1. Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disease after Alzheimer’s disease [
1] and affects around 120.000–150.000 individuals in Spain [
2]. Excellent symptomatic treatment is available, although no neuroprotective medication has been found so far. Even though the average age of onset is 60 years, the number of diagnoses under the age of 50 is increasing [
3]. Given that PD prevalence increases with age [
3], and considering the increase of life expectancy, the number of people affected by PD is predicted to strongly increase in the future [
4].
PD is characterized by motor symptoms including bradykinesia, resting tremor and muscle rigidity, but also by non-motor symptoms. These include cognitive impairment, mood disorders and depression, and may appear even at early disease stages [
5,
6]. Moreover, non-motor symptoms are often misdiagnosed because PD is mainly diagnosed on clinical motor symptomatology, following the United Kingdom Parkinson’s Disease Society Brain Bank (UK-PDSBB) criteria [
7,
8]. The Movement Disorder Society’s clinical diagnostic criteria for PD (MDS-PD) are intended for use specifically in research; however, they can be used as a general guide for clinical diagnosis. MDS-PD include supportive criteria apart from motor symptoms [
9]. Non-motor symptoms in the prodromal phase are usually not very specific (except for rapid eye movement [REM] sleep behavior disorder [RBD]), so they are not strong enough by themselves to reach a PD diagnosis. Recent studies have allowed PD diagnosis at prodromal stages in individuals with risk factors (hyposmia, depression and constipation, among others) or RBD itself [
10]. PD’s heterogeneous presentation reflects its complex and multifactorial etiogenesis, its diverse clinical course [
11] and probably a different pathogenic mechanism. Therefore, PD management is a major challenge because clinical response to treatment is also heterogeneous and disease treatment has to be personalized.
There is no first-choice treatment for PD management, although many pharmacological and non-pharmacological strategies are available. Among pharmacological treatments, levodopa, dopaminergic agonists (DA), catechol-O-methyltransferase inhibitors (COMTI) and monoaminooxidase B inhibitors (MAOI-B) are the most common therapies for PD, used both alone or in combination [
3]. Since several motor, non-motor symptoms and related complications must be treated, PD management is often complex.
As a chronic progressive disease, PD has a great impact on patients’ and caregivers’ private, social and professional lives. PD caused more than 200,000 deaths and 3.2 million disability-adjusted life-years (DALYs) worldwide in 2016, and more than 4000 deaths and 54,175 DALYs in Spain [
12]. Moreover, it also causes substantial societal burden and entails an important economic impact [
13].
Considering the high incidence of the disease, its increased prevalence due to population aging and the unmet needs regarding diagnosis and treatment, it is crucial to better understand PD management to optimize and design future strategies. Thus, the aim of the PARKINSON 2030 project was to discuss and reach a consensus using the Delphi method (a process used to arrive at a group opinion or decision by surveying a panel of experts in which the experts respond to several rounds of questionnaires, and the responses are aggregated and shared with the group after each round) among a panel of experts in movement disorders on the current situation, their 10-year forecast of the general management of PD in daily clinical practice and to establish recommendations on the diagnostic and therapeutic management of PD.
2. Materials and Methods
We specifically used a modified Delphi method (a group consensus strategy that systematically uses literature reviews, opinions of stakeholders and the judgment of experts within a field to reach agreement) [
14,
15,
16] to better understand the management and the socioeconomic burden of PD in Spain. This Delphi approach was carried out in 6 successive phases: creation of an Advisory Committee, definition of criteria to select panelists, design of the Delphi questionnaire, Delphi survey administration, data collection and data analysis.
The Advisory Committee included 4 experts in movement disorders, members of the Study Group of Movement Disorders of the Spanish Neurology Society (Sociedad Española de Neurología, SEN). The Advisory Committee defined the project and created the first version of the Delphi questionnaire.
Panelists included were experts in movement disorders from different regions of Spain. The list of participating panelists is shown in
Table S1.
