
A Pilot Study Assessing the Effects of Goal Management Training on Cognitive Functions among Individuals with Major Depressive Disorder and the Effect of Post-Traumatic Symptoms on Response to Intervention

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
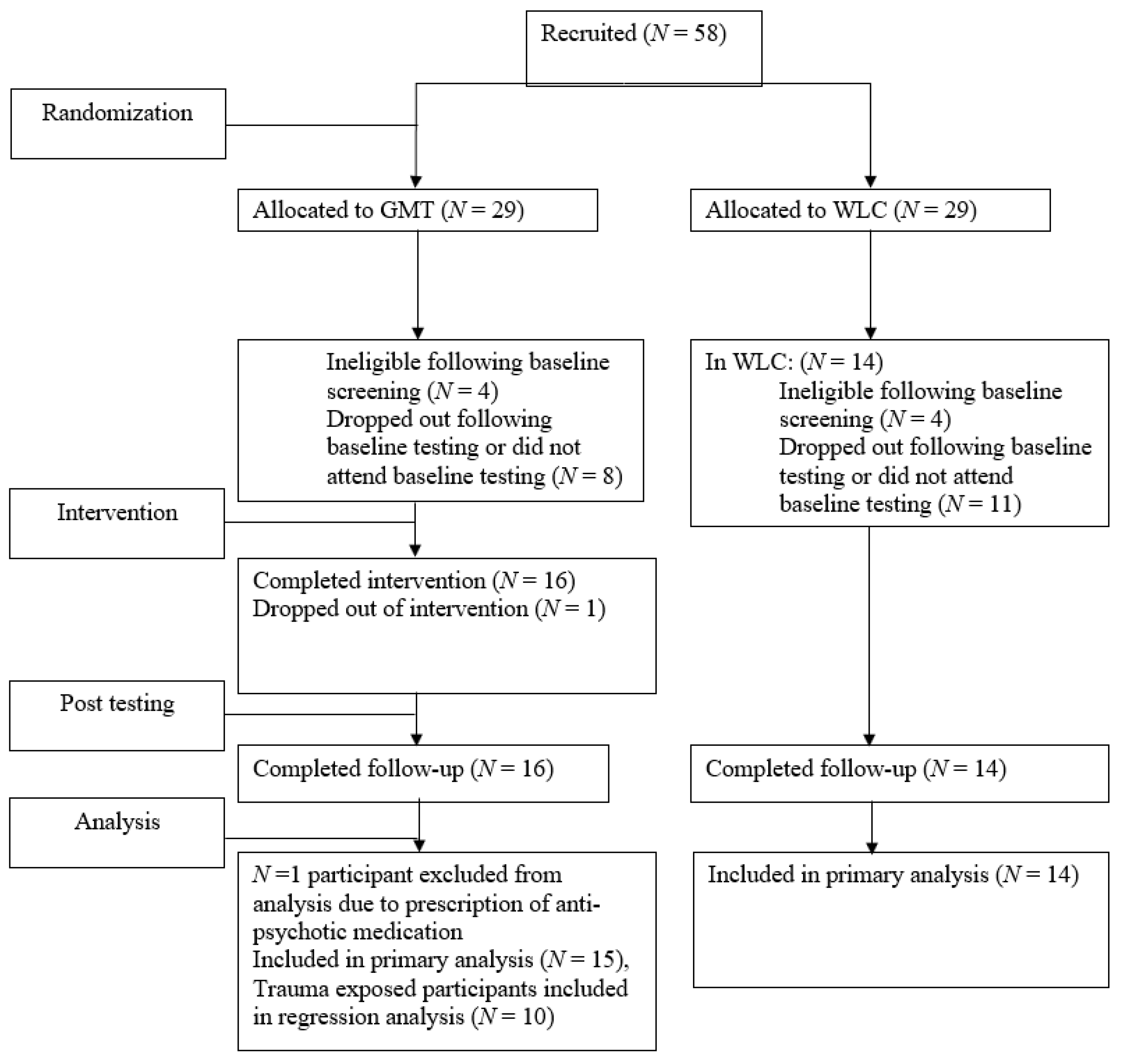
2.1. Participants
2.2. Experimental Design and Procedure
2.3. Study Conditions
2.3.1. GMT
2.3.2. WLC
2.4. Measures and Materials
2.4.1. Clinical Interviews
2.4.2. Symptom Measures
2.4.3. Subjective Cognition
2.4.4. Neuropsychological Assessment
2.5. Data Analysis
3. Results
3.1. Neuropsychological Assessment
3.1.1. Attention/Concentration and Processing Speed
3.1.2. Response Inhibition
3.1.3. Self-Report Questionnaires
3.1.4. PTSD Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, VA, USA, 2022. [Google Scholar] [CrossRef]
- Angelakis, S.; Nixon, R. The Comorbidity of PTSD and MDD: Implications for Clinical Practice and Future Research. Behav. Change 2015, 32, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Afifi, T.O.; MacMillan, H.L.; Boyle, M.; Taillieu, T.; Cheung, K.; Sareen, J. Child abuse and mental disorders in Canada. Can. Med. Assoc. J. 2014, 186, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, R.A.; Schell, T.L.; Hambarsoomian, K.; Marshall, G.N.; Belzberg, H. Prevalence of PTSD and Major Depression following trauma-center hospitalization. J. Trauma 2010, 69, 1560–1566. [Google Scholar] [PubMed] [Green Version]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.C.; Matt, G.; Wrocklage, K.M.; Crnich, C.; Jordan, J.; Southwick, S.M.; Krystal, J.H.; Schweinsburg, B.C. A quantitative meta-analysis of neurocognitive functioning in posttraumatic stress disorder. Psychol. Bull. 2015, 141, 105–140. [Google Scholar] [CrossRef]
- Bora, E.; Harrison, B.J.; Yücel, M.; Pantelis, C. Cognitive impairment in euthymic major depressive disorder: A meta-analysis. Psychol. Med. 2013, 43, 2017–2026. [Google Scholar] [CrossRef]
- Larsen, S.E.; Fleming, C.J.E.; Resick, P.A. Residual symptoms following empirically supported treatment for PTSD. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 207–215. [Google Scholar] [CrossRef]
