
The Role of Ketamine in the Treatment of Bipolar Depression: A Scoping Review
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Study Inclusion
2.3. Data Extraction and Analysis
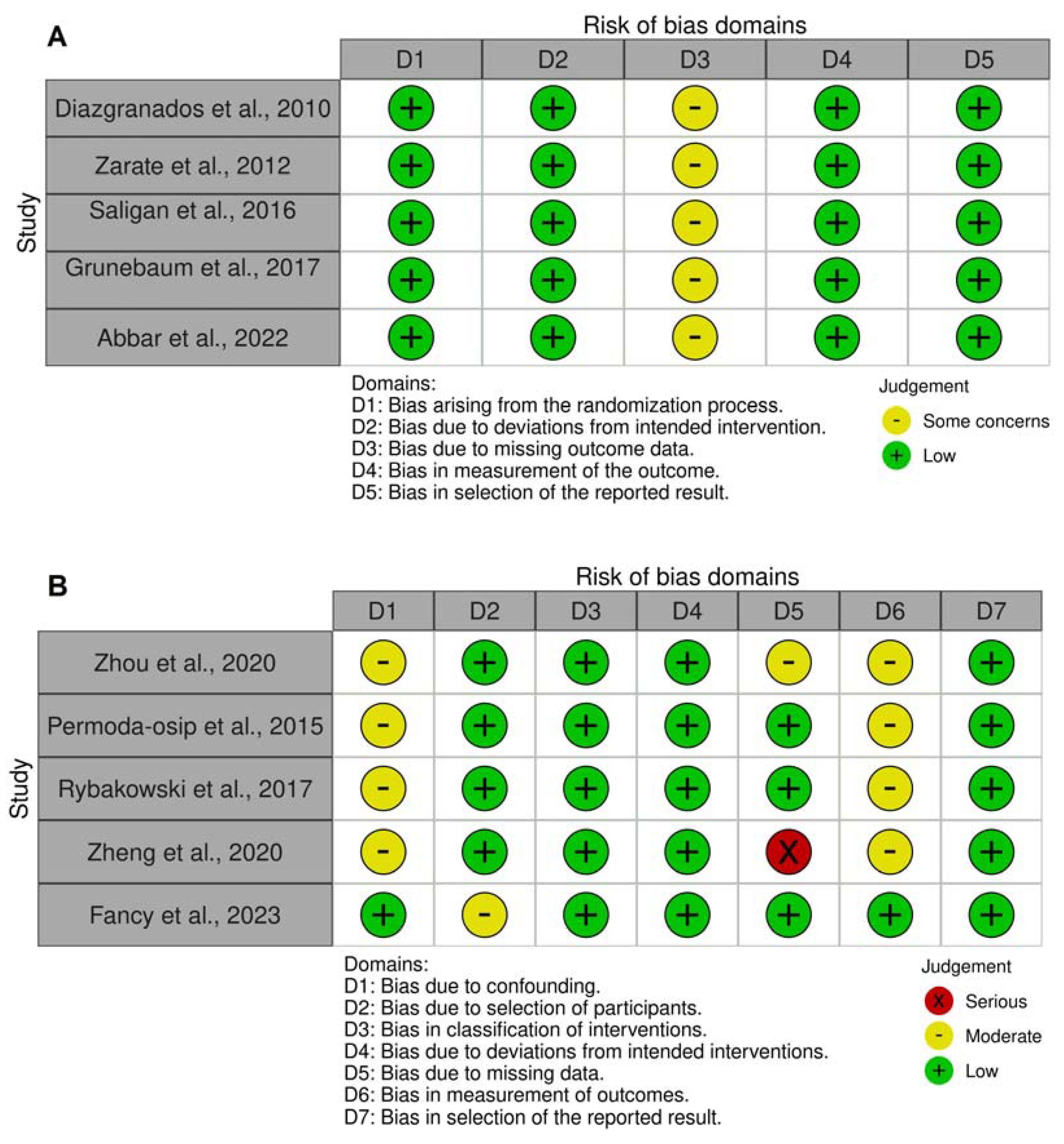
2.4. Risk of Bias Assessment
3. Results
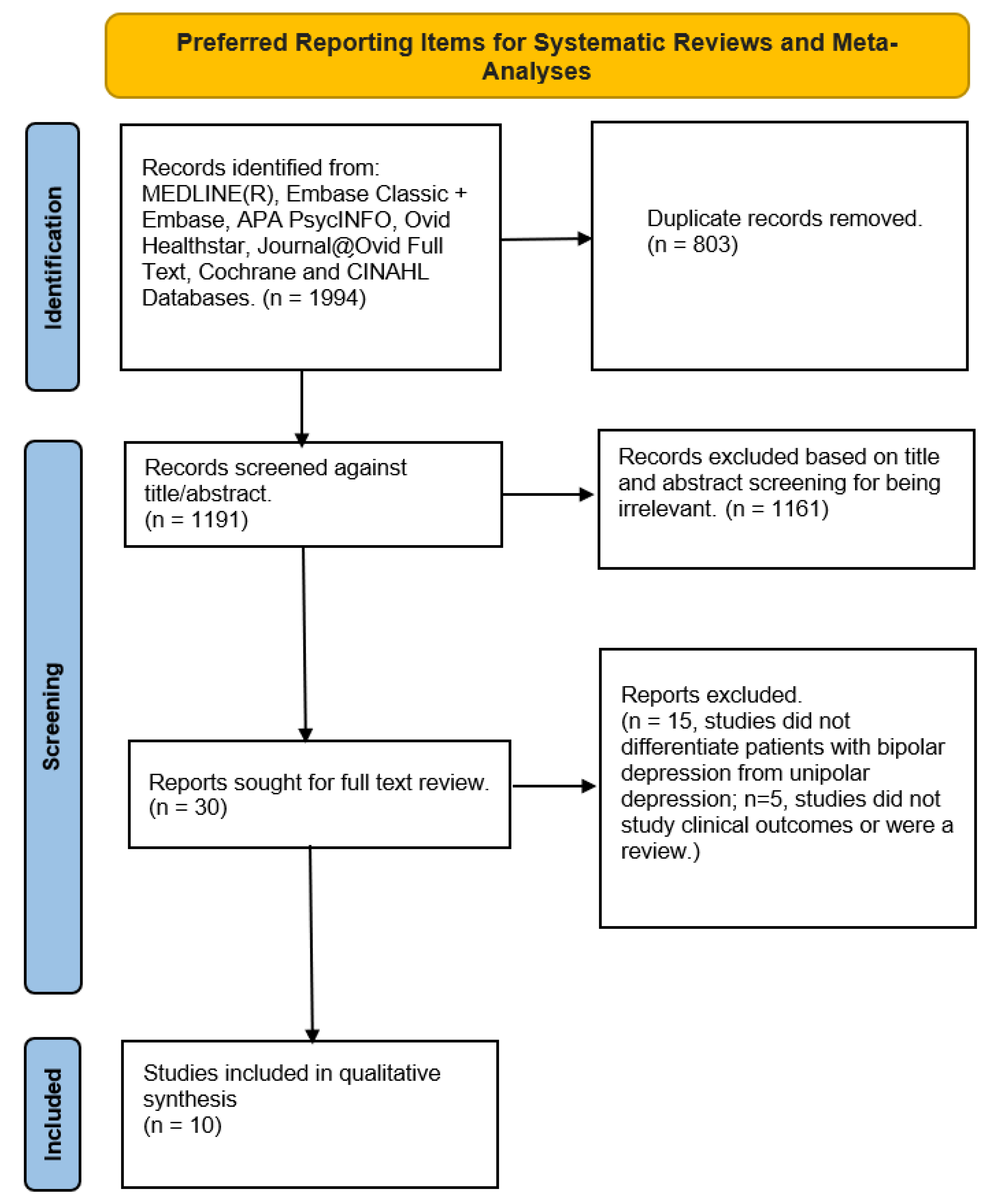
3.1. Search Results
3.2. Study Characteristics and Quality Appraisal
3.3. Efficacy of Ketamine Use in Bipolar Depression
3.4. Effectiveness of Ketamine Use in Bipolar Depression
3.5. Safety and Tolerability of Ketamine Use in Bipolar Depression
4. Discussion
4.1. Future Research
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vieta, E.; Berk, M.; Schulze, T.G.; Carvalho, A.F.; Suppes, T.; Calabrese, J.R.; Gao, K.; Miskowiak, K.W.; Grande, I. Bipolar Disorders. Nat. Rev. Dis. Primer 2018, 4, 18008. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.R. Prevalence and Correlates of Bipolar Spectrum Disorder in the World Mental Health Survey Initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E. Clinical Management and Burden of Bipolar Disorder: Results from a Multinational Longitudinal Study (WAVE-Bd). Int. J. Neuropsychopharmacol. 2013, 16, 1719–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berk, M. Staging in Bipolar Disorder: From Theoretical Framework to Clinical Utility. World Psychiatry 2017, 16, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, A.F.; Firth, J.; Vieta, E. Bipolar Disorder. N. Engl. J. Med. 2020, 383, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Bonnín, C.d.M.; Reinares, M.; Martínez-Arán, A.; Jiménez, E.; Sánchez-Moreno, J.; Solé, B.; Montejo, L.; Vieta, E. Improving Functioning, Quality of Life, and Well-Being in Patients with Bipolar Disorder. Int. J. Neuropsychopharmacol. 2019, 22, 467–477. [Google Scholar] [CrossRef]
- Altamura, A.C. Duration of Untreated Illness and Suicide in Bipolar Disorder: A Naturalistic Study. Eur. Arch. Psychiatry Clin. Neurosci. 2010, 260, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Gonda, X. Suicidal Behaviour in Bipolar Disorder: Epidemiology, Characteristics and Major Risk Factors. J. Affect. Disord. 2012, 143, 16–26. [Google Scholar] [CrossRef]
- Dome, P.; Rihmer, Z.; Gonda, X. Suicide Risk in Bipolar Disorder: A Brief Review. Medicina 2019, 55, 403. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, R.S.; Calabrese, J.R. Bipolar Depression: The Clinical Characteristics and Unmet Needs of a Complex Disorder. Curr. Med. Res. Opin. 2019, 35, 1993–2005. [Google Scholar] [CrossRef] [Green Version]
- Levenberg, K.; Cordner, Z.A. Bipolar Depression: A Review of Treatment Options. Gen. Psychiatry 2022, 35, e100760. [Google Scholar] [CrossRef]
- Muneer, A. Pharmacotherapy of Bipolar Disorder with Quetiapine: A Recent Literature Review and an Update. Clin. Psychopharmacol. Neurosci. 2015, 13, 25–35. [Google Scholar] [CrossRef] [Green Version]
- Jawad, M.Y.; Alnefeesi, Y.; Lui, L.M.W.; Ceban, F.; Chen-Li, D.C.J.; Teopiz, K.; Jaberi, S.; Gillissie, E.S.; Vincenzo, J.D.D.; Rosenblat, J.D.; et al. Olanzapine and Samidorphan Combination Treatment: A Systematic Review. J. Affect. Disord. 2022, 301, 99–106. [Google Scholar] [CrossRef]