Preparation and Administration of the Questionnaire and Data Analysis
A literature search that included guidelines, reviews and other types of critical synthesis of scientific literature, as well as a bottom-up search from the main references to identify other papers of interest was carried out, and the initial questionnaire developed. The questionnaire addressed nine topics: the epidemiology of PD, the pathophysiology of PD, PD’s impact on patients and caregivers, PD diagnosis, PD follow-up, PD treatment, the economic impact of PD, the current and future situation of PD and the role of patient and caregiver associations. The initial version of the questionnaire was validated by 14 additional experts in movement disorders, acting as the National Committee of experts (
Figure S1). The questionnaire was held to two rounds of voting between October–December 2019 (first wave) and September–November 2020 (second wave). Panelists completed the questionnaire through an online platform that ensured data anonymity and confidentiality.
All questions about the current situation used a 4-level scale, which varied depending on the question (never, rarely, often, always; or, strongly disagree, disagree, agree, strongly agree; or, not important, not very important, important, very important; or, not useful, not very useful, useful, very useful; or, no impact, little impact, quite some impact, a lot of impact). All questions referring to future trends used a nine-point Likert-type ordinal scale, divided in three categories: 1 to 3 (it will decrease), 4 to 6 (it will not change) and 7 to 9 (it will increase). When ≥70% of panelists agreed in one category of response, that item was considered to have reached “consensus” on that category. Otherwise, the item was stated as “undetermined” and sent for a second round of votes, together with all comments made by panelists in face-to-face meetings.
Between the two rounds of voting, panelists attended 7 face-to-face local meetings moderated by the members of the National Committee of experts. In these meetings, the results of wave 1 were presented and discussed, and the items of the questionnaire to include in wave 2 were agreed upon. Although 12 meetings were planned, due to the state of alarm decree by COVID-19 in March 2020, only 7 meetings were held. All items that did not reach consensus in the first wave were included in the second wave.
The final results of the Delphi survey were further evaluated and discussed by the Advisory and National Committees.
4. Discussion
The outcomes of this project provide data on current diagnosis and management of PD and its trends towards 2030 in Spain. This project included panelists with extensive experience in PD and the main results show a future perspective of PD management similar or better than nowadays.
PD is one of the most prevalent neurodegenerative diseases at present [
1], and most experts (92%) considered that prevalence will increase by 2030, in accordance with estimates published in 2005, predicting that the number of individuals with PD would double by 2030 [
4].
The Parkinson’s Disease Survey Observing the Quality of Care (Encuesta de Parkinson Observando la Calidad Asistencial, EPOCA) study carried out in Spain showed that more than half of patients get PD diagnosis between 1 and 5 years from the first symptom [
17], which is quite delayed, and this gap significantly increases in patients with early-onset. Besides, according to SEN, up to 24% of PD patients have been misdiagnosed [
3]. Therefore, efforts should be put towards an early and accurate diagnosis of PD, shortening the time to obtain PD diagnosis and rapid referral, as needs identified by study panelists.
Main criteria used for PD diagnosis are UK-PDSBB criteria and MDS criteria. When UK-PDSBB criteria are used, non-motor symptoms are not included, although these symptoms significantly contribute to health status and quality of life in PD [
18]. In contrast, new MDS criteria [
9] include motor symptoms and supportive criteria (non-motor symptoms). In our study, a trend towards a change to PD definition including non-motor or atypical symptoms, MDS criteria, and probably functional neuroimaging findings is observed.
Neuropsychiatric disorders (depression, apathy, sleep disturbances and anxiety) are common in PD patients; however, are often underrecognized and undertreated. In particular, >80% of PD patients develop dementia after 20 years, and hallucinations are consistently associated with progressive cognitive deterioration and dementia in PD [
19,
20,
21]. According with data form the literature, our expert panel agreed that these symptoms would become relevant prognostic factors for PD patients in the future.
