
The Effect of Severity of Obstructive Sleep Apnea on Sleep Bruxism in Respiratory Polygraphy Study

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
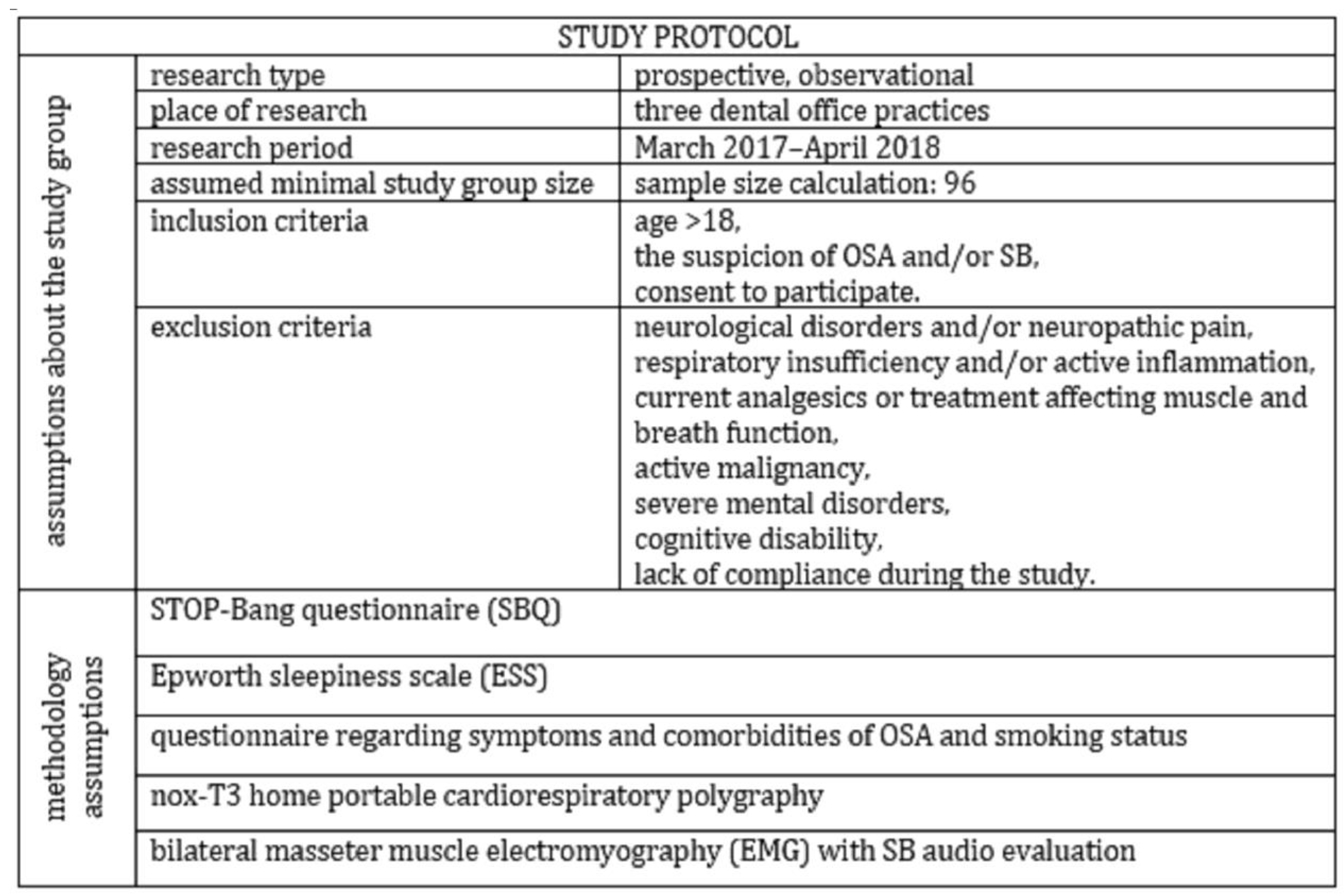
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Velly, A.M.; Nakane, T.; Masuda, Y.; Maki, S. Age is associated with self-reported sleep bruxism, independently of tooth loss. Sleep Breath 2012, 16, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Hollowell, D.E.; Bhandary, P.R.; Funsten, A.W.; Suratt, P.M. Respiratory related recruitment of the masseter: Response to hypercapnia and loading. J. Appl. Physiol. 1991, 70, 2508–2513. [Google Scholar] [CrossRef] [PubMed]
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.-L. Obstructive sleep apnea syndrome. Nat. Rev. Dis. Primers. 2015, 1, 15015. [Google Scholar] [CrossRef]
- Jokubauskas, L.; Baltrušaitytė, A. Relationship between obstructive sleep apnoea syndrome and sleep bruxism: A systematic review. J. Oral Rehabil. 2017, 44, 144–153. [Google Scholar] [CrossRef]
- Hosoya, H.; Kitaura, H.; Hashimoto, T.; Ito, M.; Kinbara, M.; Deguchi, T.; Irokawa, T.; Ohisa, N.; Ogawa, H.; Takano-Yamamoto, T. Relationship between sleep bruxism and sleep respiratory events in patients with obstructive sleep apnea syndrome. Sleep Breath 2014, 18, 837–844. [Google Scholar] [CrossRef]
- Saito, M.; Yamaguchi, T.; Mikami, S.; Watanabe, K.; Gotouda, A.; Okada, K.; Hishikawa, R.; Shibuya, E.; Shibuya, Y.; Lavigne, G. Weak association between sleep bruxism and obstructive sleep apnea. A sleep laboratory study. Sleep Breath 2016, 20, 703–709. [Google Scholar] [CrossRef]
- Sjöholm, T.T.; Lowe, A.A.; Miyamoto, K.; Fleetham, J.A.; Ryan, C.F. Sleep bruxism in patients with sleep-disordered breathing. Arch. Oral Biol. 2000, 45, 889–896. [Google Scholar] [CrossRef]
- Carra, M.C.; Rompre, P.H.; Kato, T.; Parrino, L.; Terzano, M.G.; Lavigne, G.J.; Macaluso, G.M. Sleep bruxism and sleep arousal: An experimental challenge to assess the role of cyclic alternating pattern. J. Oral Rehabil. 2011, 38, 635–642. [Google Scholar] [CrossRef]
- Sjöholm, T.; Polo, O.; Mäntyvaara, J.; Tanner, J.; Piha, J.; Lehtinen, I. Does sleep bruxism serve a physiological purpose? Electroencephalogr. Clin. Neurophysiol. 1996, 99, 24. [Google Scholar] [CrossRef]