- Blair, H.A. Lumateperone: First Approval. Drugs 2020, 80, 417–423. [Google Scholar] [CrossRef]
- Jawad, M.Y.; Alnefeesi, Y.; Ceban, F.; Lui, L.M.W.; Jaberi, S.; Di Vincenzo, J.D.; Amirbeik, L.; Chen-Li, D.C.J.; Teopiz, K.; Phan, L.; et al. Lumateperone for the Treatment of Adults With Schizophrenia: A Systematic Review. Curr. Psychiatry Rep. 2022, 24, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Volkmann, C.; Bschor, T.; Köhler, S. Lithium Treatment Over the Lifespan in Bipolar Disorders. Front. Psychiatry 2020, 11, 377. [Google Scholar] [CrossRef]
- Diaz, A.P.; Fernandes, B.S.; Quevedo, J.; Sanches, M.; Soares, J.C. Treatment-Resistant Bipolar Depression: Concepts and Challenges for Novel Interventions. Braz. J. Psychiatry 2021, 44, 178–186. [Google Scholar] [CrossRef]
- Martinez-Aran, A. Functional Outcome in Bipolar Disorder: The Role of Clinical and Cognitive Factors. Bipolar Disord. 2007, 9, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Levinson, A.J.; Young, L.T.; Fitzgerald, P.B.; Daskalakis, Z.J. Cortical Inhibitory Dysfunction in Bipolar Disorder: A Study Using Transcranial Magnetic Stimulation. J. Clin. Psychopharmacol. 2007, 27, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Wassermann, E.M.; Greenberg, B.D.; Nguyen, M.B.; Murphy, D.L. Motor Cortex Excitability Correlates with an Anxiety-Related Personality Trait. Biol. Psychiatry 2001, 50, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Daskalakis, Z.J.; Christensen, B.K.; Chen, R.; Fitzgerald, P.B.; Zipursky, R.B.; Kapur, S. Evidence for Impaired Cortical Inhibition in Schizophrenia Using Transcranial Magnetic Stimulation. Arch. Gen. Psychiatry 2002, 59, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Hagihara, H.; Takao, K.; Walton, N.M.; Matsumoto, M.; Miyakawa, T. Immature Dentate Gyrus: An Endophenotype of Neuropsychiatric Disorders. Neural Plast. 2013, 2013, 318596. [Google Scholar] [CrossRef] [Green Version]
- Yamasaki, N.; Maekawa, M.; Kobayashi, K.; Kajii, Y.; Maeda, J.; Soma, M.; Takao, K.; Tanda, K.; Ohira, K.; Toyama, K.; et al. Alpha-CaMKII Deficiency Causes Immature Dentate Gyrus, a Novel Candidate Endophenotype of Psychiatric Disorders. Mol. Brain 2008, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, S.; Nazzi, C.; Thayer, J.F. Fear-Induced Bradycardia in Mental Disorders: Foundations, Current Advances, Future Perspectives. Neurosci. Biobehav. Rev. 2023, 149, 105163. [Google Scholar] [CrossRef]
- Battaglia, S.; Di Fazio, C.; Vicario, C.M.; Avenanti, A. Neuropharmacological Modulation of N-Methyl-D-Aspartate, Noradrenaline and Endocannabinoid Receptors in Fear Extinction Learning: Synaptic Transmission and Plasticity. Int. J. Mol. Sci. 2023, 24, 5926. [Google Scholar] [CrossRef] [PubMed]
- Jawad, M.Y.; Di Vincenzo, J.D.; Ceban, F.; Jaberi, S.; Lui, L.M.W.; Gillissie, E.S.; Alnafeesi, Y.; Rosenblat, J.D.; McIntyre, R.S. The Efficacy and Safety of Adjunctive Intranasal Esketamine Treatment in Major Depressive Disorder: A Systematic Review and Meta-Analysis. Expert. Opin. Drug. Saf. 2022, 21, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Alnefeesi, Y.; Chen-Li, D.; Krane, E.; Jawad, M.Y.; Rodrigues, N.B.; Ceban, F.; Di Vincenzo, J.D.; Meshkat, S.; Ho, R.C.M.; Gill, H.; et al. Real-World Effectiveness of Ketamine in Treatment-Resistant Depression: A Systematic Review & Meta-Analysis. J. Psychiatr. Res. 2022, 151, 693–709. [Google Scholar] [CrossRef] [PubMed]
