
Brain Connectivity and Graph Theory Analysis in Alzheimer’s and Parkinson’s Disease: The Contribution of Electrophysiological Techniques

 , and
, and
Abstract
:1. Introduction
2. Alzheimer’s Disease and Graph Theory
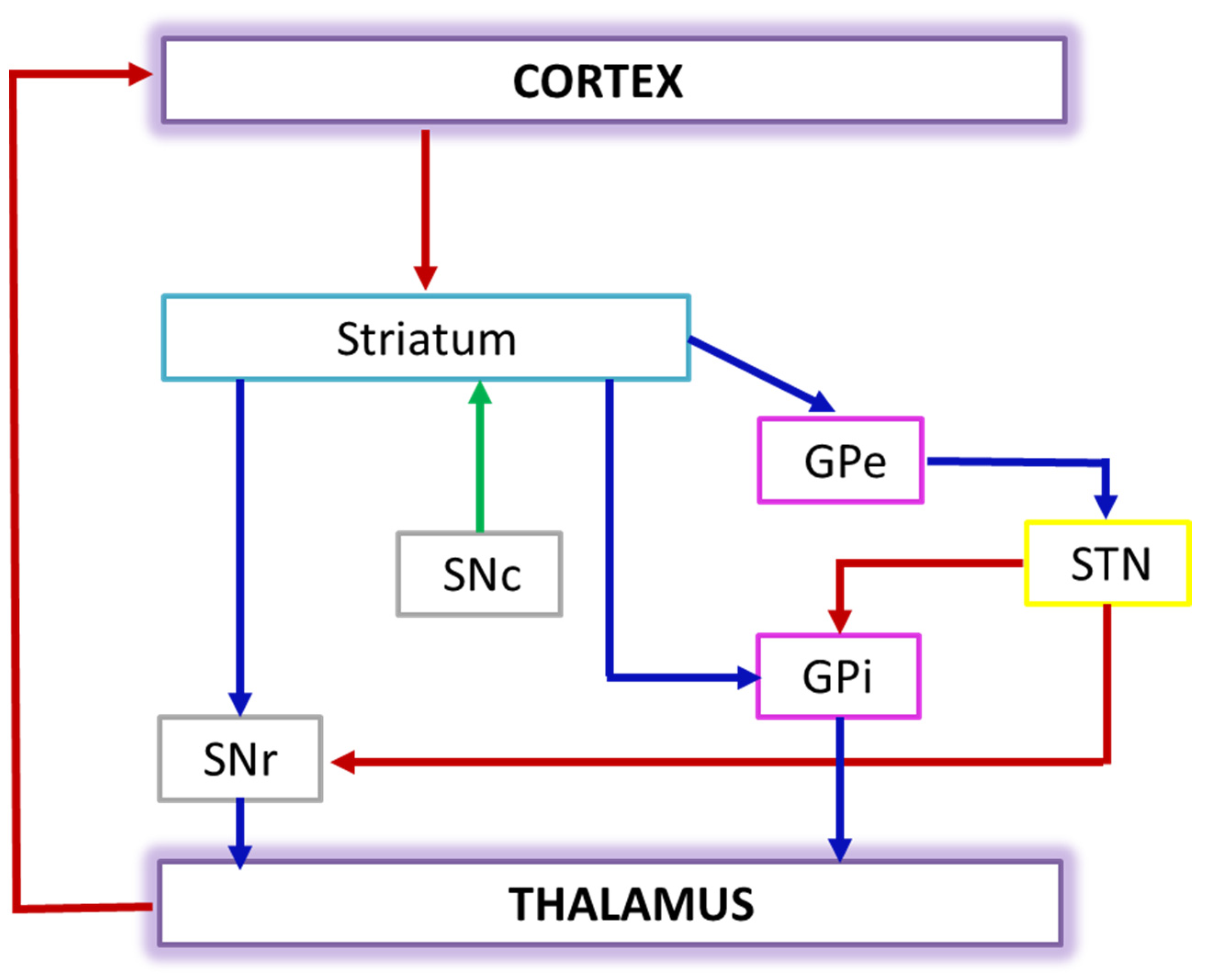
3. Parkinson’s Disease and Graph Theory
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sporns, O.; Chialvo, D.R.; Kaiser, M.; Hilgetag, C.C. Organization, development and function of complex brain networks. Trends Cogn. Sci. 2004, 8, 418–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sporns, O. The human connectome: A complex network. Ann. N. Y. Acad. Sci. 2011, 1224, 109–125. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Ferilli, M.A.; Rossini, L.; Ferreri, F. Clinical neurophysiology of brain plasticity in aging brain. Curr. Pharm. Des. 2013, 19, 6426–6439. [Google Scholar] [CrossRef]
- Sporns, O.; Tononi, G.; Kötter, R. The human connectome: A structural description of the human brain. PLoS Comput. Biol. 2005, 1, e42. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Di Iorio, R.; Bentivoglio, M.; Bertini, G.; Ferreri, F.; Gerloff, C.; Ilmoniemi, R.J.; Miraglia, F.; Nitsche, M.A.; Pestilli, F.; et al. Methods for analysis of brain connectivity: An IFCN-sponsored review. Clin. Neurophysiol. 2019, 130, 1833–1858. [Google Scholar] [CrossRef]
- Tononi, G.; Sporns, O.; Edelman, G.M. A measure for brain complexity: Relating functional segregation and integration in the nervous system. Proc. Natl. Acad. Sci. USA 1994, 91, 5033–5037. [Google Scholar] [CrossRef] [Green Version]
- Arendt, T. Synaptic degeneration in Alzheimer’s disease. Acta Neuropathol. 2009, 118, 167–179. [Google Scholar] [CrossRef]
- Blennow, K.; Cowburn, R.F. The neurochemistry of Alzheimer’s disease. Acta Neurol. Scand. Suppl. 1996, 168, 77–86. [Google Scholar] [CrossRef]
- Delbeuck, X.; Van der Linden, M.; Collette, F. Alzheimer’s disease as a disconnection syndrome? Neuropsychol. Rev. 2003, 13, 79–92. [Google Scholar] [CrossRef]
- Rossini, P.M.; Di Iorio, R.; Vecchio, F.; Anfossi, M.; Babiloni, C.; Bozzali, M.; Bruni, A.C.; Cappa, S.F.; Escudero, J.; Fraga, F.J.; et al. Early diagnosis of Alzheimer’s disease: The role of biomarkers including advanced EEG signal analysis. Report from the IFCN-sponsored panel of experts. Clin. Neurophysiol. 2020, 131, 1287–1310. [Google Scholar] [CrossRef]
