
Anticipatory Motor Planning and Control of Grasp in Children with Unilateral Spastic Cerebral Palsy

 and
and
Abstract
:1. Introduction
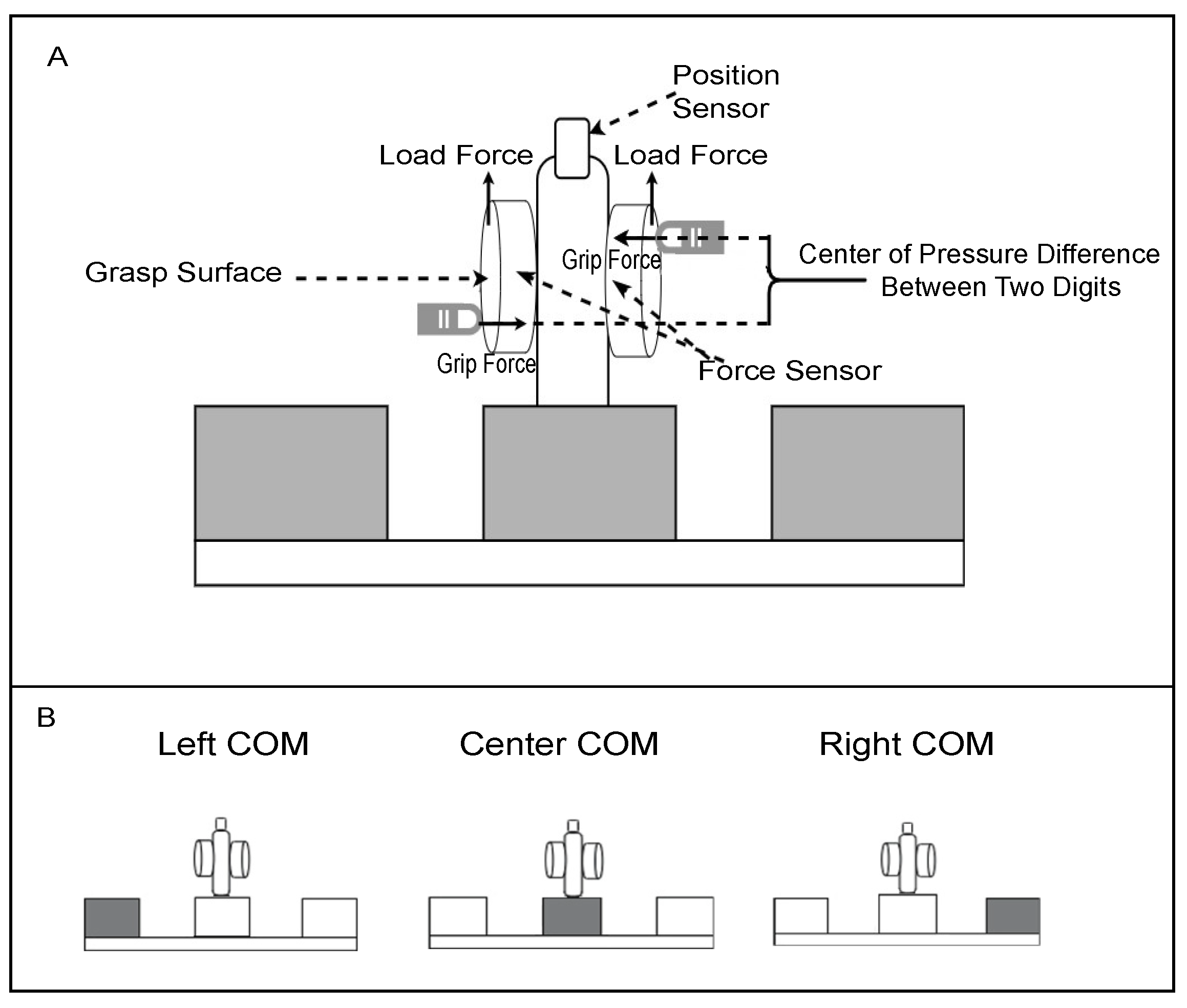
2. Materials and Methods
