
Changes in Default Mode Network Connectivity in Resting-State fMRI in People with Mild Dementia Receiving Cognitive Stimulation Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessments and Procedures
2.3. Magnetic Resonance Imaging (MRI) Data Acquisition and Preprocessing
2.4. Data Analyses
3. Results
3.1. Demographics, Cognitive Reserve Proxies, and Neuropsychological Profile
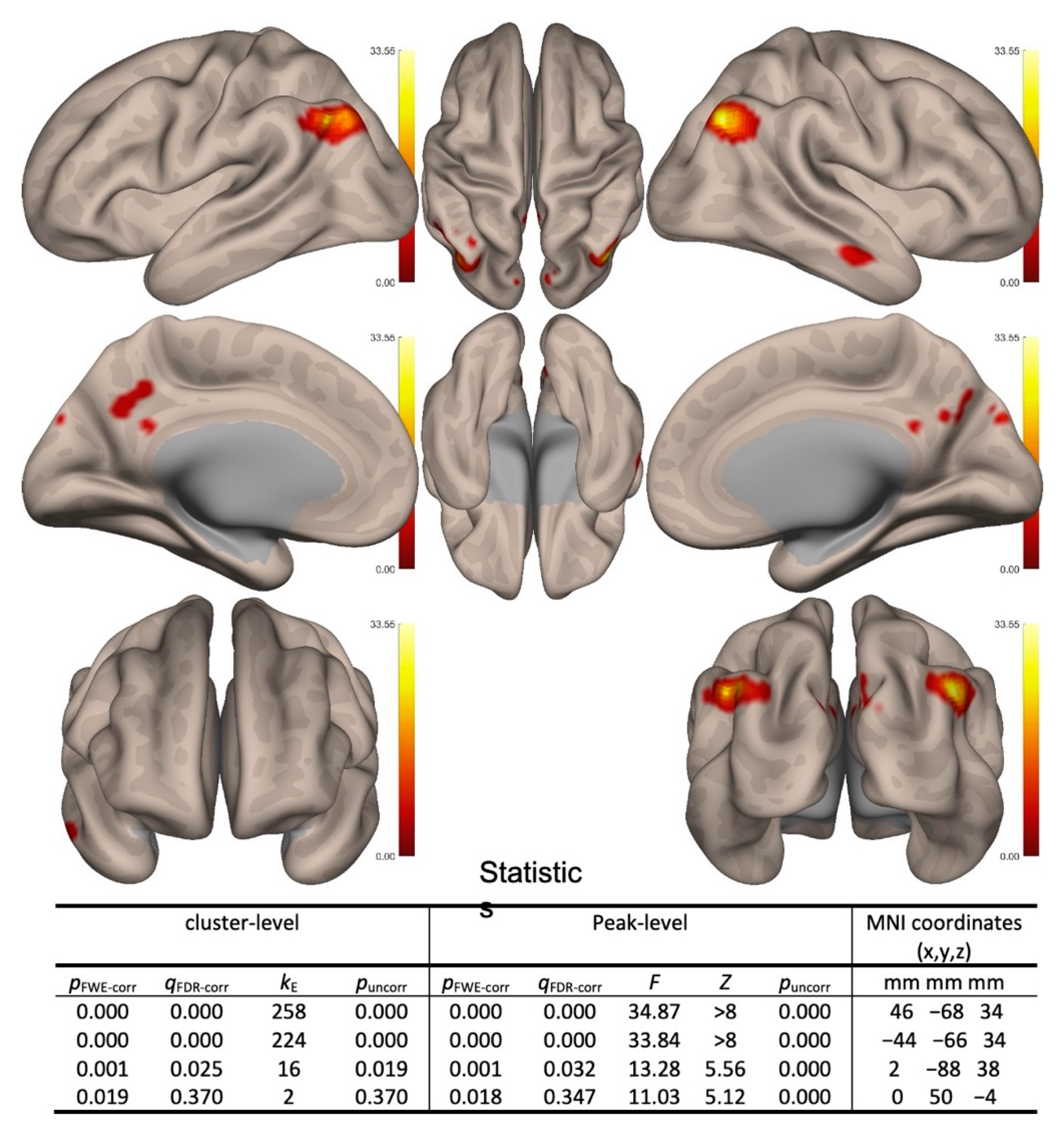
3.2. Within-Subject Changes
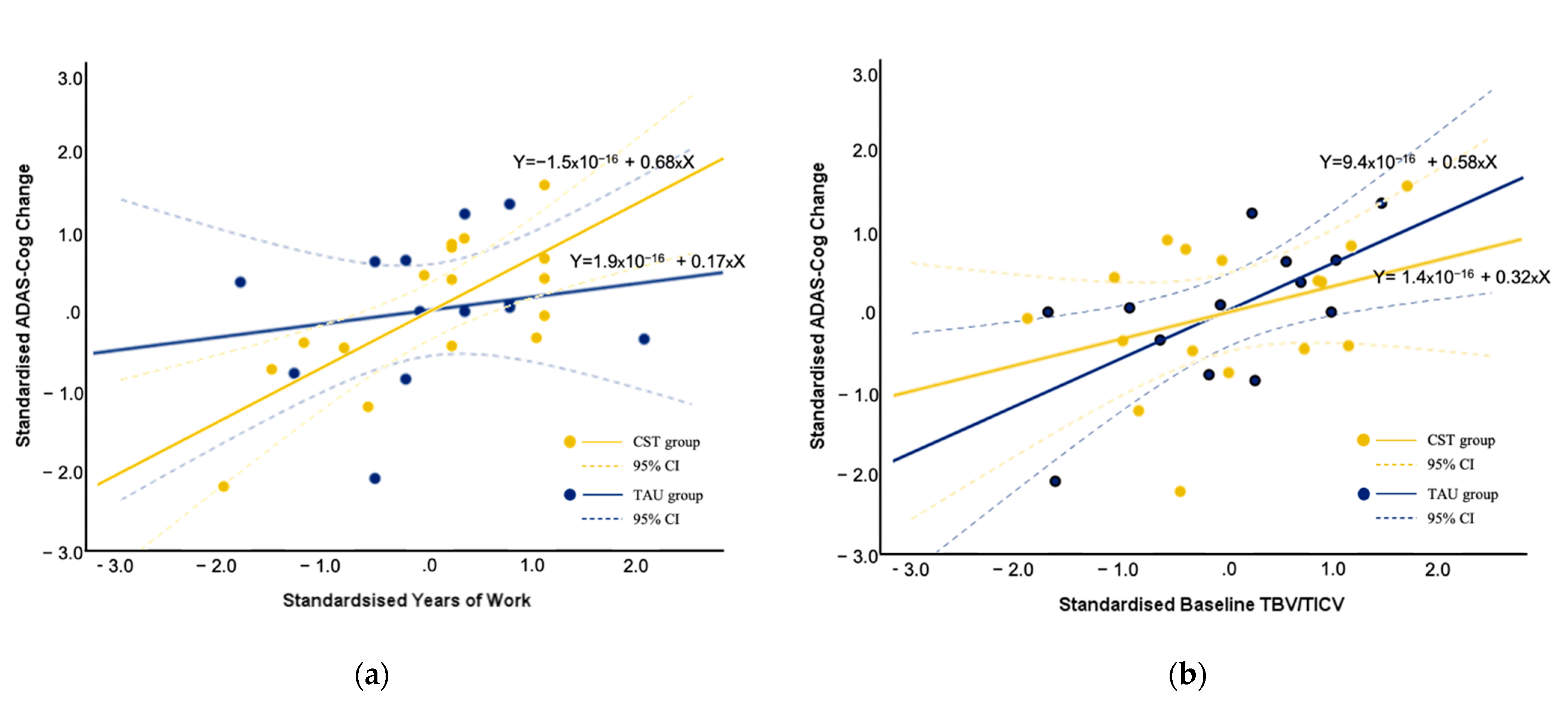
3.3. Predictors of Cognitive Changes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016: Improving Healthcare for Poeple Living with Dementia; Alzheimer’s Disease International: London, UK, 2016. [Google Scholar]
- Wong, G.; Knapp, M. Should we move dementia research funding from a cure to its care? Expert Rev. Neurother. 2020, 20, 303–305. [Google Scholar] [CrossRef] [Green Version]
- NICE. Dementia: Assessment, Management and Support for People Living with Dementia and their Carers; The National Institute for Health and Care Excellence (NICE): London, UK, 2018. [Google Scholar]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD005562. [Google Scholar] [CrossRef] [PubMed]
- Huntley, J.D.; Gould, R.L.; Liu, K.; Smith, M.; Howard, R.J. Do cognitive interventions improve general cognition in dementia? A meta-analysis and meta-regression. BMJ Open 2015, 5, e005247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spector, A.; Thorgrimsen, L.; Woods, B.; Royan, L.; Davies, S.; Butterworth, M.; Orrell, M. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: Randomised controlled trial. Br. J. Psychiatry 2003, 183, 248–254. [Google Scholar] [CrossRef]
- Spector, A.; Orrell, M. Using a biopsychosocial model of dementia as a tool to guide clinical practice. Int. Psychogeriatr. 2010, 22, 957–965. [Google Scholar] [CrossRef]
- Spector, A.; Orrell, M.; Woods, B. Cognitive Stimulation Therapy (CST): Effects on different areas of cognitive function for people with dementia. Int. J. Geriatr. Psychiatry 2010, 25, 1253–1258. [Google Scholar] [CrossRef]
