
Effects of Combined Intervention of rTMS and Neurotransmitter Drugs on the Brain Functional Networks in Patients with Cognitive Impairment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Repetitive Transcranial Magnetic Stimulation Intervention
2.3. Neuropsychological Assessment
2.4. fMRI Acquisition
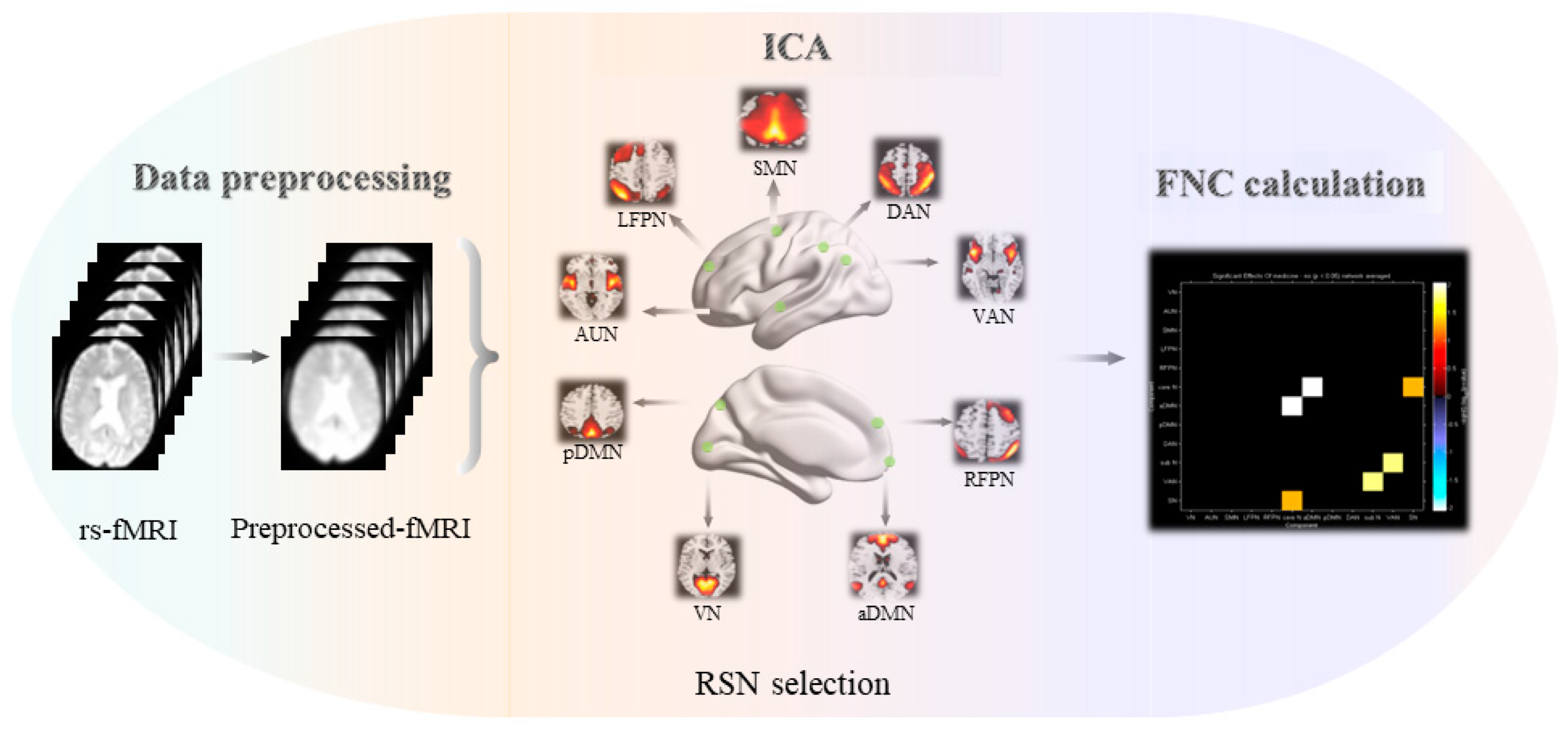
2.5. Data Preprocessing
2.6. Identification of Resting-State Networks
2.7. Inter-Network Connectivity Analysis
2.8. Intra-Network Connectivity Analysis
2.9. Statistical Analysis
3. Results
3.1. Demographic and Neuropsychological Data
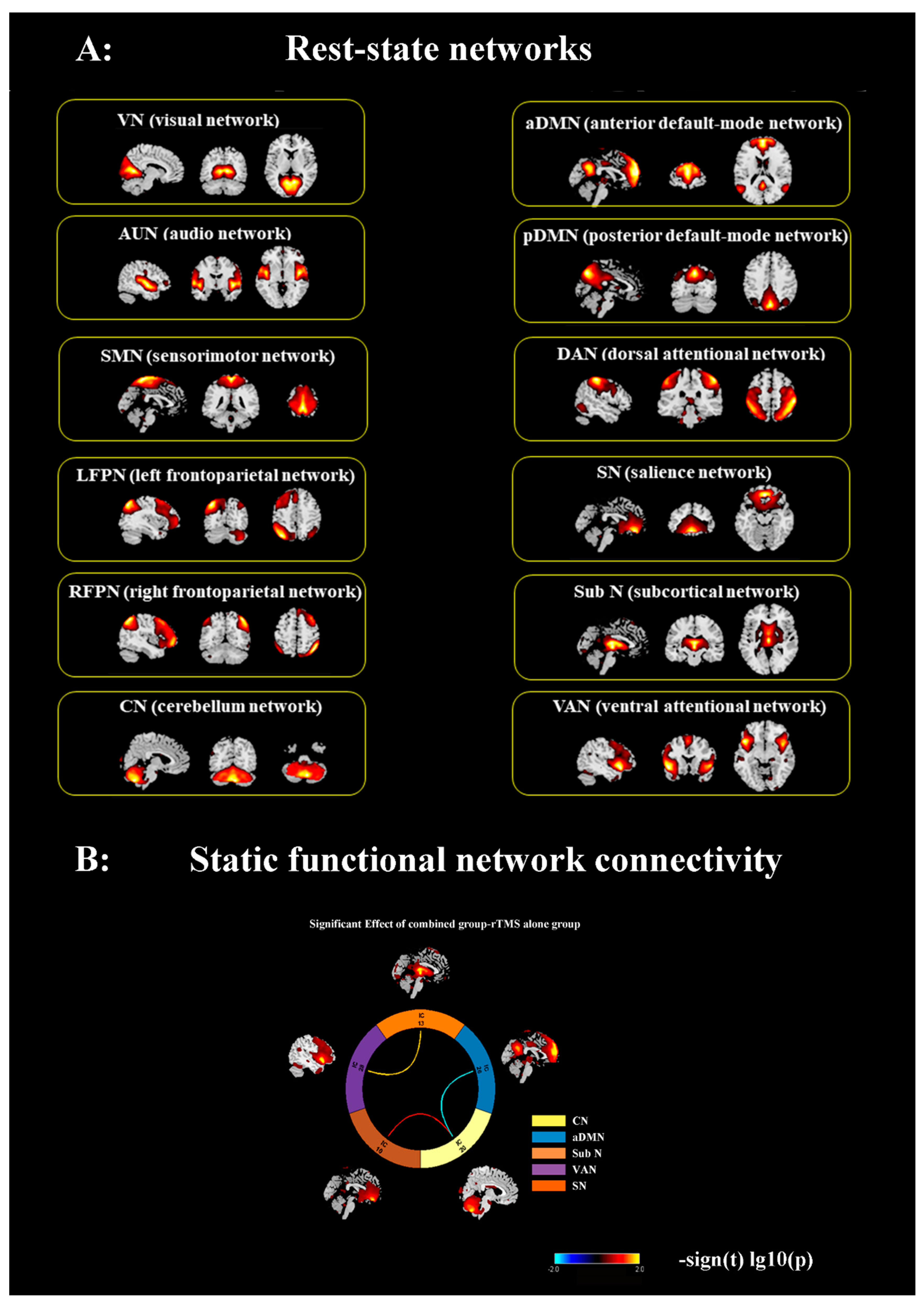
3.2. ICA and Determination of RSNs
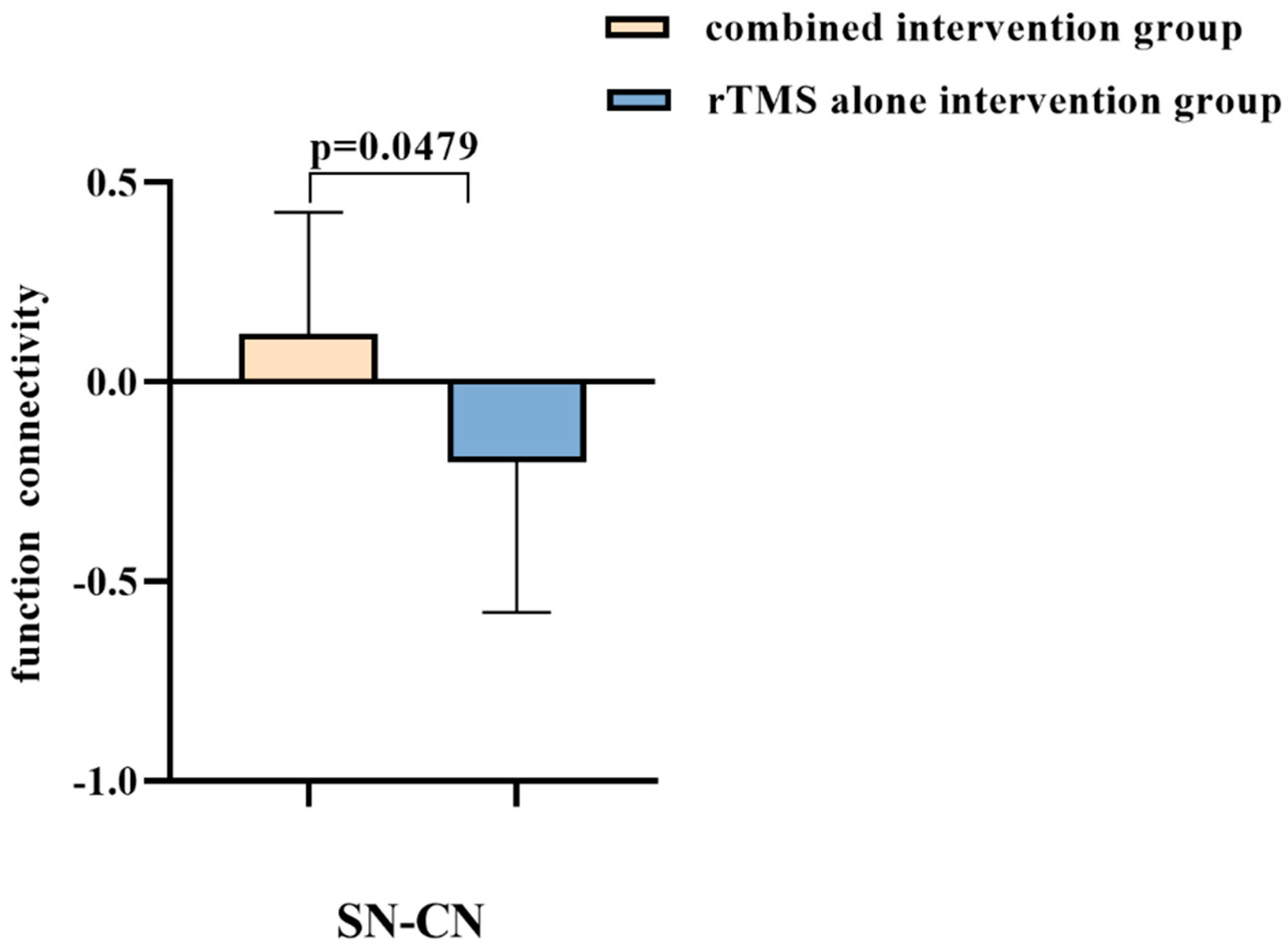
3.3. Combined Intervention Reconstruct Inter-Network Connectivity of Cerebellum
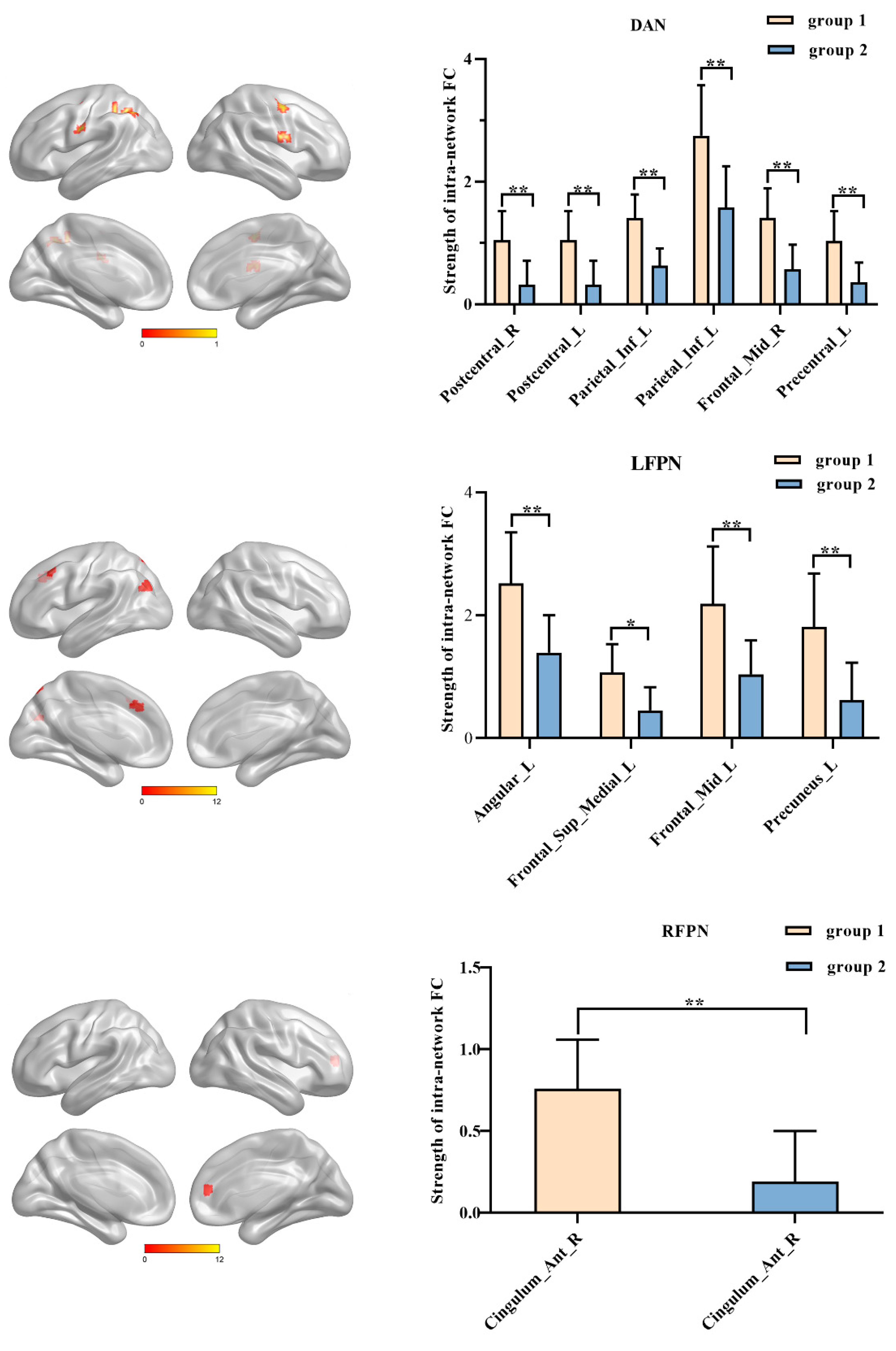
3.4. Combined Intervention Improves the Strength of Intra-Network Connectivity within Frontal-Parietal Regions
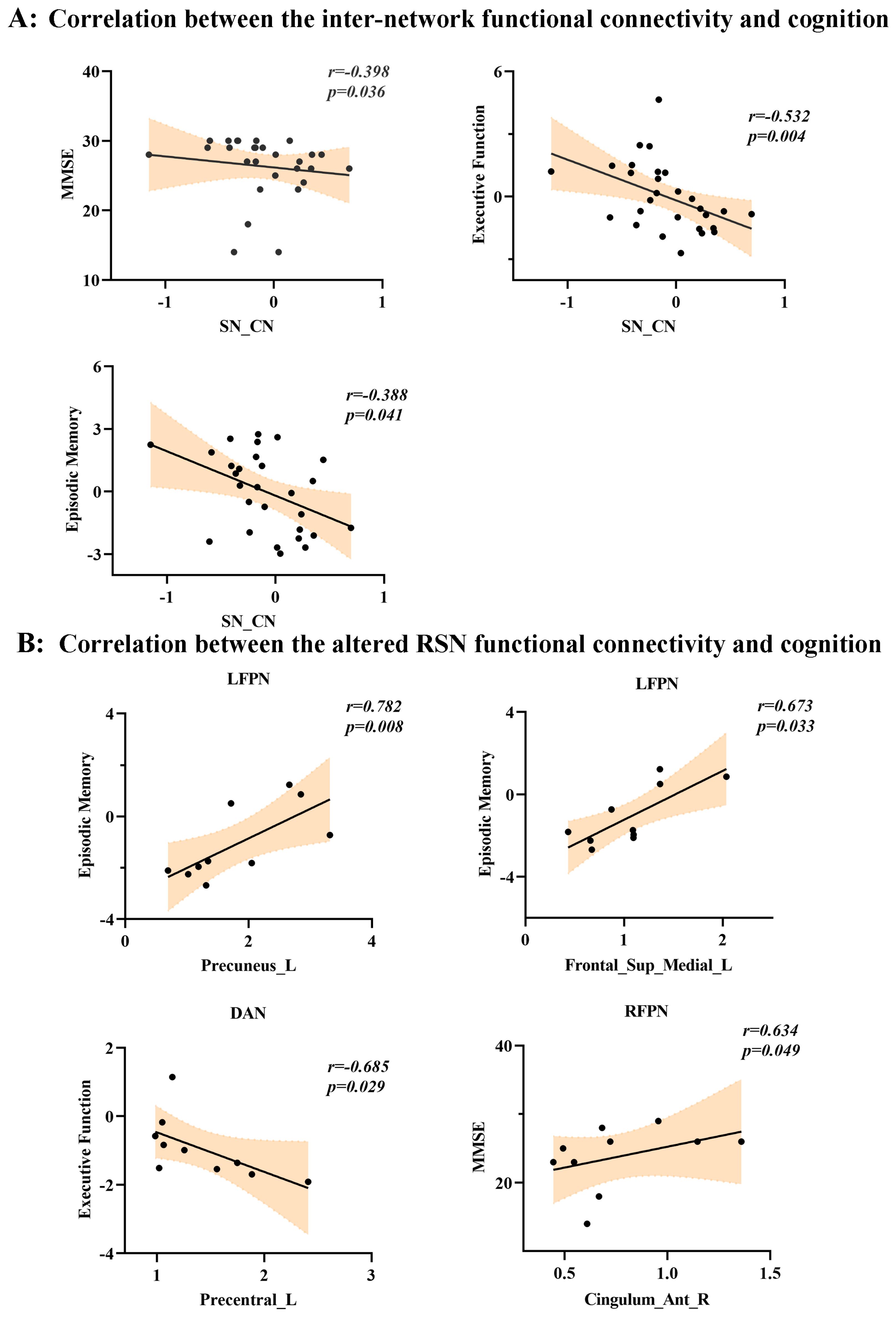
3.5. Differential Inter-Network/Intra-Network Connectivity Patterns and Behavioral Significance
4. Discussion
4.1. Neurotransmitter Drugs Combined with rTMS Intervention Can Reconstruct Functional Connectivity Associated with Cerebellum
4.2. Neurotransmitter Drugs Combined with rTMS Intervention Can Enhance Functional Connectivity within Frontal-Parietal Regions
4.3. Limitations and Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hebert, L.E.; Scherr, P.A.; Beckett, L.A.; Albert, M.S.; Pilgrim, D.M.; Chown, M.J.; Funkenstein, H.H.; Evans, D.A. Age-specific incidence of Alzheimer’s disease in a community population. JAMA 1995, 273, 1354–1359. [Google Scholar] [CrossRef]
- Zhao, Z.; Wu, J.; Fan, M.; Yin, D.; Tang, C.; Gong, J.; Xu, G.; Gao, X.; Yu, Q.; Yang, H.; et al. Altered intra- and inter-network functional coupling of resting-state networks associated with motor dysfunction in stroke. Hum. Brain Mapp. 2018, 39, 3388–3397. [Google Scholar] [CrossRef]
- Yang, Z.; Sheng, X.; Qin, R.; Chen, H.; Shao, P.; Xu, H.; Yao, W.; Zhao, H.; Xu, Y.; Bai, F.; et al. Cognitive Improvement via Left Angular Gyrus-Navigated Repetitive Transcranial Magnetic Stimulation Inducing the Neuroplasticity of Thalamic System in Amnesic Mild Cognitive Impairment Patients. J. Alzheimers Dis. JAD 2022, 86, 537–551. [Google Scholar] [CrossRef]
- Muir, J.L. Acetylcholine, aging, and Alzheimer’s disease. Pharmacol. Biochem. Behav. 1997, 56, 687–696. [Google Scholar] [CrossRef]
- Conway, M.E. Alzheimer’s disease: Targeting the glutamatergic system. Biogerontology 2020, 21, 257–274. [Google Scholar] [CrossRef] [Green Version]
