
Win and Loss Responses in the Monetary Incentive Delay Task Mediate the Link between Depression and Problem Drinking
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Subjects
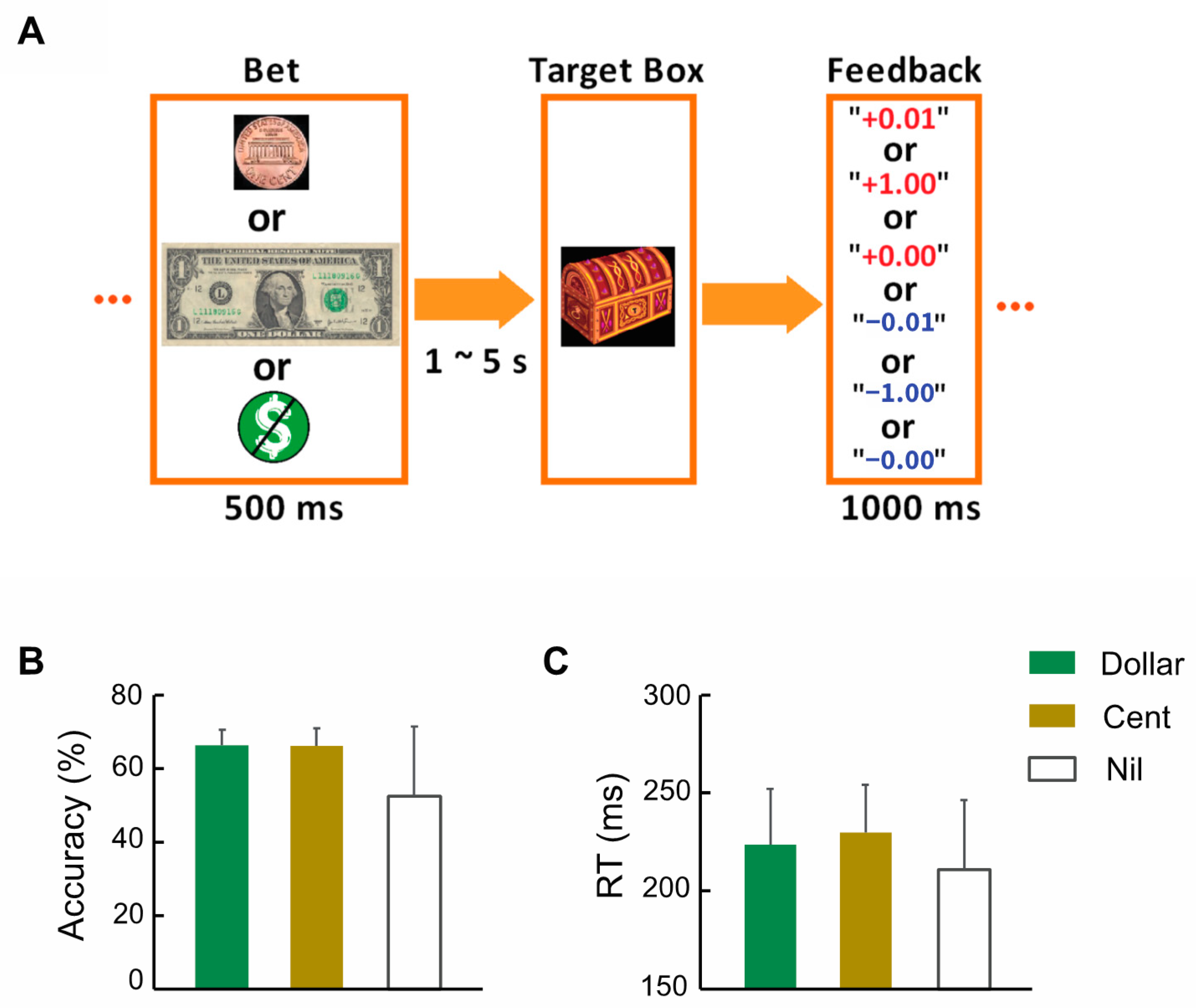
2.2. Assessments, Monetary Incentive Delay Task (MIDT), and Imaging Protocol
2.3. Imaging Data Preprocessing and Group Analyses
2.4. Mediation Analyses
3. Results
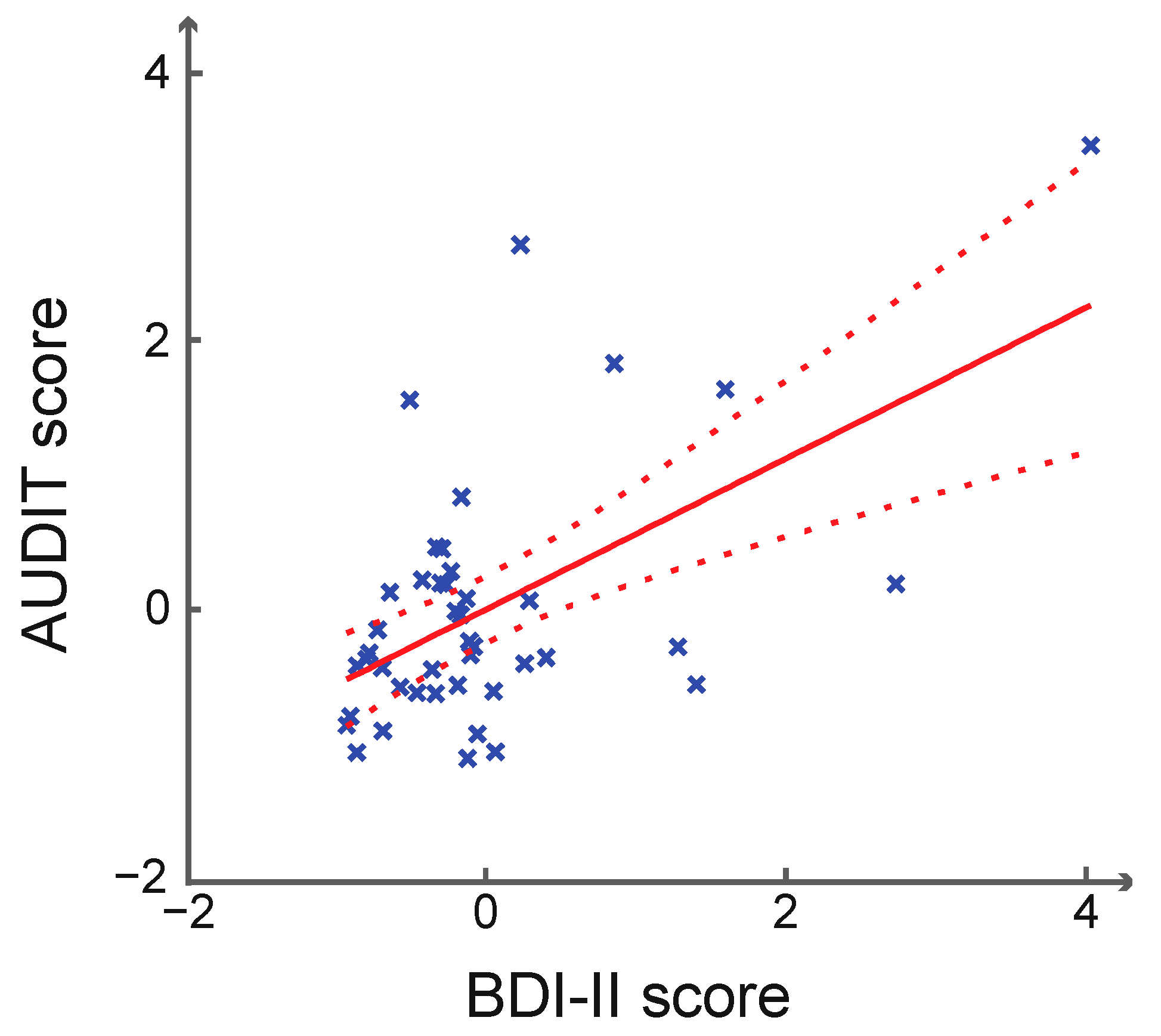
3.1. Clinical Characteristics and Behavioral Performance
3.2. Brain Activations of Win vs. Nil and Loss vs. Nil
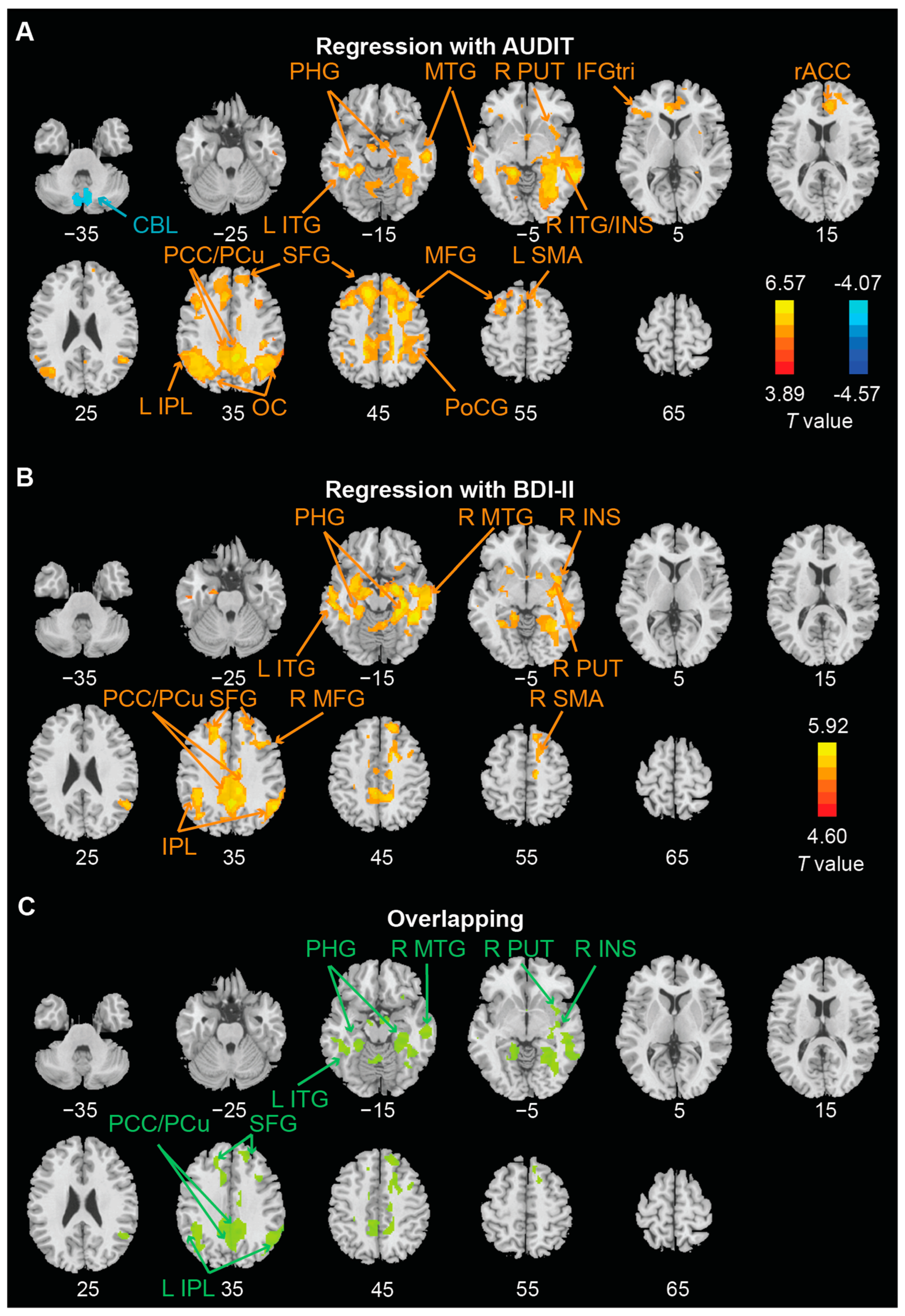
3.3. Whole Brain Regressions on AUDIT and BDI-II Scores
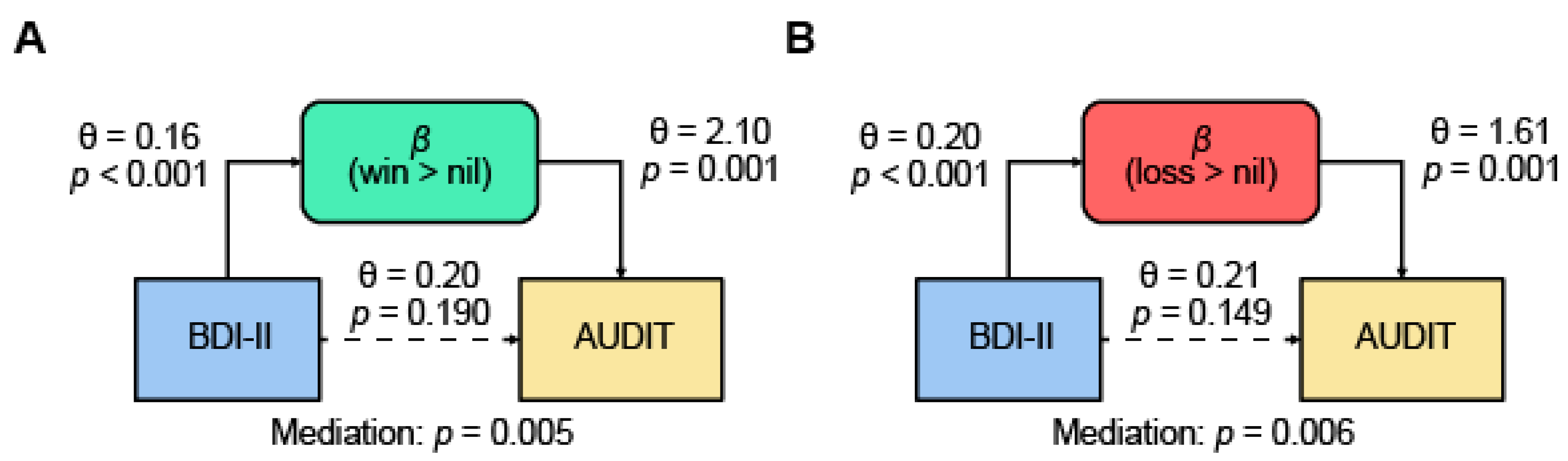
3.4. Mediation Models
4. Discussion
4.1. Depression and Alcohol Misuse Shared Neural Responses to Monetary Win and Loss
4.2. Shared Neural Responses Mediated the Link of Depression and Alcohol Misuse
4.3. Limitations of the Study and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boden, J.M.; Fergusson, D.M. Alcohol and depression. Addiction 2011, 106, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Whiteford, H.A.; Ferrari, A.J.; Degenhardt, L.; Feigin, V.; Vos, T. The global burden of mental, neurological and substance use disorders: An analysis from the Global Burden of Disease Study 2010. PLoS ONE 2015, 10, e0116820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Carniglia, A.; Keyes, K.M.; Hasin, D.S.; Cerdá, M. Psychiatric comorbidities in alcohol use disorder. Lancet Psychiatry 2019, 6, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Grant, B.F.; Harford, T.C. Comorbidity between DSM-IV alcohol use disorders and major depression: Results of a national survey. Drug Alcohol Depend. 1995, 39, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Swendsen, J.D.; Merikangas, K.R. The comorbidity of depression and substance use disorders. Clin. Psychol. Rev. 2000, 20, 173–189. [Google Scholar] [CrossRef]
- Tilki, M. The social contexts of drinking among Irish men in London. Drugs Educ. Prev. Policy 2006, 13, 247–261. [Google Scholar] [CrossRef]
- Caldwell, T.M.; Rodgers, B.; Jorm, A.F.; Christensen, H.; Jacomb, P.A.; Korten, A.E.; Lynskey, M.T. Patterns of association between alcohol consumption and symptoms of depression and anxiety in young adults. Addiction 2002, 97, 583–594. [Google Scholar] [CrossRef]
- Bell, S.; Britton, A.; Kubinova, R.; Malyutina, S.; Pajak, A.; Nikitin, Y.; Bobak, M. Drinking pattern, abstention and problem drinking as risk factors for depressive symptoms: Evidence from three urban Eastern European populations. PLoS ONE 2014, 9, e104384. [Google Scholar] [CrossRef] [Green Version]
- McHugh, R.K.; Weiss, R.D. Alcohol use disorder and depressive disorders. Alcohol Res. Curr. Rev. 2019, 40, arcr.v40.1.01. [Google Scholar] [CrossRef] [Green Version]