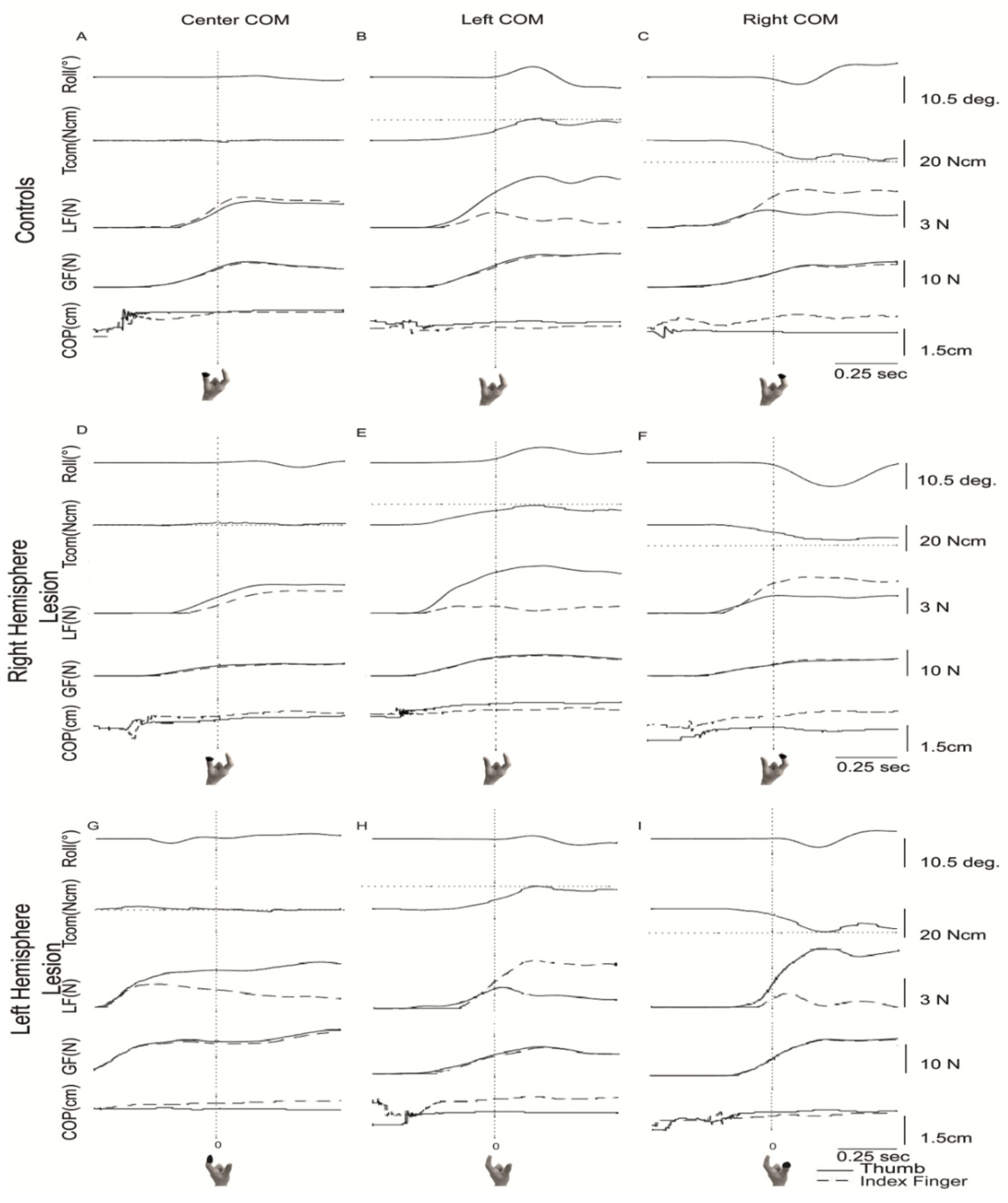
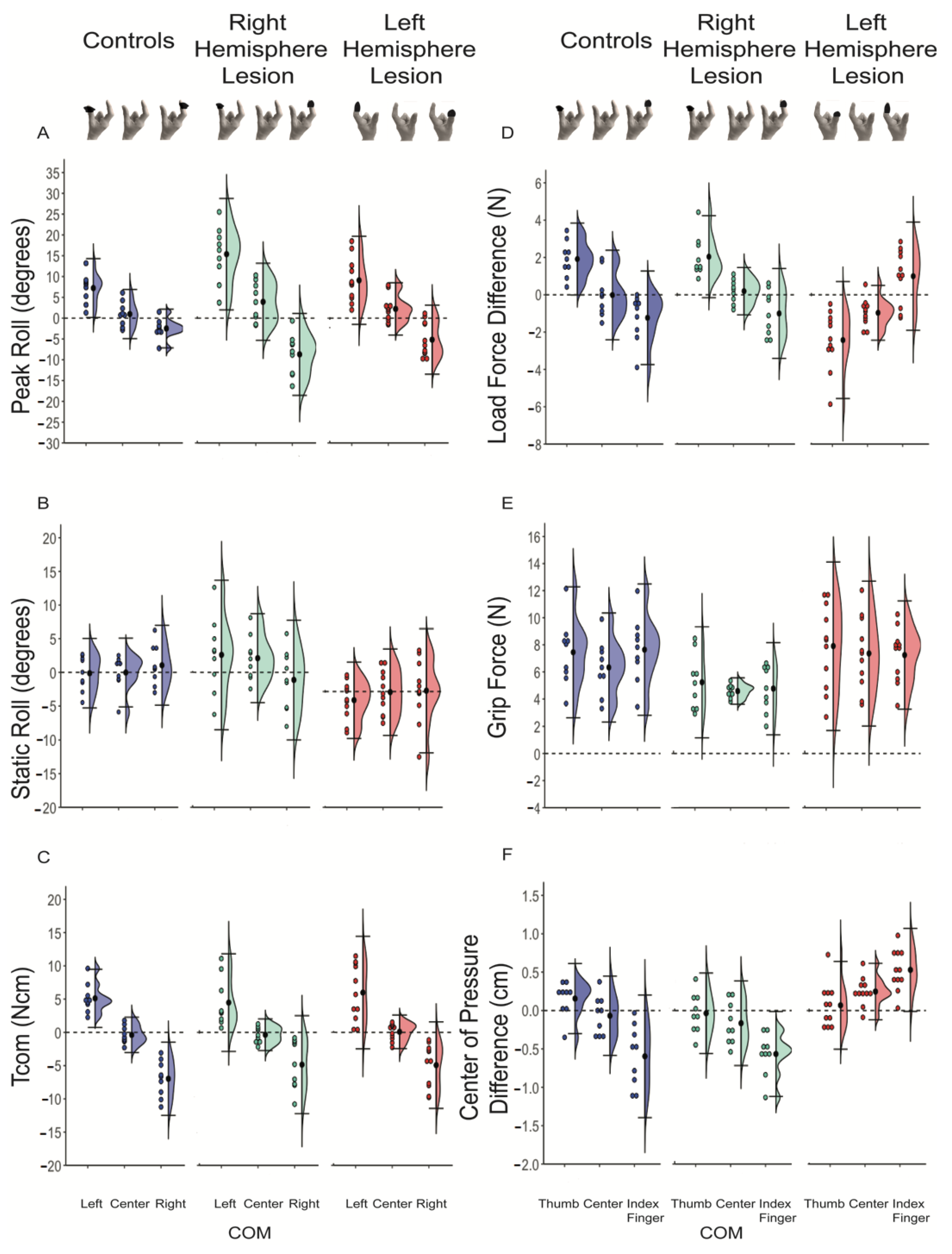
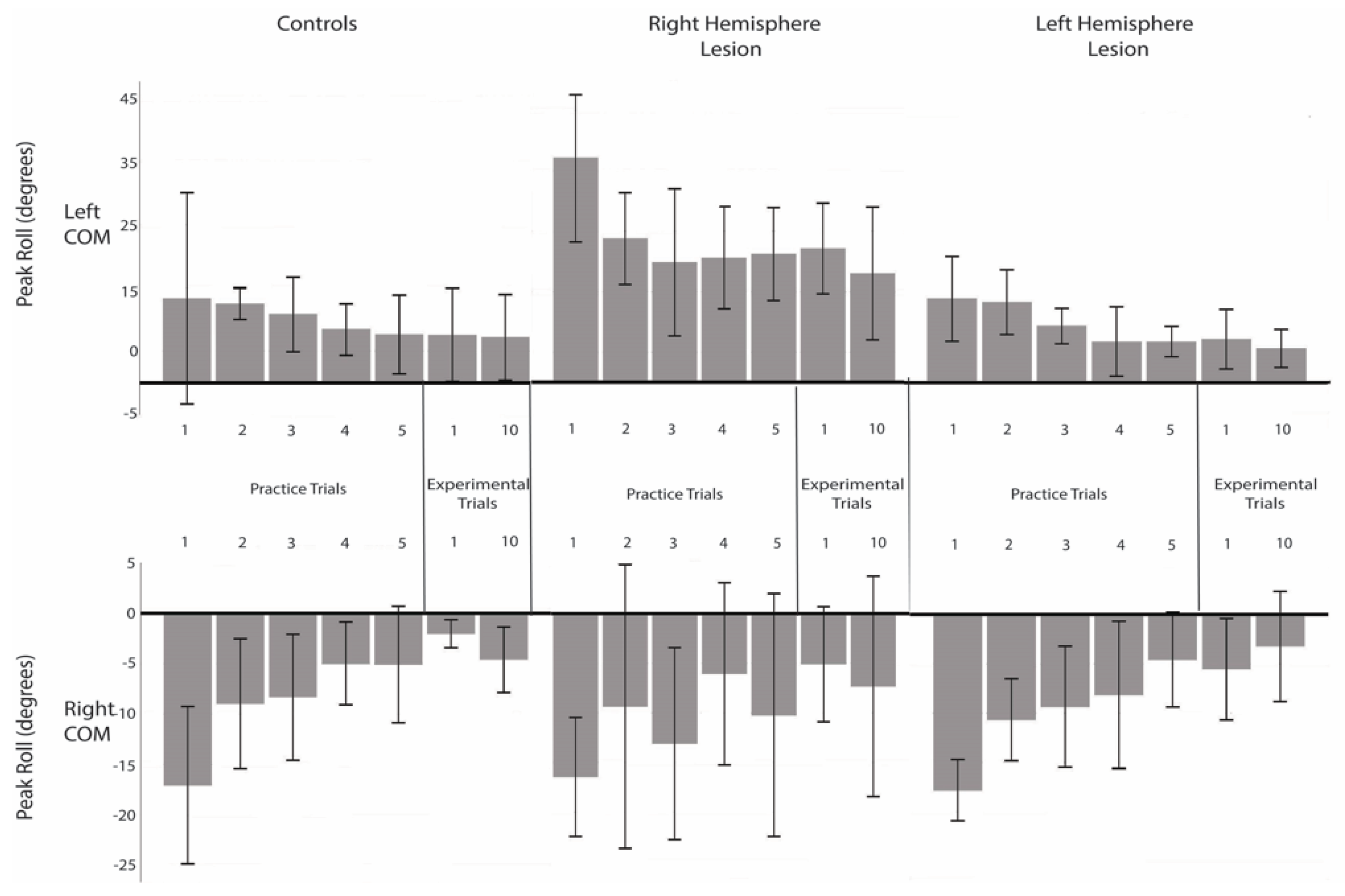
- Peak object roll—recorded within 500 ms after lift onset (lift-off), the angle of the object in the frontal plane. Positive values for peak object roll signify a counterclockwise roll (towards the left) and negative values signify a clockwise roll (towards the right).