- Bahji, A.; Zarate, C.A.; Vazquez, G.H. Ketamine for Bipolar Depression: A Systematic Review. Int. J. Neuropsychopharmacol. 2021, 24, 535–541. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Chen-Li, D.; Rosenblat, J.D.; Rodrigues, N.B.; Carvalho, I.; Lui, L.M.W.; Gill, H.; Narsi, F.; Mansur, R.B.; et al. The Acute Antisuicidal Effects of Single-Dose Intravenous Ketamine and Intranasal Esketamine in Individuals with Major Depression and Bipolar Disorders: A Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2021, 134, 57–68. [Google Scholar] [CrossRef] [PubMed]
- d’Andrea, G.; Pettorruso, M.; Lorenzo, G.D.; Mancusi, G.; McIntyre, R.S.; Martinotti, G. Rethinking Ketamine and Esketamine Action: Are They Antidepressants with Mood-Stabilizing Properties? Eur. Neuropsychopharmacol. 2023, 70, 49–55. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, R.S.; Berk, M.; Brietzke, E.; Goldstein, B.I.; López-Jaramillo, C.; Kessing, L.V.; Malhi, G.S.; Nierenberg, A.A.; Rosenblat, J.D.; Majeed, A.; et al. Bipolar Disorders. Lancet 2020, 396, 1841–1856. [Google Scholar] [CrossRef]
- Cuellar, A.K.; Johnson, S.L.; Winters, R. Distinctions between Bipolar and Unipolar Depression. Clin. Psychol. Rev. 2005, 25, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 6 August 2021).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diazgranados, N.; Ibrahim, L.; Brutsche, N.E.; Newberg, A.; Kronstein, P.; Khalife, S.; Kammerer, W.A.; Quezado, Z.; Luckenbaugh, D.A.; Salvadore, G.; et al. A Randomized Add-on Trial of an N-Methyl-D-Aspartate Antagonist in Treatment-Resistant Bipolar Depression. Arch. Gen. Psychiatry 2010, 67, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Zarate, C.A.; Brutsche, N.E.; Ibrahim, L.; Franco-Chaves, J.; Diazgranados, N.; Cravchik, A.; Selter, J.; Marquardt, C.A.; Liberty, V.; Luckenbaugh, D. A. Replication of Ketamine’s Antidepressant Efficacy in Bipolar Depression: A Randomized Controlled Add-on Trial. Biol. Psychiatry 2012, 71, 939–946. [Google Scholar] [CrossRef] [Green Version]
- Grunebaum, M.F.; Ellis, S.P.; Keilp, J.G.; Moitra, V.K.; Cooper, T.B.; Marver, J.E.; Burke, A.K.; Milak, M.S.; Sublette, M.E.; Oquendo, M.A.; et al. Ketamine versus Midazolam in Bipolar Depression with Suicidal Thoughts: A Pilot Midazolam-Controlled Randomized Clinical Trial. Bipolar Disord. 2017, 19, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Abbar, M.; Demattei, C.; El-Hage, W.; Llorca, P.-M.; Samalin, L.; Demaricourt, P.; Gaillard, R.; Courtet, P.; Vaiva, G.; Gorwood, P.; et al. Ketamine for the Acute Treatment of Severe Suicidal Ideation: Double Blind, Randomised Placebo Controlled Trial. BMJ 2022, 376, e067194. [Google Scholar] [CrossRef] [PubMed]