- Feldstein Ewing, S.W.; Filbey, F.M.; Chandler, L.D.; Hutchison, K.E. Exploring the relationship between depressive and anxiety symptoms and neuronal response to alcohol cues. Alcohol. Clin. Exp. Res. 2010, 34, 396–403. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Boden, J.M.; Horwood, L.J. Tests of causal links between alcohol abuse or dependence and major depression. Arch. Gen. Psychiatry 2009, 66, 260–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldham, S.; Murawski, C.; Fornito, A.; Youssef, G.; Yucel, M.; Lorenzetti, V. The anticipation and outcome phases of reward and loss processing: A neuroimaging meta-analysis of the monetary incentive delay task. Hum. Brain Mapp. 2018, 39, 3398–3418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Chaudhary, S.; Chiang-shan, R.L. Shared and distinct neural activity during anticipation and outcome of win and loss: A meta-analysis of the monetary incentive delay task. Neuroimage 2022, 264, 119764. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.H.; Alloy, L.B.; Smith, D.V. Meta-analysis of reward processing in major depressive disorder reveals distinct abnormalities within the reward circuit. Transl. Psychiatry 2019, 9, 293. [Google Scholar] [CrossRef] [Green Version]
- Eshel, N.; Roiser, J.P. Reward and punishment processing in depression. Biol. Psychiatry 2010, 68, 118–124. [Google Scholar] [CrossRef]
- Admon, R.; Pizzagalli, D.A. Dysfunctional Reward Processing in Depression. Curr. Opin. Psychol. 2015, 4, 114–118. [Google Scholar] [CrossRef] [Green Version]
- Pizzagalli, D.A.; Holmes, A.J.; Dillon, D.G.; Goetz, E.L.; Birk, J.L.; Bogdan, R.; Dougherty, D.D.; Iosifescu, D.V.; Rauch, S.L.; Fava, M. Reduced caudate and nucleus accumbens response to rewards in unmedicated individuals with major depressive disorder. Am. J. Psychiatry 2009, 166, 702–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Callaghan, G.; Stringaris, A. Reward processing in adolescent depression across neuroimaging modalities. Z. Kinder Jugendpsychiatrie Psychother. 2019, 47, 535–541. [Google Scholar] [CrossRef]
- Knutson, B.; Greer, S.M. Anticipatory affect: Neural correlates and consequences for choice. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2008, 363, 3771–3786. [Google Scholar] [CrossRef] [Green Version]
- Craske, M.G.; Meuret, A.E.; Ritz, T.; Treanor, M.; Dour, H.J. Treatment for anhedonia: A neuroscience driven approach. Depress. Anxiety 2016, 33, 927–938. [Google Scholar] [CrossRef]
- Stoy, M.; Schlagenhauf, F.; Sterzer, P.; Bermpohl, F.; Hägele, C.; Suchotzki, K.; Schmack, K.; Wrase, J.; Ricken, R.; Knutson, B. Hyporeactivity of ventral striatum towards incentive stimuli in unmedicated depressed patients normalizes after treatment with escitalopram. J. Psychopharmacol. 2012, 26, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Dichter, G.S.; Kozink, R.V.; McClernon, F.J.; Smoski, M.J. Remitted major depression is characterized by reward network hyperactivation during reward anticipation and hypoactivation during reward outcomes. J. Affect. Disord. 2012, 136, 1126–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotlib, I.H.; Sivers, H.; Gabrieli, J.D.; Whitfield-Gabrieli, S.; Goldin, P.; Minor, K.L.; Canli, T. Subgenual anterior cingulate activation to valenced emotional stimuli in major depression. Neuroreport 2005, 16, 1731–1734. [Google Scholar] [CrossRef]
