | 14.0% |
| Distally deployed device | 5/9 | 55.6% | 1/9 | 11.1% |
| Proximally deployed device | 29/57 | 50.9% | 9/57 | 15.8% |
| Combined proximally and distally deployed devices | 3/7 | 42.9% | 1/7 | 14.3% |
| Intra-clot deployed device | 7/11 | 63.6% | 2/11 | 18.2% |
| Good Outcome (mRS ≤ 2) | Death (mRS = 6) | |||
|---|---|---|---|---|
| Total | 14/84 | 16.7% | 25/84 | 29.8% |
| With IVT | 3/31 | 9.7% | 10/31 | 32.3% |
| Without IVT | 11/53 | 20.8% | 15/53 | 28.3% |
| With IAF | 7/27 | 25.9% | 8/27 | 29.6% |
| Without IAF | 7/57 | 12.3% | 17/57 | 29.8% |
| Distally deployed device | 1/9 | 11.1% | 2/9 | 22.2% |
| Proximally deployed device | 8/57 | 14.0% | 18/57 | 31.6% |
| Combined proximally and distally deployed devices | 1/7 | 14.3% | 2/7 | 28.6% |
| Intra-clot deployed device | 4/11 | 36.4% | 3/11 | 27.3% |
4. Discussion

5. Conclusions
Conflict of Interest
References
- Haley, E.C.; Lyden, P.D.; Johnston, K.C.; Hemmen, T.M. TNK in Stroke Investigators A pilot dose-escalation safety study of tenecteplase in acute ischemic stroke. Stroke 2005, 36, 607–612. [Google Scholar] [CrossRef]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Executive summary: Heart disease and stroke statistics—2012 update: A report from the American Heart Association. Circulation 2012, 125, 188–197. [Google Scholar] [CrossRef]
- Liberatore, G.T.; Samson, A.; Bladin, C.; Schleuning, W.-D.; Medcalf, R.L. Vampire bat salivary plasminogen activator (desmoteplase): A unique fibrinolytic enzyme that does not promote neurodegeneration. Stroke 2003, 34, 537–543. [Google Scholar] [CrossRef]
- Del Zoppo, G.J.; Higashida, R.T.; Furlan, A.J.; Pessin, M.S.; Rowley, H.A.; Gent, M. PROACT: A phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke 1998, 29, 4–11. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Ali, Z.; Suri, M.F.; Kim, S.H.; Shatla, A.A.; Ringer, A.J.; Lopes, D.K.; Guterman, L.R.; Hopkins, L.N. Intra-arterial third-generation recombinant tissue plasminogen activator (reteplase) for acute ischemic stroke. Neurosurgery 2001, 49, 41–48; discussion 48–50. [Google Scholar]
- Lapchak, P.A.; Araujo, D.M.; Pakola, S.; Song, D.; Wei, J.; Zivin, J.A. Microplasmin: A novel thrombolytic that improves behavioral outcome after embolic strokes in rabbits. Stroke 2002, 33, 2279–2284. [Google Scholar] [CrossRef]
- Adams, H.P.; Leclerc, J.R.; Bluhmki, E.; Clarke, W.; Hansen, M.D.; Hacke, W. Measuring outcomes as a function of baseline severity of ischemic stroke. Cerebrovasc. Dis. 2004, 18, 124–129. [Google Scholar] [CrossRef]
- Junghans, U.; Seitz, R.J.; Aulich, A.; Freund, H.J.; Siebler, M. Bleeding risk of tirofiban, a nonpeptide GPIIb/IIIa platelet receptor antagonist in progressive stroke: An open pilot study. Cerebrovasc. Dis. 2001, 12, 308–312. [Google Scholar] [CrossRef]
- Junghans, U.; Seitz, R.J.; Ritzl, A.; Wittsack, H.-J.; Fink, G.R.; Freund, H.J.; Siebler, M. Ischemic brain tissue salvaged from infarction by the GP IIb/IIIa platelet antagonist tirofiban. Neurology 2002, 58, 474–476. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Schwamm, L.H.; Hirsch, J.A. Endovascular approaches to acute stroke, part 1: Drugs, devices, and data. AJNR Am. J. Neuroradiol. 2009, 30, 649–661. [Google Scholar] [CrossRef]
- Rosamond, W.; Flegal, K.; Friday, G.; Furie, K.; Go, A.; Greenlund, K.; Haase, N.; Ho, M.; Howard, V.; Kissela, B.; et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2007 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007, 115, e69–e171. [Google Scholar] [CrossRef]
- Furlan, A.; Higashida, R.; Wechsler, L.; Gent, M.; Rowley, H.; Kase, C.; Pessin, M.; Ahuja, A.; Callahan, F.; Clark, W.M.; et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: A randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA 1999, 282, 2003–2011. [Google Scholar] [CrossRef]
