
Effect of Dual-Task Motor-Cognitive Training in Preventing Falls in Vulnerable Elderly Cerebrovascular Patients: A Pilot Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Mixed Motor and Cognitive Training (MixT)
2.3. Motor-Cognitive Dual-Task Training (DTT)

{kind=link}
{kind=link}
{kind=link}
| MixT | DTT | |
|---|---|---|
| Training | Motor training (1) + cognitive training (2) | Motor-cognitive dual-task training (1) |
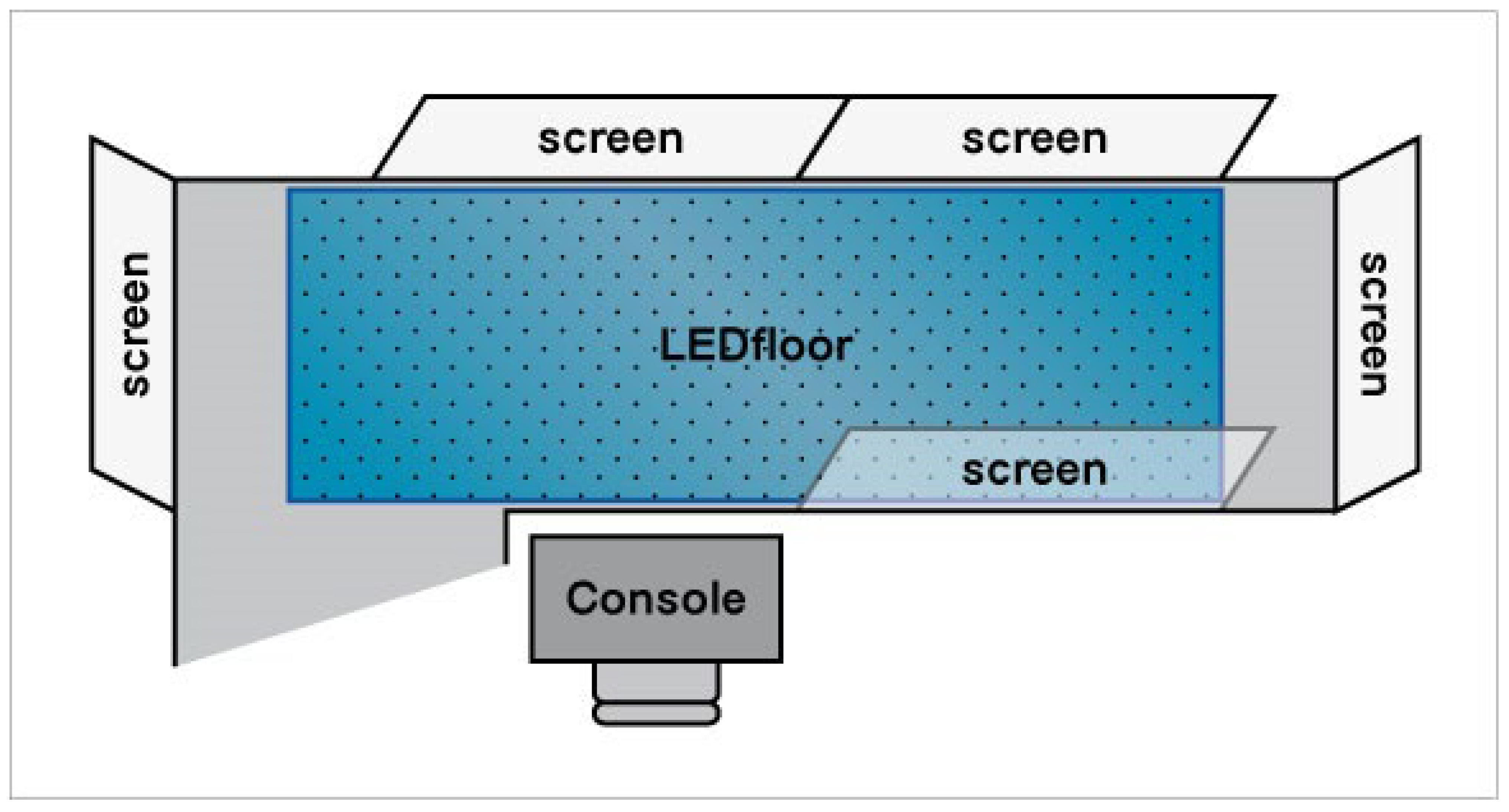
| Materials | (1) an empty room (2) a computerized touch-screen platform | (1) a dual-task room: three sensory carpets (2 m) (medium density smooth, sandy, and cobbled) and a video projector + five screens, a walkable led floor (4.5 m × 1.5 m), and an audio/video controller console. |
| Exercises | (1) Motor training: warm-up (stretching, squat with spread legs, squat with spread legs in anteroposterior) + functional balance (lift up heels, lift up tiptoes, lift up heels/tiptoes, lateral load shift, lateral load shift with contralateral leg flexion, lateral load shift with contralateral leg flexion and torso rotation, forward load shift, hip lift up opposite the support leg, load holding for 10 s, load holding with heel lift up, leg flexion/alternate leg flexion, leg flexion and extension/alternate leg flexion and extension, leg flexion and extension backwards, foot sliding forth and back) and gait (walking forward, walking forward oblique, walking forward flexing torso, walking forward oblique flexing torso, walking forward on a wide curve, walking backward, walking backward in line) (2) Cognitive training: executive functions and attention (similarities, differences, analogies, picture sort, be a piano player, take away menu, train guidance, guess who, n-black, remember the sequence) + memory (remember the picture, remember the melody, hide and find, remember the order, remember the design, find the pairs, who belongs where), constructional praxis (puzzle, copy of figures), language (synonymous, antonymous), logical reasoning (incomplete grids, symbol addiction, domino), and orientation (my home, travelling in Europe) exercises. | (1) Motor/cognitive training: with sensory carpets (subtraction, sounds, letters and words, go/no go), and with walkable led floor (Walking Stroop, Walking Trail Making Test, avoid the holes, shopping list) exercises. |
| How much | 15 sessions: (1) motor training + (2) cognitive training, 60 (30 + 30) min/day, 3 days/weeks, 5 weeks. | 15 sessions: (1) simultaneous motor/cognitive tasks, 40 min/day, 3 days/weeks, 5 weeks. |
| Who provided | Both MixT and DTT interventions were carried out by rehabilitation therapists with over 3 years of experience. Verbal assistance was provided by the intervention therapist as needed (e.g., to correct performance of exercises). Intervention measures were developed by experimental researchers. | |