- Smoski, M.J.; Felder, J.; Bizzell, J.; Green, S.R.; Ernst, M.; Lynch, T.R.; Dichter, G.S. fMRI of alterations in reward selection, anticipation, and feedback in major depressive disorder. J. Affect. Disord. 2009, 118, 69–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bremner, J.D.; Vythilingam, M.; Vermetten, E.; Charney, D.S. Effects of antidepressant treatment on neural correlates of emotional and neutral declarative verbal memory in depression. J. Affect. Disord. 2007, 101, 99–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, C.; Redlich, R.; Grotegerd, D.; Meinert, S.; Dohm, K.; Schneider, I.; Zaremba, D.; Forster, K.; Alferink, J.; Bolte, J.; et al. Differential Abnormal Pattern of Anterior Cingulate Gyrus Activation in Unipolar and Bipolar Depression: An fMRI and Pattern Classification Approach. Neuropsychopharmacology 2017, 42, 1399–1408. [Google Scholar] [CrossRef] [Green Version]
- Hall, G.B.; Milne, A.M.; Macqueen, G.M. An fMRI study of reward circuitry in patients with minimal or extensive history of major depression. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 187–198. [Google Scholar] [CrossRef]
- Smoski, M.J.; Rittenberg, A.; Dichter, G.S. Major depressive disorder is characterized by greater reward network activation to monetary than pleasant image rewards. Psychiatry Res. Neuroimaging 2011, 194, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Wrase, J.; Schlagenhauf, F.; Kienast, T.; Wüstenberg, T.; Bermpohl, F.; Kahnt, T.; Beck, A.; Ströhle, A.; Juckel, G.; Knutson, B. Dysfunction of reward processing correlates with alcohol craving in detoxified alcoholics. Neuroimage 2007, 35, 787–794. [Google Scholar] [CrossRef]
- Büchel, C.; Peters, J.; Banaschewski, T.; Bokde, A.L.; Bromberg, U.; Conrod, P.J.; Flor, H.; Papadopoulos, D.; Garavan, H.; Gowland, P. Blunted ventral striatal responses to anticipated rewards foreshadow problematic drug use in novelty-seeking adolescents. Nat. Commun. 2017, 8, 14140. [Google Scholar] [CrossRef]
- Beck, A.; Schlagenhauf, F.; Wüstenberg, T.; Hein, J.; Kienast, T.; Kahnt, T.; Schmack, K.; Hägele, C.; Knutson, B.; Heinz, A. Ventral striatal activation during reward anticipation correlates with impulsivity in alcoholics. Biol. Psychiatry 2009, 66, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Forbes, E.E.; Rodriguez, E.E.; Musselman, S.; Narendran, R. Prefrontal response and frontostriatal functional connectivity to monetary reward in abstinent alcohol-dependent young adults. PLoS ONE 2014, 9, e94640. [Google Scholar] [CrossRef] [Green Version]
- Bjork, J.M.; Smith, A.R.; Hommer, D.W. Striatal sensitivity to reward deliveries and omissions in substance dependent patients. Neuroimage 2008, 42, 1609–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanczuk-Seiferth, N.; Koehler, S.; Dreesen, C.; Wustenberg, T.; Heinz, A. Pathological gambling and alcohol dependence: Neural disturbances in reward and loss avoidance processing. Addict. Biol. 2015, 20, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Crane, N.A.; Gorka, S.M.; Weafer, J.; Langenecker, S.A.; de Wit, H.; Phan, K.L. Preliminary evidence for disrupted nucleus accumbens reactivity and connectivity to reward in binge drinkers. Alcohol Alcohol. 2017, 52, 647–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilman, J.M.; Smith, A.R.; Bjork, J.M.; Ramchandani, V.A.; Momenan, R.; Hommer, D.W. Cumulative gains enhance striatal response to reward opportunities in alcohol-dependent patients. Addict. Biol. 2015, 20, 580–593. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.; Kirsch, M.; Gerchen, M.F.; Kiefer, F.; Kirsch, P. Striatal activation and frontostriatal connectivity during non-drug reward anticipation in alcohol dependence. Addict. Biol. 2017, 22, 833–843. [Google Scholar] [CrossRef]