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N. Engl. J. Med. 1995, 333, 1581–1587. [CrossRef]
- Jahan, R.; Duckwiler, G.R.; Kidwell, C.S.; Sayre, J.W.; Gobin, Y.P.; Villablanca, J.P.; Saver, J.; Starkman, S.; Martin, N.; Viñuela, F. Intraarterial thrombolysis for treatment of acute stroke: experience in 26 patients with long-term follow-up. AJNR Am. J. Neuroradiol. 1999, 20, 1291–1299. [Google Scholar]
- Caplan, L.R.; Mohr, J.P.; Kistler, J.P.; Koroshetz, W. Should thrombolytic therapy be the first-line treatment for acute ischemic stroke? Thrombolysis—not a panacea for ischemic stroke. N. Engl. J. Med. 1997, 337, 1309–1310; discussion 1313. [Google Scholar] [CrossRef]
- Ueda, T.; Sakaki, S.; Yuh, W.T.; Nochide, I.; Ohta, S. Outcome in acute stroke with successful intra-arterial thrombolysis and predictive value of initial single-photon emission-computed tomography. J. Cereb. Blood Flow Metab. 1999, 19, 99–108. [Google Scholar]
- Saver, J.L. Number needed to treat estimates incorporating effects over the entire range of clinical outcomes: Novel derivation method and application to thrombolytic therapy for acute stroke. Arch. Neurol. 2004, 61, 1066–1070. [Google Scholar] [CrossRef]
- Pillai, J.J.; Lanzieri, C.F.; Trinidad, S.B.; Tarr, R.W.; Sunshine, J.L.; Lewin, J.S. Initial angiographic appearance of intracranial vascular occlusions in acute stroke as a predictor of outcome of thrombolysis: Initial experience. Radiology 2001, 218, 733–738. [Google Scholar]
- Hacke, W.; Donnan, G.; Fieschi, C.; Kaste, M.; von Kummer, R.; Broderick, J.P.; Brott, T.; Frankel, M.; Grotta, J.C.; Haley, E.C.; et al. Association of outcome with early stroke treatment: Pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004, 363, 768–774. [Google Scholar] [CrossRef]
- Arnold, M.; Schroth, G.; Nedeltchev, K.; Loher, T.; Remonda, L.; Stepper, F.; Sturzenegger, M.; Mattle, H.P. Intra-arterial thrombolysis in 100 patients with acute stroke due to middle cerebral artery occlusion. Stroke 2002, 33, 1828–1833. [Google Scholar] [CrossRef]
- Rha, J.-H.; Saver, J.L. The impact of recanalization on ischemic stroke outcome: A meta-analysis. Stroke 2007, 38, 967–973. [Google Scholar] [CrossRef]
- Berlis, A.; Lutsep, H.; Barnwell, S.; Norbash, A.; Wechsler, L.; Jungreis, C.A.; Woolfenden, A.; Redekop, G.; Hartmann, M.; Schumacher, M. Mechanical thrombolysis in acute ischemic stroke with endovascular photoacoustic recanalization. Stroke 2004, 35, 1112–1116. [Google Scholar] [CrossRef]
- Lewandowski, C.A.; Frankel, M.; Tomsick, T.A.; Broderick, J.; Frey, J.; Clark, W.; Starkman, S.; Grotta, J.; Spilker, J.; Khoury, J.; Brott, T. Combined intravenous and intra-arterial r-TPA venous intra-arterial therapy of acute ischemic stroke: Emergency Management of Stroke (EMS) Bridging Trial. Stroke 1999, 30, 2598–2605. [Google Scholar] [CrossRef]
- Kleindorfer, D.; Lindsell, C.J.; Brass, L.; Koroshetz, W.; Broderick, J.P. National US estimates of recombinant tissue plasminogen activator use: ICD-9 codes substantially underestimate. Stroke 2008, 39, 924–928. [Google Scholar] [CrossRef]
- Sundt, T.M.; Smith, H.C.; Campbell, J.K.; Vlietstra, R.E.; Cucchiara, R.F.; Stanson, A.W. Transluminal angioplasty for basilar artery stenosis. Mayo Clin. Proc. 1980, 55, 673–680. [Google Scholar]
- Tomsick, T.; Broderick, J.; Carrozella, J.; Khatri, P.; Hill, M.; Palesch, Y.; Khoury, J. Interventional Management of Stroke II Investigators Revascularization results in the Interventional Management of Stroke II trial. AJNR Am. J. Neuroradiol. 2008, 29, 582–587. [Google Scholar] [CrossRef]