- Parlar, M.; Frewen, P.A.; Oremus, C.; Lanius, R.A.; McKinnon, M.C. Dissociative symptoms are associated with reduced neuropsychological performance in patients with recurrent depression and a history of trauma exposure. Eur. J. Psychotraumatol. 2016, 7, 29061. [Google Scholar] [CrossRef]
- Lam, R.W.; Kennedy, S.H.; McIntyre, R.S.; Khullar, A. Cognitive dysfunction in major depressive disorder: Effects on psychosocial functioning and implications for treatment. Can. J. Psychiatry 2014, 59, 649–654. [Google Scholar] [CrossRef] [Green Version]
- Yen, Y.C.; Rebok, G.W.; Gallo, J.J.; Jones, R.N.; Tennstedt, S.L. Depressive symptoms impair everyday problem-solving ability through cognitive abilities in late life. Am. J. Ger. Psychiatry 2011, 19, 142–150. [Google Scholar] [CrossRef] [Green Version]
- McLennan, S.N.; Mathias, J.L. The depression-executive dysfunction (DED) syndrome and response to antidepressants: A meta-analytic review. Int. J. Ger. Psychiatry 2010, 25, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Crews, W.D.; Harrison, D.W. The neuropsychology of depression and its implications for cognitive therapy. Neuropsychol. Rev. 1995, 5, 81–123. [Google Scholar] [CrossRef] [PubMed]
- Nijdam, M.J.; Gersons, B.P.; Olff, M. Response to psychotherapy for posttraumatic stress disorder: The role of pretreatment verbal memory performance. J. Clin. Psychiatry 2015, 76, e1023–e1028. [Google Scholar] [CrossRef] [PubMed]
- Motter, J.N.; Pimontel, M.A.; Rindskopf, D.; Devanand, D.P.; Doraiswamy, P.M.; Sneed, J.R. Computerized cognitive training and functional recovery in major depressive disorder: A meta-analysis. J. Affect. Dis. 2016, 189, 184–191. [Google Scholar] [CrossRef]
- Preiss, M.; Shatil, E.; Čermáková, R.; Cimermanová, D.; Ram, I. Personalized cognitive training in unipolar and bipolar disorder: A study of cognitive functioning. Front. Hum. Neurosci. 2013, 7, 108. [Google Scholar] [CrossRef] [Green Version]