- Andrews, M.M.; Meda, S.A.; Thomas, A.D.; Potenza, M.N.; Krystal, J.H.; Worhunsky, P.; Stevens, M.C.; O’Malley, S.; Book, G.A.; Reynolds, B. Individuals family history positive for alcoholism show functional magnetic resonance imaging differences in reward sensitivity that are related to impulsivity factors. Biol. Psychiatry 2011, 69, 675–683. [Google Scholar] [CrossRef] [Green Version]
- Dhingra, I.; Zhang, S.; Zhornitsky, S.; Le, T.M.; Wang, W.; Chao, H.H.; Levy, I.; Li, C.R. The effects of age on reward magnitude processing in the monetary incentive delay task. Neuroimage 2020, 207, 116368. [Google Scholar] [CrossRef]
- First, M.B. Structured clinical interview for DSM-IV axis I disorders. Biom. Res. Dep. 1995. Available online: https://cir.nii.ac.jp/crid/1573387451015011328 (accessed on 1 December 2022).
- Bohn, M.J.; Babor, T.F.; Kranzler, H.R. The Alcohol Use Disorders Identification Test (AUDIT): Validation of a screening instrument for use in medical settings. J. Stud. Alcohol 1995, 56, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De la Fuente, J.R.; Grant, M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson-Koku, G. Beck depression inventory. Occup. Med. 2016, 66, 174–175. [Google Scholar] [CrossRef] [Green Version]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerström test for nicotine dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Dhingra, I.; Zhang, S.; Zhornitsky, S.; Wang, W.; Le, T.M.; Li, C.R. Sex differences in neural responses to reward and the influences of individual reward and punishment sensitivity. BMC Neurosci. 2021, 22, 12. [Google Scholar] [CrossRef]
- Zhornitsky, S.; Dhingra, I.; Le, T.M.; Wang, W.; Li, C.R.; Zhang, S. Reward-Related Responses and Tonic Craving in Cocaine Addiction: An Imaging Study of the Monetary Incentive Delay Task. Int. J. Neuropsychopharmacol. 2021, 24, 634–644. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593. [Google Scholar] [CrossRef]
- Hung, C.C.; Zhang, S.; Chen, C.M.; Duann, J.R.; Lin, C.P.; Lee, T.S.; Li, C.R. Striatal functional connectivity in chronic ketamine users: A pilot study. Am. J. Drug Alcohol Abuse 2020, 46, 31–43. [Google Scholar] [CrossRef]
- Osborne, D.M.; Pearson-Leary, J.; McNay, E.C. The neuroenergetics of stress hormones in the hippocampus and implications for memory. Front. Neurosci. 2015, 9, 164. [Google Scholar] [CrossRef] [Green Version]
- Frank, D.; Kafkas, A. Expectation-driven novelty effects in episodic memory. Neurobiol. Learn. Mem. 2021, 183, 107466. [Google Scholar] [CrossRef] [PubMed]
- Otte, C.; Gold, S.M.; Penninx, B.W.; Pariante, C.M.; Etkin, A.; Fava, M.; Mohr, D.C.; Schatzberg, A.F. Major depressive disorder. Nat. Rev. Dis. Prim. 2016, 2, 16065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunimatsu, A.; Yasaka, K.; Akai, H.; Kunimatsu, N.; Abe, O. MRI findings in posttraumatic stress disorder. J. Magn. Reson. Imaging 2020, 52, 380–396. [Google Scholar] [CrossRef] [PubMed]