- Rossini, P.M. Aging and brain connectivity via electroencephalographic recordings. Neuroscience 2019, 422, 228–229. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.H.; Capetillo-Zarate, E.; Lin, M.T.; Milner, T.A.; Gouras, G.K. Co-occurrence of Alzheimer’s disease ß-amyloid and τ pathologies at synapses. Neurobiol. Aging 2010, 31, 1145–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoffers, D.; Bosboom, J.L.; Deijen, J.B.; Wolters, E.C.h.; Stam, C.J.; Berendse, H.W. Increased cortico-cortical functional connectivity in early-stage Parkinson’s disease: An MEG study. Neuroimage 2008, 41, 212–222. [Google Scholar] [CrossRef]
- Tessitore, A.; Esposito, F.; Vitale, C.; Santangelo, G.; Amboni, M.; Russo, A.; Corbo, D.; Cirillo, G.; Barone, P.; Tedeschi, G. Default-mode network connectivity in cognitively unimpaired patients with Parkinson disease. Neurology 2012, 79, 2226–2232. [Google Scholar] [CrossRef] [PubMed]
- Ponsen, M.M.; Stam, C.J.; Bosboom, J.L.; Berendse, H.W.; Hillebrand, A. A three dimensional anatomical view of oscillatory resting-state activity and functional connectivity in Parkinson’s disease related dementia: An MEG study using atlas-based beamforming. Neuroimage Clin. 2012, 2, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Chaudhuri, K.R.; Healy, D.G.; Schapira, A.H.; Excellence, N.I.f.C. Non-motor symptoms of Parkinson’s disease: Diagnosis and management. Lancet Neurol. 2006, 5, 235–245. [Google Scholar] [CrossRef]
- Sporns, O. Graph theory methods: Applications in brain networks. Dialogues Clin. Neurosci. 2018, 20, 111–121. [Google Scholar]
- Friston, K.J.; Tononi, G.; Reeke, G.N.; Sporns, O.; Edelman, G.M. Value-dependent selection in the brain: Simulation in a synthetic neural model. Neuroscience 1994, 59, 229–243. [Google Scholar] [CrossRef]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Li, Z.; Liu, C.; Wang, Q.; Liang, K.; Han, C.; Qiao, H.; Zhang, J.; Meng, F. Abnormal Functional Brain Network in Parkinson’s Disease and the Effect of Acute Deep Brain Stimulation. Front. Neurol. 2021, 12, 715455. [Google Scholar] [CrossRef]
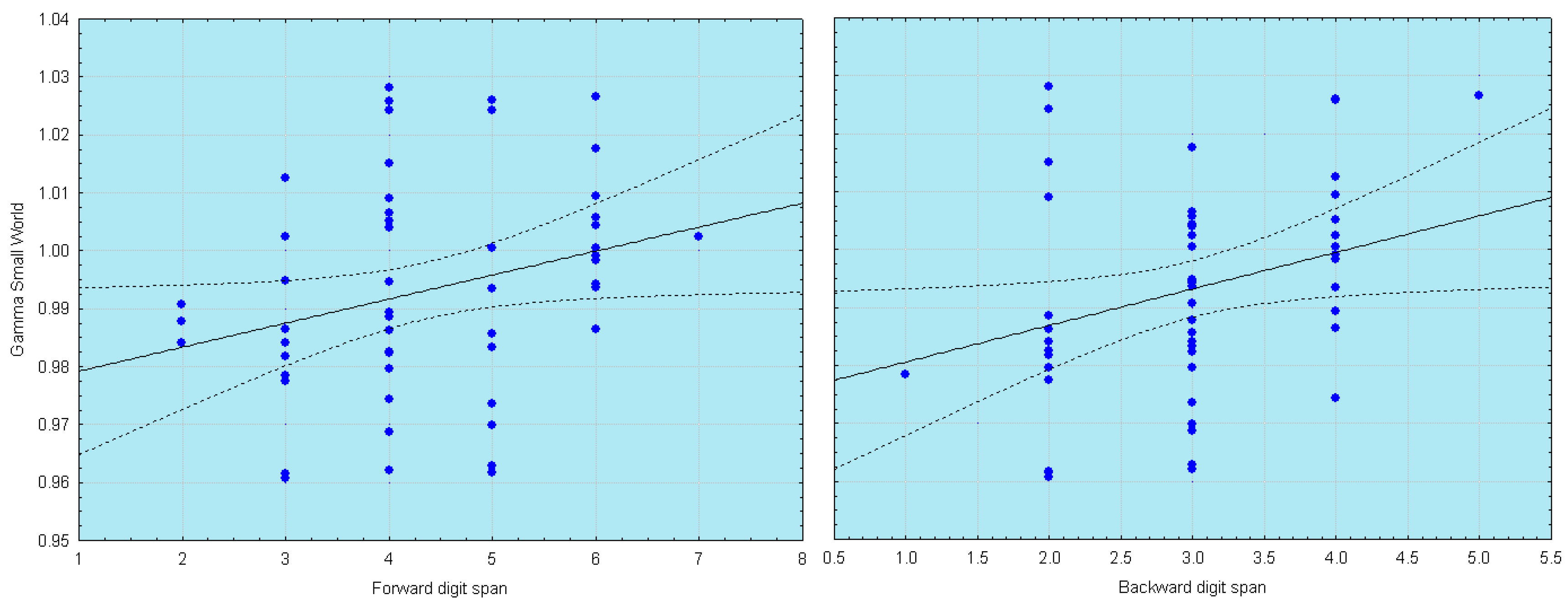
- Vecchio, F.; Pappalettera, C.; Miraglia, F.; Alù, F.; Orticoni, A.; Judica, E.; Cotelli, M.; Pistoia, F.; Rossini, P.M. Graph Theory on Brain Cortical Sources in Parkinson’s Disease: The Analysis of ‘Small World’ Organization from EEG. Sensors 2021, 21, 7266. [Google Scholar] [CrossRef] [PubMed]
- Utianski, R.L.; Caviness, J.N.; van Straaten, E.C.; Beach, T.G.; Dugger, B.N.; Shill, H.A.; Driver-Dunckley, E.D.; Sabbagh, M.N.; Mehta, S.; Adler, C.H.; et al. Graph theory network function in Parkinson’s disease assessed with electroencephalography. Clin. Neurophysiol. 2016, 127, 2228–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revankar, G.S.; Kajiyama, Y.; Hattori, N.; Shimokawa, T.; Nakano, T.; Mihara, M.; Mori, E.; Mochizuki, H. Prestimulus Low-Alpha Frontal Networks Are Associated with Pareidolias in Parkinson’s Disease. Brain Connect. 