- Saligan, L.N.; Luckenbaugh, D.A.; Slonena, E.E.; Machado-Vieira, R.; Zarate, C.A.J. An Assessment of the Anti-Fatigue Effects of Ketamine from a Double-Blind, Placebo-Controlled, Crossover Study in Bipolar Disorder. J. Affect. Disord. 2016, 194, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Rybakowski, J.K.; Permoda-Osip, A.; Bartkowska-Sniatkowska, A. Ketamine Augmentation Rapidly Improves Depression Scores in Inpatients with Treatment-Resistant Bipolar Depression. Int. J. Psychiatry Clin. Pract. 2017, 21, 99–103. [Google Scholar] [CrossRef]
- Zhuo, C.; Ji, F.; Tian, H.; Wang, L.; Jia, F.; Jiang, D.; Chen, C.; Zhou, C.; Lin, X.; Zhu, J. Transient Effects of Multi-Infusion Ketamine Augmentation on Treatment-Resistant Depressive Symptoms in Patients with Treatment-Resistant Bipolar Depression—An Open-Label Three-Week Pilot Study. Brain Behav. 2020, 10, e01674. [Google Scholar] [CrossRef]
- Zheng, W.; Zhou, Y.-L.; Liu, W.-J.; Wang, C.-Y.; Zhan, Y.-N.; Lan, X.-F.; Zhang, B.; Ning, Y.-P. A Preliminary Study of Adjunctive Ketamine for Treatment-Resistant Bipolar Depression. J. Affect. Disord. 2020, 275, 38–43. [Google Scholar] [CrossRef]
- Fancy, F.; Rodrigues, N.B.; Di Vincenzo, J.D.; Chau, E.H.; Sethi, R.; Husain, M.I.; Gill, H.; Tabassum, A.; Mckenzie, A.; Phan, L.; et al. Real-World Effectiveness of Repeated Ketamine Infusions for Treatment-Resistant Bipolar Depression. Bipolar Disord. 2023, 25, 99–109. [Google Scholar] [CrossRef]
- Permoda-Osip, A.; Kisielewski, J.; Bartkowska-Sniatkowska, A.; Rybakowski, J.K. Single Ketamine Infusion and Neurocognitive Performance in Bipolar Depression. Pharmacopsychiatry 2015, 48, 78–79. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Rosenblat, J.D.; Nemeroff, C.B.; Sanacora, G.; Murrough, J.W.; Berk, M.; Brietzke, E.; Dodd, S.; Gorwood, P.; Ho, R.; et al. Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. Am. J. Psychiatry 2021, 178, 383–399. [Google Scholar] [CrossRef]
- Zheng, W.; Gu, L.-M.; Sun, C.-H.; Zhou, Y.-L.; Wang, C.-Y.; Lan, X.-F.; Zhang, B.; Ning, Y.-P. Comparative Effectiveness of Repeated Ketamine Infusions in Treating Anhedonia in Bipolar and Unipolar Depression. J. Affect. Disord. 2022, 300, 109–113. [Google Scholar] [CrossRef]
- Li, W.; Zhou, Y.; Liu, W.; Wang, C.; Lan, X.; Zhang, Z.; Zhang, F.; Ye, Y.; Liu, H.; Wu, K.; et al. Long-Term Outcomes of Repeated Ketamine Infusions in Patients with Unipolar and Bipolar Depression: A Naturalistic Follow-up Study. J. Affect. Disord. 2022, 300, 172–178. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Lipsitz, O.; Rodrigues, N.B.; Lee, Y.; Cha, D.S.; Vinberg, M.; Lin, K.; Malhi, G.S.; Subramaniapillai, M.; Kratiuk, K.; et al. The Effectiveness of Ketamine on Anxiety, Irritability, and Agitation: Implications for Treating Mixed Features in Adults with Major Depressive or Bipolar Disorder. Bipolar Disord. 2020, 22, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, N.B.; McIntyre, R.S.; Lipsitz, O.; Lee, Y.; Subramaniapillai, M.; Kratiuk, K.; Majeed, A.; Nasri, F.; Gill, H.; Mansur, R.B.; et al. The Effect of Repeated Doses of Intravenous Ketamine on Measures of Workplace Attendance and Productivity in Adults with Major Depressive and Bipolar Disorder: Results from the Canadian Rapid Treatment Center of Excellence. Psychiatry Res. 2021, 300, 113860. [Google Scholar] [CrossRef]
