
A Systematic Review of Neurofeedback for the Management of Motor Symptoms in Parkinson’s Disease

 , ,
, ,
Abstract
:1. Introduction
Review Question and Objectives
- The effectiveness of neurofeedback as a treatment for reducing PD motor symptom severity.
- The importance of specific protocol parameters for effective and reliable neurofeedback in terms of training regime, targeted brain activity, delivery of brain activity feedback signal, and changes in brain activity.
- The association between specific neurofeedback protocols and clinical outcomes.
2. Methods
2.1. Ethical Considerations
2.2. Inclusion Criteria
2.2.1. Population
2.2.2. Intervention
2.2.3. Comparison
2.2.4. Outcomes
- Immediate and long-term sustained changes in brain activity following neurofeedback.
- Immediate and long-term sustained changes in motor function or performance as measured by physiology (e.g., electromyography (EMG)) and/or other objective clinical outcome measures such as the Unified Parkinson’s Disease rating scale (UPDRS) or a questionnaire assessment of PD symptoms.
- Neurofeedback protocol (i.e., targeted brain activity, presentation of brain activity to participants, criteria for “successful” neurofeedback).
- Neurofeedback training details (i.e., who provides the neurofeedback training, guidance provided to participants, training regime).
- The relationship between the above neurofeedback details and neurofeedback outcomes (i.e., success at neurofeedback and clinical outcomes).
2.2.5. Types of Studies
2.3. Search Strategy
2.4. Information Sources
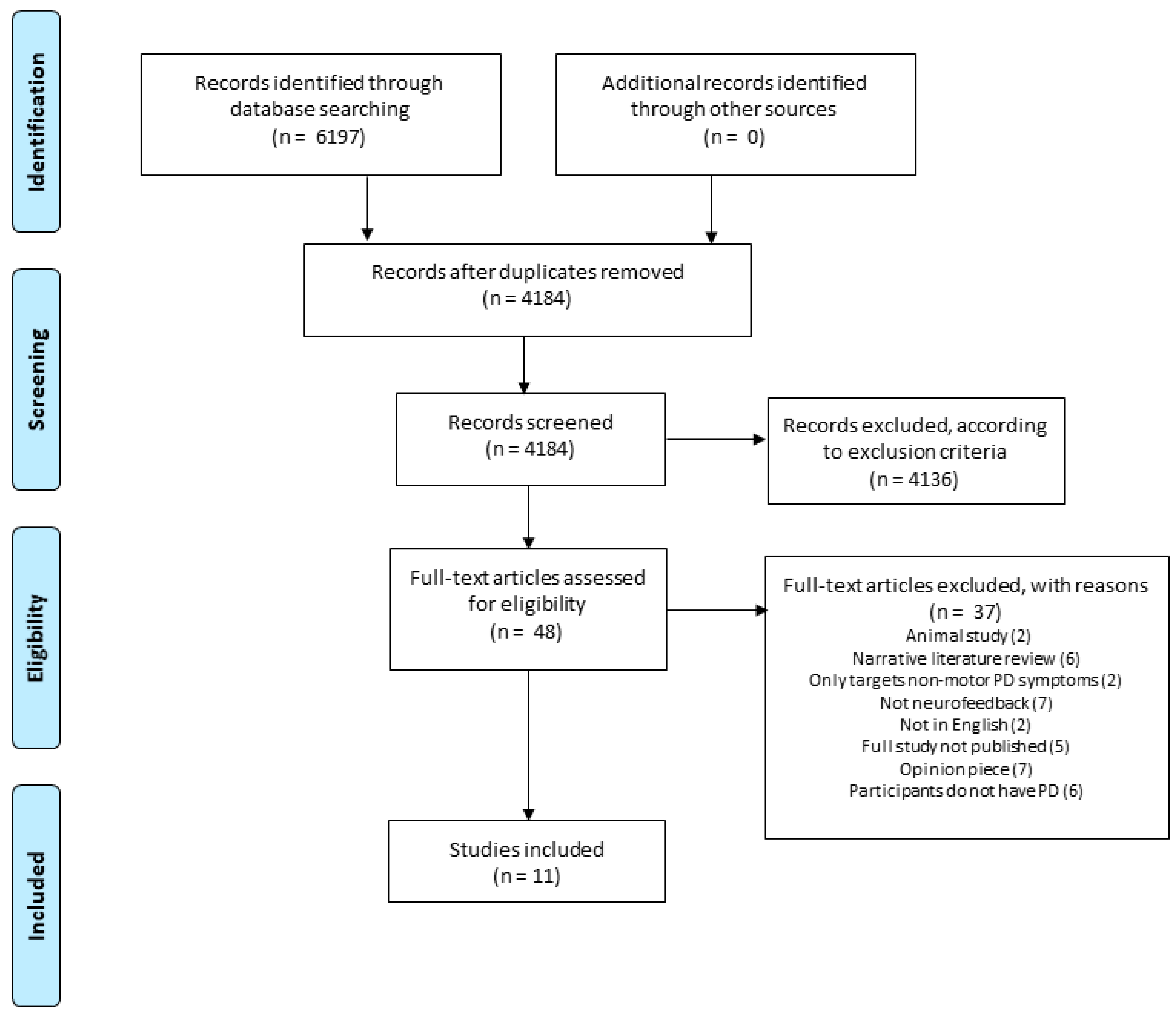
2.5. Study Selection
2.6. Assessment of Methodological Quality
2.7. Data Extraction
2.8. Data Synthesis
2.9. Assessing Certainty in Findings
3. Results
4. Discussion
4.1. Insufficient Clinical Information and Perspectives
4.2. Limitations in Numerical Data Reporting
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Schrag, A. Quality of life and depression in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 151–157. [Google Scholar] [CrossRef]
- Leroi, I.; Ahearn, D.J.; Andrews, M.; McDonald, K.R.; Bryne, J.E.; Burns, A. Behavioural disorders, disability and quality of life in Parkinson’s disease. Age Ageing 2011, 40, 614–621. [Google Scholar] [CrossRef] [Green Version]
- Radad, K.; Gille, G.; Rausch, W.-D. Short review on dopamine agonists: Insight into clinical and research studies relevant to Parkinson’s disease. Pharmacol. Rep. 2005, 57, 701–712. [Google Scholar]
- Sixel-Döring, F.; Trenkwalder, C.; Kappus, C.; Hellwig, D. Skin complications in deep brain stimulation for Parkinson’s disease: Frequency, time course, and risk factors. Acta Neurochir. 2010, 152, 195–200. [Google Scholar] [CrossRef]
- Xiaowu, H.; Xiufeng, J.; Xiaoping, Z.; Bin, H.; Laixing, W.; Yiqun, C.; Jinchuan, L.; Aiguo, J.; Jianmin, L. Risks of intracranial hemorrhage in patients with Parkinson’s disease receiving deep brain stimulation and ablation. Parkinsonism Relat. Disord. 2010, 16, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, J.M.; Tagliati, M.; Alterman, R.L.; Lozano, A.M.; Stefani, A.; Horak, F.B.; Okun, M.S.; Foote, K.D.; Krack, P.; Pahwa, R.; et al. Deep brain stimulation for Parkinson disease: An expert consensus and review of key issues. Arch. Neurol. 2011, 68, 165. [Google Scholar] [CrossRef]