- IMS Study Investigators. Combined intravenous and intra-arterial recanalization for acute ischemic stroke: The Interventional Management of Stroke Study. Stroke 2004, 35, 904–911. [CrossRef]
- IMS II Trial Investigators. The Interventional Management of Stroke (IMS) II Study. Stroke 2007, 38, 2127–2135. [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- Khatri, P.; Hill, M.D.; Palesch, Y.Y.; Spilker, J.; Jauch, E.C.; Carrozzella, J.A.; Demchuk, A.M.; Martin, R.; Mauldin, P.; Dillon, C.; et al. Methodology of the Interventional Management of Stroke III Trial. Int. J. Stroke 2008, 3, 130–137. [Google Scholar] [CrossRef]
- Del Zoppo, G.J.; Saver, J.L.; Jauch, E.C.; Adams, H.P.; American Heart Association Stroke Council. Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: A science advisory from the American Heart Association/American Stroke Association. Stroke 2009, 40, 2945–2948. [Google Scholar] [CrossRef]
- Phatouros, C.C.; Higashida, R.T.; Malek, A.M.; Smith, W.S.; Mully, T.W.; DeArmond, S.J.; Dowd, C.F.; Halbach, V.V. Endovascular stenting of an acutely thrombosed basilar artery: Technical case report and review of the literature. Neurosurgery 1999, 44, 667–673. [Google Scholar] [CrossRef]
- Kleindorfer, D.; Kissela, B.; Schneider, A.; Woo, D.; Khoury, J.; Miller, R.; Alwell, K.; Gebel, J.; Szaflarski, J.; Pancioli, A.; et al. Eligibility for recombinant tissue plasminogen activator in acute ischemic stroke: A population-based study. Stroke 2004, 35, e27–e29. [Google Scholar] [CrossRef]
- Nakano, S.; Iseda, T.; Yoneyama, T.; Kawano, H.; Wakisaka, S. Direct percutaneous transluminal angioplasty for acute middle cerebral artery trunk occlusion: An alternative option to intra-arterial thrombolysis. Stroke 2002, 33, 2872–2876. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Schwamm, L.H.; Buonanno, F.S.; Koroshetz, W.J.; Yoo, A.J.; Rabinov, J.D.; Pryor, J.C.; Hirsch, J.A. Low-pressure balloon angioplasty with adjuvant pharmacological therapy in patients with acute ischemic stroke caused by intracranial arterial occlusions. Neuroradiology 2008, 50, 331–340. [Google Scholar] [CrossRef]
- Levy, E.I.; Siddiqui, A.H.; Crumlish, A.; Snyder, K.V.; Hauck, E.F.; Fiorella, D.J.; Hopkins, L.N.; Mocco, J. First Food and Drug Administration-approved prospective trial of primary intracranial stenting for acute stroke: SARIS (stent-assisted recanalization in acute ischemic stroke). Stroke 2009, 40, 3552–3556. [Google Scholar] [CrossRef]
- Booth, N.A.; Robbie, L.A.; Croll, A.M.; Bennett, B. Lysis of platelet-rich thrombi: The role of PAI-1. Ann. N. Y. Acad. Sci. 1992, 667, 70–80. [Google Scholar] [CrossRef]
- Brommer, E.J.; Potter van Loon, B.J.; Rijken, D.C.; van Bockel, J.H. Composition and susceptibility to thrombolysis of pathological human arterial thrombi. Ann. N. Y. Acad. Sci. 1992, 667, 283–285. [Google Scholar] [CrossRef]
- Gobin, Y.P.; Starkman, S.; Duckwiler, G.R.; Grobelny, T.; Kidwell, C.S.; Jahan, R.; Pile-Spellman, J.; Segal, A.; Viñuela, F.; Saver, J.L. MERCI 1: A phase 1 study of Mechanical Embolus Removal in Cerebral Ischemia. Stroke 2004, 35, 2848–2854. [Google Scholar] [CrossRef]
- Broderick, J.P.; Palesch, Y.Y.; Demchuk, A.M.; Yeatts, S.D.; Khatri, P.; Hill, M.D.; Jauch, E.C.; Jovin, T.G.; Yan, B.; Silver, F.L.; et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N. Engl. J. Med. 2013, 368, 893–903. [Google Scholar] [CrossRef]
- Xavier, A.R.; Tiwari, A.; Kansara, A. Angioplasty and stenting for mechanical thrombectomy in acute ischemic stroke. Neurology 2012, 79, S142–S147. [Google Scholar] [CrossRef]