- Petrella, J.R.; Prince, S.E.; Krishnan, S.; Husn, H.; Kelley, L.; Doraiswamy, P.M. Effects of donepezil on cortical activation in mild cognitive impairment: A pilot double-blind placebo-controlled trial using functional MR imaging. AJNR Am. J. Neuroradiol. 2009, 30, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Risacher, S.L.; Wang, Y.; Wishart, H.A.; Rabin, L.A.; Flashman, L.A.; McDonald, B.C.; West, J.D.; Santulli, R.B.; Saykin, A.J. Cholinergic Enhancement of Brain Activation in Mild Cognitive Impairment during Episodic Memory Encoding. Front. Psychiatry 2013, 4, 105. [Google Scholar] [CrossRef] [Green Version]
- Lorenzi, M.; Beltramello, A.; Mercuri, N.B.; Canu, E.; Zoccatelli, G.; Pizzini, F.B.; Alessandrini, F.; Cotelli, M.; Rosini, S.; Costardi, D.; et al. Effect of memantine on resting state default mode network activity in Alzheimer’s disease. Drugs Aging 2011, 28, 205–217. [Google Scholar] [CrossRef]
- Zhao, J.; Li, Z.; Cong, Y.; Zhang, J.; Tan, M.; Zhang, H.; Geng, N.; Li, M.; Yu, W.; Shan, P.; et al. Repetitive transcranial magnetic stimulation improves cognitive function of Alzheimer’s disease patients. Oncotarget 2017, 8, 33864–33871. [Google Scholar] [CrossRef] [Green Version]
- Bauer, P.R.; Kalitzin, S.; Zijlmans, M.; Sander, J.W.; Visser, G.H. Cortical excitability as a potential clinical marker of epilepsy: A review of the clinical application of transcranial magnetic stimulation. Int. J. Neural Syst. 2014, 24, 1430001. [Google Scholar] [CrossRef]
- Chen, J.; Ma, N.; Hu, G.; Nousayhah, A.; Xue, C.; Qi, W.; Xu, W.; Chen, S.; Rao, J.; Liu, W.; et al. rTMS modulates precuneus-hippocampal subregion circuit in patients with subjective cognitive decline. Aging 2020, 13, 1314–1331. [Google Scholar] [CrossRef] [PubMed]
- Freedberg, M.; Reeves, J.A.; Toader, A.C.; Hermiller, M.S.; Voss, J.L.; Wassermann, E.M. Persistent Enhancement of Hippocampal Network Connectivity by Parietal rTMS Is Reproducible. eNeuro 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.X.; Rogers, L.M.; Gross, E.Z.; Ryals, A.J.; Dokucu, M.E.; Brandstatt, K.L.; Hermiller, M.S.; Voss, J.L. Targeted enhancement of cortical-hippocampal brain networks and associative memory. Science 2014, 345, 1054–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckmann, C.F.; DeLuca, M.; Devlin, J.T.; Smith, S.M. Investigations into resting-state connectivity using independent component analysis. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2005, 360, 1001–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, L.; Hu, X.; Zhu, Y.; Yuan, Y.; Liu, W.; Chen, H. Aberrant Intra- and Internetwork Functional Connectivity in Depressed Parkinson’s Disease. Sci. Rep. 2017, 7, 2568. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. J. Alzheimers Assoc. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; Zhao, Q.; Guo, Q.; Meng, H.; Wang, B.; Luo, J.; Mortimer, J.A.; Borenstein, A.R.; Hong, Z. Prevalence of mild cognitive impairment in an urban community in China: A cross-sectional analysis of the Shanghai Aging Study. Alzheimers Dement. J. Alzheimers Assoc. 2015, 11, 300–309.e2. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B.; et al. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Zhao, Z.; Lu, J.; Jia, X.; Chao, W.; Han, Y.; Jia, J.; Li, K. Selective changes of resting-state brain oscillations in aMCI: An fMRI study using ALFF. BioMed Res. Int. 2014, 2014, 920902. [Google Scholar] [CrossRef] [Green Version]