- Limousin, P.; Foltynie, T. Long-term outcomes of deep brain stimulation in Parkinson disease. Nat. Rev. Neurol. 2019, 15, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Marzbani, H.; Marateb, H.R.; Mansourian, M. Methodological Note: Neurofeedback: A Comprehensive Review on System Design, Methodology and Clinical Applications. Basic Clin. Neurosci. J. 2016, 7, 143–158. [Google Scholar] [CrossRef] [Green Version]
- Little, S.; Brown, P. What brain signals are suitable for feedback controzl of deep brain stimulation in Parkinson’s disease? Ann. N. Y. Acad. Sci. 2012, 1265, 9–24. [Google Scholar] [CrossRef]
- Sitaram, R.; Ros, T.; Stoeckel, L.; Haller, S.; Scharnowski, F.; Lewis-Peacock, J.; Weiskopf, N.; Blefari, M.L.; Rana, R.S.M.; Oblak, E.; et al. Closed-loop brain training: The science of neurofeedback. Nat. Rev. Neurosci. 2016, 18, 86–100. [Google Scholar] [CrossRef] [Green Version]
- Eklund, A. Using Real-Time fMRI to Control a Dynamical System by Brain Activity Classification. Med. Image Comput. Comput. Assist. Interv. 2009, 12, 1000–1008. [Google Scholar] [CrossRef]
- Spay, C.; Meyer, G.; Welter, M.-L.; Lau, B.; Boulinguez, P.; Ballanger, B. Functional imaging correlates of akinesia in Parkinson’s disease: Still open issues. NeuroImage Clin. 2019, 21, 101644. [Google Scholar] [CrossRef]
- Oswal, A.; Beudel, M.; Zrinzo, L.; Limousin, P.; Hariz, M.; Foltynie, T.; Litvak, V.; Brown, P. Deep brain stimulation modulates synchrony within spatially and spectrally distinct resting state networks in Parkinson’s disease. Brain 2016, 139, 1482–1496. [Google Scholar] [CrossRef]
- Cagnan, H.; Mallet, N.; Moll, C.K.E.; Gulberti, A.; Holt, A.B.; Westphal, M.; Gerloff, C.; Engel, A.K.; Hamel, W.; Magill, P.; et al. Temporal evolution of beta bursts in the parkinsonian cortical and basal ganglia network. Proc. Natl. Acad. Sci. USA 2019, 116, 16095–16104. [Google Scholar] [CrossRef] [Green Version]
- Sharott, A.; Gulberti, A.; Hamel, W.; Koppen, J.A.; Munchau, A.; Buhmann, C.; Potter-Nerger, M.; Westphal, M.; Gerloff, C.; Moll, C.K.E.; et al. Spatio-temporal dynamics of cortical drive to human subthalamic nucleus neurons in Parkinson’s disease. Neurobiol. Dis. 2018, 112, 49–62. [Google Scholar] [CrossRef]
- Brown, P. Abnormal oscillatory synchronisation in the motor system leads to impaired movement. Curr. Opin. Neurobiol. 2007, 17, 656–664. [Google Scholar] [CrossRef]
- Fogelson, N.; Williams, D.; Tijssen, M.; van Bruggen, G.; Speelman, H.; Brown, P. Different functional loops between cerebral cortex and the subthalmic area in Parkinson’s disease. Cereb. Cortex 2006, 16, 64–75. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar]
- Reuter, T. Endnote X9. 2020. Available online: https://endnote.com/product-details (accessed on 9 December 2020).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Fukuma, R.; Yanagisawa, T.; Tanaka, M.; Yoshida, F.; Hosomi, K.; Oshino, S.; Tani, N.; Kishima, H. Real-Time Neurofeedback to Modulate β-Band Power in the Subthalamic Nucleus in Parkinson’s Disease Patients. eNeuro 2018, 5. [Google Scholar] [CrossRef]