| How | Both MixT and DTT interventions was conducted in one-on-one training sessions daily. | |
| Tailoring | The intervention of both MixT and DTT groups was adjusted according to the subject’s capability. Before training, therapists make a simple and rapid assessment of patients to select the personalized intervention intensity suitable for patients. Programs can also be adjusted according to patients’ own preferences. The intensity of each session was patient-specific, with rest breaks provided upon therapist discretion and patients’ tolerance to activity. Each exercise provided increasing levels of difficulty adjusted by the therapists, consistent with the subject’s capability. | |
2.4. Outcomes
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
| Warm-up: |
| Stretching |
| Squat with spread legs |
| Squat with spread legs in anteroposterior |
| Balance: |
| Lift up heels |
| Lift up tiptoes |
| Lift up heels/tiptoes |
| Lateral load shift |
| Lateral load shift with contralateral leg flexion |
| Lateral load shift with contralateral leg flexion and torso rotation |
| Forward load shift |
| Hip lift up opposite the support leg |
| Load holding for 10 s |
| Load holding with heel lift up |
| Leg flexion/alternate leg flexion |
| Leg flexion and extension/alternate leg flexion and extension |
| Leg flexion and extension backwards |
| Foot sliding forth and back |
| Gait: |
| Walking forward |
| Walking forward oblique |
| Walking forward flexing torso |
| Walking forward oblique flexing torso |
| Walking forward on a wide curve |
| Walking backward |
| Walking backward in line |
| Executive functions and attention: |
| Similarities: the user is asked to select the correct sentence among three describing the similarity between two concepts. |
| Differences: the user is presented with a couple of words/pictures; he has to explain in what way they are different, selecting one of three sentences. |
| Analogies: the user is given one pair of related words/pictures, and another word/picture without its pair. The user must choose a word/picture that has the same relationship to the word/picture as the first pair. |
| Picture sort: there are two boxes of different color. The images are presented one by one on top of the screen, and the user has to drag and drop each image to the correct box by discovering the hidden rule inferred by the feedback given after each choice. |
| Be a piano player: the user is presented with a piano playing some notes. When a note plays, the corresponding key lights up, and the user is required to play the same note, pressing the corresponding key. Notes are presented at increasing speed. |
| Take away menu: the user must order from a take-away menu following some rules (e.g., maximum price, foods not to be ordered). |