2021, 11, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Afshari, S.; Jalili, M. Directed Functional Networks in Alzheimer’s Disease: Disruption of Global and Local Connectivity Measures. IEEE J. Biomed. Health Inform. 2017, 21, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Wang, J.; Yu, H.; Wei, X.; Yang, C.; Deng, B. Decreased coherence and functional connectivity of electroencephalograph in Alzheimer’s disease. Chaos 2014, 24, 033136. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Chaton, L.; Benquet, P.; Delval, A.; Leroy, C.; Plomhause, L.; Moonen, A.J.; Duits, A.A.; Leentjens, A.F.; van Kranen-Mastenbroek, V.; et al. Functional connectivity disruptions correlate with cognitive phenotypes in Parkinson’s disease. Neuroimage Clin. 2017, 14, 591–601. [Google Scholar] [CrossRef]
- Franciotti, R.; Falasca, N.W.; Arnaldi, D.; Famà, F.; Babiloni, C.; Onofrj, M.; Nobili, F.M.; Bonanni, L. Cortical Network Topology in Prodromal and Mild Dementia Due to Alzheimer’s Disease: Graph Theory Applied to Resting State EEG. Brain Topogr. 2019, 32, 127–141. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Stam, C.J.; Reijneveld, J.C. Graph theoretical analysis of complex networks in the brain. Nonlinear Biomed. Phys. 2007, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Xie, T.; He, Y. Mapping the Alzheimer’s brain with connectomics. Front. Psychiatry 2011, 2, 77. [Google Scholar] [CrossRef] [Green Version]
- Tijms, B.M.; Wink, A.M.; de Haan, W.; van der Flier, W.M.; Stam, C.J.; Scheltens, P.; Barkhof, F. Alzheimer’s disease: Connecting findings from graph theoretical studies of brain networks. Neurobiol. Aging 2013, 34, 2023–2036. [Google Scholar] [CrossRef] [PubMed]
- Minati, L.; Varotto, G.; D’Incerti, L.; Panzica, F.; Chan, D. From brain topography to brain topology: Relevance of graph theory to functional neuroscience. Neuroreport 2013, 24, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, F.; Vecchio, F.; Rossini, P.M. Searching for signs of aging and dementia in EEG through network analysis. Behav. Brain Res. 2017, 317, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, F.; Miraglia, F.; Maria Rossini, P. Connectome: Graph theory application in functional brain network architecture. Clin. Neurophysiol. Pract. 2017, 2, 206–213. [Google Scholar] [CrossRef]
- delEtoile, J.; Adeli, H. Graph Theory and Brain Connectivity in Alzheimer’s Disease. Neuroscientist 2017, 23, 616–626. [Google Scholar] [CrossRef]
- Rossini, P.; Miraglia, F.; Alù, F.; Cotelli, M.; Ferreri, F.; Di Iorio, R.; Iodice, F.; Vecchio, F. Neurophysiological Hallmarks of Neurodegenerative Cognitive Decline: The Study of Brain Connectivity as A Biomarker of Early Dementia. J. Pers. Med. 2020, 10, 34. [Google Scholar] [CrossRef]