- Roubec, M.; Kuliha, M.; Procházka, V.; Krajca, J.; Czerny, D.; Jonszta, T.; Krajina, A.; Sanák, D.; Langová, K.; Herzig, R.; Skoloudík, D. A Controlled Trial of Revascularization in Acute Stroke. Radiology 2012, 266, 871–878. [Google Scholar]
- Smith, W.S.; Sung, G.; Starkman, S.; Saver, J.L.; Kidwell, C.S.; Gobin, Y.P.; Lutsep, H.L.; Nesbit, G.M.; Grobelny, T.; Rymer, M.M.; et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: Results of the MERCI trial. Stroke 2005, 36, 1432–1438. [Google Scholar] [CrossRef]
- Smith, W.S.; Sung, G.; Saver, J.; Budzik, R.; Duckwiler, G.; Liebeskind, D.S.; Lutsep, H.L.; Rymer, M.M.; Higashida, R.T.; Starkman, S.; et al. Mechanical thrombectomy for acute ischemic stroke: Final results of the Multi MERCI trial. Stroke 2008, 39, 1205–1212. [Google Scholar] [CrossRef]
- Mayer, T.E.; Hamann, G.F.; Brueckmann, H. Mechanical extraction of a basilar-artery embolus with the use of flow reversal and a microbasket. N. Engl. J. Med. 2002, 347, 769–770. [Google Scholar] [CrossRef]
- Brekenfeld, C.; Schroth, G.; El-Koussy, M.; Nedeltchev, K.; Reinert, M.; Slotboom, J.; Gralla, J. Mechanical thromboembolectomy for acute ischemic stroke: Comparison of the catch thrombectomy device and the Merci Retriever in vivo. Stroke 2008, 39, 1213–1219. [Google Scholar] [CrossRef]
- Henkes, H.; Reinartz, J.; Lowens, S.; Miloslavski, E.; Roth, C.; Reith, W.; Kühne, D. A device for fast mechanical clot retrieval from intracranial arteries (Phenox clot retriever). Neurocrit. Care 2006, 5, 134–140. [Google Scholar] [CrossRef]
- Schumacher, H.C.; Meyers, P.M.; Yavagal, D.R.; Harel, N.Y.; Elkind, M.S.V.; Mohr, J.P.; Pile-Spellman, J. Endovascular mechanical thrombectomy of an occluded superior division branch of the left MCA for acute cardioembolic stroke. Cardiovasc. Intervent. Radiol. 2003, 26, 305–308. [Google Scholar] [CrossRef]
- Henkes, H.; Lowens, S.; Preiss, H.; Reinartz, J.; Miloslavski, E.; Kühne, D. A new device for endovascular coil retrieval from intracranial vessels: Alligator retrieval device. AJNR Am. J. Neuroradiol. 2006, 27, 327–329. [Google Scholar]
- Kerber, C.W.; Wanke, I.; Bernard, J.; Woo, H.H.; Liu, M.W.; Nelson, P.K. Rapid intracranial clot removal with a new device: The alligator retriever. AJNR Am. J. Neuroradiol. 2007, 28, 860–863. [Google Scholar]
- Bose, A.; Henkes, H.; Alfke, K.; Reith, W.; Mayer, T.E.; Berlis, A.; Branca, V.; Sit, S.P.; Penumbra Phase 1 Stroke Trial Investigators. The Penumbra System: A mechanical device for the treatment of acute stroke due to thromboembolism. AJNR Am. J. Neuroradiol. 2008, 29, 1409–1413. [Google Scholar] [CrossRef]
- Penumbra Pivotal Stroke Trial Investigators. The penumbra pivotal stroke trial: Safety and effectiveness of a new generation of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke 2009, 40, 2761–2768. [CrossRef]
- Tarr, R.; Hsu, D.; Kulcsar, Z.; Bonvin, C.; Rufenacht, D.; Alfke, K.; Stingele, R.; Jansen, O.; Frei, D.; Bellon, R.; et al. The POST trial: initial post-market experience of the Penumbra system: revascularization of large vessel occlusion in acute ischemic stroke in the United States and Europe. J. Neurointerv. Surg. 2010, 2, 341–344. [Google Scholar] [CrossRef]
- Ellis, J.A.; Youngerman, B.E.; Higashida, R.T.; Altschul, D.; Meyers, P.M. Endovascular treatment strategies for acute ischemic stroke. Int. J. Stroke 2011, 6, 511–522. [Google Scholar] [CrossRef]
- A Randomized, Concurrent Controlled Trial to Assess the Safety and Effectiveness of the Separator 3D as a Component of the Penumbra System in the Revascularization of Large Vessel Occlusion in Acute Ischemic Stroke. Available online: http://clinicaltrials.gov/show/NCT01584609 (accessed on 3 January 2013).