- Guo, Q.; Zhao, Q.; Chen, M.; Ding, D.; Hong, Z. A comparison study of mild cognitive impairment with 3 memory tests among Chinese individuals. Alzheimer Dis. Assoc. Disord. 2009, 23, 253–259. [Google Scholar] [CrossRef]
- Chao-Gan, Y.; Yu-Feng, Z. DPARSF: A MATLAB Toolbox for “Pipeline” Data Analysis of Resting-State fMRI. Front. Syst. Neurosci. 2010, 4, 13. [Google Scholar]
- Ashburner, J.; Friston, K.J. Unified segmentation. NeuroImage 2005, 26, 839–851. [Google Scholar] [CrossRef]
- Song, J.; Qin, W.; Liu, Y.; Duan, Y.; Liu, J.; He, X.; Li, K.; Zhang, X.; Jiang, T.; Yu, C.; et al. Aberrant functional organization within and between resting-state networks in AD. PLoS ONE 2013, 8, e63727. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wang, F.; Liu, X.; Cao, D.; Cai, L.; Jiang, X.; Yang, X.; Yang, T.; Asakawa, T. Changes in Brain Function Networks in Patients With Amnestic Mild Cognitive Impairment: A Resting-State fMRI Study. Front. Neurol. 2020, 11, 554032. [Google Scholar] [CrossRef]
- Zhao, Z.; Huang, T.; Tang, C.; Ni, K.; Pan, X.; Yan, C.; Fan, X.; Xu, D.; Luo, Y. Altered resting-state intra- and inter- network functional connectivity in patients with persistent somatoform pain disorder. PLoS ONE 2017, 12, e0176494. [Google Scholar] [CrossRef] [Green Version]
- Liao, H.; Cai, S.; Shen, Q.; Fan, J.; Wang, T.; Zi, Y.; Mao, Z.; Situ, W.; Liu, J.; Zou, T.; et al. Networks Are Associated With Depression in Patients With Parkinson’s Disease: A Resting-State Imaging Study. Front. Neurosci. 2020, 14, 573538. [Google Scholar] [CrossRef]
- Houck, J.M.; Çetin, M.S.; Mayer, A.R.; Bustillo, J.R.; Stephen, J.; Aine, C.; Cañive, J.; Perrone-Bizzozero, N.; Thoma, R.J.; Brookes, M.J.; et al. Magnetoencephalographic and functional MRI connectomics in schizophrenia via intra- and inter-network connectivity. NeuroImage 2017, 145, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Lu, L.; Shang, S.; Hu, L.; Chen, H.; Wang, P.; Zhang, H.; Chen, Y.C.; Yin, X. Disrupted functional network connectivity predicts cognitive impairment after acute mild traumatic brain injury. CNS Neurosci. Ther. 2020, 26, 1083–1091. [Google Scholar] [CrossRef]
- Wang, S.; Chen, B.; Yu, Y.; Yang, H.; Cui, W.; Fan, G.; Li, J. Altered resting-state functional network connectivity in profound sensorineural hearing loss infants within an early sensitive period: A group ICA study. Hum. Brain Mapp. 2021, 42, 4314–4326. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Zhang, D.; Qi, F.; Gao, J.; Tang, M.; Ai, K.; Yan, X.; Lei, X.; Shao, Z.; Su, Y.; et al. Dysfunctional Interaction Between the Dorsal Attention Network and the Default Mode Network in Patients With Type 2 Diabetes Mellitus. Front. Hum. Neurosci. 2021, 15, 796386. [Google Scholar] [CrossRef] [PubMed]