- Hallett, M.; de Haan, W.; Deco, G.; Dengler, R.; Di Iorio, R.; Gallea, C.; Gerloff, C.; Grefkes, C.; Helmich, R.C.; Kringelbach, M.L.; et al. Human brain connectivity: Clinical applications for clinical neurophysiology. Clin. Neurophysiol. 2020, 131, 1621–1651. [Google Scholar] [CrossRef]
- de Haan, W.; Pijnenburg, Y.A.; Strijers, R.L.; van der Made, Y.; van der Flier, W.M.; Scheltens, P.; Stam, C.J. Functional neural network analysis in frontotemporal dementia and Alzheimer’s disease using EEG and graph theory. BMC Neurosci. 2009, 10, 101. [Google Scholar] [CrossRef] [Green Version]
- Stam, C.J.; de Haan, W.; Daffertshofer, A.; Jones, B.F.; Manshanden, I.; van Cappellen van Walsum, A.M.; Montez, T.; Verbunt, J.P.; de Munck, J.C.; van Dijk, B.W.; et al. Graph theoretical analysis of magnetoencephalographic functional connectivity in Alzheimer’s disease. Brain 2009, 132, 213–224. [Google Scholar] [CrossRef]
- Vecchio, F.; Miraglia, F.; Marra, C.; Quaranta, D.; Vita, M.G.; Bramanti, P.; Rossini, P.M. Human brain networks in cognitive decline: A graph theoretical analysis of cortical connectivity from EEG data. J. Alzheimers Dis. 2014, 41, 113–127. [Google Scholar] [CrossRef]
- Poza, J.; Garcia, M.; Gomez, C.; Bachiller, A.; Carreres, A.; Hornero, R. Characterization of the spontaneous electroencephalographic activity in Alzheimer’s disease using disequilibria and graph theory. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2013, 2013, 5990–5993. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, F.; Miraglia, F.; Quaranta, D.; Granata, G.; Romanello, R.; Marra, C.; Bramanti, P.; Rossini, P.M. Cortical connectivity and memory performance in cognitive decline: A study via graph theory from EEG data. Neuroscience 2016, 316, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, F.; Miraglia, F.; Piludu, F.; Granata, G.; Romanello, R.; Caulo, M.; Onofrj, V.; Bramanti, P.; Colosimo, C.; Rossini, P.M. “Small World” architecture in brain connectivity and hippocampal volume in Alzheimer’s disease: A study via graph theory from EEG data. Brain Imaging Behav. 2017, 11, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Frantzidis, C.A.; Vivas, A.B.; Tsolaki, A.; Klados, M.A.; Tsolaki, M.; Bamidis, P.D. Functional disorganization of small-world brain networks in mild Alzheimer’s Disease and amnestic Mild Cognitive Impairment: An EEG study using Relative Wavelet Entropy (RWE). Front. Aging Neurosci. 2014, 6, 224. [Google Scholar] [CrossRef] [Green Version]
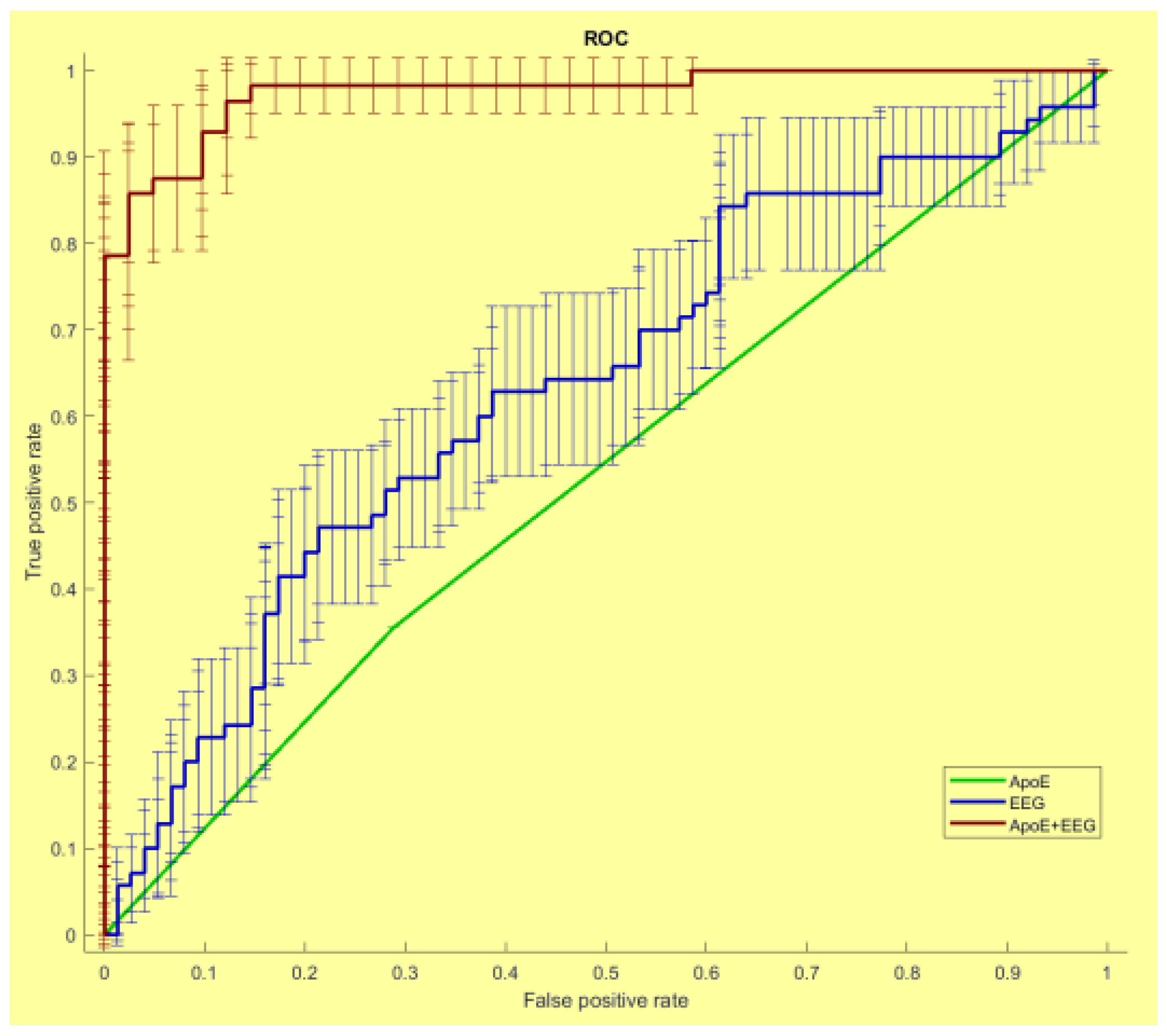