- Rodrigues, N.B.; McIntyre, R.S.; Lipsitz, O.; Cha, D.S.; Lee, Y.; Gill, H.; Majeed, A.; Phan, L.; Nasri, F.; Ho, R.; et al. Changes in Symptoms of Anhedonia in Adults with Major Depressive or Bipolar Disorder Receiving IV Ketamine: Results from the Canadian Rapid Treatment Center of Excellence. J. Affect. Disord. 2020, 276, 570–575. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sr. No. | Lead Author | Study Type | Total Participants | Intervention (Dosage) | Control | Concomitant Medications | Primary Objective | Psychometric Tool Used | Findings | Any Report of Hypomanic/Manic Switching | Limitations |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Zhuo et al., 2020 | Open label study (3-week) | 38 patients with treatment-resistant bipolar disorder (TRBD); 22 males and 16 females. | 0.5 mg/kg; Total 10 infusions | None | Patients continued their original medication regimen including mood stabilizers and antipsychotics. | Therapeutic effects and associated brain alterations following multi-infusion ketamine augmentation in patients with TRBD. | 17-item Hamilton Depression Scale (HAMD-17) | Significant differences in HAMD scores after 1 week. (mean reduction = 49.8%, p < 0.05). However, relapse of symptoms in 2nd week. By the 21st day, more severe depressive symptoms were reported compared to the baseline. (Baseline HAMD score: 36.5 ± 2.8 and at 21st day: 39.0 ± 2.4). | None reported | Use of self-comparison (no control). Short duration (3-weeks). Excluded patients with suicidal ideation. |
| 2. | Permoda-Osip et al., 2015 | Non-randomized, uncontrolled trial | 18 patients with baseline Hamilton Depression Rating Scale (HDRS) score more than 18 (4 males and 14 females). | A single dose of 0.5 mg/kg over 45 min | None | Mood stabilizers throughout the duration of the study. Antidepressants were stopped 7 days before infusion. | To measure the change in neurocognitive performance before and on the 3rd day after a single dose of ketamine infusion in patients with a diagnosis of bipolar disorder and in depressed state taking mood stabilizing drugs and to correlate it with the antidepressant effect of the intervention. | 17-item Hamilton Depression Rating Scale (HDRS) Neurocognitive tests: Trail making test (TMT) and Stroop color-word interference test | The HDRS scores were reduced by an average of 11 points on the 3rd day and by 12 points on the 7th day post-infusion (24 ± 5, 13 ± 6, and 12 ± 7, respectively). Eight patients had at least 50% reduction of HDRS scores on the 7th day compared to the baseline. Performance on neurocognitive tests improved significantly on the 3rd day after infusion. The degree of improvement in the neurocognitive test scores correlated positively with the degree of baseline impairment on the tests. | None reported | Small sample size. No control group. Possible practice effect on cognitive test performance (with no control group to control the bias). Discontinuation of antidepressants 7 days before the intervention might have fluctuated the cognition. |