- Zuo, X.N.; Kelly, C.; Adelstein, J.S.; Klein, D.F.; Castellanos, F.X.; Milham, M.P. Reliable intrinsic connectivity networks: Test-retest evaluation using ICA and dual regression approach. NeuroImage 2010, 49, 2163–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Qin, W.; Liu, Y.; Zhang, Y.; Jiang, T.; Yu, C. Altered resting-state network connectivity in congenital blind. Hum. Brain Mapp. 2014, 35, 2573–2581. [Google Scholar] [CrossRef]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. Off. J. Soc. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Wu, C.; Matias, C.; Foltynie, T.; Limousin, P.; Zrinzo, L.; Akram, H. Dynamic Network Connectivity Reveals Markers of Response to Deep Brain Stimulation in Parkinson’s Disease. Front. Hum. Neurosci. 2021, 15, 729677. [Google Scholar] [CrossRef]
- Beckmann, C.F.; Smith, S.M. Probabilistic independent component analysis for functional magnetic resonance imaging. IEEE Trans. Med. Imaging 2004, 23, 137–152. [Google Scholar] [CrossRef]
- Habas, C. Functional Connectivity of the Cognitive Cerebellum. Front. Syst. Neurosci. 2021, 8, 15. [Google Scholar] [CrossRef]
- Hardwick, R.M.; Therrien, A.S.; Lesage, E. Non-invasive stimulation of the motor cerebellum has potential cognitive confounds. Brain Stimul. 2021, 14, 922–923. [Google Scholar] [CrossRef]
- Ferrari, C.; Cattaneo, Z.; Oldrati, V.; Casiraghi, L.; Castelli, F.; D’Angelo, E.; Vecchi, T. TMS Over the Cerebellum Interferes with Short-term Memory of Visual Sequences. Sci. Rep. 2018, 8, 6722. [Google Scholar] [CrossRef] [Green Version]
- Zheng, W.; Liu, X.; Song, H.; Li, K.; Wang, Z. Altered Functional Connectivity of Cognitive-Related Cerebellar Subregions in Alzheimer’s Disease. Front. Aging Neurosci. 2017, 9, 143. [Google Scholar] [CrossRef] [Green Version]
- Gatti, D.; Van Vugt, F.; Vecchi, T. A causal role for the cerebellum in semantic integration: A transcranial magnetic stimulation study. Sci. Rep. 2020, 10, 18139. [Google Scholar] [CrossRef]
- Bernard, J.A.; Seidler, R.D. Moving forward: Age effects on the cerebellum underlie cognitive and motor declines. Neurosci. Biobehav. Rev. 2014, 42, 193–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmahmann, J.D. The cerebellum and cognition. Neurosci. Lett. 2019, 688, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Balsters, J.H.; Whelan, C.D.; Robertson, I.H.; Ramnani, N. Cerebellum and cognition: Evidence for the encoding of higher order rules. Cereb. Cortex 2013, 23, 1433–1443. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.; Hu, J.; Ma, W.; Wang, D.; Yao, Q.; Shi, J. Altered baseline activity and connectivity associated with cognitive impairment following acute cerebellar infarction: A resting-state fMRI study. Neurosci. Lett. 2019, 692, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Zhu, D.; Ma, W.; Yao, Q.; Li, Q.; Shi, J. Differences Changes in Cerebellar Functional Connectivity Between Mild Cognitive Impairment and Alzheimer’s Disease: A Seed-Based Approach. Front. Neurol. 2021, 12, 645171. [Google Scholar] [CrossRef]