- Vecchio, F.; Miraglia, F.; Iberite, F.; Lacidogna, G.; Guglielmi, V.; Marra, C.; Pasqualetti, P.; Tiziano, F.D.; Rossini, P.M. Sustainable method for Alzheimer dementia prediction in mild cognitive impairment: Electroencephalographic connectivity and graph theory combined with apolipoprotein E. Ann. Neurol. 2018, 84, 302–314. [Google Scholar] [CrossRef]
- Miraglia, F.; Vecchio, F.; Marra, C.; Quaranta, D.; Alù, F.; Peroni, B.; Granata, G.; Judica, E.; Cotelli, M.; Rossini, P.M. Small World Index in Default Mode Network Predicts Progression from Mild Cognitive Impairment to Dementia. Int. J. Neural. Syst. 2020, 30, 2050004. [Google Scholar] [CrossRef]
- Cecchetti, G.; Agosta, F.; Basaia, S.; Cividini, C.; Cursi, M.; Santangelo, R.; Caso, F.; Minicucci, F.; Magnani, G.; Filippi, M. Resting-state electroencephalographic biomarkers of Alzheimer’s disease. Neuroimage Clin. 2021, 31, 102711. [Google Scholar] [CrossRef]
- Vecchio, F.; Miraglia, F.; Gorgoni, M.; Ferrara, M.; Iberite, F.; Bramanti, P.; De Gennaro, L.; Rossini, P.M. Cortical connectivity modulation during sleep onset: A study via graph theory on EEG data. Hum. Brain Mapp. 2017, 38, 5456–5464. [Google Scholar] [CrossRef] [Green Version]
- Abazid, M.; Houmani, N.; Boudy, J.; Dorizzi, B.; Mariani, J.; Kinugawa, K. A Comparative Study of Functional Connectivity Measures for Brain Network Analysis in the Context of AD Detection with EEG. Entropy 2021, 23, 1553. [Google Scholar] [CrossRef]
- Kocagoncu, E.; Quinn, A.; Firouzian, A.; Cooper, E.; Greve, A.; Gunn, R.; Green, G.; Woolrich, M.W.; Henson, R.N.; Lovestone, S.; et al. Tau pathology in early Alzheimer’s disease is linked to selective disruptions in neurophysiological network dynamics. Neurobiol. Aging 2020, 92, 141–152. [Google Scholar] [CrossRef]
- Tait, L.; Stothart, G.; Coulthard, E.; Brown, J.T.; Kazanina, N.; Goodfellow, M. Network substrates of cognitive impairment in Alzheimer’s Disease. Clin. Neurophysiol. 2019, 130, 1581–1595. [Google Scholar] [CrossRef]
- Vecchio, F.; Quaranta, D.; Miraglia, F.; Pappalettera, C.; Di Iorio, R.; L’Abbate, F.; Cotelli, M.; Marra, C.; Rossini, P.M. Neuronavigated Magnetic Stimulation combined with cognitive training for Alzheimer’s patients: An EEG graph study. Geroscience 2021, 44, 159–172. [Google Scholar] [CrossRef]
- Vecchio, F.; Miraglia, F.; Alú, F.; Orticoni, A.; Judica, E.; Cotelli, M.; Rossini, P.M. Contribution of Graph Theory Applied to EEG Data Analysis for Alzheimer’s Disease versus Vascular Dementia Diagnosis. J. Alzheimers Dis. 2021, 82, 871–879. [Google Scholar] [CrossRef]