- Tsujisakaa, A.; Harakia, S.; Nonouebd, S.; Mikamib, A.; Adachib, H.; Mizumoria, T.; Yatania, H.; Yoshidae, A.; Katobe, T. The occurrence of respiratory events in young subjects with a frequent rhythmic masticatory muscle activity: A pilot study. J. Prosthodont. Res. 2018, 62, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Bogunia-Kubik, K.; Mazur, G.; Danel, D.; Smardz, J.; Wojakowska, A.; Poreba, R.; Dratwa, M.; Chaszczewska-Markowska, M.; Winocur, E.; et al. Genetic basis of sleep bruxism and sleep apnea—Response to a medical puzzle. Sci. Rep. 2020, 10, 7497. [Google Scholar] [CrossRef]
- Hou, H.; Zhao, Y.; Yu, W.; Dong, H.; Xue, X.; Ding, J.; Xing, W.; Wang, W. Association of obstructive sleep apnea with hypertension: A systematic review and meta-analysis. J. Glob. Health. 2018, 8, 010405. [Google Scholar] [CrossRef] [PubMed]
- Munoz, R.; Duran-Cantolla, J.; Martinez-Vila, E.; Gallego, J.; Rubio, R.; Aizpuru, F.; De La Torre, G. Severe sleep apnea and risk of ischemic stroke in the elderly. Stroke 2006, 37, 2317–2321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasheghani-Farahani, A.; Kazemnejad, F.; Sadeghniiat-Haghighi, K.; Saadat, S.; Tavakolipoor, P.; Yazdani, T.; Alidoosti, M.; Ghasem-Amooeian, V.; Ashraf, H. Obstructive sleep apnea and severity of coronary artery disease. Caspian J. Intern. Med. 2018, 9, 276–282. [Google Scholar] [CrossRef]
- Mehra, R.; Benjamin, E.J.; Shahar, E.; Gottlieb, D.J.; Nawabit, R.; Kirchner, H.; Sahadevan, J.; Redline, S. Sleep Heart Health Study Association of nocturnal arrhythmias with sleep-disordered breathing: The Sleep Heart Health Study. Am. J. Respir Crit Care Med. 2006, 173, 910–916. [Google Scholar] [CrossRef] [Green Version]
- Young, T.; Finn, L.; Peppard, P.E. Sleep disordered breathing and mortality: Eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008, 31, 1071–1078. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Bader, G.; Lavigne, G. Sleep bruxism; an overview of an oromandibular sleep movement disorder. Sleep Med. Rev. 2000, 4, 27–43. [Google Scholar] [CrossRef]
- Martynowicz, H.; Gac, P.; Brzecka, A.; Poreba, R.; Wojakowska, A.; Mazur, G.; Smardz, J.; Wieckiewicz, M. The Relationship between Sleep Bruxism and Obstructive Sleep Apnea Based on Polysomnographic Findings. J. Clin. Med. 2019, 8, 1653. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M.; Türp, J.C. Risk factors for bruxism. Swiss. Dent. J. 2018, 128, 118–124. [Google Scholar] [PubMed]
