
Endoscopic Endonasal Resection of the Medial Wall of the Cavernous Sinus and Its Impact on Outcomes of Pituitary Surgery: A Systematic Review and Meta-Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
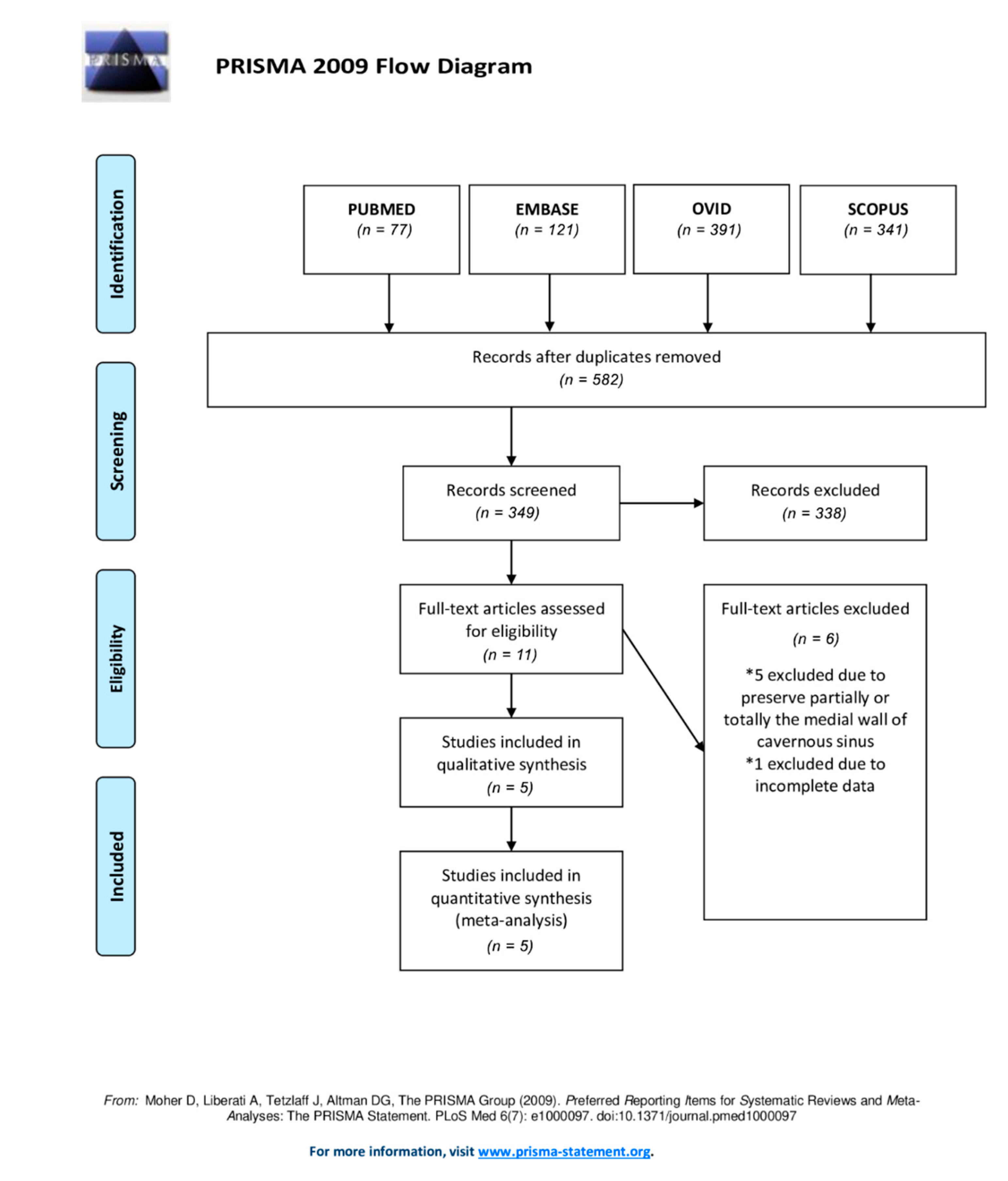
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Statistical Analysis
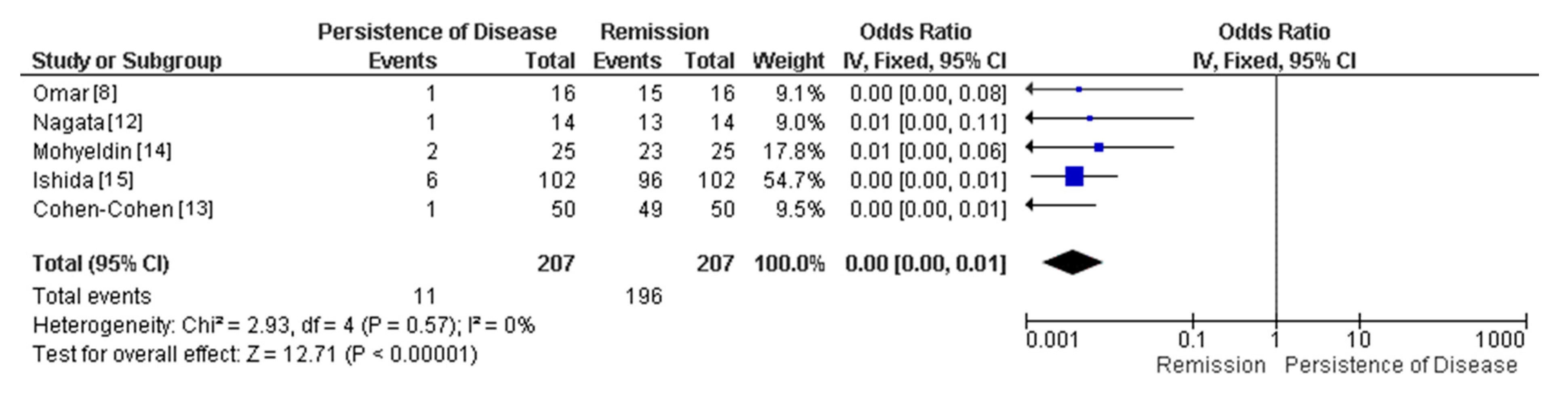
3. Results
3.1. Study Selection
3.2. Demographics and Tumor Characteristics of Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CS | Cavernous Sinus |
| MW | MedialWall |
| CN | Cranial Nerve |
| CSF | Cerebrospinal Fluid |
References
- Molitch, M.E. Diagnosis and Treatment of Pituitary Adenomas: A Review. JAMA 2017, 317, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Gondim, J.A.; Schops, M.; de Almeida, J.P.; de Albuquerque, L.A.; Gomes, E.; Ferraz, T.; Barroso, F.A. Endoscopic endonasal transsphenoidal surgery: Surgical results of 228 pituitary adenomas treated in a pituitary center. Pituitary 2010, 13, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Marigil Sanchez, M.; Karekezi, C.; Almeida, J.P.; Kalyvas, A.; Castro, V.; Velasquez, C.; Gentili, F. Management of Giant Pituitary Adenomas: Role and Outcome of the Endoscopic Endonasal Surgical Approach. Neurosurg. Clin. N. Am. 2019, 30, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.P.; Gentili, F. Endoscopic skull base surgery and the evolution of approaches to anterior cranial base lesions. J. Neurosurg. Sci. 2021, 65, 101–102. [Google Scholar] [CrossRef] [PubMed]
- Scotti, G.; Yu, C.Y.; Dillon, W.P.; Norman, D.; Colombo, N.; Newton, T.H.; De Groot, J.; Wilson, C.B. MR imaging of cavernous sinus involvement by pituitary adenomas. AJR Am. J. Roentgenol. 1988, 151, 799–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oruçkaptan, H.H.; Senmevsim, O.; Ozcan, O.E.; Ozgen, T. Pituitary adenomas: Results of 684 surgically treated patients and review of the literature. Surg. Neurol. 2000, 53, 211–219. [Google Scholar] [CrossRef]
- Almeida, J.P.; de Andrade, E.; Reghin-Neto, M.; Radovanovic, I.; Recinos, P.F.; Kshettry, V.R. From Above and Below: The Microsurgical Anatomy of Endoscopic Endonasal and Transcranial Microsurgical Approaches to the Parasellar Region. World Neurosurg. 2022, 159, e139–e160. [Google Scholar] [CrossRef] [PubMed]
- Omar, A.T., 2nd; Munoz, D.G.; Goguen, J.; Lee, J.M.; Rotondo, F.; Kovacs, K.; Cusimano, M.D. Resection of the medial wall of the cavernous sinus in functioning pituitary adenomas: Technical note and outcomes in a matched-cohort study. Clin. Neurol. Neurosurg. 2020, 200, 106306. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, E.H. Cushing’s Disease: Lessons Learned From 1500 Cases. Neurosurgery 2017, 64 (Suppl. 1), 27–36. [Google Scholar] [CrossRef] [PubMed]