- Siegle, G.J.; Price, R.B.; Jones, N.P.; Ghinassi, F.; Painter, T.; Thase, M.E. You gotta work at it: Pupillary indices of task focus are prognostic for response to a neurocognitive intervention for rumination in depression. Clin. Psychol. Sci. 2014, 2, 455–471. [Google Scholar] [CrossRef]
- Trapp, W.; Engel, S.; Hajak, G.; Lautenbacher, S.; Gallhofer, B. Cognitive remediation for depressed inpatients: Results of a pilot randomized controlled trial. Aust. New Zealand J. Psychiatry 2016, 50, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Harvey, A.G.; Lee, J.; Smith, R.L.; Gumport, N.B.; Hollon, S.D.; Rabe-Hesketh, S.; Hein, K.; Dolsen, M.R.; Hamen, K.; Kanady, J.C.; et al. Improving outcome for mental disorders by enhancing memory for treatment. Behav. Res. Ther. 2016, 81, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Gumport, N.B.; Dong, L.; Lee, J.Y.; Harvey, A.G. Patient learning of treatment contents in cognitive therapy. J. Behav. Ther. Exp. Psychiatry 2018, 58, 51–59. [Google Scholar] [CrossRef]
- Bowie, C.R.; Gupta, M.; Holshausen, K.; Jokic, R.; Best, M.; Milev, R. Cognitive remediation for treatment-resistant depression: Effects on cognition and functioning and the role of online homework. J. Nerv. Ment. Dis. 2013, 201, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.; Robertson, I.H.; Clare, L.; Carter, G.; Hong, J.; Wilson, B.A.; Duncan, J.S.; Stuss, D.T. Rehabilitation of executive functioning: An experimental–clinical validation of Goal Management Training. J. Int. Neuropsychol. Soc. 2000, 6, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.; Schweizer, T.A.; O’Connor, C.; Turner, G.; Gillingham, S.; Stuss, D.T.; Manly, T.; Robertson, I.H. Rehabilitation of Executive Functioning in Patients with Frontal Lobe Brain Damage with Goal Management Training. Front. Hum. Neurosci. 2011, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antony, M.M.; Bieling, P.J.; McCabe, R.E. Cognitive-Behavioral Therapy in Groups; The Guilford Press: New York, NY, USA, 2009; Available online: https://books.google.ca/books?hl=en&lr=&id=tVtoyte1AEIC&oi=fnd&pg=PP1&dq=bieling+antony+mccabe+2009&ots=u8bq9brrWP&sig=Ff1jFKFaUguMVDUSFLjxNn8Kiv8 (accessed on 29 June 2022).