- Lazarov, A.; Zhu, X.; Suarez-Jimenez, B.; Rutherford, B.R.; Neria, Y. Resting-state functional connectivity of anterior and posterior hippocampus in posttraumatic stress disorder. J. Psychiatr. Res. 2017, 94, 15–22. [Google Scholar] [CrossRef]
- Galandra, C.; Basso, G.; Manera, M.; Crespi, C.; Giorgi, I.; Vittadini, G.; Poggi, P.; Canessa, N. Salience network structural integrity predicts executive impairment in alcohol use disorders. Sci. Rep. 2018, 8, 14481. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Tian, F.; Zhang, H.; Zeng, J.; Chen, T.; Wang, S.; Jia, Z.; Gong, Q. Cortical and subcortical gray matter shrinkage in alcohol-use disorders: A voxel-based meta-analysis. Neurosci. Biobehav. Rev. 2016, 66, 92–103. [Google Scholar] [CrossRef]
- Tomasi, D.; Wiers, C.E.; Manza, P.; Shokri-Kojori, E.; Michele-Vera, Y.; Zhang, R.; Kroll, D.; Feldman, D.; McPherson, K.; Biesecker, C. Accelerated aging of the amygdala in alcohol use disorders: Relevance to the dark side of addiction. Cereb. Cortex 2021, 31, 3254–3265. [Google Scholar] [CrossRef]
- Campbell, S.; MacQueen, G. The role of the hippocampus in the pathophysiology of major depression. J. Psychiatry Neurosci. 2004, 29, 417–426. [Google Scholar]
- Alba-Ferrara, L.; Müller-Oehring, E.; Sullivan, E.; Pfefferbaum, A.; Schulte, T. Brain responses to emotional salience and reward in alcohol use disorder. Brain Imaging Behav. 2016, 10, 136–146. [Google Scholar] [CrossRef] [Green Version]
- Walker, C.; Kuhn, C.M.; Risher, M.-L. The effects of peri-adolescent alcohol use on the developing hippocampus. Int. Rev. Neurobiol. 2021, 160, 251–280. [Google Scholar] [CrossRef]
- Zorlu, N.; Çapraz, N.; Oztekin, E.; Bagci, B.; Di Biase, M.A.; Zalesky, A.; Gelal, F.; Bora, E.; Durmaz, E.; Beşiroğlu, L. Rich club and reward network connectivity as endophenotypes for alcohol dependence: A diffusion tensor imaging study. Addict. Biol. 2019, 24, 265–274. [Google Scholar] [CrossRef] [PubMed]
- McCoy, A.N.; Crowley, J.C.; Haghighian, G.; Dean, H.L.; Platt, M.L. Saccade reward signals in posterior cingulate cortex. Neuron 2003, 40, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Grupe, D.W.; Nitschke, J.B. Uncertainty and anticipation in anxiety: An integrated neurobiological and psychological perspective. Nat. Rev. Neurosci. 2013, 14, 488–501. [Google Scholar] [CrossRef] [PubMed]
- Andrzejewski, J.A.; Greenberg, T.; Carlson, J.M. Neural correlates of aversive anticipation: An activation likelihood estimate meta-analysis across multiple sensory modalities. Cogn. Affect. Behav. Neurosci. 2019, 19, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Manza, P.; Hu, S.; Chao, H.H.; Zhang, S.; Leung, H.-C.; Chiang-shan, R.L. A dual but asymmetric role of the dorsal anterior cingulate cortex in response inhibition and switching from a non-salient to salient action. Neuroimage 2016, 134, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Ide, J.S.; Shenoy, P.; Angela, J.Y.; Chiang-Shan, R.L. Bayesian prediction and evaluation in the anterior cingulate cortex. J. Neurosci. 2013, 33, 2039–2047. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Sallie, S.N.; Cui, H.; Zeng, N.; Du, J.; Yuan, T.; Li, D.; De Ridder, D.; Zhang, C. Anterior cingulate cortex in addiction: New insights for neuromodulation. Neuromodulation Technol. Neural Interface 2021, 24, 187–196. [Google Scholar] [CrossRef]