- Peak velocity of roll = peak object speed and direction of the rotation of the object during the initial roll of the object.
- Static roll = the degree the initial roll had been corrected at mid-lift.
- Load force (LF)—vertical component of the force counteracting weight and inertia produced by each digit at lift-off.
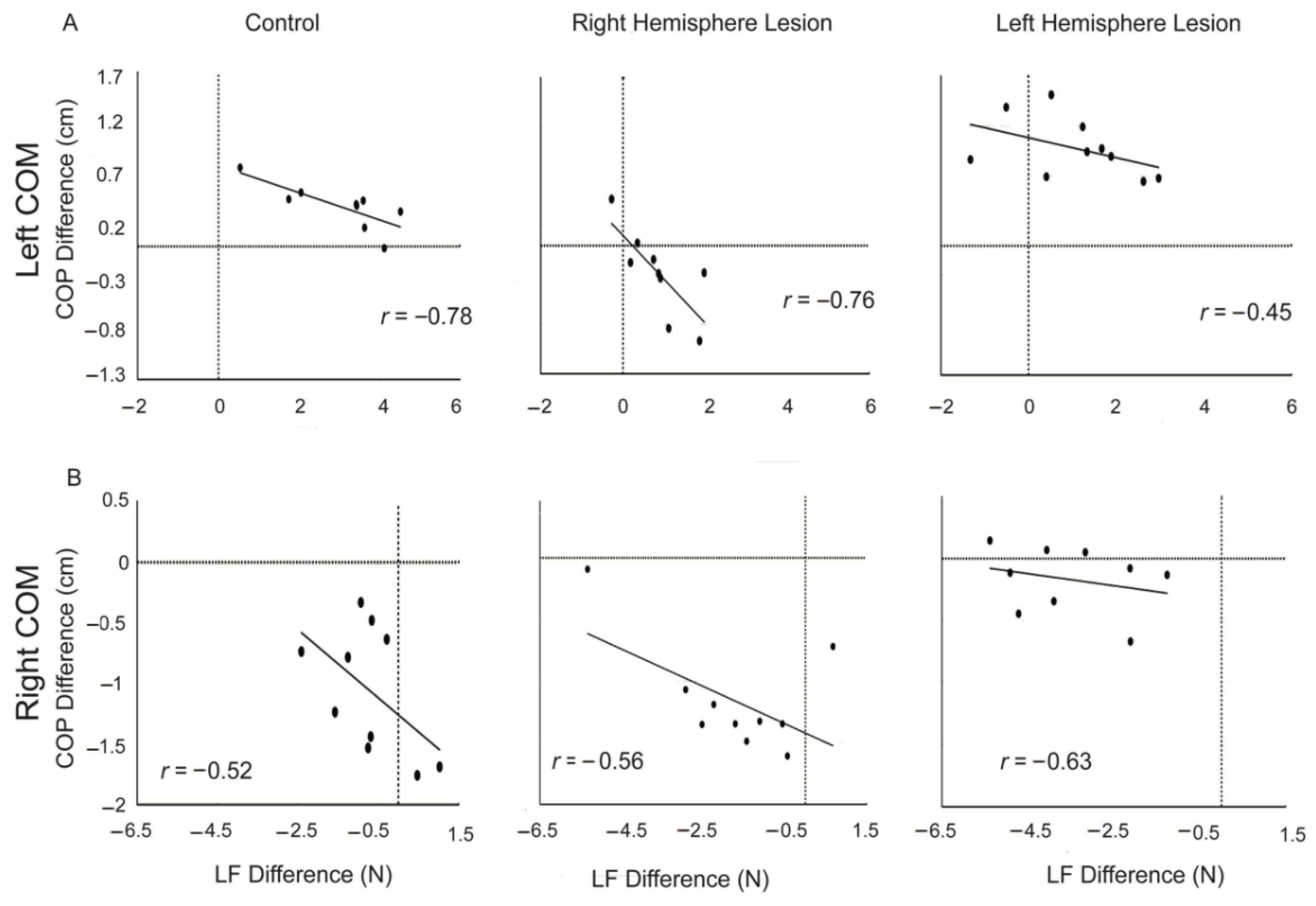
- Load force difference (LF Difference) = LF left − LF right. Positive values indicate larger LF from the digit on the left grip surface, whereas negative values indicate larger LF from the digit on the right grip surface.
- Grip Force (GF)—average normal (perpendicular to the grip surface) component of the force produced by each digit at lift-off.
- Center of pressure (COP)—vertical coordinate of the point of application of the digit on the grip surface, measured in (cm) at lift-off, signaling digit position.
- Center of pressure difference (COP Difference) = COP left − COP right. Positive values indicate higher left digit than right digit COP, whereas negative values indicate higher right digit than left digit COP.