- Lobbia, A.; Carbone, E.; Faggian, S.; Gardini, S.; Piras, F.; Spector, A.; Borella, E. The efficacy of cognitive stimulation therapy (CST) for people with mild-to-moderate dementia. Eur. Psychol. 2018, 24, 257–277. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, K.; Poo, M.M. Activity-dependent neural plasticity from bench to bedside. Neuron 2013, 80, 729–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassett, D.S.; Wymbs, N.F.; Porter, M.A.; Mucha, P.J.; Carlson, J.M.; Grafton, S.T. Dynamic reconfiguration of human brain networks during learning. Proc. Natl. Acad. Sci. USA 2011, 108, 7641–7646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The brain’s default network: Anatomy, function, and relevance to disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef] [Green Version]
- Greicius, M.D.; Krasnow, B.; Reiss, A.L.; Menon, V. Functional connectivity in the resting brain: A network analysis of the default mode hypothesis. Proc. Natl. Acad. Sci. USA 2003, 100, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Greicius, M.D.; Supekar, K.; Menon, V.; Dougherty, R.F. Resting-state functional connectivity reflects structural connectivity in the default mode network. Cereb. Cortex 2009, 19, 72–78. [Google Scholar] [CrossRef]
- Bullmore, E.; Sporns, O. The economy of brain network organization. Nat. Rev. Neurosci. 2012, 13, 336–349. [Google Scholar] [CrossRef]
- Raichle, M.E.; MacLeod, A.M.; Snyder, A.Z.; Powers, W.J.; Gusnard, D.A.; Shulman, G.L. A default mode of brain function. Proc. Natl. Acad. Sci. USA 2001, 98, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Buckner, R.L.; Snyder, A.Z.; Shannon, B.J.; LaRossa, G.; Sachs, R.; Fotenos, A.F.; Sheline, Y.I.; Klunk, W.E.; Mathis, C.A.; Morris, J.C.; et al. Molecular, structural, and functional characterization of Alzheimer’s disease: Evidence for a relationship between default activity, amyloid, and memory. J. Neurosci. 2005, 25, 7709–7717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bressler, S.L.; Menon, V. Large-scale brain networks in cognition: Emerging methods and principles. Trends Cogn. Sci. 2010, 14, 277–290. [Google Scholar] [CrossRef]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef] [PubMed]
- Fransson, P. Spontaneous low-frequency BOLD signal fluctuations: An fMRI investigation of the resting-state default mode of brain function hypothesis. Hum. Brain Mapp. 2005, 26, 15–29. [Google Scholar] [CrossRef]