- Ohayon, M.M.; Li, K.K.; Guilleminault, C. Risk factors for sleep bruxism in the general population. Chest 2001, 119, 53–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagappa, M.; Wong, J.; Singh, M.; Wong, D.T.; Chung, F. An update on the various practical applications of the STOP-Bang questionnaire in anesthesia, surgery, and perioperative medicine. Curr. Opin. Anaesthesiol. 2017, 30, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Winck, M.; Drummond, M.; Viana, P.; Pinho, J.C.; Winck, J.C. Sleep bruxism associated with obstructive sleep apnoea syndrome—A pilot study using a new portable device. Rev. Port. Pneumol. 2017, 23, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Martynowicz, H.; Dymczyk, P.; Dominiak, M.; Kazubowska, K.; Skomro, R.; Poreba, R.; Gac, P.; Wojakowska, A.; Mazur, G.; Wieckiewicz, M. Evaluation of Intensity of Sleep Bruxism in Arterial Hypertension. J. Clin. Med. 2018, 7, 327. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V.; American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; Version 2.4.; American Academy of Sleep Medicine: Darien, IL, USA, 2017. [Google Scholar]
- Manfredini, D.; Guarda-Nardini, L.; Marchese-Ragona, R.; Lobbezoo, F. Theories on possible temporal relationships between sleep bruxism and obstructive sleep apnea events. An expert opinion. Sleep Breath 2015, 19, 1459–1465. [Google Scholar] [CrossRef]
- Wieczorek, T.; Wieckiewicz, M.; Smardz, J.; Wojakowska, A.; Michalek-Zrabkowska, M.; Mazur, G.; Martynowicz, H. Sleep structure in sleep bruxism: A polysomnographic study including bruxism activity phenotypes across sleep stages. J. Sleep Res. 2020, 29, e13028. [Google Scholar] [CrossRef]
- Klasser, G.D.; Rei, N.; Lavigne, G.J. Sleep bruxism etiology: The evolution of a changing paradigm. J. Can. Dent. Assoc. 2015, 81, f2. [Google Scholar]
- Inana, R.; Benbir, G.; Karadeniz, D.; Yavlal, F.; Kiziltanb, M.E. Sleep bruxism is related to decreased inhibitory control of trigeminal motoneurons, but not with reticulobulbar system. Neurol. Sci. 2017, 38, 75–81. [Google Scholar] [CrossRef]
- Abe, Y.; Suganuma, T.; Ishii, M.; Yamamoto, G.; Gunji, T.; Clark, G.T.; Tachikawa, T.; Kiuchi, Y.; Igarashi, Y.; Baba, K. Association of genetic, psychological and behavioral factors with sleep bruxism in a Japanese population. J. Sleep Res. 2012, 21, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.; Manzini, C.; Huynh, N.T. Sleep bruxism. In Principles and Practice of Sleep Medicine, 5th ed.; Kryger, M.H., Roth, T., Dement, W.C., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2011; pp. 1128–1139. [Google Scholar]