- Grimaldi, G.; Argyropoulos, G.P.; Boehringer, A.; Celnik, P.; Edwards, M.J.; Ferrucci, R.; Galea, J.M.; Groiss, S.J.; Hiraoka, K.; Kassavetis, P.; et al. Non-invasive cerebellar stimulation—A consensus paper. Cerebellum 2014, 13, 121–138. [Google Scholar] [CrossRef]
- Farzan, F.; Pascual-Leone, A.; Schmahmann, J.D.; Halko, M. Enhancing the Temporal Complexity of Distributed Brain Networks with Patterned Cerebellar Stimulation. Sci. Rep. 2016, 6, 23599. [Google Scholar] [CrossRef] [Green Version]
- Esterman, M.; Thai, M.; Okabe, H.; DeGutis, J.; Saad, E.; Laganiere, S.E.; Halko, M.A. Network-targeted cerebellar transcranial magnetic stimulation improves attentional control. NeuroImage 2017, 156, 190–198. [Google Scholar] [CrossRef]
- Daskalakis, Z.J.; Paradiso, G.O.; Christensen, B.K.; Fitzgerald, P.B.; Gunraj, C.; Chen, R. Exploring the connectivity between the cerebellum and motor cortex in humans. J. Physiol. 2004, 557, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Gatti, D.; Rinaldi, L.; Cristea, I.; Vecchi, T. Probing cerebellar involvement in cognition through a meta-analysis of TMS evidence. Sci. Rep. 2021, 11, 14777. [Google Scholar] [CrossRef] [PubMed]
- Thakral, P.P.; Madore, K.P.; Schacter, D.L. A Role for the Left Angular Gyrus in Episodic Simulation and Memory. J. Neurosci. Off. J. Soc. Neurosci. 2017, 37, 8142–8149. [Google Scholar] [CrossRef] [PubMed]
- Seghier, M.L. The angular gyrus: Multiple functions and multiple subdivisions. Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2013, 19, 43–61. [Google Scholar] [CrossRef] [Green Version]
- Binder, J.R.; Desai, R.H. The neurobiology of semantic memory. Trends Cogn. Sci. 2011, 15, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; Kahn, I.; Snyder, A.Z.; Raichle, M.E.; Buckner, R.L. Evidence for a frontoparietal control system revealed by intrinsic functional connectivity. J. Neurophysiol. 2008, 100, 3328–3342. [Google Scholar] [CrossRef] [Green Version]
- Gilmore, A.W.; Nelson, S.M.; McDermott, K.B. A parietal memory network revealed by multiple MRI methods. Trends Cogn. Sci. 2015, 19, 534–543. [Google Scholar] [CrossRef]
- Daselaar, S.M.; Porat, Y.; Huijbers, W.; Pennartz, C.M. Modality-specific and modality-independent components of the human imagery system. NeuroImage 2010, 52, 677–685. [Google Scholar] [CrossRef]
- Gilboa, A.; Winocur, G.; Grady, C.L.; Hevenor, S.J.; Moscovitch, M. Remembering our past: Functional neuroanatomy of recollection of recent and very remote personal events. Cereb. Cortex 2004, 14, 1214–1225. [Google Scholar] [CrossRef] [Green Version]