| 3. | Rybakowski et al., 2017 | Open label clinical trial | 53 patients (13 males and 40 females) with bipolar disorder with depression score of at least 18 on HDRS Scale. | A single dose of 0.5 mg/kg over 40 min | None | Mood stabilizers throughout the duration of the study. Most of the patients were receiving more than one mood stabilizer. Antidepressants were stopped 7 days before infusion. | To investigate the effectiveness of a single ketamine infusion in patients with bipolar disorder. | 17-item Hamilton Depression Rating Scale (HDRS) | 13 patients met the criteria for response (50% reduction in HDRS scores) at 24 h and 27 patients met the criteria at day 7. The criteria for remission was met by 8 and 14 patients at day 1 and 7, respectively. The response was significantly more frequent in males than females. | None reported (within the 7-day period) | Open label. Uneven gender proportion. Antidepressants were tapered off only 7 days before infusion. |
| 4. | Grunebaum et al., 2017 | Randomized clinical trial | 16 patients (10 females and 6 males) with scores ≥ 16 on HDRS-17 and a score of ≥ 4 on the scale for suicidal ideation (SSI). | Ketamine hydrochloride 0.5 mg/kg in 100 mL of saline over 40 min | Midazolam 0.02 mg/kg in 100 mL of saline over 40 min | Patients continued to take the psychometric drugs they were taking except for the benzodiazepines up to 24 h before infusion. | A feasibility study to evaluate the effect of ketamine versus midazolam infusion on suicidal ideation in bipolar depression. | Clinician-rated SSI for suicidal ideation Hamilton Depression Rating Scale (HDRS-17) | There was an estimated decrease of 5.84 points on SSI at day 1 for patients on ketamine compared to the midazolam group (p = 0.074). Similar results were reported for improvement in HDRS-17 scale (six-point decrease with p = 0.109). 4 out of 7 on ketamine were classified as responders (50% response) compared to 1 out of 9 for midazolam (CI not significant). Similarly, 3/7 in the ketamine group were remitters compared to 1/9 randomized to midazolam. | None reported | Small pilot sample (limited power). Lower than recommended dose of midazolam was used which might have minimized the effect of midazolam. |
| 5. | Zheng et al., 2020 | Single arm open label trial | 16 patients (13 males and 3 females). | Six intravenous infusions of 0.5 mg/kg ketamine over 40 min on a thrice weekly basis were administered. | Self-control (Results after the first infusion were compared with the results after the sixth infusion). | Patients continued to take the prescribed antidepressant regimen (at least 4 weeks before screening and infusion) along with other psychotropic agents as augmentation. | A pilot study investigating the antidepressant, anti-suicidal effects and safety of six consecutive infusions of ketamine. | Montgomery–Asberg Depression Rating Scale (MADRS) | After 1st infusion: Rate of response and remission reported as 21.1% (95% CI = 0.9–21.2) and 15.8% (95% CI = 0–33.9), respectively. After 6th infusion: Rate of response and remission are 73.7% (95% CI = 51.9–95.5) and 63.2% (95% CI = 39.3–87.0), respectively. Large and significant decreases in both MADRS scores and SSI-part-1 were noted: 5.8, p < 0.001 and 0.8, p = 0.018. These findings were maintained across the subsequent infusions. | None reported | Small sample size. No control group. Short follow up period of only 2 weeks. |