- Postrzech-Adamczyk, K.; Nahorecki, A.; Zatońska, K.; Lawson, J.; Wołyniec, M.; Skomro, R.; Szuba, A. Prevalence and Risk of Obstructive Sleep Apnea and Arterial Hypertension in the Adult Population in Poland: An Observational Subset of the International Prospective Urban Rural Epidemiology (PURE) Study. Adv. Exp. Med. Biol. 2019, 1222, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Câmara-Souza, M.B.; de Figueredo, O.M.C.; Rodrigues Garcia, R.C.M. Association of sleep bruxism with oral health-related quality of life and sleep quality. Clin. Oral Investig. 2018, 23, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Neu, D.; Baniasadi, N.; Newell, J.; Styczen, D.; Glineur, R.; Mairesse, O. Effect of sleep bruxism duration on perceived sleep quality in middle-aged subjects. Eur. J. Oral Sci. 2018, 126, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Stansbury, R.C.; Strollo, P.J. Clinical manifestations of sleep apnea. J. Thorac. Dis. 2015, 7, E298–E310. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Studied Group (n = 119) | SBQ ≥ 3 (n = 52) | SBQ < 3 (n = 52) | p |
|---|---|---|---|---|
| BEI (n/hour) | 2.80 ± 3.08 | 3.39 ± 3.63 | 2.27 ± 2.50 | 0.03 * |
| Phasic (n/hour) | 1.00 ± 1.54 | 1.30 ± 1.76 | 0.77 ± 1.33 | 0.07 |
| Tonic (n/hour) | 0.92 ± 1.08 | 1.12 ± 1.38 | 0.76 ± 0.77 | 0.08 |
| Mixed (n/hour) | 0.89 ± 1.18 | 1.07 ± 1.40 | 0.74 ± 0.98 | 0.14 * |
| AHI (n/hour) | 12.16 ± 13.90 | 21.19 ± 16.05 | 5.19 ± 5.74 | 0.00 ** |
| ODI (n/hour) | 12.53 ± 13.39 | 21.40 ± 15.26 | 5.71 ± 5.61 | 0.00 ** |
| Snore (%) | 10.21 ± 15.13 | 16.43 ± 17.80 | 5.48 ± 10.64 | 0.00 ** |
| OA (n/hour) | 4.16 ± 8.10 | 8.15 ± 10.77 | 1.07 ± 2.36 | 0.00 ** |
| MA (n/hour) | 0.24 ± 0.82 | 0.52 ± 1.19 | 0.03 ± 0.08 | 0.00 ** |
| CA (n/hour) | 0.73 ± 1.23 | 0.99 ± 1.58 | 0.50 ± 0.83 | 0.03 * |
| Hypopnea (n/hour) | 7.04 ± 6.77 | 11.52 ± 7.18 | 3.61 ± 3.80 | 0.00 ** |
| Cheyne–Stokes (%) | 0.21 ± 1.55 | 0.48 ± 2.34 | 0.00 ± 0.00 | 0.10 |
| Mean SpO2 (%) | 93.70 ± 1.84 | 92.71 ± 1.73 | 94.48 ± 1.53 | 0.00 ** |
| Min SO2 (%) | 85.61 ± 5.36 | 82.87 ± 5.05 | 87.68 ± 4.65 | 0.00 ** |
| SpO2 < 90% (%) | 5.47 ± 13.24 | 9.86 ± 17.44 | 2.11 ± 7.27 | 0.00 * |