- Addis, D.R.; Moscovitch, M.; Crawley, A.P.; McAndrews, M.P. Recollective qualities modulate hippocampal activation during autobiographical memory retrieval. Hippocampus 2004, 14, 752–762. [Google Scholar] [CrossRef]
- Legostaeva, L.; Poydasheva, A.; Iazeva, E.; Sinitsyn, D.; Sergeev, D.; Bakulin, I.; Lagoda, D.; Kremneva, E.; Morozova, S.; Ryabinkina, Y.; et al. Stimulation of the Angular Gyrus Improves the Level of Consciousness. Brain Sci. 2019, 9, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilakantan, A.S.; Bridge, D.J.; Gagnon, E.P.; VanHaerents, S.A.; Voss, J.L. Stimulation of the Posterior Cortical-Hippocampal Network Enhances Precision of Memory Recollection. Curr. Biol. CB 2017, 27, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Cocchi, L.; Halford, G.S.; Zalesky, A.; Harding, I.H.; Ramm, B.J.; Cutmore, T.; Shum, D.H.; Mattingley, J.B. Complexity in relational processing predicts changes in functional brain network dynamics. Cereb. Cortex 2014, 24, 2283–2296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, M.W.; Reynolds, J.R.; Power, J.D.; Repovs, G.; Anticevic, A.; Braver, T.S. Multi-task connectivity reveals flexible hubs for adaptive task control. Nat. Neurosci. 2013, 16, 1348–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornito, A.; Harrison, B.J.; Zalesky, A.; Simons, J.S. Competitive and cooperative dynamics of large-scale brain functional networks supporting recollection. Proc. Natl. Acad. Sci. USA 2012, 109, 12788–12793. [Google Scholar] [CrossRef] [Green Version]
- Hearne, L.J.; Cocchi, L.; Zalesky, A.; Mattingley, J.B. Reconfiguration of Brain Network Architectures between Resting-State and Complexity-Dependent Cognitive Reasoning. J. Neurosci. Off. J. Soc. Neurosci. 2017, 37, 8399–8411. [Google Scholar] [CrossRef] [Green Version]
- Koch, G.; Bonnì, S.; Pellicciari, M.C.; Casula, E.P.; Mancini, M.; Esposito, R.; Ponzo, V.; Picazio, S.; Di Lorenzo., F.; Serra, L.; et al. Transcranial magnetic stimulation of the precuneus enhances memory and neural activity in prodromal Alzheimer’s disease. NeuroImage 2018, 169, 302–311. [Google Scholar] [CrossRef] [Green Version]
- Brissenden, J.A.; Levin, E.J.; Osher, D.E.; Halko, M.A.; Somers, D.C. Functional Evidence for a Cerebellar Node of the Dorsal Attention Network. J. Neurosci. Off. J. Soc. Neurosci. 2016, 36, 6083–6096. [Google Scholar] [CrossRef] [Green Version]
- Reuter-Lorenz, P.A.; Cappell, K.A. Neurocognitive Aging and the Compensation Hypothesis. Curr. Dir. Psychol. Sci. 2008, 17, 177–182. [Google Scholar] [CrossRef]
- Goekoop, R.; Rombouts, S.A.; Jonker, C.; Hibbel, A.; Knol, D.L.; Truyen, L.; Barkhof, F.; Scheltens, P. Challenging the cholinergic system in mild cognitive impairment: A pharmacological fMRI study. NeuroImage 2004, 23, 1450–1459. [Google Scholar] [CrossRef]