- Stamenova, V.; Levine, B. Effectiveness of goal management training® in improving executive functions: A meta-analysis. Neuropsychol. Rehabil. 2018, 29, 1569–1599. [Google Scholar] [CrossRef]
- Hagen, B.I.; Lau, B.; Joormann, J.; Småstuen, M.C.; Landrø, N.I.; Stubberud, J. Goal management training as a cognitive remediation intervention in depression: A randomized controlled trial. J. Affect. Dis. 2020, 275, 268–277. [Google Scholar] [CrossRef]
- Boyd, J.E.; O’Connor, C.; Protopopescu, A.; Jetly, R.; Rhind, S.G.; Lanius, R.A.; McKinnon, M.C. An Open-Label Feasibility Trial Examining the Effectiveness of a Cognitive Training Program, Goal Management Training, in Individuals with Posttraumatic Stress Disorder. Chronic Stress 2019, 3, 1–13. [Google Scholar] [CrossRef]
- Protopopescu, A.; O’Connor, C.; Cameron, D.; Boyd, J.E.; Lanius, R.A.; McKinnon, M.C. A Pilot Randomized Controlled Trial of Goal Management Training in Canadian Military Members, Veterans, and Public Safety Personnel Experiencing Post-Traumatic Stress Symptoms. Brain Sci. 2022, 12, 377. [Google Scholar] [CrossRef]
- Cameron, D.H.; McCabe, R.E.; Rowa, K.; O’Connor, C.; McKinnon, M.C. A pilot study examining the use of Goal Management Training in individuals with obsessive-compulsive disorder. Pilot Feasibility Stud. 2020, 6, 151. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-4-TR; American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Balker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33. [Google Scholar]
- Weathers, F.W.; Blake, D.D.; Schnurr, P.P.; Kaloupek, D.G.; Marx, B.P.; Keane, T.M. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5). 2013; U.S. Department of Veteran’s Affairs. Available online: https://www.ptsd.va.gov/professional/assessment/adult-int/caps.asp (accessed on 30 June 2015).
- Fydrich, T.; Dowdall, D.; Chambless, D.L. Reliability and validity of the Beck Anxiety Inventory. J. Anxiety Dis. 1992, 6, 55–61. [Google Scholar] [CrossRef]
- Steer, R.A.; Ranieri, W.F.; Beck, A.T.; Clark, D.A. Further evidence for the validity of the beck anxiety inventory with psychiatric outpatients. J. Anxiety Dis. 1993, 7, 195–205. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory-II (BDI-II); Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Personal. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Steer, R.A.; Ball, R.; Ranieri, W.F.; Beck, A.T. Further evidence for the construct validity of the Beck Depression Inventory-II with psychiatric outpatients. Psychol. Rep. 1997, 80, 443–446. [Google Scholar] [CrossRef]
- Broadbent, D.E.; Cooper, P.F.; Fitzgerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bridger, R.S.; Johnsen, S.Å.K.; Brasher, K. Psychometric properties of the cognitive failures questionnaire. Ergonomics 2013, 56, 1515–1524. [Google Scholar] [CrossRef]
- Conners, C.K. Conners’ Continuous Performance Test II: Computer Program for Windows Technical Guide and Software Manual; Multi-Health Systems: North Tonawanda, NY, USA, 2000. [Google Scholar]
- Reitan, R.M.; Wolfson, D. The Halstead-Reitan Neuropsychological Battery: Theory and Clinical Interpretation; Neuropsychology Press: Tucson, AZ, USA, 1985. [Google Scholar]