- Subramanian, L.; Hindle, J.V.; Johnston, S.; Roberts, M.V.; Husain, M.; Goebel, R.; Linden, D. Real-time functional magnetic resonance imaging neurofeedback for treatment of Parkinson’s disease. J. Neurosci. 2011, 31, 16309–16317. [Google Scholar] [CrossRef]
- Erickson-Davis, C.R.; Anderson, J.S.; Wielinski, C.L.; Richter, S.A.; Parashos, S.A. Evaluation of Neurofeedback Training in the Treatment of Parkinson’s Disease: A Pilot Study. J. Neurother. 2012, 16, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, L.; Morris, M.B.; Brosnan, M.; Turner, D.L.; Morris, H.R.; Linden, D.E.J. Functional Magnetic Resonance Imaging Neurofeedback-guided Motor Imagery Training and Motor Training for Parkinson’s Disease: Randomized Trial. Front. Behav. Neurosci. 2016, 10, 111. [Google Scholar] [CrossRef] [Green Version]
- Buyukturkoglu, K.; Rana, M.; Ruiz, S.; Hackley, S.A.; Soekadar, S.R.; Birbaumer, N.; Sitaram, R. Volitional Regulation of Supplementary Motor Area with FMRI-BCI Neurofeedback in Parkinson’s Diseases: A Pilot Study. J. Neurol. Sci. 2013, 30, 180. [Google Scholar]
- Fumuro, T.; Matsuhashi, M.; Mitsueda, T.; Inouchi, M.; Hitomi, T.; Nakagawa, T.; Matsumoto, R.; Kawamata, J.; Inoue, H.; Mima, T.; et al. Bereitschaftspotential augmentation by neuro-feedback training in Parkinson’s disease. Clin. Neurophysiol. 2013, 124, 1398–1405. [Google Scholar] [CrossRef] [Green Version]
- He, S.; Syed, E.; Torrecillos, F.; Tinkhauser, G.; Fischer, P.; Pogosyan, A.; Pereira, E.; Ashkan, K.; Hasegawa, H.; Brown, P.; et al. Beta Oscillation-Targeted Neurofeedback Training Based on Subthalamic LFPs in Parkinsonian Patients. In Proceedings of the International IEEE/EMBS Conference on Neural Engineering (NER), San Francisco, CA, USA, 20–23 March 2019; pp. 81–84. [Google Scholar] [CrossRef]
- Tinaz, S.; Para, K.; Vives-Rodriguez, A.; Martinez-Kaigi, V.; Nalamada, K.; Sezgin, M.; Scheinost, D.; Hampson, M.; Louis, E.D.; Constable, R. Insula as the Interface Between Body Awareness and Movement: A Neurofeedback-Guided Kinesthetic Motor Imagery Study in Parkinson’s Disease. Front. Hum. Neurosci. 2018, 12, 496. [Google Scholar] [CrossRef]
- Kasahara, K.; Hoshino, H.; Furusawa, Y.; DaSalla, C.S.; Honda, M.; Murata, M.; Hanakawa, T. Initial experience with a sensorimotor rhythm-based brain-computer interface in a Parkinson’s disease patient. Brain-Comput. Interfaces 2018, 5, 88–96. [Google Scholar] [CrossRef]
- Thompson, M.; Thompson, L. Biofeedback for Movement Disorders (Dystonia with Parkinson’s Disease): Theory and Preliminary Results. J. Neurother. 2002, 6, 51–70. [Google Scholar]
- Khanna, P.; Carmena, J.M. Using Brain-Machine Interfaces to Study Motor Cortical Population Activity; University of California: Berkeley, CA, USA, 2017. [Google Scholar]
- Esmail, S.; Linden, D. Neural Networks and Neurofeedback in Parkinson’s Disease. Neuroregulation 2014, 1, 240–272. [Google Scholar] [CrossRef] [Green Version]
- Devergnas, A.; Caiola, M.; Pittard, D.; Wichmann, T. Cortical Phase–Amplitude Coupling in a Progressive Model of Parkinsonism in Nonhuman Primates. Cereb. Cortex 2017, 29, 167–177. [Google Scholar] [CrossRef]