- Solé-Padullés, C.; Bartrés-Faz, D.; Lladó, A.; Bosch, B.; Peña-Gómez, C.; Castellví, M.; Rami, L.; Bargalló, N.; Sánchez-Valle, R.; Molinuevo, J.L.; et al. Donepezil treatment stabilizes functional connectivity during resting state and brain activity during memory encoding in Alzheimer’s disease. J. Clin. Psychopharmacol. 2013, 33, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Goveas, J.S.; Xie, C.; Ward, B.D.; Wu, Z.; Li, W.; Franczak, M.; Jones, J.L.; Antuono, P.G.; Li, S.J. Recovery of hippocampal network connectivity correlates with cognitive improvement in mild Alzheimer’s disease patients treated with donepezil assessed by resting-state fMRI. J. Magn. Reson. Imaging JMRI 2011, 34, 764–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.; Yang, H.; Zhang, J. Donepezil’s Effects on Brain Functions of Patients With Alzheimer Disease: A Regional Homogeneity Study Based on Resting-State Functional Magnetic Resonance Imaging. Clin. Neuropharmacol. 2019, 42, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Saykin, A.J.; Wishart, H.A.; Rabin, L.A.; Flashman, L.A.; McHugh, T.L.; Mamourian, A.C.; Santulli, R.B. Cholinergic enhancement of frontal lobe activity in mild cognitive impairment. Brain J. Neurol. 2004, 127, 1574–1583. [Google Scholar] [CrossRef] [Green Version]
- Griffanti, L.; Wilcock, G.K.; Voets, N.; Bonifacio, G.; Mackay, C.E.; Jenkinson, M.; Zamboni, G. Donepezil Enhances Frontal Functional Connectivity in Alzheimer’s Disease: A Pilot Study. Dement. Geriatr. Cogn. Disord. Extra 2016, 6, 518–528. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Combined Intervention Group | rTMS-Alone Intervention Group | p Value |
|---|---|---|---|
| (n = 10) | (n = 18) | ||
| Demographics | |||
| Age (years) means ± SD | 68.40 ± 4.95 | 65.78 ± 8.30 | 0.371 |
| Education (years) IQR | 9.00 (12.75−9.00) | 12.00 (15.00−9.00) | 0.146 |
| Gender (male/female) | 4/6 | 7/11 | 0.954 |
| General cognition | |||
| MMSE | 25.50 (26.50−21.75) | 29.00 (30.00−27.00) | 0.002 * |
| MoCA | 21.00 (26.25−18.75) | 24.50 (26.00−22.50) | 0.332 |
| Composition Z scores of each cognitive domain | |||
| Episodic Memory | −1.07 ± 1.43 | 0.59 ± 3.512 | 0.022 * |
| AVLT-DR | 3.80 ± 2.49 | 6.06 ± 3.73 | 0.100 |
| VR-DR (WMS) | −0.91 (0.124−(−1.46)) | 0.73 (1.16−0.02) | 0.010 * |
| Information Processing Speed | −1.34 (−0.28−(−2.61)) | 1.06 (2.26−(−1.76)) | 0.077 |
| TMT-A (inverse) | −0.44 (−0.98−(−0.19)) | 0.07 (0.88−(−0.51)) | 0.010 * |
| Stroop A (inverse) | −0.33 ± 0.79 | 0.18 ± 1.08 | 0.201 |
| Stroop B (inverse) | −0.42(−0.24−(−0.72)) | 0.33 (0.72−(−0.48)) | 0.035 * |
| Language | −0.46(0.67−(−1.20)) | 0.57 (1.35−(−1.32)) | 0.408 |
| CVF | −0.31 ± 0.76 | 0.17 ± 1.09 | 0.224 |
| BNT | 0.33(0.55−(−0.11)) | 0.24 (0.52(−0.30)) | 0.689 |
| Visuospatial Processing Function | 0.39(0.93−(−0.97)) | 0.93 (0.93−(−0.16)) | 0.460 |
| CDT | 0.62(0.62−(−0.74)) | 0.62 (0.62−(−0.74)) | 0.906 |