- Harel, M.; Perini, I.; Kämpe, R.; Alyagon, U.; Shalev, H.; Besser, I.; Sommer, W.H.; Heilig, M.; Zangen, A. Repetitive transcranial magnetic stimulation in alcohol dependence: A randomized, double-blind, sham-controlled proof-of-concept trial targeting the medial prefrontal and anterior cingulate cortices. Biol. Psychiatry 2022, 91, 1061–1069. [Google Scholar] [CrossRef]
- Fujiwara, J.; Tobler, P.N.; Taira, M.; Iijima, T.; Tsutsui, K.-I. Segregated and integrated coding of reward and punishment in the cingulate cortex. J. Neurophysiol. 2009, 101, 3284–3293. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Mohan, A.; De Ridder, D.; Sunaert, S.; Vanneste, S. The neural correlates of the unified percept of alcohol-related craving: A fMRI and EEG study. Sci. Rep. 2018, 8, 923. [Google Scholar] [CrossRef] [Green Version]
- Hepner, K.A.; Hunter, S.B.; Edelen, M.O.; Zhou, A.J.; Watkins, K. A comparison of two depressive symptomatology measures in residential substance abuse treatment clients. J. Subst. Abus. Treat. 2009, 37, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dum, M.; Pickren, J.; Sobell, L.C.; Sobell, M.B. Comparing the BDI-II and the PHQ-9 with outpatient substance abusers. Addict. Behav. 2008, 33, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-A.; Kim, E.; Morris, R.G.; Park, W.-S. Exploring the non-linear relationship between alcohol consumption and depression in an elderly population in Gangneung: The Gangneung Health Study. Yonsei Med. J. 2015, 56, 418–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baskin-Sommers, A.R.; Foti, D. Abnormal reward functioning across substance use disorders and major depressive disorder: Considering reward as a transdiagnostic mechanism. Int. J. Psychophysiol. 2015, 98, 227–239. [Google Scholar] [CrossRef]
- van Hemel-Ruiter, M.E.; de Jong, P.J.; Ostafin, B.D.; Wiers, R.W. Reward sensitivity, attentional bias, and executive control in early adolescent alcohol use. Addict. Behav. 2015, 40, 84–90. [Google Scholar] [CrossRef]
- Shankman, S.A.; Klein, D.N.; Tenke, C.E.; Bruder, G.E. Reward sensitivity in depression: A biobehavioral study. J. Abnorm. Psychol. 2007, 116, 95. [Google Scholar] [CrossRef] [Green Version]
- Aloi, J.; Blair, K.S.; Crum, K.I.; Bashford-Largo, J.; Zhang, R.; Lukoff, J.; Carollo, E.; White, S.F.; Hwang, S.; Filbey, F.M. Alcohol use disorder, but not cannabis use disorder, symptomatology in adolescents is associated with reduced differential responsiveness to reward versus punishment feedback during instrumental learning. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2020, 5, 610–618. [Google Scholar] [CrossRef]
- Guo, W.; Liu, F.; Yu, M.; Zhang, J.; Zhang, Z.; Liu, J.; Xiao, C.; Zhao, J. Decreased regional activity and network homogeneity of the fronto-limbic network at rest in drug-naive major depressive disorder. Aust. N. Z. J. Psychiatry 2015, 49, 550–556. [Google Scholar] [CrossRef]