| Train guidance: the user is presented a group of persons on the screen moving in different directions. The aim of the task consists of choosing the direction of the central person, suppressing automatic response to the stimuli. |
| Guess who: the user is asked to eliminate candidates, and correctly guess the mystery person, chosen using the cues provided. |
| N-back: a sequence of pictures is presented. The user is asked to touch the screen when a picture matches with a picture presented n steps earlier in the sequence (e.g., 1, 2, or 3…). On the side, a green flag or a red X appear based on whether the answer is right or wrong. |
| Remember the sequence: the user is presented with an array with a start box colored. All possible pictures that can be displaced on the array are presented at the bottom of the array. The sequence starts with one picture positioned in one box next to the start box. Then, the clear array is re-presented, and the user has to drag the correct picture into the correct position. Then, two other pictures are presented, each time in a different sequence, and so on. The user is notified upon making a mistake, and there are no time limits to complete each sequence. |
| Memory |
| Remember the picture: the task is presented with a photo album of one large and several smaller photos. The largest photo—the one to remember—is replaced with another one after a few seconds. Among the smaller photos is the one that was shown previously, and needs to be chosen from. The user is notified when making a mistake, and then the game starts from the beginning. |
| Remember the melody: the user is presented with a piano playing some notes, with the corresponding key lighting up. The user is asked to remember in which specific sequence the notes were played, and to reproduce the melody. The user is notified upon making a mistake, and then the game starts from the beginning. |
| Hide and find: The user is shown of a fully-furnished and fully-decorated room, and is asked to hide 5–10 items in there. After a 15–20 min delay, the user is asked to recall where he has hidden the various objects. |
| Remember the order: the user is shown a menu, and is asked to memorize a list of dishes. Immediately after, the user is asked to recognize the studied materials among distracters. |
| Remember the design: the user is shown a design drawn on a 9-dot matrix, and is asked to encode it. Subsequently, the user is asked to reproduce the pattern on screen. |
| Find the pairs: the user is shown a grid of paired cards. After the cards are covered, the user is asked to find the matching pictures. |
| Who belongs where: the user has to choose the correct profession of famous people, dragging the pictures in the right category among two alternatives. |
| Constructional praxis |
| Puzzle: the user is shown pieces of a puzzle, and is asked to put them onto a grid in order to make the picture. There is no time limit to complete the game. |