- Li, R.; Nguyen, T.; Potter, T.; Zhang, Y. Dynamic cortical connectivity alterations associated with Alzheimer’s disease: An EEG and fNIRS integration study. Neuroimage Clin. 2019, 21, 101622. [Google Scholar] [CrossRef]
- Vecchio, F.; Miraglia, F.; Alù, F.; Menna, M.; Judica, E.; Cotelli, M.; Rossini, P.M. Classification of Alzheimer’s Disease with Innovative EEG Biomarkers in a Machine Learning Implementation. J. Alzheimers Dis. 2020, 75, 1253–1261. [Google Scholar] [CrossRef]
- Bočková, M.; Rektor, I. Impairment of brain functions in Parkinson’s disease reflected by alterations in neural connectivity in EEG studies: A viewpoint. Clin. Neurophysiol. 2019, 130, 239–247. [Google Scholar] [CrossRef]
- Olde Dubbelink, K.T.; Hillebrand, A.; Stoffers, D.; Deijen, J.B.; Twisk, J.W.; Stam, C.J.; Berendse, H.W. Disrupted brain network topology in Parkinson’s disease: A longitudinal magnetoencephalography study. Brain 2014, 137, 197–207. [Google Scholar] [CrossRef] [Green Version]
- Peláez Suárez, A.A.; Berrillo Batista, S.; Pedroso Ibáñez, I.; Casabona Fernández, E.; Fuentes Campos, M.; Chacón, L.M. EEG-Derived Functional Connectivity Patterns Associated with Mild Cognitive Impairment in Parkinson’s Disease. Behav. Sci. 2021, 11, 40. [Google Scholar] [CrossRef]
- Mehraram, R.; Kaiser, M.; Cromarty, R.; Graziadio, S.; O’Brien, J.T.; Killen, A.; Taylor, J.P.; Peraza, L.R. Weighted network measures reveal differences between dementia types: An EEG study. Hum. Brain Mapp. 2020, 41, 1573–1590. [Google Scholar] [CrossRef] [Green Version]
- Fogelson, N.; Li, L.; Li, Y.; Fernandez-Del-Olmo, M.; Santos-Garcia, D.; Peled, A. Functional connectivity abnormalities during contextual processing in schizophrenia and in Parkinson’s disease. Brain Cogn. 2013, 82, 243–253. [Google Scholar] [CrossRef]
- Bočková, M.; Výtvarová, E.; Lamoš, M.; Klimeš, P.; Jurák, P.; Halámek, J.; Goldemundová, S.; Baláž, M.; Rektor, I. Cortical network organization reflects clinical response to subthalamic nucleus deep brain stimulation in Parkinson’s disease. Hum. Brain Mapp. 2021, 42, 5626–5635. [Google Scholar] [CrossRef]
- Smith, S.M.; Miller, K.L.; Salimi-Khorshidi, G.; Webster, M.; Beckmann, C.F.; Nichols, T.E.; Ramsey, J.D.; Woolrich, M.W. Network modelling methods for FMRI. Neuroimage 2011, 54, 875–891. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Description |
|---|---|
| Clustering Coefficient, C | The number of connections that exist between the nearest neighbors of a node as a proportion of maximum number of possible connections. It reflects the tendency of a network to form topologically organized circuits and it is often interpreted as a metric of information segregation in networks [20]. |