- Tucker, D.M.; Luu, P.; Frishkoff, G.; Quiring, J.; Poulsen, C. Frontolimbic response to negative feedback in clinical depression. J. Abnorm. Psychol. 2003, 112, 667. [Google Scholar] [CrossRef]
- Kamarajan, C.; Porjesz, B.; Jones, K.A.; Choi, K.; Chorlian, D.B.; Padmanabhapillai, A.; Rangaswamy, M.; Stimus, A.T.; Begleiter, H. The role of brain oscillations as functional correlates of cognitive systems: A study of frontal inhibitory control in alcoholism. Int. J. Psychophysiol. 2004, 51, 155–180. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, S.; Cardellicchio, P.; Di Fazio, C.; Nazzi, C.; Fracasso, A.; Borgomaneri, S. The Influence of Vicarious Fear-Learning in “Infecting” Reactive Action Inhibition. Front. Behav. Neurosci. 2022, 16, 946263. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Cardellicchio, P.; Di Fazio, C.; Nazzi, C.; Fracasso, A.; Borgomaneri, S. Stopping in (e)motion: Reactive action inhibition when facing valence-independent emotional stimuli. Front. Behav. Neurosci. 2022, 16, 998714. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Spekker, E.; Szabo, A.; Polyak, H.; Vecsei, L. Modelling the neurodevelopmental pathogenesis in neuropsychiatric disorders. Bioactive kynurenines and their analogues as neuroprotective agents-in celebration of 80th birthday of Professor Peter Riederer. J. Neural Transm. 2022, 129, 627–642. [Google Scholar] [CrossRef]
- Tanaka, M.; Szabo, A.; Spekker, E.; Polyak, H.; Toth, F.; Vecsei, L. Mitochondrial Impairment: A Common Motif in Neuropsychiatric Presentation? The Link to the Tryptophan-Kynurenine Metabolic System. Cells 2022, 11, 2607. [Google Scholar] [CrossRef] [PubMed]
- Klinedinst, N.J.; Regenold, W.T. A mitochondrial bioenergetic basis of depression. J. Bioenerg. Biomembr. 2015, 47, 155–171. [Google Scholar] [CrossRef]
- Sikalidis, A.K.; Kelleher, A.H.; Kristo, A.S. Mediterranean Diet. Encyclopedia 2021, 1, 371–387. [Google Scholar] [CrossRef]
- Sikalidis, A.K.; Kelleher, A.H.; Maykish, A.; Kristo, A.S. Non-Alcoholic Beverages, Old and Novel, and Their Potential Effects on Human Health, with a Focus on Hydration and Cardiometabolic Health. Medicina 2020, 56, 490. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men (n = 27) | Women (n = 16) | t | p | |
|---|---|---|---|---|
| Age (years) | 44.9 ± 11.3 | 46.4 ± 15.6 | −0.34 | 0.71 |
| Education (years) | 15.0 ± 3.6 | 14.8 ± 3 | 0.27 | 0.79 |
| AUDIT score | 7.8 ± 9.3 | 4.9 ± 4.8 | 1.15 | 0.26 |
| BDI-II score | 5.0 ± 8.7 | 7.7 ± 8.8 | −0.96 | 0.34 |
| FTND score | 0.4 ± 1.4 | 0.8 ± 2.2 | −0.63 | 0.53 |
| Volume (mm3) | Peak Z | MNI Coordinate (mm) | Side | Identified Brain Region | ||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| Regression with AUDIT | ||||||
| Positive with Win > Nil | ||||||
| 100,845 | 5.34 | −15 | 29 | 43 | L/R | DLPFC, SFG, Precentral G, SMA |
| 4.84 | 36 | −31 | 40 | L/R | IPL, PCC, Precuneus | |
| 49,815 | 5.27 | −21 | −37 | −11 | L | Hippocampus, Amygdala |
| 5.21 | 54 | −46 | −5 | R | Temporal G | |
| 6669 | 4.48 | 6 | 41 | 13 | L/R | ACC |
| 2862 | 4.06 | −9 | −7 | −11 | L/R | Hypothalamus |
| 2511 | 3.85 | −33 | 32 | 4 | L | IFG |
| Negative with Win > Nil | ||||||