| Copy of figures: the user is asked to copy the geometrical figures using fingers. |
| Language |
| Synonymous: a set of words are presented in two different lists. The user is required to draw a line with his finger between the words on the left and their synonyms on the right. |
| Antonymous: a set of words are presented in two different lists. The user is required to draw a line with his finger between the words on the left and their antonyms on the right. |
| Logical reasoning |
| Incomplete grids: the user is asked to complete the image representing a visuo-spatial pattern by inserting the right tile in a multiple choice. |
| Symbol addition: the user is asked to solve arithmetic operations using symbols instead of digits. |
| Domino: the user is asked to pair identical dominos by placing each tile next to the corresponding one. |
| Orientation |
| My home: the user has to find a way to move a person into a house following different indications to cover a specific trail. |
| Travelling in Europe: the user is asked to make a virtual tour selecting several countries following a specific sequence. |
| Sensory carpets (medium density smooth, sandy, and cobbled) |
| Subtraction: the user is asked to walk forward on a carpet by subtracting from 50, one (i.e., 50-1; easy), two (i.e., 50-2; medium), or three (i.e., 50-3 difficult) numbers. |
| Sounds: the user is asked to walk forward on a carpet by listening a sound (e.g., sound of bell, phone, intercom, train, rain, etc.; easy), by listening a sound and naming it (medium), or by listening a sound and making a judgment (i.e., natural/artificial, coherent/incoherent) on it (difficult). |
| Letters and words: the user is asked to walk forward on a carpet by saying the letters of the alphabet out loud (a letter at every step; easy), by saying words that begin with a certain letter (medium) out loud, or by saying words that belong to a certain category out loud (e.g., animals; difficult). |
| Go/No go: the user is asked to walk forward on a carpet respecting congruent (i.e., walk at a green light, and stop at a red light; easy), or incongruent (i.e., stop at a green light, and walk at a red light; easy) signals projected on a screen. |
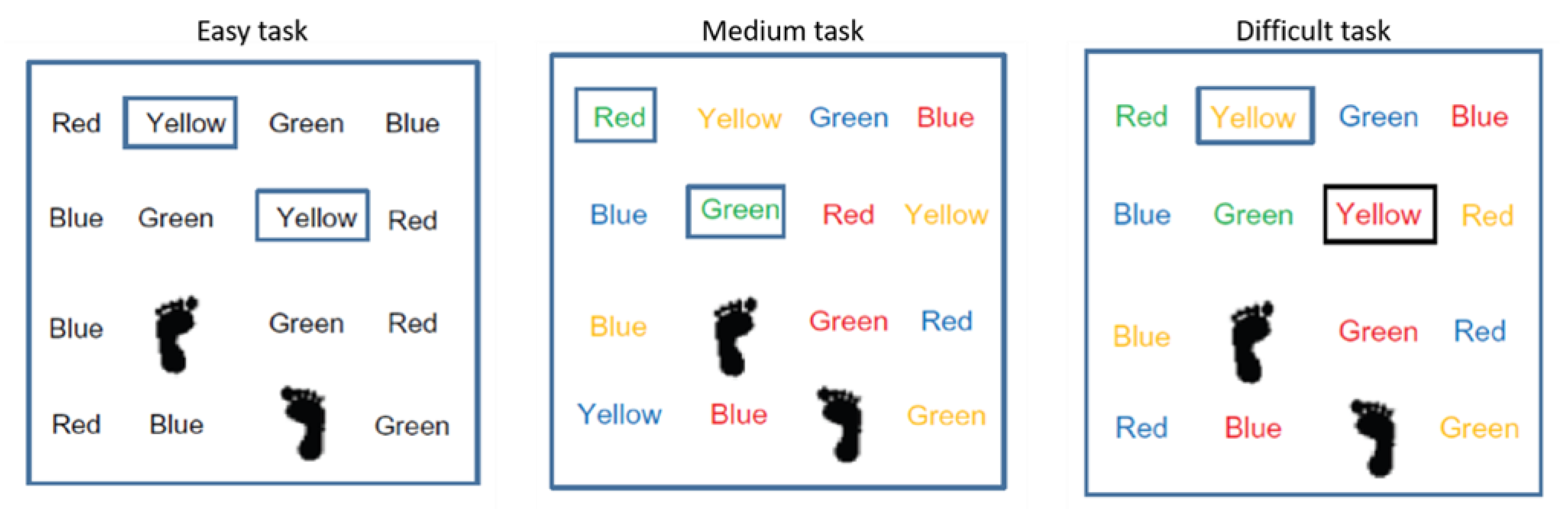
| Walking Stroop: the user is asked to walk forward a walkable led floor with black words naming colors (e.g., red, yellow, green, blue), following words naming a color (e.g., yellow), and saying the color out loud (e.g., yellow) (easy); or to walk forward on a walkable led floor with colored words, naming correspondent (e.g., word “green” colored in green) and non-correspondent colors (e.g., word “red” colored in green), following words’ colors in a certain color (e.g., all words colored in green), and saying the followed color out loud (e.g., green) (medium); or to walk forward on a walkable led floor with colored words, naming correspondent (e.g., word “yellow” colored in yellow) and non-correspondent colors (e.g., word “yellow” colored in red), following words naming a certain color (e.g., all words “yellow”) and saying the followed color out loud (e.g., “yellow”) (difficult). (Figure A1) |