| Path Length, PL | The minimum number of edges that must be traversed to go from one node to another. It is used as a measure of global integration of the network [20]. |
| Small-world, SW | The ratio of the normalized clustering coefficient and normalized path length. It describes a balance between segregation and integration network properties integrating the information of global and local network characteristics [21]. |
| Divergence | Measure of the broadness of the weighted degree distribution, where weighted degree is the summed weights of all edges connected to a node [22]. |
| Modularity | Ratio of the intra- and intermodular connectivity strength where modules are subgraphs containing nodes that are more strongly connected to themselves than to other nodes. Modularity is a measure of the strength of the modules [22]. |
| Efficiency | The ability of information exchange within the network [23]. |
| Global efficiency | Measure of network integration and its overall performance for information transferring. This measure is inversely related to the average shortest path length [24]. |
| Local efficiency | Local efficiency, which has a similar interpretation as clustering coefficient, measures the compactness of the subnetwork [25]. |
| Centrality | The importance of a node and its direct impact on adjacent brain areas [23]. |
| Betweenness | Used to investigate the contribution of each node to all other node pairs on the shortest path. It measures not only the importance of the nodes, but also the amount of information flowing through the node [25]. |
| Strength | The sum of weights of connections (edges) of node. The strength can be averaged over the whole network to obtain a global measure of connection weights [26]. |
| Degree | The degree of a node is the sum of its incoming (afferent) and outgoing (efferent) edges [27]. |
| In-degree | Number of afferent connections to the node [27]. |
| Out-degree | Number of efferent connections to the node [27]. |
| Assortativity coefficient | The assortativity coefficient represents a measure of a network’s resilience. It is a correlation coefficient between the degrees of all vertices on two opposite ends of an edge [27]. |
| Authors | Recording Type | Graph Parameters | Main Results (All Results Refer to AD vs. Healthy) |
|---|---|---|---|
| Stam et al., 2007 [29] | EEG | PL C |
|
| Stam et al., 2009 [39] | MEG | PL C |
|
| de Haan et al., 2009 [38] | EEG | PL C |
|
| Poza et al., 2013 [41] | EEG | PL C |
|
| Wang et al., 2014 [25] | EEG | PL C Global Efficiency Local Efficiency SW |
|
| Vecchio et al., 2014 [40] | EEG | PL C |
|
| Frantzidis et al., 2014 [44] | EEG | SW |
-SW ↓ MMSE ↓; SW ↓ MoCA ↓ |