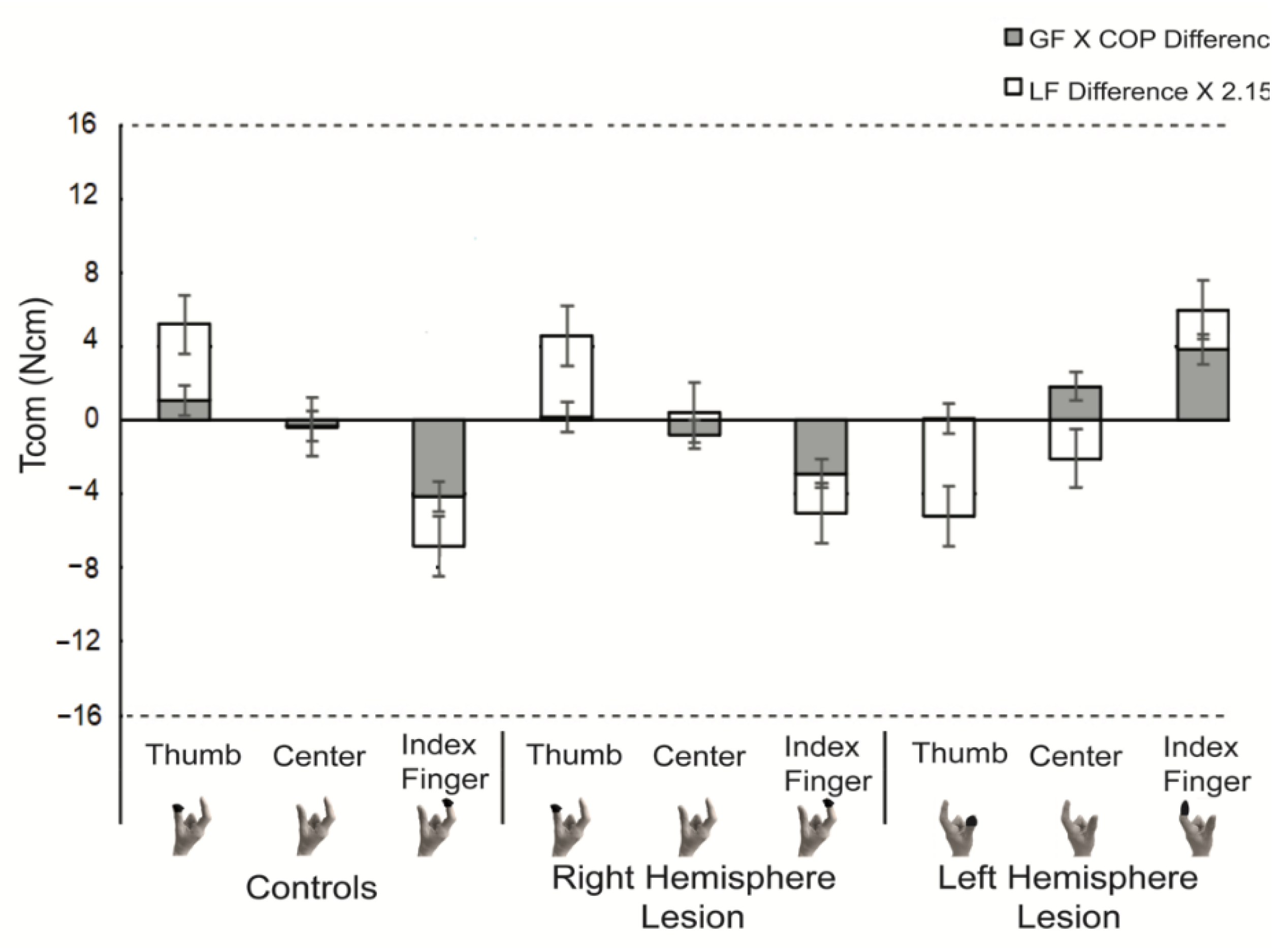
- Compensatory torque (Tcom)—anticipatory torque generated by the digits, in response to object torque, at lift-off. A positive Tcom signifies a clockwise torque, while a negative Tcom signifies a counter-clockwise torque.
- Where half of grip width was 2.15 cm.
- Object torque was ±16 Ncm.