| Walking Trail Making Test: the user is asked to walk forward on a walkable led floor with numbers or numbers + letters following in ascending order (from 1 to 20 and/or from a to z) numbers (easy), or numbers + letters (difficult). |
| Avoid the holes: the user is asked to walk forward on a walkable led floor that simulates a street, avoiding holes that appear on one side (easy) or on both sides (medium) of the street, and by following the directions on signs projected on a screen (e.g., stop, raise your arms). |
| Shopping list: the user is asked to walk forward on a walkable led floor that simulates a street by looking at (projected on a screen) or listening to some shopping list items (e.g., milk, eggs, soap). She/he is asked to cross the street by remembering the shopping list. |

References
- Ayoung-Chee, P.; McIntyre, L.; Ebel, B.E.; Mack, C.D.; McCormick, W.; Maier, R.V. Long-term outcomes of ground-level falls in the elderly. J. Trauma Acute Care Surg. 2014, 76, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Peel, N.M. Epidemiology of falls in older age. Can. J. Aging 2011, 30, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Sapmaz, M.; Mujdeci, B. The effect of fear of falling on balance and dual task performance in the elderly. Exp. Gerontol. 2021, 147, 111250. [Google Scholar] [CrossRef] [PubMed]
- Denissen, S.; Staring, W.; Kunkel, D.; Pickering, R.M.; Lennon, S.; Geurts, A.C.; Weerdesteyn, V.; Verheyden, G.S.A.F. Interventions for preventing falls in people after stroke. Cochrane Database Syst. Rev. 2019, 10, CD008728. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. J. Am. Geriatr. Soc. 2007, 55, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Yang, H.; Zhou, Q.; Pan, H. Effects of cognitive motor dual-task training on stroke patients: A RCT-based meta-analysis. J. Clin. Neurosci. 2021, 92, 175–182. [Google Scholar] [CrossRef]
- Fuller, G.F. Falls in the elderly. Am. Fam. Physician 2000, 61, 2159–2168. [Google Scholar]
- Tan, K.M.; Tan, M.P. Stroke and falls-clash of the two titans in geriatrics. Geriatrics 2016, 1, 31. [Google Scholar] [CrossRef]
- Ahmad Ainuddin, H.; Romli, M.H.; Hamid, T.A.; Salim, M.S.F.; Mackenzie, L. Stroke Rehabilitation for Falls and Risk of Falls in Southeast Asia: A Scoping Review with Stakeholders’ Consultation. Front. Public Health 2021, 9, 611793. [Google Scholar] [CrossRef]
- Faria-Fortini, I.; Polese, J.C.; Faria, C.D.C.M.; Scianni, A.A.; Nascimento, L.R.; Teixeira-Salmela, L.F. Fall Efficacy Scale-International cut-off score discriminates fallers and non-fallers individuals who have had stroke. J. Bodyw. Mov. Ther. 2021, 26, 167–173. [Google Scholar] [CrossRef]