- Assess the Penumbra System in the Treatment of Acute Stroke (THERAPY). Available online: http://clinicaltrials.gov/show/NCT01429350 (accessed on 3 January 2013).
- Saver, J.L.; Jahan, R.; Levy, E.I.; Jovin, T.G.; Baxter, B.; Nogueira, R.G.; Clark, W.; Budzik, R.; Zaidat, O.O.; SWIFT Trialists. Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): A randomized, parallel-group, non-inferiority trial. Lancet 2012, 380, 1241–1249. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Lutsep, H.L.; Gupta, R.; Jovin, T.G.; Albers, G.W.; Walker, G.A.; Liebeskind, D.S.; Smith, W.S.; TREVO 2 Trialists. Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke (TREVO 2): A randomised trial. Lancet 2012, 380, 1231–1240. [Google Scholar] [CrossRef]
- Mendonça, N.; Flores, A.; Pagola, J.; Rubiera, M.; Rodríguez-Luna, D.; Miquel, M.A.D.; Cardona, P.; Quesada, H.; Mora, P.; Alvarez-Sabín, J.; et al. Trevo versus Solitaire a Head-to-Head Comparison between Two Heavy Weights of Clot Retrieval. J. Neuroimaging 2012. [Google Scholar] [CrossRef]
- Ciccone, A.; Valvassori, L.; Nichelatti, M.; Sgoifo, A.; Ponzio, M.; Sterzi, R.; Boccardi, E.; SYNTHESIS Expansion Investigators. Endovascular treatment for acute ischemic stroke. N. Engl. J. Med. 2013, 368, 904–913. [Google Scholar] [CrossRef]
- Kidwell, C.S.; Jahan, R.; Gornbein, J.; Alger, J.R.; Nenov, V.; Ajani, Z.; Feng, L.; Meyer, B.C.; Olson, S.; Schwamm, L.H.; et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N. Engl. J. Med. 2013, 368, 914–923. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sussman, E.; Kellner, C.; McDowell, M.; Yang, P.; Nelson, E.; Greenberg, S.; Sahlein, D.; Lavine, S.; Meyers, P.; Connolly, E.S. Endovascular Thrombectomy Following Acute Ischemic Stroke: A Single-Center Case Series and Critical Review of the Literature. Brain Sci. 2013, 3, 521-539. https://doi.org/10.3390/brainsci3020521
Sussman E, Kellner C, McDowell M, Yang P, Nelson E, Greenberg S, Sahlein D, Lavine S, Meyers P, Connolly ES. Endovascular Thrombectomy Following Acute Ischemic Stroke: A Single-Center Case Series and Critical Review of the Literature. Brain Sciences. 2013; 3(2):521-539. https://doi.org/10.3390/brainsci3020521
Chicago/Turabian StyleSussman, Eric, Christopher Kellner, Michael McDowell, Peter Yang, Eric Nelson, Sophie Greenberg, Daniel Sahlein, Sean Lavine, Philip Meyers, and E. Sander Connolly. 2013. "Endovascular Thrombectomy Following Acute Ischemic Stroke: A Single-Center Case Series and Critical Review of the Literature" Brain Sciences 3, no. 2: 521-539. https://doi.org/10.3390/brainsci3020521