- Grady, C.L.; McIntosh, A.R.; Beig, S.; Keightley, M.L.; Burian, H.; Black, S.E. Evidence from functional neuroimaging of a compensatory prefrontal network in Alzheimer’s disease. J. Neurosci. 2003, 23, 986–993. [Google Scholar] [CrossRef] [Green Version]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Ferstl, E.C.; Neumann, J.; Bogler, C.; von Cramon, D.Y. The extended language network: A meta-analysis of neuroimaging studies on text comprehension. Hum. Brain Mapp. 2008, 29, 581–593. [Google Scholar] [CrossRef] [Green Version]
- De Luca, M.; Beckmann, C.F.; De Stefano, N.; Matthews, P.M.; Smith, S.M. fMRI resting state networks define distinct modes of long-distance interactions in the human brain. Neuroimage 2006, 29, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Ferre, P.; Benhajali, Y.; Steffener, J.; Stern, Y.; Joanette, Y.; Bellec, P. Resting-state and Vocabulary Tasks Distinctively Inform On Age-Related Differences in the Functional Brain Connectome. Lang. Cogn. Neurosci. 2019, 34, 949–972. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Gud, Y.; Dong, W.; Zhao, M.; Tiana, J.; Suna, T.; Yua, X.; Ouyang, G.; Wanga, H. Lower small-worldness of intrinsic brain networks facilitates the cognitive protection of intellectual engagement in elderly people without dementia: A near-infrared spectroscopy study. Am. J. Geriatr. Psychiatry 2020, 28, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Cao, X.; Hou, C.; Li, T.; Cheng, Y.; Jiang, L.; Luo, C.; Li, C.; Yao, D. Effects of Cognitive Training on Resting-State Functional Connectivity of Default Mode, Salience, and Central Executive Networks. Front. Aging Neurosci. 2016, 8, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.T.Y.; Au, A.C.L.; Wong, G.H.Y. Neuropsychological understanding of CST. In Cognitive Stimulation Therapy for Dementia: History, Evolution and Internationalism; Yates, L.A., Yates, J., Orrell, M., Spector, A., Woods, B., Eds.; Routledge: London, UK, 2018. [Google Scholar]
- Chiu, H.F.K.; Lee, H.C.; Chung, W.S.; Kwong, P.K. Reliability and validity of the Cantonese version of Mini-Mental State Examination—A preliminary study. East Asian Arch. Psychiatry 1994, 4, 25–28. [Google Scholar]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Wong, G.H.Y. CST for Hong Kong Chinese: Cultural adaption and mechanisms of change. In Proceedings of the Cognitive Stimulation Therapy (CST) for Dementia: An International Perspective, London, UK, 10 July 2015. [Google Scholar]
- Rosen, W.G.; Mohs, R.C.; Davis, K.L. A new rating scale for Alzheimer’s disease. Am. J. Psychiatry 1984, 141, 1356–1364. [Google Scholar] [PubMed]