3. Results
3.1. Peak Object Roll and Compensatory Torque
3.2. Components of Compensatory Torque
3.3. Relationship and Discrepancy between Object Roll and Tcom
3.4. Covariation of Digit Forces and Placement
4. Discussion
4.1. Children with USCP Have Anticipatory Control of Digit Forces and Torque
4.2. Children with USCP Demonstrated a Maladaptive Digit Placement Strategy
4.3. Lesion Side Influenced the Ability to Minimize Peak Roll
4.4. Covariation of Digit Placement and Forces in Order to Achieve Tcom
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Crajé, C.; Aarts, P.; Nijhuis-van der Sanden, M.; Steenbergen, B. Action planning in typically and atypically developing children (unilateral cerebral palsy). Res. Dev. Disabil. 2010, 31, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, B.; Jongbloed-Pereboom, M.; Spruijt, S.; Gordon, A.M. Impaired motor planning and motor imagery in children with unilateral spastic cerebral palsy: Challenges for the future of pediatric rehabilitation. Dev. Med. child Neurol. 2013, 55 (Suppl. 4), 43–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lust, J.M.; Spruijt, S.; Wilson, P.H.; Steenbergen, B. Motor planning in children with cerebral palsy: A longitudinal perspective. J. Clin. Exp. Neuropsychol. 2018, 40, 559–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbaum, D.A.; Marchak, F.; Barnes, H.J.; Vaughan, J.; Slotta, J.D.; Jorgensen, M.J. Constraints for action selection: Overhand versus underhand grips. In Attention and Performance 13: Motor Representation and Control; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1990; pp. 321–342. [Google Scholar]
- Mutsaarts, M.; Steenbergen, B.; Bekkering, H. Anticipatory planning deficits and task context effects in hemiparetic cerebral palsy. Exp. Brain Res. 2006, 172, 151–162. [Google Scholar] [CrossRef]
- Janssen, L.; Steenbergen, B. Typical and atypical (cerebral palsy) development of unimanual and bimanual grasp planning. Res. Dev. Disabil. 2011, 32, 963–971. [Google Scholar] [CrossRef]
- Martinie, O.; Mercier, C.; Gordon, A.M.; Robert, M.T. Upper Limb Motor Planning in Individuals with Cerebral Palsy Aged between 3 and 21 Years Old: A Systematic Review. Brain Sci. 2021, 11, 920. [Google Scholar] [CrossRef] [PubMed]
- Forssberg, H.; Kinoshita, H.; Eliasson, A.C.; Johansson, R.S.; Westling, G.; Gordon, A.M. Development of human precision grip. Exp. Brain Res. 1992, 90, 393–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, A.M.; Forssberg, H.; Johansson, R.S.; Eliasson, A.C.; Westling, G. Development of human precision grip. III. Integration of visual size cues during the programming of isometric forces. Exp. Brain Res. 1992, 90, 399–403. [Google Scholar] [CrossRef]
- Gordon, A.M. Chapter 3 Development of the Reach to Grasp Movement. In Advances in Psychology; Bennett, K.M.B., Castiello, U., Eds.; North-Holland: Amsterdam, The Netherlands, 1994; Volume 105, pp. 37–56. [Google Scholar]
- Johansson, R.S.; Westling, G. Coordinated isometric muscle commands adequately and erroneously programmed for the weight during lifting task with precision grip. Exp. Brain Res. 1988, 71, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.M.; Westling, G.; Cole, K.J.; Johansson, R.S. Memory representations underlying motor commands used during manipulation of common and novel objects. J. Neurophysiol. 1993, 69, 1789–1796. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Gordon, A.M.; Forssberg, H. Impaired anticipatory control of isometric forces during grasping by children with cerebral palsy. Dev. Med. Child Neurol. 1992, 34, 216–225. [Google Scholar] [CrossRef]
- Duff, S.V.; Gordon, A.M. Learning of grasp control in children with hemiplegic cerebral palsy. Dev. Med. Child Neurol. 2003, 45, 746–757. [Google Scholar] [CrossRef]
- Gordon, A.M.; Duff, S.V. Fingertip forces during object manipulation in children with hemiplegic cerebral palsy. I: Anticipatory scaling. Dev. Med. Child Neurol. 1999, 41, 166–175. [Google Scholar] [CrossRef]
- Bleyenheuft, Y.; Thonnard, J.-L. Predictive and Reactive Control of Precision Grip in Children With Congenital Hemiplegia. Neurorehabilit. Neural Repair 2010, 24, 318–327. [Google Scholar] [CrossRef]
- Gordon, A.M.; Charles, J.; Duff, S.V. Fingertip forces during object manipulation in children with hemiplegic cerebral palsy. II: Bilateral coordination. Dev. Med. Child Neurol. 1999, 41, 176–185. [Google Scholar] [CrossRef]