- Schmid, A.A.; Yaggi, H.K.; Burrus, N.; McClain, V.; Austin, C.; Ferguson, J.; Fragoso, C.; Sico, J.J.; Miech, E.J.; Matthias, M.S.; et al. Circumstances and consequences of falls among people with chronic stroke. J. Rehabil. Res. Dev. 2013, 50, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.F.; Yin, J.H.; Tung, T.H.; Shimada, T. Falls efficacy among stroke survivors living in the community. Disabil. Rehabil. 2011, 33, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.A.; Rittma, M. Consequences of poststroke falls: Activity limitation, increased dependence, and the development of fear of falling. Am. J. Occup. Ther. 2009, 63, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Hopewell, S.; Adedire, O.; Copsey, B.J.; Boniface, G.J.; Sherrington, C.; Clemson, L.; Close, J.C.; Lamb, S.E. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2018, 7, CD012221. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 2012, CD007146. [Google Scholar] [CrossRef]
- Barban, F.; Annicchiarico, R.; Melideo, M.; Federici, A.; Lombardi, M.G.; Giuli, S.; Ricci, C.; Adriano, F.; Griffini, I.; Silvestri, M.; et al. Reducing Fall Risk with Combined Motor and Cognitive Training in Elderly Fallers. Brain Sci. 2017, 7, 19. [Google Scholar] [CrossRef]
- Herold, F.; Hamacher, D.; Schega, L.; Müller, N.G. Thinking While Moving or Moving While Thinking—Concepts of Motor-Cognitive Training for Cognitive Performance Enhancement. Front. Aging Neurosci. 2018, 10, 228. [Google Scholar] [CrossRef]
- Ruffieux, J.; Keller, M.; Lauber, B.; Taube, W. Changes in Standing and Walking Performance Under Dual-Task Conditions Across the Lifespan. Sports Med. 2015, 45, 1739–1758. [Google Scholar] [CrossRef]
- Zukowski, L.A.; Tennant, J.E.; Iyigun, G.; Giuliani, C.A.; Plummer, P. Dual-tasking impacts gait, cognitive performance, and gaze behavior during walking in a real-world environment in older adult fallers and non-fallers. Exp. Gerontol. 2021, 150, 111342. [Google Scholar] [CrossRef]
- Yang, Y.R.; Chen, Y.C.; Lee, C.S.; Cheng, S.J.; Wang, R.Y. Dual-task-related gait changes in individuals with stroke. Gait Posture 2007, 25, 185–190. [Google Scholar] [CrossRef]
- Mori, T.; Takeuchi, N.; Izumi, S.I. Prefrontal cortex activation during a dual task in patients with stroke. Gait Posture 2018, 59, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.D.N.; Afonso, S.V.; Felipe, L.R.; Oliveira, R.A.; Patrizzi Martins, L.J.; Pascucci Sande de Souza, L.A. Dual-task intervention based on trail making test: Effects on Parkinson’s disease. J. Bodyw. Mov. Ther. 2021, 27, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Sturnieks, D.L.; Menant, J.; Valenzuela, M.; Delbaere, K.; Sherrington, C.; Herbert, R.D.; Lampit, A.; Broadhouse, K.; Turner, J.; Schoene, D.; et al. Effect of cognitive-only and cognitive-motor training on preventing falls in community-dwelling older people: Protocol for the smartstep randomised controlled trial. BMJ Open 2019, 9, e029409. [Google Scholar] [CrossRef] [PubMed]