- Sharott, A.; Vinciati, F.; Nakamura, K.C.; Magill, P.J. A Population of Indirect Pathway Striatal Projection Neurons Is Selectively Entrained to Parkinsonian Beta Oscillations. J. Neurosci. 2017, 37, 9977–9998. [Google Scholar] [CrossRef] [Green Version]
- West, T.O.; Berthouze, L.; Halliday, D.M.; Litvak, V.; Sharott, A.; Magill, P.; Farmer, S. Propagation of beta/gamma rhythms in the cortico-basal ganglia circuits of the parkinsonian rat. J. Neurophysiol. 2018, 119, 1608–1628. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Frech, F.; Zamarbide, I.; Alegre, M.; Rodriguez-Oroz, M.C.; Guridi, J.; Manrique, M.; Valencia, M.; Artieda, J.; Obeso, J.A. Slow oscillatory activity and levodopa-induced dyskinesias in Parkinson’s disease. Brain 2006, 129, 1748–1757. [Google Scholar] [CrossRef] [Green Version]
- Foffani, G.; Bianchi, A.M.; Baselli, G.; Priori, A. Movement-related frequency modulation of beta oscillatory activity in the human subthalamic nucleus. J. Physiol. 2005, 568, 699–711. [Google Scholar] [CrossRef]
- De Vries, I.E.; Daffertshofer, A.; Stegeman, D.F.; Boonstra, T.W. Functional connectivity in the neuromuscular system underlying bimanual coordination. J. Neurophysiol. 2016, 116, 2576–2585. [Google Scholar] [CrossRef] [Green Version]
- Gatev, P.; Darbin, O.; Wichmann, T. Oscillations in the basal ganglia under normal conditions and in movement disorders. Mov. Disord. 2006, 21, 1566–1577. [Google Scholar] [CrossRef]
- Lofredi, R.; Tan, H.; Neumann, W.-J.; Yeh, C.-H.; Schneider, G.-H.; Kuhn, A.A.; Brown, P. Beta bursts during continuous movements accompany the velocity decrement in Parkinson’s disease patients. Neurobiol. Dis. 2019, 127, 462–471. [Google Scholar] [CrossRef]
- Torrecillos, F.; Tinkhauser, G.; Fischer, P.; Green, A.L.; Aziz, T.Z.; Foltynie, T.; Limousin, P.; Zrinzo, L.; Ashkan, K.; Brown, P.; et al. Modulation of Beta Bursts in the Subthalamic Nucleus Predicts Motor Performance. J. Neurosci. 2018, 38, 8905–8917. [Google Scholar] [CrossRef] [Green Version]
- He, S.; Everest-Phillips, C.; Clouter, A.; Brown, P.; Tan, H. Neurofeedback-Linked Suppression of Cortical β Bursts Speeds Up Movement Initiation in Healthy Motor Control: A Double-Blind Sham-Controlled Study. J. Neurosci. 2020, 40, 4021–4032. [Google Scholar] [CrossRef] [Green Version]
- Cole, S.R.; van der Meij, R.; Peterson, E.J.; de Hemptinne, C.; Starr, P.A.; Voytek, B. Nonsinusoidal beta oscillations reflect cortical pathophysiology in Parkinson’s disease. J. Neurosci. 2017, 37, 4830–4840. [Google Scholar] [CrossRef]
- Rivlin-Etzion, M.; Marmor, O.; Saban, G.; Rosin, B.; Haber, S.N.; Vaadia, E.; Prut, Y.; Bergman, H. Low-Pass Filter Properties of Basal Ganglia Cortical Muscle Loops in the Normal and MPTP Primate Model of Parkinsonism. J. Neurosci. 2008, 28, 633–649. [Google Scholar] [CrossRef]
- Ros, T.; Enriquez-Geppert, S.; Zotev, V.; Young, K.D.; Wood, G.; Whitfield-Gabrieli, S.; Wan, F.; Vuilleumier, P.; Vialatte, F.; Van De Ville, D.; et al. Consensus on the reporting and experimental design of clinical and cognitive-behavioural neurofeedback studies (CRED-nf checklist). Brain 2020, 143, 1674–1685. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Quasi Experimental Studies | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | * Total | ||||