- Rindler, R.S.; Leonel, L.C.; Graepel, S.; Agosti, E.; Kerezoudis, P.; Pinheiro-Neto, C.D.; Peris-Celda, M. The endonasal midline inferior intercavernous approach to the cavernous sinus: Technical note, cadaveric step-by-step illustration, and case presentation. Acta Neurochir. 2022, 164, 2573–2580. [Google Scholar] [CrossRef] [PubMed]
- Truong, H.Q.; Lieber, S.; Najera, E.; Alves-Belo, J.T.; Gardner, P.A.; Fernandez-Miranda, J.C. The medial wall of the cavernous sinus. Part 1: Surgical anatomy, ligaments, and surgical technique for its mobilization and/or resection. J. Neurosurg. 2018, 131, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Nagata, Y.; Takeuchi, K.; Yamamoto, T.; Ishikawa, T.; Kawabata, T.; Shimoyama, Y.; Wakabayashi, T. Removal of the Medial Wall of the Cavernous Sinus for Functional Pituitary Adenomas: A Technical Report and Pathologic Significance. World Neurosurg. 2019, 126, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Cohen, S.; Gardner, P.A.; Alves-Belo, J.T.; Truong, H.Q.; Snyderman, C.H.; Wang, E.W.; Fernandez-Miranda, J.C. The medial wall of the cavernous sinus. Part 2: Selective medial wall resection in 50 pituitary adenoma patients. J. Neurosurg. 2018, 131, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Mohyeldin, A.; Katznelson, L.J.; Hoffman, A.R.; Asmaro, K.; Ahmadian, S.S.; Eltobgy, M.M.; Nayak, J.V.; Patel, Z.M.; Hwang, P.H.; Fernandez-Miranda, J.C. Prospective intraoperative and histologic evaluation of cavernous sinus medial wall invasion by pituitary adenomas and its implications for acromegaly remission outcomes. Sci. Rep. 2022, 12, 9919. [Google Scholar] [CrossRef] [PubMed]
- Ishida, A.; Shiramizu, H.; Yoshimoto, H.; Kato, M.; Inoshita, N.; Miki, N.; Ono, M.; Yamada, S. Resection of the Cavernous Sinus Medial Wall Improves Remission Rate in Functioning Pituitary Tumors: Retrospective Analysis of 248 Consecutive Cases. Neurosurgery 2022. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, H.; Fukuhara, N.; Horiguchi, K.; Yamada, S. Aggressive transsphenoidal resection of tumors invading the cavernous sinus in patients with acromegaly: Predictive factors, strategies, and outcomes. J. Neurosurg. 2014, 121, 505–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micko, A.S.; Wöhrer, A.; Wolfsberger, S.; Knosp, E. Invasion of the cavernous sinus space in pituitary adenomas: Endoscopic verification and its correlation with an MRI-based classification. J. Neurosurg. 