- Wechsler, D. Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV); Psychological Corporation: San Antonio, TX, USA, 2008. [Google Scholar]
- Golden, C.J. Stroop Color and Word Test: A Manual for Clinical and Experimental Uses; Stoelting Co.: Chicago, IL, USA, 1978. [Google Scholar]
- Grant, D.A.; Berg, E. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J. Exp. Psychol. 1948, 38, 404–411. [Google Scholar] [CrossRef]
- Delis, D.C.; Kramer, J.H.; Kaplan, E.; Ober, B.A. California Verbal Learning Test-II (CVLT-II); The Psychological Corporation: San Antonio, TX, USA, 2000. [Google Scholar]
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence-Second Edition (WASI-II); NCS Pearson: San Antonio, TX, USA, 2011. [Google Scholar]
- O’Connor, C.; Robertson, I.H.; Levine, B. The prosthetics of vigilant attention: Random cuing cuts processing demands. Neuropsychology 2011, 25, 535–543. [Google Scholar] [CrossRef]
- Nixon, R.D.; Nearmy, D.M. Treatment of comorbid posttraumatic stress disorder and major depressive disorder: A pilot study. J. Trauma. Stress 2011, 24, 451–455. [Google Scholar] [CrossRef]
- Buist-Bouwman, M.A.; Ormel, J.; De Graaf, R.; De Jonge, P.; Van Sonderen, E.; Vollebergh, W.A.M.; ESEMeD/MHEDEA 2000 investigators. Mediators of the association between depression and role functioning. Acta Psychiatr. Scand. 2008, 118, 451–458. [Google Scholar] [CrossRef] [Green Version]
- Pentaraki, A.D. Treatment outcomes in depression: Reducing drop-out rates in cognitive therapy. BJPsych Adv. 2018, 24, 101–109. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| GMT Session | Description |
|---|---|
| Session 1: The Absent Mind, the Present Mind | Introduce the concept of absentmindedness and normalize the experience. Explain present-mindedness using mindfulness techniques. |
| Session 2: Absentminded Slip-Ups | Introduce construct of absentminded slips with examples, and discuss emotional and practical consequences. Introduce the “Body Scan” mindfulness exercise. |
| Session 3: The Automatic Pilot | Describe “automatic pilot” as being a habitual mechanism which can lead to inappropriate responses or actions if not monitored. Introduce the “Breathing Exercise” mindfulness technique. |
| Session 4: Stop the Automatic Pilot | Participants are introduced to the “STOP!” technique as a method of bringing one’s attention to the present to monitor current behavior. The short “Breath Focus” mindfulness exercise is described. |
| Session 5: The Mental Blackboard | The construct of working memory as a “mental blackboard,” which can be erased or over saturated with information, is explained. Participants are taught to check “the mental blackboard” to keep current goals at the forefront of memory. Introduce how to incorporate present-mindedness (specifically the “Breath Focus”) into behavior monitoring and executing difficult tasks as a method for increasing accuracy and memory. |
| Session 6: State Your Goal | Describe how goals can become entangled when attempting to multi-task. Introduce the concept of stating one’s goal as a way to aid encoding and recall of that goal. |