- Alexopoulos, G.S.; Abrams, R.C.; Young, R.C.; Shamoian, C.A. Cornell Scale for Depression in Dementia. Biol. Psychiatry 1988, 23, 271–284. [Google Scholar] [CrossRef]
- Holden, U.P.; Woods, R.T. Positive Approaches to Dementia Care, 3rd ed.; Churchill Livingstone: Edinburgh, UK, 1995. [Google Scholar]
- Ashburner, J.; Friston, K.J. Unified segmentation. Neuroimage 2005, 26, 839–851. [Google Scholar] [CrossRef]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef] [Green Version]
- Behzadi, Y.; Restom, K.; Liau, J.; Liu, T.T. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage 2007, 37, 90–101. [Google Scholar] [CrossRef] [Green Version]
- Friston, K.J.; Williams, S.; Howard, R.; Frackowiak, R.S.; Turner, R. Movement-related effects in fMRI time-series. Magn. Reson. Med. 1996, 35, 346–355. [Google Scholar] [CrossRef]
- Power, J.D.; Mitra, A.; Laumann, T.O.; Snyder, A.Z.; Schlaggar, B.L.; Petersen, S.E. Methods to detect, characterize, and remove motion artifact in resting state fMRI. Neuroimage 2014, 84, 320–341. [Google Scholar] [CrossRef] [PubMed]
- Chai, X.J.; Castanon, A.N.; Ongur, D.; Whitfield-Gabrieli, S. Anticorrelations in resting state networks without global signal regression. Neuroimage 2012, 59, 1420–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissenbacher, A.; Kasess, C.; Gerstl, F.; Lanzenberger, R.; Moser, E.; Windischberger, C. Correlations and anticorrelations in resting-state functional connectivity MRI: A quantitative comparison of preprocessing strategies. Neuroimage 2009, 47, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Ashburner, J.; Friston, K.J. Voxel-based morphometry—The methods. Neuroimage 2000, 11, 805–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, M.D.; Raichle, M.E. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat. Rev. Neurosci. 2007, 8, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Weiss, B.A. Fisher’s r-to-Z Transformation Calculator to Compare Two Independent Samples [Computer Software]. Available online: https://blogs.gwu.edu/weissba/teaching/calculators/fishers-z-transformation/ (accessed on 22 August 2021).
- Pieramico, V.; Esposito, R.; Sensi, F.; Cilli, F.; Mantini, D.; Mattei, P.A.; Frazzini, V.; Ciavardelli, D.; Gatta, V.; Ferretti, A. Combination training in aging individuals modifies functional connectivity and cognition, and is potentially affected by dopamine-related genes. PLoS ONE 2012, 7, e43901. [Google Scholar] [CrossRef] [PubMed]