2015, 122, 803–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakomkin, N.; Van Gompel, J.J.; Post, K.D.; Cho, S.S.; Lee, J.Y.K.; Hadjipanayis, C.G. Fluorescence guided surgery for pituitary adenomas. J. Neurooncol. 2021, 151, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Chibbaro, S.; Signorelli, F.; Milani, D.; Cebula, H.; Scibilia, A.; Bozzi, M.T.; Messina, R.; Zaed, I.; Todeschi, J.; Ollivier, I.; et al. Primary Endoscopic Endonasal Management of Giant Pituitary Adenomas: Outcome and Pitfalls from a Large Prospective Multicenter Experience. Cancers 2021, 13, 3603. [Google Scholar] [CrossRef] [PubMed]
- Lonser, R.R.; Ksendzovsky, A.; Wind, J.J.; Vortmeyer, A.O.; Oldfield, E.H. Prospective evaluation of the characteristics and incidence of adenoma-associated dural invasion in Cushing disease. J. Neurosurg. 2012, 116, 272–279. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient and Tumor Characteristics | |
|---|---|
| Sex | Number of cases (%) |
| Male | 88 (42.31%) |
| Female | 120 (57.69%) |
| Mean Age | 48.87 |
| Knosp Grade | |
| Grade 0 | 42 (20.19%) |
| Grade 1 | 77 (37.02%) |
| Grade 2 | 53 (25.48%) |
| Grade 3 | 31 (14.90%) |
| Grade 4 | 5 (2.40%) |
| Previous Surgery | 19 (9.13%) |
| Tumor Size * | |
| Macroadenoma | 108 (59.34%) |
| Microadenoma | 74 (40.66%) |
| Tumor Type | |
| Non-functional | 15 (7.21%) |
| ACTH adenoma | 39 (18.75%) |
| Prolactinoma | 25 (12.02%) |
| GH adenoma | 127 (61.065%) |
| TSH-secreting adenoma | 2 (0.96%) |
| Complication Rate | 10/208 (4.81%) |
| Remission § | 196/207 (94.69%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Macêdo Filho, L.J.M.; Diógenes, A.V.G.; Barreto, E.G.; Pahwa, B.; Samson, S.L.; Chaichana, K.; Quinones-Hinojosa, A.; Almeida, J.P. Endoscopic Endonasal Resection of the Medial Wall of the Cavernous Sinus and Its Impact on Outcomes of Pituitary Surgery: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 1354. https://doi.org/10.3390/brainsci12101354
de Macêdo Filho LJM, Diógenes AVG, Barreto EG, Pahwa B, Samson SL, Chaichana K, Quinones-Hinojosa A, Almeida JP. Endoscopic Endonasal Resection of the Medial Wall of the Cavernous Sinus and Its Impact on Outcomes of Pituitary Surgery: A Systematic Review and Meta-Analysis. Brain Sciences. 2022; 12(10):1354. https://doi.org/10.3390/brainsci12101354
Chicago/Turabian Stylede Macêdo Filho, Leonardo J. M., Ana Vitória G. Diógenes, Esther G. Barreto, Bhavya Pahwa, Susan L. Samson, Kaisorn Chaichana, Alfredo Quinones-Hinojosa, and Joao Paulo Almeida. 2022. "Endoscopic Endonasal Resection of the Medial Wall of the Cavernous Sinus and Its Impact on Outcomes of Pituitary Surgery: A Systematic Review and Meta-Analysis" Brain Sciences 12, no. 10: 1354. https://doi.org/10.3390/brainsci12101354