- Lapierre, N.; Um Din, N.; Igout, M.; Chevrier, J.; Belmin, J. Effects of a Rehabilitation Program Using a Patient-Personalized Exergame on Fear of Falling and Risk of Falls in Vulnerable Older Adults: Protocol for a Randomized Controlled Group Study. JMIR Res. Protoc. 2021, 10, e24665. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Canbek, J.; Fulk, G.; Nof, L.; Echternach, J. Test-retest reliability and construct validity of the Tinetti performance-oriented mobility assessment in people with stroke. J. Neurol. Phys. Ther. 2013, 37, 14–19. [Google Scholar] [CrossRef]
- Perrochon, A.; Kemoun, G.; Watelain, E.; Berthoz, A. Walking Stroop carpet: An innovative dual-task concept for detecting cognitive impairment. Clin. Interv. Aging 2013, 8, 317–328. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Butland, R.J.; Pang, J.; Gross, E.R.; Woodcock, A.A.; Geddes, D.M. Two-, six-, and 12-minute walking tests in respiratory disease. Br. Med. J. 1982, 284, 1607–1608. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Liu, J.Y.W.; Fong, K.N.K.; Qin, J.; Leung, P.K.; Sin, O.S.K.; Hon, P.Y.; Suen, L.W.; Tse, M.K.; Lai, C.K. Feasibility and Effects of Virtual Reality Motor-Cognitive Training in Community-Dwelling Older People with Cognitive Frailty: Pilot Randomized Controlled Trial. JMIR Serious Games 2021, 9, e28400. [Google Scholar] [CrossRef]
- Liu, Y.C.; Yang, Y.R.; Tsai, Y.A.; Wang, R.Y. Cognitive and motor dual task gait training improve dual task gait performance after stroke—A randomized controlled pilot trial. Sci. Rep. 2017, 7, 4070. [Google Scholar] [CrossRef] [PubMed]
- De Barros, G.M.; Melo, F.; Domingos, J.; Oliveira, R.; Silva, L.; Fernandes, J.B.; Godinho, C. The Effects of Different Types of Dual Tasking on Balance in Healthy Older Adults. J. Pers. Med. 2021, 11, 933. [Google Scholar] [CrossRef] [PubMed]
- Varela-Vásquez, L.A.; Minobes-Molina, E.; Jerez-Roi, J. Dual-task exercises in older adults: A structured review of current literature. J. Frailty Sarcopenia Falls 2020, 5, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Sekendiz, B.; Cuğ, M.; Korkusuz, F. Effects of Swiss ball core strength training on strength, endurance, flexibility, and balance in sedentary women. J. Strength Cond. Res. 2010, 24, 3032–3040. [Google Scholar] [CrossRef]
- Barboza, N.M.; Terra, M.B.; Bueno, M.E.B.; Christofoletti, G.; Smaili, S.M. Physiotherapy Versus Physiotherapy Plus Cognitive Training on Cognition and Quality of Life in Parkinson Disease: Randomized Clinical Trial. Am. J. Phys. Med. Rehabil. 2019, 98, 460–468. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Lopes, K.J.; Costa, D.F.; Santos, L.F.; Castro, D.P.; Bastone, A.C. Prevalence of fear of falling among a population of older adults and its correlation with mobility, dynamic balance, risk and history of falls. Braz. J. Phys. Ther. 2009, 13, 223–229. [Google Scholar] [CrossRef]