- Fu, Q.; Zhang, W.; Santello, M. Anticipatory Planning and Control of Grasp Positions and Forces for Dexterous Two-Digit Manipulation. J. Neurosci. 2010, 30, 9117. [Google Scholar] [CrossRef] [Green Version]
- Salimi, I.; Hollender, I.; Frazier, W.; Gordon, A.M. Specificity of Internal Representations Underlying Grasping. J. Neurophysiol. 2000, 84, 2390–2397. [Google Scholar] [CrossRef]
- Zhang, W.; Gordon, A.M.; Fu, Q.; Santello, M. Manipulation After Object Rotation Reveals Independent Sensorimotor Memory Representations of Digit Positions and Forces. J. Neurophysiol. 2010, 103, 2953–2964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Q.; Marco, S. Coordination between Digit Forces and Positions: Interactions between Anticipatory and Feedback Control. J. Neurophysiol. 2014, 111, 1519–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernstein, N.A. The co-ordination and regulation of movements; Pergamon Press: Oxford, UK, 1967. [Google Scholar]
- Steenbergen, B.; Meulenbroek, R.G.; Rosenbaum, D.A. Constraints on grip selection in hemiparetic cerebral palsy: Effects of lesional side, end-point accuracy, and context. Brain Res. Cogn. Brain Res. 2004, 19, 145–159. [Google Scholar] [CrossRef] [PubMed]
- Crajé, C.; van der Kamp, J.; Steenbergen, B. Visual information for action planning in left and right congenital hemiparesis. Brain Res. 2009, 1261, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, E.V.; Pearse, J.E.; Eyre, J.A.; Basu, A.P. Motor planning ability is not related to lesion side or functional manual ability in children with hemiplegic cerebral palsy. Exp. Brain Res. 2013, 231, 239–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajenbrink, H.; Crichton, A.; Steenbergen, B.; Hoare, B. The development of anticipatory action planning in children with unilateral cerebral palsy. Res. Dev. Disabil. 2019, 85, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Gordon, A.M.; Charles, J.; Steenbergen, B. Steenbergen. Fingertip Force Planning During Grasp Is Disrupted by Impaired Sensorimotor Integration in Children with Hemiplegic Cerebral Palsy. Pediatr. Res. 2006, 60, 587–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukos, J.R.; Ansuini, C.; Santello, M. Anticipatory Control of Grasping: Independence of Sensorimotor Memories for Kinematics and Kinetics. J. Neurosci. 2008, 28, 12765–12774. [Google Scholar] [CrossRef] [Green Version]
- Kamp, J.; Steenbergen, B.; Masters, R. Explicit and implicit motor learning in children with unilateral cerebral palsy. Disabil. Rehabil. 2017, 40, 1–8. [Google Scholar] [CrossRef]
- Steenbergen, B.; van der Kamp, J.; Verneau, M.; Jongbloed-Pereboom, M.; Masters, R.S. Implicit and explicit learning: Applications from basic research to sports for individuals with impaired movement dynamics. Disabil. Rehabil. 2010, 32, 1509–1516. [Google Scholar] [CrossRef]
- Marneweck, M.; Lee-Miller, T.; Santello, M.; Gordon, A.M. Digit Position and Forces Covary during Anticipatory Control of Whole-Hand Manipulation. Front. Hum. Neurosci. 2016, 10, 461. [Google Scholar] [CrossRef] [Green Version]
- Lukos, J.; Ansuini, C.; Santello, M. Choice of Contact Points during Multidigit Grasping: Effect of Predictability of Object Center of Mass Location. J. Neurosci. 2007, 27, 3894–3903. [Google Scholar] [CrossRef] [Green Version]
- Mutha, P.K.; Haaland, K.Y.; Sainburg, R.L. The effects of brain lateralization on motor control and adaptation. J. Mot. Behav. 2012, 44, 455–469. [Google Scholar] [CrossRef]
- Ogden, J.A. Anterior-posterior interhemispheric differences in the loci of lesions producing visual hemineglect. Brain Cogn. 1985, 4, 59–75. [Google Scholar] [CrossRef]
- Ickx, G.; Hatem, S.M.; Riquelme, I.; Friel, K.M.; Henne, C.; Araneda, R.; Gordon, A.M.; Bleyenheuft, Y. Impairments of Visuospatial Attention in Children with Unilateral Spastic Cerebral Palsy. Neural Plast. 2018, 2018, 1435808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee-Miller, T.; Santello, M.; Gordon, A.M. Hand forces and placement are modulated and covary during anticipatory control of bimanual manipulation. J. Neurophysiol. 2019, 121, 2276–2290. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Demographic and Clinical Characteristics | Children with USCP (Left Hemisphere Lesion) (n = 11) | Children with USCP (Right Hemisphere Lesion) (n = 9) | Control Group (n = 9) |