| Session 7: Making Decisions | Introduce the concept of conflicting goals and detail strategies for how to make decisions. Review methods for keeping track of complex goals using to-do lists. |
| Session 8: Splitting Tasks into Subtasks | Practice completing tasks that are too complex to rely on working memory only, and detail strategies for how to divide large goals into a series of smaller, more manageable subgoals. |
| Session 9: STOP! | Review the material covered across previous sessions and underscore the importance of goal monitoring (the “STOP!” technique). |
| Variable | Group | Mean (SD) | |||
| Age | GMT | 52.0 (8.77) | |||
| WLC | 46.64 (11.69) | ||||
| Education | GMT | 14.80 (2.01) | |||
| WLC | 15.43 (2.90) | ||||
| Medication | Group | % | |||
| Anti-depressant (e.g., SSRI, SNIR, Tricyclic) | GMT | 80.00 | |||
| WL | 92.86 | ||||
| Atypical Antipsychotic | GMT | 20.00 | |||
| WL | 35.71 | ||||
| Benzodiazepine | GMT | 40.00 | |||
| WL | 28.57 | ||||
| Anti-convulsant | GMT | 20.00 | |||
| WL | 7.14 | ||||
| Lithium | GMT | 13.33 | |||
| WL | 7.14 | ||||
| Variable | Group | Time 1 Mean (SD) | Time 2 Mean (SD) | Time 3 Mean (SD) | Pairwise Comparisons |
| BAI Total Score | GMT | 23.13 (12.54) | 19,47 (11.96) | 21.45 (13.17) | ↓ T1 to T2 * |
| WLC | 27.00 (16.06) | 27.50 (15.97) | 25.71 (14.54) | n.s. | |
| BDI Total Score | GMT | 29.46 (11.33) | 25.60 (13.73) | 25.20 (11.90) | n.s. |
| WLC | 30.07 (12.42) | 28.64 (14.28) | 31.93 (12.04) | n.s. | |
| CFQ Total Score | GMT | 58.43 (13.09) | 51.85 (16.82) | 51.12 (13.92) | ↓ T1 to T2 ** |
| WLC | 59.64 (12.86) | 60.79 (11.46) | 60.07 (10.77) | n.s. | |
| CVLT Trial 1–5 T-Score | GMT | 52.27 (8.23) | 59.00 (9.50) | 57.50 (8.15) | n.s. |
| WLC | 53.79 (12.09) | 56.50 (11.84) | 57.21 (11.99) | n.s. | |
| CVLT Short Delay Free Recall Z-Score | GMT | 0.03 (0.72) | 0.53 (0.94) | 0.67 (0.81) | n.s. |
| WLC | 0.25 (1.24) | 0.61 (1.11) | 0.75 (1.31) | n.s. | |
| CVLT Long Delay Free Recall Z-Score | GMT | −0.02 (0.62) | 0.41 (0.85) | 0.38 (0.88) | n.s. |
| WLC | 0.32 (1.28) | 0.43 (1.22) | 0.39 (1.36) | n.s. | |
| CVLT Total Repetitions Z-Score | GMT | 0.27 (1.19) | 0.17 (1.04) | 0.21 (0.89) | n.s. |
| WLC | 0.00 (0.76) | −0.11 (0.98) | −0.04 (1.18) | n.s. | |
| CVLT Total Intrusions Z-Score | GMT | −0.20 (0.82) | −0.20 (0.89) | −0.21 (0.94) | n.s. |
| WLC | −0.11 (0.63) | 0.14 (0.89) | 0.18 (1.19) | n.s. | |
| Stroop Word T-Score | GMT | 40.93 (7.79) | 39.07 (7.41) | 38.73 (8.51) | n.s. |
| WLC | 42.00 (10.96) | 43.79 (12.27) | 44.29 (12.74) | n.s. | |
| Stroop Color T-Score | GMT | 40.43 (5.98) | 40.43 (8.93) | 39.81 (8.76) | n.s. |
| WLC | 40.07 (8.06) | 39.21 (10.05) | 40.43 (9.77) | n.s. | |
| Stroop Interference T-Score | GMT | 48.29 (7.55) | 52.36 (6.59) | 49.84 (6.96) | ↑ T1 to T2 * |
| WLC | 46.86 (9.41) | 48.50 (7.36) | 48.00 (8.77) | n.s. | |
| Stroop Color-Word T-Score | GMT | 46.32 (9.34) | 51.00 (9.69) | 50.23 (9.62) | ↑ T1 to T2 *** |
| WLC | 51.21 (5.77) | 51.29 (7.85) | 51.65 (4.75) | n.s. | |