| Vecchio et al., 2016 [42] | EEG | SW | Pearson’s correlation:
|
| Miraglia et al., 2017 [33] | EEG | SW |
|
| Vecchio et al., 2017 [34] | EEG | SW | Pearson’s correlations:
|
| Saeedeh Afshari and Mahdi Jalili, 2017 [24] | EEG | Global efficiency Local efficiency |
|
| Vecchio et al., 2018 [45] | EEG | SW |
|
| Franciotti et al., 2019 [27] | EEG | Degree In-degree Out-degree Assortative Coefficient |
|
| Li et al., 2019 [54] | EEG | Degree C Centrality |
|
| Vecchio et al., 2020 [55] | EEG | SW |
|
| Miraglia et al., 2020 [46] | EEG | SW |
|
| Cecchetti et al., 2021 [47] | EEG | PL C |
|
| Majd Abazid et al., 2021 [49] | EEG | PL C Degree Efficiency Betweenness |
|
| Kocagoncu 2020 [50] | E/MEG | SW | Pearson’s correlation:
|
| Tait et al., 2019 [51] | EEG | SW | Pearson’s correlation:
|
| Vecchio et al., 2021 [52] | EEG | SW | Pearson’s correlations:
|
| Vecchio et al., 2021 [53] | EEG | SW |
|
| Authors | Recording Type | Graph Parameters | Main Results |
|---|---|---|---|
| Fogelson et al., 2013 [60] | EEG | C PL |
|
| Olde Dubbelink et al., 2014 [57] | MEG | C PL |
|
| Utianski et al., 2016 [22] | EEG | C PL Divergence Modularity |
|
| Hassan et al., 2017 [26] | EEG | C PL Modularity Strength |
|
| Mehraram et al., 2020 [59] | EEG | Node degree C PL SW Modularity |
|
| Bočková et al., 2021 [61] | EEG | Node strength C PL Modularity |
|
| Suárez et al., 2021 [58] | EEG | C PL Local efficiency Global connectivity |
|
| Vecchio et al., 2021 [21] | EEG | SW |
|
| Li et al., 2021 [20] | EEG | C PL Global efficiency Local efficiency |
|
| Revankar et al., 2021 [23] | EEG | C PL Efficiency Centrality |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miraglia, F.; Vecchio, F.; Pappalettera, C.; Nucci, L.; Cotelli, M.; Judica, E.; Ferreri, F.; Rossini, P.M. Brain Connectivity and Graph Theory Analysis in Alzheimer’s and Parkinson’s Disease: The Contribution of Electrophysiological Techniques. Brain Sci. 2022, 12, 402. https://doi.org/10.3390/brainsci12030402
Miraglia F, Vecchio F, Pappalettera C, Nucci L, Cotelli M, Judica E, Ferreri F, Rossini PM. Brain Connectivity and Graph Theory Analysis in Alzheimer’s and Parkinson’s Disease: The Contribution of Electrophysiological Techniques. Brain Sciences. 2022; 12(3):402. https://doi.org/10.3390/brainsci12030402
Chicago/Turabian StyleMiraglia, Francesca, Fabrizio Vecchio, Chiara Pappalettera, Lorenzo Nucci, Maria Cotelli, Elda Judica, Florinda Ferreri, and Paolo Maria Rossini. 2022. "Brain Connectivity and Graph Theory Analysis in Alzheimer’s and Parkinson’s Disease: The Contribution of Electrophysiological Techniques" Brain Sciences 12, no. 3: 402. https://doi.org/10.3390/brainsci12030402