- Shigihara, Y.; Hoshi, H.; Shinada, K.; Okada, T.; Kamada, H. Non-pharmacological treatment changes brain activity in patients with dementia. Sci. Rep. 2020, 10, 6744. [Google Scholar] [CrossRef] [Green Version]
- Onder, G.; Zanetti, O.; Giacobini, E.; Frisoni, G.B.; Bartorelli, L.; Carbone, G.; Lambertucci, P.; Silveri, M.C.; Bernabei, R. Reality orientation therapy combined with cholinesterase inhibitors in Alzheimer’s disease: Randomised controlled trial. Br. J. Psychiatry 2005, 187, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeshurun, Y.; Nguyen, M.; Hasson, U. The default mode network: Where the idiosyncratic self meets the shared social world. Nat. Rev. Neurosci. 2021, 22, 181–192. [Google Scholar] [CrossRef]
- Sormaz, M.; Murphy, C.; Wang, H.T.; Hymers, M.; Karapanagiotidis, T.; Poerio, G.; Margulies, D.S.; Jefferies, E.; Smallwood, J. Default mode network can support the level of detail in experience during active task states. Proc. Natl. Acad. Sci. USA 2018, 115, 9318–9323. [Google Scholar] [CrossRef] [Green Version]
- Vatansever, D.; Menon, D.K.; Stamatakis, E.A. Default mode contributions to automated information processing. Proc. Natl. Acad. Sci. USA 2017, 114, 12821–12826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Buckingham, UK, 1997. [Google Scholar]
- Lou, H.C.; Luber, B.; Crupain, M.; Keenan, J.P.; Nowak, M.; Kjaer, T.W.; Sackeim, H.A.; Lisanby, S.H. Parietal cortex and representation of the mental Self. Proc. Natl. Acad. Sci. USA 2004, 101, 6827–6832. [Google Scholar] [CrossRef] [Green Version]
- Davidson, P.S.; Anaki, D.; Ciaramelli, E.; Cohn, M.; Kim, A.S.; Murphy, K.J.; Troyer, A.K.; Moscovitch, M.; Levine, B. Does lateral parietal cortex support episodic memory? Evidence from focal lesion patients. Neuropsychologia 2008, 46, 1743–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strikwerda-Brown, C.; Grilli, M.D.; Andrews-Hanna, J.; Irish, M. “All is not lost”-Rethinking the nature of memory and the self in dementia. Ageing Res. Rev. 2019, 54, 100932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Johndro, H.; Budson, A.E.; Gutchess, A. Influence of self-referential mode on memory for aMCI patients. Cogn. Neuropsychol. 2020, 37, 46–57. [Google Scholar] [CrossRef]