| 4266 | 4.06 | 6 | −70 | −35 | L/R | CBL |
| Positive with Loss > Nil | ||||||
| 68,796 | 5.97 | 54 | −31 | −8 | R | Temporal G, Hippocampus, Amygdala, Hypothalamus |
| 5.29 | −12 | −58 | −20 | L | CBL | |
| 84,375 | 5.10 | 18 | −46 | 40 | L/R | Precuneus, DLPFC, MPFC, MCC |
| 4.90 | 60 | −55 | 31 | R | IPL, Precentral G, | |
| 3078 | 4.49 | −33 | 11 | −8 | L | Insula |
| 4806 | 4.30 | −33 | −1 | 40 | L | Precentral gyrus |
| 2538 | 4.30 | 9 | 59 | −5 | R | VMPFC |
| Negative with Loss > Nil | ||||||
| None | ||||||
| Regression with BDI | ||||||
| Positive with Win > Nil | ||||||
| 54,324 | 4.95 | 21 | −7 | −17 | R | Hippocampus, Amygdala, Hypothalamus |
| 4.76 | 45 | −43 | −14 | R | Temporal G | |
| 33,696 | 4.63 | −6 | −40 | 40 | L | Precuneus, PCC, DLPFC, SFG, SMA |
| 6048 | 4.57 | 57 | −61 | 34 | R | IPL |
| 4401 | 4.29 | −42 | −40 | 34 | L | IPL |
| 6399 | 4.26 | −12 | 23 | 40 | L | SFG |
| Negative with Win > Nil | ||||||
| None | ||||||
| Positive with Loss > Nil | ||||||
| 10,665 | 4.89 | −18 | −10 | −20 | L | Hippocampus, Amygdala, Temporal G |
| 25,326 | 4.81 | 24 | −10 | −14 | R | Hippocampus, Amygdala, Temporal G, CBL |
| 6399 | 4.21 | 63 | −46 | 37 | R | IPL |
| 4320 | 4.08 | 21 | 59 | 22 | R | SFG |
| 4158 | 3.84 | −9 | −7 | 34 | L | MCC |
| 2403 | 3.67 | −6 | −37 | 40 | L | MCC |
| Negative with Loss > Nil | ||||||
| None | ||||||
| p Values | |||||||
|---|---|---|---|---|---|---|---|
| X | M | Y | X → M | M → Y | X → Y | Mediated X → Y | Mediation |
| Win > Nil | |||||||
| AUDIT | BDI | Brain | <0.001 | 0.006 | <0.001 | <0.001 | 0.021 |
| Brain | BDI | AUDIT | <0.001 | 0.190 | <0.001 | <0.001 | 0.204 |
| AUDIT | Brain | BDI | <0.001 | 0.006 | <0.001 | 0.190 | 0.013 |
| BDI | Brain | AUDIT | <0.001 | <0.001 | <0.001 | 0.190 | 0.005 * |
| Brain | AUDIT | BDI | <0.001 | 0.190 | <0.001 | 0.006 | 0.201 |
| BDI | AUDIT | Brain | <0.001 | <0.001 | <0.001 | 0.006 | 0.009 |
| Loss > Nil | |||||||
| AUDIT | BDI | Brain | <0.001 | 0.010 | <0.001 | <0.001 | 0.029 |
| Brain | BDI | AUDIT | <0.001 | 0.149 | <0.001 | <0.001 | 0.166 |
| AUDIT | Brain | BDI | <0.001 | 0.010 | <0.001 | 0.149 | 0.020 |
| BDI | Brain | AUDIT | <0.001 | <0.001 | <0.001 | 0.149 | 0.006 * |
| Brain | AUDIT | BDI | <0.001 | 0.149 | <0.001 | 0.010 | 0.162 |
| BDI | AUDIT | Brain | <0.001 | <0.001 | <0.001 | 0.010 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Dhingra, I.; Le, T.M.; Zhornitsky, S.; Zhang, S.; Li, C.-S.R. Win and Loss Responses in the Monetary Incentive Delay Task Mediate the Link between Depression and Problem Drinking. Brain Sci. 2022, 12, 1689. https://doi.org/10.3390/brainsci12121689
Chen Y, Dhingra I, Le TM, Zhornitsky S, Zhang S, Li C-SR. Win and Loss Responses in the Monetary Incentive Delay Task Mediate the Link between Depression and Problem Drinking. Brain Sciences. 2022; 12(12):1689. https://doi.org/10.3390/brainsci12121689
Chicago/Turabian StyleChen, Yu, Isha Dhingra, Thang M. Le, Simon Zhornitsky, Sheng Zhang, and Chiang-Shan R. Li. 2022. "Win and Loss Responses in the Monetary Incentive Delay Task Mediate the Link between Depression and Problem Drinking" Brain Sciences 12, no. 12: 1689. https://doi.org/10.3390/brainsci12121689