|---|---|---|---|
| Age, years | 12.45 ± 2.30 | 11.33 ± 2.35 | 11.29 ± 2.56 |
| Gender, females | 4 (36.4%) | 7 (77.8%) | 7 (77.8%) |
| MACS Score | |||
| I | 4 (36.4%) | 3 (33.3%) | N/A |
| II | 4 (36.4%) | 6 (54.5%) | N/A |
| III | 3 (27.3%) | 0 (0%) | N/A |
| Jebsen Score | 41 ± 67.45 | 43.97 ± 298.30 | N/A |
| Main Variables | Left COM | Center COM | Right COM | Group Effect F, p Value (ηp2) | COM Effect F, p Value (ηp2) | Interaction F, p Value (ηp2) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C | RHL | LHL | C | RHL | LHL | C | RHL | LHL | ||||
| Peak Roll (degrees) | 7.24 ± 3.54 | 15.38 ± 6.70 | 9.09 ± 5.30 | 0.98 ± 2.96 | 3.93 ± 4.63 | 2.22 ± 3.14 | −2.99 ± 2.59 | −8.71 ± 4.92 | −5.18 ± 4.15 | – | – | F(2.78,36.18) = 6.03, p < 0.01(0.32) |
| Tcom (Ncm) | 4.31 (3.82, 5.70) | 3.13 (1.80, 7.95) | 5.34 (2.69, 11.00) | −0.98 (−1.36, 0.65) | −0.39 (−1.56, 0.53) | −0.71 (−1.40, 1.09) | −6.53 (−10.00, −4.38) | −4.12 (−8.28, −1.02) | −3.91 (−7.40, −1.68) | LCM: p = 0.594 CCM: p = 0.903 RCM: p = 0.168 | C: χ2 (2) = 18.00, p < 0.001 RHL: χ2 (2) = 16.22, p < 0.001 LHL: χ2 (2) =20.18, p < 0.001 | – |
| LF Diff (N) | 1.91 ± 0.96 | 2.04 ± 1.10 | 1.00 ± 1.45 | −0.01 ± 1.20 | 0.19 ± 0.63 | −1.00 ± 0.73 | −1.23 ± 1.25 | −1.00 ± 1.20 | −2.43 ± 1.57 | F(2,26) =7.72, p < 0.01 (0.37) | F(1.38, 35.94) = 61.51, p < 0.001 (0.70) | F(2.77,35.95) = 0.09, p = 0.97 (0.01) |
| GF (N) | 7.62 (5.76, 8.37) | 4.99 (3.59, 7.20) | 7.89 (5.89, 8.23) | 6.20 (4.72, 7.77) | 5.09 (4.29, 5.23) | 7.29 (4.87, 8.81) | 8.09 (6.40, 9.12) | 4.69 (3.05, 6.48) | 8.53 (4.83, 11.11) | LCM: p = 0.14 CCM: p = 0.06 RCM: p = 0.02 | C: χ2 (2) = 6.89, p = 0.03 RHL: χ2 (2) = 0.22, p = 0.90 LHL: χ2 (2) = 2.18, p = 0.34 | – |
| COP Diff (cm) | 0.16 ± 0.23 | −0.04 ± 0.26 | 0.53 ± 0.27 | −0.07 ± 0.26 | −0.17 ± 0.28 | 0.25 ± 0.18 | −0.60 ± 0.40 | −0.57 ± 0.28 | 0.07 ± 0.29 | F(2, 26) = 22.15, p < 0.001 (0.63) | F(2,25) = 31.37, p < 0.001 (0.72) | F(4,50) = 2.02, p = 0.106 (0.14) |
| Peak Velocity of Roll | 51.73 ± 18.64 | 86.90 ± 39.82 | 63.46 ± 31.61 | 8.25 ± 24.71 | 30.05 ± 29.40 | 22.97 ± 22.40 | −24.13 ± 14.82 | −60.16 ± 30.32 | −39.15 ± 32.84 | – | – | (F(2.90, 37.69) = 3.64, p = 0.02 (0.22) |
| Static Roll | −0.13 ± 2.59 | 2.60 ± 5.54 | −1.12 ± 2.47 | −0.03 ± 2.56 | 2.11 ± 3.30 | −0.06 ± 2.80 | 1.06 ± 3.00 | −1.12 ± 4.43 | 0.11 ± 4.02 | – | – | F(3.00,38.91) = 2.89, p < 0.05 (0.18) |
| Time to Peak Roll | 0.24 ± 0.07 | 0.27 ± 0.07 | 0.18 ± 0.08 | 0.18 ± 0.04 | 0.20 ± 0.04 | 0.18 ± 0.05 | 0.23 ± 0.07 | 0.46 ± 0.71 | 0.22 ± 0.06 | F(2,26) = 1.82, p > 0.18 (0.12) | F(1.04, 26.93) = 2.02, p = 0.17 (0.07) | F(2.07, 26.93) = 0.83, p = 0.45 (0.06) |
| COP diff X GF | 1.07 ± 1.81 | 0.18 ± 1.61 | 3.85 ± 2.13 | −0.33 ± 1.52 | −0.78 ± 1.30 | 1.83 ± 1.21 | −4.17 ± 2.67 | −2.89 ± 2.10 | 0.10 ± 1.84 | F(2,26) = 20.48 p < 0.001 (0.61) | F(1.59,41.22) = 43.44, p < 0.001 (0.63) | F(3.17,41.22) = 5.43, p = 0.21 (0.11) |
| Left COM | Center COM | Right COM | Overall | |
|---|---|---|---|---|
| Correlation between Tcom and peak roll | ||||
| Controls | −0.60 | −0.67 | −0.70 | −0.62 |
| Right Hemisphere Lesion | −0.59 | −0.58 | −0.29 | −0.50 |
| Left Hemisphere Lesion | −0.68 | −0.54 | −0.41 | −0.55 |
| Covariation between LF difference and COP difference | ||||
| Controls | −0.69 | −0.77 | −0.47 | −0.79 |
| Right Hemisphere Lesion | −0.57 | −0.81 | −0.49 | −0.65 |
| Left Hemisphere Lesion | −0.53 | −0.82 | −0.68 | −0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutterman, J.; Lee-Miller, T.; Friel, K.M.; Dimitropoulou, K.; Gordon, A.M. Anticipatory Motor Planning and Control of Grasp in Children with Unilateral Spastic Cerebral Palsy. Brain Sci. 2021, 11, 1161. https://doi.org/10.3390/brainsci11091161
Gutterman J, Lee-Miller T, Friel KM, Dimitropoulou K, Gordon AM. Anticipatory Motor Planning and Control of Grasp in Children with Unilateral Spastic Cerebral Palsy. Brain Sciences. 2021; 11(9):1161. https://doi.org/10.3390/brainsci11091161
Chicago/Turabian StyleGutterman, Jennifer, Trevor Lee-Miller, Kathleen M. Friel, Katherine Dimitropoulou, and Andrew M. Gordon. 2021. "Anticipatory Motor Planning and Control of Grasp in Children with Unilateral Spastic Cerebral Palsy" Brain Sciences 11, no. 9: 1161. https://doi.org/10.3390/brainsci11091161