- Stephen, R.; Liu, Y.; Ngandu, T.; Antikainen, R.; Hulkkonen, J.; Koikkalainen, J.; Kemppainen, N.; Lotjonen, J.; Levalahti, E.; Parkkola, R.; et al. Brain volumes and cortical thickness on MRI in the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER). Alzheimer’s Res. Ther. 2019, 11, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Mean (SD)/n (%) | Baseline | Follow-Up | ||||
|---|---|---|---|---|---|---|
| CST (n = 16) | TAU (n = 13) | t/χ2 | CST (n = 16) | TAU (n = 13) | t/χ2 | |
| Female, n | 12 (75.0) | 7 (53.85) | 0.89 | - | - | - |
| Age, years | 80.65 (6.18) | 79.92 (6.13) | −0.27 | - | - | - |
| Duration of diagnosis, years | 1.87 (1.64) | 2.91 (1.72) | 1.37 | - | - | - |
| Education, years | 3.41 (4.14) | 6.15 (5.19) | 1.61 | - | - | - |
| Any formal education, n | 7 (43.75) | 12 (92.31) | 8.29 ** | - | - | - |
| Work, years | 35.25 (15.02) | 41.91 (12.57) | 1.15 | - | - | - |
| ADAS-Cog total | 20.49 (6.76) | 25.59 (9.82) | 1.03 | 18.74 (6.48) | 23.31 (8.71) | 1.65 |
| Memory & learning | 16.39 (5.45) | 18.44 (7.04) | 0.75 | 14.91 (5.52) | 18.46 (6.41) | 1.62 |
| Language | 1.82 (1.94) | 3.77 (4.19) | 1.70 | 1.88 (1.58) | 3.31 (3.40) | 1.53 |
| Praxis | 1.94 (1.14) | 1.38 (1.45) | −1.18 | 1.94 (1.85) | 1.62 (1.04) | −0.57 |
| CSDD | 3.35 (5.27) | 5.23 (10.09) | 0.66 | 2.24 (2.54) | 2.77 (3.35) | 0.50 |
| HCS | 7.24 (5.75) | 17.29 (9.86) | 3.15 * | 7.41 (5.09) | 16.00 (8.43) | 3.10 * |
| Grey matter, cm3 | 500.29 (38.89) | 502.39 (54.21) | 0.12 | 495.06 (39.01) | 482.82 (50.18) | −0.73 |
| White matter, cm3 | 392.53 (48.12) | 387.54 (52.42) | −0.27 | 394.47 (49.22) | 377.09 (52.89) | −0.89 |
| TICV, cm3 | 1393.41 (137.39) | 1439.31 (145.47) | 0.88 | 1393.41 (134.40) | 1429.64 (154.53) | 0.66 |
| GM/TICV | 0.36 (0.02) | 0.35 (0.02) | −1.31 | 0.36 (0.02) | 0.34 (0.02) | −2.33 * |
| WM/TICV | 0.28 (0.02) | 0.27 (0.03) | −1.42 | 0.28 (0.02) | 0.26 (0.03) | −2.04 |
| TBV/TICV | 0.64 (0.03) | 0.62 (0.04) | −1.77 | 0.64 (0.02) | 0.60 (0.04) | −2.81 * |
| DMN rs-FC, r | 0.24 (0.10) | 0.34 (0.21) | 1.61 | 0.36 (0.19) | 0.32 (0.13) | −0.66 |
| CEN rs-FC, r | 0.37 (0.19) | 0.32 (0.12) | −0.66 | 0.36 (0.18) | 0.31 (0.17) | −0.72 |
| LAN rs-FC, r | 0.27 (0.14) | 0.28 (0.18) | 0.29 | 0.24 (0.15) | 0.27 (0.14) | −0.59 |
| Time gap between behavioral and MRI assessments, days | 42 (21.5) | 23 (17.5) | 2.99 ** | 64 (35.2) | 14.5 (13.0) | 4.87 *** |
| CST (n = 16) | TAU (n = 13) | |||
|---|---|---|---|---|