| Mean oxygen desaturation (%) | 4.09 ± 1.29 | 4.65 ± 1.49 | 3.64 ± 0.91 | 0.00 * |
| Mean heart rate (beats/minute) | 62.26 ± 7.48 | 63.01 ± 8.01 | 61.93 ± 6.88 | 0.43 |
| Max heart rate (beats/minute) | 97.48 ± 16.30 | 93.58 ± 10.56 | 100.72 ± 19.43 | 0.02 * |
| Min heart rate (beats/minute) | 48.52 ± 7.17 | 48.48 ± 8.00 | 48.78 ± 6.47 | 0.77 |
| Parameter | % | n | |
|---|---|---|---|
| AHI (n/hour) | <5 | 36.97 | 44 |
| ≥5 < 15 | 37.81 | 45 | |
| ≥15 < 30 | 11.76 | 14 | |
| ≥30 | 12.60 | 15 | |
| BEI (n/hour) | <2 | 58.82 | 70 |
| ≥2 < 4 | 18.48 | 22 | |
| ≥4 | 27.73 | 33 | |
| Group | AHI < 5 | AHI <23 | AHI > 23 |
|---|---|---|---|
| Parameters | BEI (n/hour) | ||
| AHI (n/hour) | 0.10 | 0.22 * | 0.05 |
| ODI (n/hour) | −0.07 | 0.19 | 0.06 |
| Snore (%) | −0.07 | 0.01 | 0.48 * |
| OA (n/hour) | 0.42 * | 0.18 | 0.03 |
| MA (n/hour) | 0.00 | 0.20 * | −0.05 |
| CA (n/hour) | 0.10 | 0.14 | 0.06 |
| Hypopnea (n/hour) | −0.10 | 0.17 | 0.04 |
| Mean SpO2 (%) | 0.33 * | −0.07 | 0.08 |
| Min SpO2 (%) | 0.35 * | −0.12 | 0.10 |
| SpO2 < 90% (%) | 0.15 | 0.30 * | −0.07 |
| Mean oxygen desaturation (%) | −0.10 | 0.09 | −0.02 |
| Mean heart rate (beats/minute) | −0.06 | 0.05 | −0.06 |
| Max heart rate (beats/minute) | −0.08 | 0.02 | −0.00 |
| Min heart rate (beats/minute) | −0.23 | −0.24 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazubowska-Machnowska, K.; Jodkowska, A.; Michalek-Zrabkowska, M.; Wieckiewicz, M.; Poreba, R.; Dominiak, M.; Gac, P.; Mazur, G.; Kanclerska, J.; Martynowicz, H. The Effect of Severity of Obstructive Sleep Apnea on Sleep Bruxism in Respiratory Polygraphy Study. Brain Sci. 2022, 12, 828. https://doi.org/10.3390/brainsci12070828
Kazubowska-Machnowska K, Jodkowska A, Michalek-Zrabkowska M, Wieckiewicz M, Poreba R, Dominiak M, Gac P, Mazur G, Kanclerska J, Martynowicz H. The Effect of Severity of Obstructive Sleep Apnea on Sleep Bruxism in Respiratory Polygraphy Study. Brain Sciences. 2022; 12(7):828. https://doi.org/10.3390/brainsci12070828
Chicago/Turabian StyleKazubowska-Machnowska, Klaudia, Anna Jodkowska, Monika Michalek-Zrabkowska, Mieszko Wieckiewicz, Rafal Poreba, Marzena Dominiak, Pawel Gac, Grzegorz Mazur, Justyna Kanclerska, and Helena Martynowicz. 2022. "The Effect of Severity of Obstructive Sleep Apnea on Sleep Bruxism in Respiratory Polygraphy Study" Brain Sciences 12, no. 7: 828. https://doi.org/10.3390/brainsci12070828