| 6. | Fancy et al., 2023 | Open label Observational Study | 66 patients with treatment-resistant bipolar disorder (27 males and 39 females). | Four intravenous infusions of ketamine 0.5–0.75 mg/kg over a 40-min period. Started with 2 doses of 0.5 mg/kg and increased to 0.75 mg/kg in the 3rd and 4th infusion in case of inadequate response. | None | Patients continued to take their prescribed psychotropic medication. | To evaluate the real-word effectiveness of repeated ketamine infusions for TRBD in a community clinic setting. | Quick Inventory for Depression Symptomatology-Self Report-16 (QIDS-SR16) Generalized Anxiety Disorder-7 (GAD-7) Sheehan Disability Scale | There was a significant reduction of QIDS-SR16 scores from baseline to all subsequent timepoints (p < 0.001). In addition, a significant difference was observed in the QIDS-SR16 scores from post-infusion 1 to post-infusion 3 (p < 0.001) and post-treatment assessment visit (p < 0.05). 35% of patients were classified as responders (50% response) and 20% patients achieved remission at follow-up 1 week following the fourth infusion. QIDS suicidality item score decreased significantly over time with treatment (p < 0.001). The difference was also significant between post-infusion scores and post-treatment scores (p < 0.05). Anxiety scores also decreased significantly from baseline to post-infusion 3 and post-treatment (p < 0.05 and p < 0.001, respectively). | Treatment emergent hypomania in three patients (4.5%)–might be due to co-administration of antidepressants. No case of mania reported. | No control group. Small sample size. Patients were required to bear the cost of the treatment leading to a potential selection or expectancy bias. Potential confounding by psychotropic drugs or medical comorbidities as study was conducted on patients under treatment at the community clinic. |
| 7. | Diazgranados et al., 2010 | Randomized controlled trial | 18 patients with TRBD.(12 females and 6 males). | 0.5 mg/kg infused in normal saline. | 0.9% Normal saline | Patients were only allowed to take lithium or valproate only. | To determine whether an N-methyl-daspartate–receptor antagonist produces rapid antidepressant effects in subjects with bipolar depression. | Montgomery–Åsberg Depression Rating Scale (MADRS) | The effect sizes for change in MADRS were 0.52 (95% confidence interval (CI), 0.28–0.76) at 40 min, 0.67 (95% CI, 0.42– 0.91) at day 1, and 0.22 (95% CI, −0.03 to 0.48) at day 14. The largest effect was seen 2 days after infusion (d = 0.80; 95% CI, 0.55–1.04) | One participant in ketamine and one participant in control group developed mania. | Small sample size. Normal saline could have masked proper blinding. Tapering of some of the current medications might have led to bias. |