| VR-C | 0.31(0.31−0.20) | 0.31(0.31−0.31) | 0.724 |
| Executive Function | −1.17 (−0.48−(−1.52)) | 0.55 (1.49−(−0.75)) | 0.014 * |
| TMT-B (inverse) | −0.44 (−0.59−(−0.31)) | −0.18 (0.51−(−0.56)) | 0.270 |
| Stroop C (inverse) | −0.77 (0.075−(−1.20)) | 0.44 (0.96−(−0.31)) | 0.004 * |
| Inter-Network FC | t-Value | p-Value |
|---|---|---|
| aDMN-CN | −2.81 | 0.009 |
| SN-CN | 2.07 | 0.0479 |
| sub N-VAN | 2.57 | 0.0158 |
| Brain Regions | Cluster Size | Peak Intensity | Peak MNI Coordinate | |
|---|---|---|---|---|
| (mm3) | x,y,z (mm) | |||
| LFPN | ||||
| Angular_L | 459 | 4.0923 | −45 −75 30 | |
| Frontal_Sup_Medial_L | 540 | 3.5118 | −9 33 36 | |
| Frontal_Mid_L | 459 | 3.9411 | −39 24 45 | |
| Precuneus_L | 270 | 4.3838 | −12 −72 57 | |
| aDMN | ||||
| Frontal_Sup_Medial_L | 378 | 3.8797 | −3 57 21 | |
| Frontal_Mid_L | 648 | 4.0521 | −27 33 30 | |
| Frontal_Sup_Medial_R | 432 | 4.2036 | 12 45 45 | |
| Precentral_L | 432 | 4.1363 | −39 −9 57 | |
| CN | ||||
| Fusiform_L | 378 | 3.8623 | −33 −48 −21 | |
| DAN | ||||
| Postcentral_R | 405 | 3.5456 | 63 3 21 | |
| Postcentral_L | 324 | 4.3801 | −57 −6 30 | |
| Parietal_Inf_L | 891 | 4.5272 | −39 −57 42 | |
| Parietal_Inf_L | 540 | 4.4364 | −45 −45 51 | |
| Frontal_Mid_R | 1026 | 4.754 | 39 −6 51 | |
| Precentral_L | 270 | 4.6901 | −36 −12 51 | |
| pDMN | ||||
| Caudate_L | 351 | 4.3674 | −9 −3 3 | |
| Precuneus_L | 378 | 4.6397 | −6 −51 48 | |
| Precuneus_R | 351 | 3.3809 | 12 −51 51 | |
| RFPN | ||||
| Cingulum_Ant_R | 432 | 4.9952 | 12 48 12 | |
| SMN | ||||
| Cingulum_Mid_R | 621 | 3.6626 | 9 −36 45 | |
| Precuneus_L | 270 | 3.6859 | −15 −45 51 | |
| Postcentral_L | 1647 | 4.9895 | −21 −30 63 | |
| Precuneus_R | 945 | 4.4568 | 9 −63 60 | |
| VAN | ||||
| Frontal_Inf_Orb_L | 378 | 4.5632 | −27 15 −18 | |
| Putamen_L | 405 | 4.6378 | −12 6 −3 | |
| Insula_R | 270 | 3.9312 | 42 0 0 | |
| Frontal_Mid_L | 297 | 3.92 | −48 27 39 | |
| Supp_Motor_Area_L | 540 | 4.2135 | −3 3 48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Qin, Z.; Chen, H.; Yang, Z.; Wang, L.; Qin, R.; Zhao, H.; Bai, F. Effects of Combined Intervention of rTMS and Neurotransmitter Drugs on the Brain Functional Networks in Patients with Cognitive Impairment. Brain Sci. 2023, 13, 419. https://doi.org/10.3390/brainsci13030419
Li M, Qin Z, Chen H, Yang Z, Wang L, Qin R, Zhao H, Bai F. Effects of Combined Intervention of rTMS and Neurotransmitter Drugs on the Brain Functional Networks in Patients with Cognitive Impairment. Brain Sciences. 2023; 13(3):419. https://doi.org/10.3390/brainsci13030419
Chicago/Turabian StyleLi, Mengyun, Zhiming Qin, Haifeng Chen, Zhiyuan Yang, Lianlian Wang, Ruomeng Qin, Hui Zhao, and Feng Bai. 2023. "Effects of Combined Intervention of rTMS and Neurotransmitter Drugs on the Brain Functional Networks in Patients with Cognitive Impairment" Brain Sciences 13, no. 3: 419. https://doi.org/10.3390/brainsci13030419