| WASI Coding Scaled Score | GMT | 10.50 (2.24) | 11.07 (2.06) | 11.09 (2.39) | ↑ T1 to T2 ** |
| WLC | 9.86 (3.09) | 10.21 (3.31) | 10.36 (3.59) | n.s. | |
| TMT-A T-Score | GMT | 49.79 (8.35) | 52.00 (12.17) | 52.63 (13.58) | n.s. |
| WLC | 47.00 (12.86) | 49.50 (12.82) | 52.64 (9.38) | ↑ T1 to T3 * | |
| TMT-B T-Score | GMT | 50.29 (10.0) | 51.36 (8.22) | 52.18 (15.13) | n.s. |
| WLC | 48.57 (11.69) | 52.71 (14.31) | 53.29 (13.47) | ↑ T1 to T3 * | |
| WCST Total Correct T-Score | GMT | 67.23 (11.20) | 71.38 (11.33) | 66.68 (6.14) | n.s. |
| WLC | 67.71 (9.24) | 72.36 (10.76) | 72.36 (13.12) | n.s. | |
| WCST Total Errors T-Score | GMT | 49.92 (9.89) | 51.08 (7.85) | 50.30 (11.07) | n.s. |
| WLC | 47.00 (11.34) | 47.93 (8.90) | 47.79 (8.95) | n.s. | |
| WCST Perseverative Errors T-Score | GMT | 50.61 (7.68) | 51.69 (8.46) | 51.80 (8.90) | n.s. |
| WLC | 47.93 (10.28) | 48.86 (7.28) | 48.64 (9.190 | n.s. | |
| WCST Non-Perseverative Errors T-Score | GMT | 49.38 (11.64) | 49.69 (7.36) | 47.90 (12.13) | n.s. |
| WLC | 46.71 (10.99) | 46.21 (9.36) | 46.29 (8.41) | n.s. | |
| CPT Omission Error T-Score | GMT | 57.99 (12.57) | 51.42 (14.66) | 51.26 (12.38) | n.s. |
| WLC | 51.97 (12.46) | 50.83 (6.95) | 54.92 (14.13) | n.s. | |
| CPT Commission Errors | GMT | 52.63 (9.44) | 45.93 (7.91) | 46.11 (6.93) | ↓ T1 to T2 * |
| WLC | 53.31 (13.14) | 50.84 (12.04) | 50.45 (12.63) | n.s. | |
| CPT Hit Reaction Time T-Score | GMT | 55.10 (11.41) | 56.49 (8.63) | 53.70 (8.01) | n.s. |
| WLC | 57.83 (11.80) | 55.27 (11.72) | 58.20 (12.43) | n.s. | |
| CPT Variability T-Score | GMT | 54.71 (9.46) | 51.24 (11.48) | 54.50 (11.53) | n.s. |
| WLC | 56.59 (15.06) | 53.28 (13.11) | 52.98 (16.11) | n.s. | |
| CPT d’ T-Score | GMT | 49.40 (10.06) | 46.09 (9.65) | 45.89 (9.49) | ↑ T1 to T3 * |
| WLC | 51.14 (13.96) | 50.03 (10.37) | 47.62 (10.72) | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyd, J.E.; Sanger, B.D.; Cameron, D.H.; Protopopescu, A.; McCabe, R.E.; O’Connor, C.; Lanius, R.A.; McKinnon, M.C. A Pilot Study Assessing the Effects of Goal Management Training on Cognitive Functions among Individuals with Major Depressive Disorder and the Effect of Post-Traumatic Symptoms on Response to Intervention. Brain Sci. 2022, 12, 864. https://doi.org/10.3390/brainsci12070864
Boyd JE, Sanger BD, Cameron DH, Protopopescu A, McCabe RE, O’Connor C, Lanius RA, McKinnon MC. A Pilot Study Assessing the Effects of Goal Management Training on Cognitive Functions among Individuals with Major Depressive Disorder and the Effect of Post-Traumatic Symptoms on Response to Intervention. Brain Sciences. 2022; 12(7):864. https://doi.org/10.3390/brainsci12070864
Chicago/Turabian StyleBoyd, Jenna E., Brahm D. Sanger, Duncan H. Cameron, Alina Protopopescu, Randi E. McCabe, Charlene O’Connor, Ruth A. Lanius, and Margaret C. McKinnon. 2022. "A Pilot Study Assessing the Effects of Goal Management Training on Cognitive Functions among Individuals with Major Depressive Disorder and the Effect of Post-Traumatic Symptoms on Response to Intervention" Brain Sciences 12, no. 7: 864. https://doi.org/10.3390/brainsci12070864