| 8. | Zarate et al., 2012 | Randomized controlled trial | 15 with bipolar disorder (8 females and 7 males). | 0.5 mg/kg infused in normal saline. | 0.9% Normal saline | Patients were only allowed to take lithium or valproate only) | The efficacy of ketamine infusion in reducing depressive symptoms in bipolar depression | MADRS | Depressive symptoms as well as suicidal ideation significantly improved in subjects receiving ketamine compared to placebo (d = 0.89, 95% C.I. = 0.61–1.16 and 0.98, 95% C.I. = 0.64–1.33, respectively); this improvement remained significant through Day 3. | None reported | Small sample size. Normal saline could have masked proper blinding. Tapering of some of the current medications might have led to bias. |
| 9. | Saligan et al., 2016 | Exploratory analysis of randomized crossover-controlled trial. | 36 bipolar depression patients (21 females and 15 males). | 0.5 mg/kg infused in normal saline. | 0.9% Normal saline | Patients were only allowed to take lithium or valproate only. | To study anti-fatigue properties of ketamine in bipolar depression. | NIH-Brief Fatigue Inventory (NIH-BFI) | Ketamine lowered fatigue scores compared to placebo from 40 min post-treatment. The largest anti-fatigue effects between placebo and ketamine was at day 2 (d = 0.58, p < 0.05). | One participant in ketamine and one participant in control group developed mania. | Small sample size. Normal saline could have masked proper blinding. Tapering of some of the current medications might have led to bias. |
| 10. | Abbar et al., 2022 | Randomized controlled trial | 26 participants with bipolar disorder (Gender distribution not reported). | 0.5 mg/kg infused in normal saline. | 0.9% Normal saline. | Patients continued their as usual medication. | To study the anti-suicidal effects of ketamine in a suicidal crisis. | Scale for Suicide Ideation (SSI) | 84.6% (n = 22; ketamine) vs. 28.0% (n = 7; placebo) reported resolution of suicidal symptoms (SSI < 4). The odds ratio for resolution of suicidal ideation was 14.1 (3.0 to 92.2, p < 0.001) in bipolar disorder patients at day 3 post treatment. | None reported | Small sample size. Normal saline could have masked proper blinding. Patients were allowed to take cannabis and other current medications. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jawad, M.Y.; Qasim, S.; Ni, M.; Guo, Z.; Di Vincenzo, J.D.; d’Andrea, G.; Tabassum, A.; Mckenzie, A.; Badulescu, S.; Grande, I.; et al. The Role of Ketamine in the Treatment of Bipolar Depression: A Scoping Review. Brain Sci. 2023, 13, 909. https://doi.org/10.3390/brainsci13060909
Jawad MY, Qasim S, Ni M, Guo Z, Di Vincenzo JD, d’Andrea G, Tabassum A, Mckenzie A, Badulescu S, Grande I, et al. The Role of Ketamine in the Treatment of Bipolar Depression: A Scoping Review. Brain Sciences. 2023; 13(6):909. https://doi.org/10.3390/brainsci13060909
Chicago/Turabian StyleJawad, Muhammad Youshay, Saleha Qasim, Menglu Ni, Ziji Guo, Joshua D. Di Vincenzo, Giacomo d’Andrea, Aniqa Tabassum, Andrea Mckenzie, Sebastian Badulescu, Iria Grande, and et al. 2023. "The Role of Ketamine in the Treatment of Bipolar Depression: A Scoping Review" Brain Sciences 13, no. 6: 909. https://doi.org/10.3390/brainsci13060909