- Kumar, A.; Carpenter, H.; Morris, R.; Lliffe, S.; Kendrick, D. Which factors are associated with fear of falling in community-dwelling older people? Age Ageing 2014, 43, 76–84. [Google Scholar] [CrossRef]


| MixT Group (n = 13) | DTT Group (n = 13) | p Value | |
|---|---|---|---|
| Age (years) a | 79.8 ± 8.7 | 75.4 ± 5.5 | 0.15 |
| Sex (male/female) b | 3/10 | 9/4 | 0.02 |
| POMA tot a | 18.8 ± 6.6 | 18.8 ± 2.6 | 0.96 |
| POMA-B a | 11.0 ± 4.6 | 10.4 ± 2.0 | 0.76 |
| POMA-G a | 7.8 ± 2.6 | 8.4 ± 1.7 | 0.42 |
| FES-I a | 33.8 ± 12.4 | 35.1 ± 11.4 | 0.65 |
| 6-MWT (m) a | 237.8 ± 195.0 | 279.9 ± 139.5 | 0.48 |
| Gait speed (m/s) a | 0.7 ± 0.5 | 0.8 ± 0.4 | 0.48 |
| MixT Group (n = 13) | DTT Group (n = 13) | Inter-Group Differences | |||
|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||
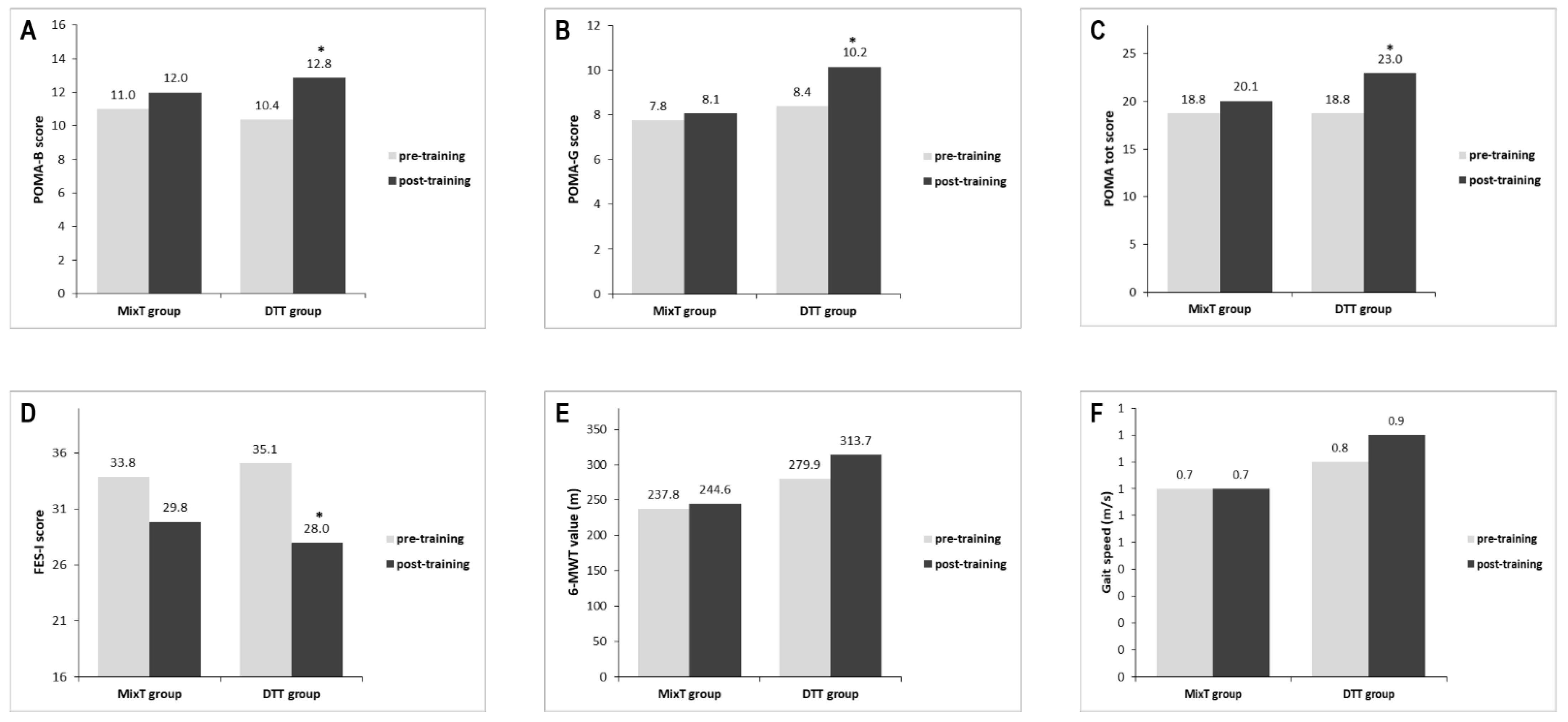
| POMA-tot a | 18.8 ± 6.7 | 20.1 ± 6.4 | 18.8 ± 2.6 | 23.0 ± 2.6 | |
| Change values b | 1.3 ± 1.9 | 4.2 ± 1.4 | p = 0.001 | ||
| POMA-B a | 11.0 ± 4.6 | 12.0 ± 4.1 | 10.4 ± 2.0 | 12.8 ± 2.0 | |
| Change values b | 1.0 ± 1.7 | 2.5 ± 1.6 | p = 0.03 | ||
| POMA-G a | 7.8 ± 2.6 | 8.1 ± 2.9 | 8.4 ± 1.7 | 10.2 ± 1.2 | |
| Change values b | 0.3 ± 0.8 | 1.8 ± 1.1 | p = 0.001 | ||
| FES-I a | 33.8 ± 12.4 | 29.8 ± 9.0 | 35.1 ± 11.4 | 28.0 ± 9.8 | |
| Change values b | −4.0 ± 9.1 | −7.1 ± 6.3 | p = 0.08 | ||
| 6-MWT (m) a | 237.8 ± 195.1 | 244.6 ± 205.4 | 279.9 ± 139.5 | 313.7 ± 106.0 | |
| Change values b | 6.7 ± 44.4 | 33.8 ± 75.1 | p = 0.72 | ||
| Gait speed (m/s) a | 0.7 ± 0.5 | 0.7 ± 0.6 | 0.8 ± 0.4 | 0.9 ± 0.3 | |
| Change values b | 0.0 ± −0.1 | 0.1 ± 0.2 | p = 0.72 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spanò, B.; Lombardi, M.G.; De Tollis, M.; Szczepanska, M.A.; Ricci, C.; Manzo, A.; Giuli, S.; Polidori, L.; Griffini, I.A.; Adriano, F.; et al. Effect of Dual-Task Motor-Cognitive Training in Preventing Falls in Vulnerable Elderly Cerebrovascular Patients: A Pilot Study. Brain Sci. 2022, 12, 168. https://doi.org/10.3390/brainsci12020168
Spanò B, Lombardi MG, De Tollis M, Szczepanska MA, Ricci C, Manzo A, Giuli S, Polidori L, Griffini IA, Adriano F, et al. Effect of Dual-Task Motor-Cognitive Training in Preventing Falls in Vulnerable Elderly Cerebrovascular Patients: A Pilot Study. Brain Sciences. 2022; 12(2):168. https://doi.org/10.3390/brainsci12020168
Chicago/Turabian StyleSpanò, Barbara, Maria G. Lombardi, Massimo De Tollis, Maria A. Szczepanska, Claudia Ricci, Alice Manzo, Simone Giuli, Lorenzo Polidori, Ivo A. Griffini, Fulvia Adriano, and et al. 2022. "Effect of Dual-Task Motor-Cognitive Training in Preventing Falls in Vulnerable Elderly Cerebrovascular Patients: A Pilot Study" Brain Sciences 12, no. 2: 168. https://doi.org/10.3390/brainsci12020168