| Buyukturkoglu et al. [26] | Y | N | N | N | Y | N | N | U | Y | 33% | ||||
| Fukama et al. [22] | Y | Y | Y | Y | Y | N | Y | Y | Y | 89% | ||||
| Fumuro et al. [27] | Y | U | Y | N | Y | N | Y | Y | Y | 67% | ||||
| He et al. [28] | Y | U | U | N | Y | Y | Y | U | Y | 56% | ||||
| Subramanian et al. [23] | Y | U | U | Y | Y | N | Y | Y | Y | 67% | ||||
| Tinaz et al. [29] | Y | Y | U | Y | U | N | N | Y | Y | 56% | ||||
| RCTs | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | * Total |
| Erikson-Davis et al. [24] | U | U | N | N | N | U | N | N/A | Y | Y | Y | N | N | 23% |
| Subramanian et al. [25] | Y | N | U | N | N | Y | N | N | Y | N | Y | Y | N | 38% |
| Case reports | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | * Total | |||||
| Kasahara et al. [30] | Y | N | Y | Y | Y | N | N | N | 50% | |||||
| Thompson & Thompson [31] | N | N | Y | N | Y | Y | U | N | 38% | |||||
| Cross-sectional studies | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | * Total | |||||
| Khanna & Carmena [32] | N | N | Y | N | N | N | Y | Y | 38% |
| Author | Aim | Targeted PD Symptom | Country | Design | Intervention Condition | Control Condition | Total N |
|---|---|---|---|---|---|---|---|
| Buyukturkoglu et al., (2013) [26] | Examining the effectiveness of real-time fMRI neurofeedback (reinforcement of SMA BOLD signal) on hand motor performance | Hand-motor performance/akinesia | USA | Case study | fMRI neurofeedback, finger tapping | No control condition | 1 |
| Erikson-Davis et al., (2012) [24] | Testing if scalp EEG neurofeedback (reinforcement of 12–15 Hz, suppression 4–10 Hz and 11–30 Hz) would lead to a decrease in PD motor-symptoms | Levodopa-induced dyskinesia | USA | RCT | Scalp EEG neurofeedback | Sham trial, followed by scalp EEG neurofeedback | 9 |
| Fukama et al., (2018) [22] | Examining if DBS EEG neurofeedback (reinforcement and suppression of 13–30 Hz from STN) induces plastic changes in the STN activity of individuals with PD | General motor symptoms | Japan | Quasi-experimental | DBS neurofeedback | No control condition | 8 |
| Fumuro et al., (2013) [27] | Examining whether PD patients could increase BP amplitude with scalp EEG neurofeedback | No target symptom reported | Japan | Quasi-experimental | Scalp EEG neurofeedback | No control condition | 21 |
| He et al., (2019) [28] | Investigating whether DBS EEG neurofeedback (supress beta rhythms in STN) is possible for people with PD | General motor symptoms | UK | Observational | DBS EEG neurofeedback | No control condition | 3 |
| Kasahara et al., (2018) [30] | Examining scalp EEG neurofeedback (reinforcement and suppression 9.5–12.5 Hz of SMR) in a patient with PD | No target symptom reported | Japan | Case study | Scalp EEG neurofeedback, motor imagery practice | No control condition | 1 |
| Khanna & Carmena (2017) [32] | To show that PD patients can control beta activity using DBS EEG neurofeedback | General motor symptoms | USA | Observational | DBS neurofeedback | No control condition | 3 |