| Mean (SD) | t | Mean (SD) | t | |
| ADAS-Cog total a | +1.75 (4.92) | 1.47 | +0.28 (4.31) | 0.23 |
| Memory and learning | +1.81 (4.67) | 1.60 | −0.02 (3.41) | −0.02 |
| Language | −0.05 (1.14) | −0.21 | +0.46 (1.81) | 0.92 |
| Praxis | 0.00 (1.58) | 0 | −0.23 (1.42) | −0.59 |
| CSDD | +1.12 (3.97) | 1.16 | +2.47 (7.77) | 1.14 |
| HCS | −0.18 (6.55) | −0.83 | +1.29 (2.14) | 1.59 |
| Grey matter, cm3 | −5.24 (8.93) | −2.42 * | −10.73 (14.61) | −2.44 * |
| White matter, cm3 | 1.94 (7.95) | 1.01 | −2.45 (11.99) | −0.68 |
| TICV, cm3 | 0.00 (18.36) | 0 | 5.55 (10.80) | 1.70 |
| GM/TICV | −0.003 (0.01) | −1.98 | −0.01 (0.01) | −2.45 * |
| WM/TICV | +0.001 (0.01) | 0.78 | −0.003 (0.01) | −1.31 |
| TBV/TICV | +0.002 (0.01) | 0.83 | −0.01 (0.01) | 4.39 ** |
| DMN rs-FC, r | +0.12 (0.14) | 3.31 * | −0.02 (0.21) | −0.32 |
| CEN rs-FC, r | −0.01 (0.21) | −0.10 | −0.01 (0.17) | −0.27 |
| LAN rs-FC, r | −0.03 (0.16) | −0.70 | −0.01 (0.19) | −0.25 |
| ADAS-Cog Change a | |||||
|---|---|---|---|---|---|
| CST Group (n = 16) | TAU Group (n = 13) | Comparison of Fisher’s-Z, z (p) | |||
| r | Fisher’s-Z | r | Fisher’s-Z | ||
| Work, years | 0.75 ** | 0.97 | 0.20 | 0.20 | 1.83 (p = 0.06) |
| Baseline TBV/TICV | 0.42 | 0.45 | 0.66 * | 0.79 | 0.82 (p = 0.41) |
| Baseline DMN rs-FC, r | -0.41 | -0.44 | 0.12 | 0.12 | 1.32 (p = 0.19) |
| Baseline CEN rs-FC, r | 0.13 | 0.13 | 0.58 | 0.66 | 1.26 (p = 0.21) |
| Baseline LAN rs-FC, r | 0.27 | 0.27 | 0.25 | 0.26 | 0.05 (p = 0.96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, T.; Spector, A.; Mograbi, D.C.; Cheung, G.; Wong, G.H.Y. Changes in Default Mode Network Connectivity in Resting-State fMRI in People with Mild Dementia Receiving Cognitive Stimulation Therapy. Brain Sci. 2021, 11, 1137. https://doi.org/10.3390/brainsci11091137
Liu T, Spector A, Mograbi DC, Cheung G, Wong GHY. Changes in Default Mode Network Connectivity in Resting-State fMRI in People with Mild Dementia Receiving Cognitive Stimulation Therapy. Brain Sciences. 2021; 11(9):1137. https://doi.org/10.3390/brainsci11091137
Chicago/Turabian StyleLiu, Tianyin, Aimee Spector, Daniel C. Mograbi, Gary Cheung, and Gloria H. Y. Wong. 2021. "Changes in Default Mode Network Connectivity in Resting-State fMRI in People with Mild Dementia Receiving Cognitive Stimulation Therapy" Brain Sciences 11, no. 9: 1137. https://doi.org/10.3390/brainsci11091137