| Subramanian et al., (2011) [23] | Assessing whether PD patients are able to alter local brain activity to improve motor function | General motor symptoms | UK | Quasi-experimental | fMRI neurofeedback, hand movement task, home practice of motor imagery | Sham trial, hand movement task, home practice of motor imagery | 10 |
| Subramanian et al., (2016) [25] | Determining the effect of neurofeedback and motor training alone on motor and non-motor functions in PD | General motor and non-motor symptoms | UK | RCT | fMRI neurofeedback, hand motor task, Wii fit motor training, home practice of motor imagery | Wii fit motor training | 30 |
| Thompson & Thompson (2002) [31] | To present a theoretical framework for a biofeedback treatment for movement disorders using a case study involving dystonia with PD | General motor symptoms | Canada | Case study | Scalp EEG, RSA training | No control condition | 1 |
| Tinaz et al., (2018) [29] | Testing the ability of those with PD to learn to use fMRI neurofeedback (reinforcement of the right insula-dorsomedial frontal cortex functional connectivity) | General motor symptoms | USA | Quasi-experimental | fMRI neurofeedback, motor imagery practice, heartbeat counting task, home practice of motor imagery | No control condition | 8 |
| Author(s) (Date) | PD Severity Measure | Mean (SD/Range) | Outcome Measure | Change within the Intervention Condition | Change within the Control Condition | Relative Change a Between Conditions |
|---|---|---|---|---|---|---|
| Buyukturkoglu et al., (2013) [26] | Hoehn and Yahr Scale | 2.5 (SD not reported) | Button pressing reaction time in seconds | 23 (±83) | No control condition | N/A |
| Erikson-Davis et al., (2012) [24] | UPDRS-III | 20 (4–42) | Parkinson’s Disease Home Diary | 0 (SD not reported) | 2 (SD not reported) | Insufficient data for calculation |
| Modified Abnormal Involuntary Movement Scale | −2.5 (SD not reported) | −2 (SD not reported) | Insufficient data for calculation | |||
| Fukama et al., (2018) [22] | UPDRS-III | 31.13 (±20.49) | Pre-post EMG resting baselines | Not reported ** | No control condition | N/A |
| Fumuro et al., (2013) [27] | Hoehn and Yahr Scale | Not reported | None | N/A | N/A | N/A |
| He et al., (2019) [28] | None | N/A | None | N/A | N/A | N/A |
| Kasahara et al., (2018) [30] | UPDRS-III | 13 (SD not reported) | None | N/A | N/A | N/A |
| Khanna & Carmena (2017) [32] | UPDRS-III | Not reported | None | N/A | N/A | N/A |
| Subramanian et al., (2011) [23] | Hoehn and Yahr Scale | 1.3 (±0.64) | UPDRS—Motor Scale | −5.2 (SD not reported) ** | −1.6 (SD not reported) | 4.4 (SD not reported) b |
| Finger tapping test | 55.6 (SD not reported) ** | 1.2 (SD not reported) | −88 (SD not reported) b | |||
| Subramanian et al., (2016) [25] | UPDRS | 25 (±11) | UPDRS—Motor Scale | −4.5 (±3.3) *** | −1.8 (±8.3) | Sufficient data not available for calculation |
| PDQ-39 | −2.4 (±4.8) * | −3.6 (±6.5) | Sufficient data not available for calculation | |||
| Thompson & Thompson (2002) [31] | None | N/A | None | N/A | N/A | N/A |
| Tinaz et al., (2018) [29] | UPDRS | 44.8 (±5.4) | UPDRS—Motor Scale | −0.3 (±2.1) | No control condition | N/A |
| Paper | NF Type | NF Targeted Activity | NF Run Length | NF Session Length | No. Sessions | Time between Sessions | Delivery Method | Instructions Given on How to Complete the Task | Success Criteria? | Success Rates |
|---|---|---|---|---|---|---|---|---|---|---|
| Buyukturkoglu et al., (2013) [26] | fMRI | SMA Reinforcement | 22.5 s | 3–4 (Varied between participants) | 1–2 (Varied between participants) | 5 days | Thermometer (A vertical bar with height targets) | Motor imagery | Not reported | 100% |
| Erikson-Davis et al., (2012) [24] | Scalp EEG | C3 & C4 Reinforce 8–15 Hz Inhibit 4–8 Hz Inhibit 23–34 Hz | Not reported | 30 m | 24 | 1–6 days | Audio feedback | No specific instructions | Not reported | Not reported |
| Fukama et al., (2018) [22] | DBS EEG | STN Reinforce or inhibit 13–30 Hz | 10 m | 10 m | 1 | N/A | Circle whose size changed with 13–30 Hz power changes | No specific instructions | Change in pre post EEG levels as determined by t test | 75% |
| Fumuro et al., (2013) [27] | Scalp EEG | Cz Bereitschaftspotential | 10 s | 8.7 m | 2–4 | 1–6 days | A sunfish moved up or down depending on potential shift | No specific instructions | Amplitude must have exceeded a defined target level (based on baseline) and remained at that level for at least 2 s in the last 4 s of each trial | 40% and 45% for PD and control groups, respectively |
| He et al., (2019) [28] | ECoG | Left or Right STN Inhibit 13–30 Hz | 5–8 s | 30 m | 1 | N/A | A basketball moved vertically, where the basketball went higher with reduced beta power | Motor imagery of hand | Comparing ball position between neurofeedback training and no neurofeedback training sessions | 66% |
| Kasahara et al., (2018) [30] | Scalp EEG | C3 or C4 Reinforce and inhibit 9.5–12.5 Hz | 4 s | 24 min | 2 (ON and OFF) | 2 days | A falling cursor that moved left or right to hit a target depending on targeted ERD | Motor imagery of the left or right hand | Ability to hit target | On medication 65% Off medication 58% |
| Khanna & Carmena (2017) [32] | DBS EEG | STN Reinforce and inhibit 13–30 Hz | 5–15 m | 25–150 m | 1 | NA | A video game character (Mario) moved according to 13–30 Hz power | Not reported | Comparing actual performance over time to simulated performance over time to determine if actual performance exceeded distribution of chance simulated performance | 100% |
| Subramanian et al., (2011) [23] | fMRI | SMA reinforcement | 20 s | 13 m | 2 | 2–6 months | Thermometer (A vertical bar with height targets) | Motor imagery suggested | Statistically significant increase in SMA activity compared to baseline | 100% |
| Subramanian et al., (2016) [25] | fMRI | SMA reinforcement | 20 s | 12 min | 3 | 1–4 weeks | Thermometer (A vertical bar with height targets) | Motor imagery suggested | Positive “t” or “beta” value for the increase in SMA activity compared to baseline | Success rate for individuals not reported |
| Thompson & Thompson (2002) [31] | Scalp EEG | FCz-CPz or Cz Reinforce 13–15 Hz Inhibit 9–10 Hz Inhibit 25–32 Hz | Not reported | 50 m | 42 | 1 week | Not reported | Not reported | Not reported | Not reported |
| Tinaz et al., (2018) [29] | fMRI | Right insula-dorsomedial frontal cortex functional connectivity reinforcement | 8 s | 6.7–8 m | 2 | 1–2 weeks | A bar plot, where a blue bar indicated negative brain activity and a red bar indicated positive brain activity | Motor Imagery | Significant increase in brain connectivity of pre-post baseline scans | Success rate for individuals not reported |
| Author(s) (Date) | NF Type | Targeted Activity | Activity Direction | Clinical Outcome Improved? | NF Achieved? | Indicative * Support for NF Treatment? | Follow-Up? |
|---|---|---|---|---|---|---|---|
| Buyukturkoglu et al., (2013) [26] | fMRI | SMA | Reinforcement | No | Yes | No | No |
| Erikson-Davis et al., (2012) [24] | Scalp EEG | C3 & C4 8–15 Hz 4–8 Hz 23–34 Hz | Both suppression and reinforcement | No | Not reported | No | No |
| Fukama et al., (2018) [22] | DBS EEG | STN 13–30 Hz | Both suppression and reinforcement | No | Partially (75% successful) | No | No |
| Subramanian et al., (2011) [23] | fMRI | SMA activity | Reinforcement | Yes | Yes | Yes | No |
| Subramanian et al., (2016) [25] | fMRI | SMA activity | Reinforcement | Yes | Yes | Yes | No |
| Tinaz et al., (2018) [29] | fMRI | Right insula-dorsomedial frontal cortex functional connectivity | Reinforcement | Yes | Yes | Yes | No |
| No. | Section Name | Description | Reason for Suggestion |
|---|---|---|---|
| 7a | Sample Size | Sample size determination and/or calculations | No studies included a sample size calculation nor a justification for their recruitment sample size. |
| 12 | Statistical Methods and Additional Analysis | Statistical methods used for all outcome measures and any additional analysis | Many studies did not clearly report (or did not report at all) the statistical tests used nor the justification for these tests. Furthermore, many studies excluded vital information regarding means, standard deviations, error data, or p-values. |
| 13–18 | These sections all refer to results reporting | Beyond reporting outcomes measures, these sections also refer to important information such as participant flow, recruitment, baseline data, and sample size that was analysed | The results section of many studies excluded vital information needed for a meta-analysis and drawing a meaningful conclusion. Specifically, information regarding neurofeedback success rates are needed (e.g., individual success rates and success thresholds). |
| 19 | Harms | Any adverse events or unintended effects | Any treatment development must monitor side effects. No study reported this monitoring as part of their study process. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anil, K.; Hall, S.D.; Demain, S.; Freeman, J.A.; Ganis, G.; Marsden, J. A Systematic Review of Neurofeedback for the Management of Motor Symptoms in Parkinson’s Disease. Brain Sci. 2021, 11, 1292. https://doi.org/10.3390/brainsci11101292
Anil K, Hall SD, Demain S, Freeman JA, Ganis G, Marsden J. A Systematic Review of Neurofeedback for the Management of Motor Symptoms in Parkinson’s Disease. Brain Sciences. 2021; 11(10):1292. https://doi.org/10.3390/brainsci11101292
Chicago/Turabian StyleAnil, Krithika, Stephen D. Hall, Sara Demain, Jennifer A. Freeman, Giorgio Ganis, and Jonathan Marsden. 2021. "A Systematic Review of Neurofeedback for the Management of Motor Symptoms in Parkinson’s Disease" Brain Sciences 11, no. 10: 1292. https://doi.org/10.3390/brainsci11101292