Given that PD is multifactorial and its etiopathogenesis is still unknown, no valid biomarkers for diagnosis are currently available. At the present time, 90 independent PD risk-associated mutations have been identified in more than 20 genes [
22]; and it is still on-going research. Panelists also reported that geneticists will have a more relevant role in PD diagnosis, probably linked to the development of emerging technologies focused on the improvements of the knowledge of genetic risk, genetic predisposition and genetic features. Understanding the genetic factors that influence PD development will be important not only for PD diagnosis, but also for developing new and personalized treatments.
A range of biomarkers, including imaging, biochemical or genetic biomarkers have been proposed for PD diagnosis and prognosis; unfortunately, none can currently be used in real life [
23]. Nevertheless, panelists rely on their potential for improving PD management, since they agreed that the use of CSF and plasma biomarkers and structural imaging as prognostic markers of the disease will increase by 2030. Biomarkers could also provide information on disease progression and treatment efficacy in the future, being involved in monitoring follow-up. A recent study has identified a CSF biomarker (α-synuclein) associated with increased risk of subsequent diagnosis of PD or dementia with Lewy bodies [
10] approaching this promising future.
Apart from biomarkers, new sensor-based and wearable and non-wearable, hybrid technologies that can assess PD symptoms in an objective way will be useful for remote monitoring of PD patients in the future. Although nowadays its use is still limited and further research is needed, panelists agreed that they will become an important support in PD management [
24,
25].
The panelists determined that PD treatment in non-fluctuating patients should include more than one drug; however, up to 60% of the experts indicate that high-dose levodopa will continue to be used in monotherapy by 2030. Since its introduction in 1967, high-dose oral levodopa regimen for PD treatment remains uncontested [
26].
In the fluctuating PD patients, treatment with high-dose levodopa will remain unchanged in the future, even though levodopa is associated with the appearance of motor complications. Since recent reports indicate that levodopa use does not modify the disease course, its use as antiparkinsonian drug is expected to continue to be maintained in the future, although low-dose levodopa is recommended to avoid dyskinesias. Current guidelines recommend levodopa in combination; these results suggest the need for better training about polytherapy benefits in these patients. There is also a trend towards a greater use of levodopa + safinamide and the combination of levodopa + DA+ safinamide not observed with other MAOI agents. This tendency might be explained by the proven effect of safinamide in reducing motor and non-motor fluctuations, its low rate of adverse events reported in several studies and importantly, the demonstrated effect of safinamide in alleviating non-motor symptoms, including pain and depression, and on quality of life impairment [
27,
28,
29,
30].
PD in later stages is characterized by the emergence of disabling motor and non-motor symptoms, which are poorly controlled with conventional therapies and have a significant impact on the patient’s health status [
31]. In PD patients with an advanced stage, panelists observed a trend towards an increase in the use of new therapies, in particular DBS. This probably reflects that more patients will reach a device-based therapy phase, or that the available therapies will not modify the course of the disease. There is a significant need for developing treatments to modify the disease progression itself. New therapies under development such as stem cell therapies or gene-therapy [
32] and a number of symptomatic and disease modifying therapies are currently being tested in clinical trials [
33]. The application of high intense focused ultrasound (HIFU) is a quite new procedure that is being used for PD treatment. In our study, panelists agreed on its increased use in the future in spite of the fact that it is quite a new technique. They also considered HIFU as a useful tool for treating PD patients.
There is a general idea that both the appearance of motor and non-motor symptoms is relevant for deciding on a change of treatment; however, regarding symptoms beyond the CNS, experts did not consider them relevant when deciding on a change of treatment.
Guidelines state that a multidisciplinary team including professionals for assessing the personal, family, work and social situation of the patient and create personalized treatments for motor and non-motor symptoms with experience and adequate training is crucial for therapy success [
34]. The group of experts considered that the role of the neurologist specialized in PD will become more relevant in the future, as well as the role of movement disorder specialist nurses, highlighting the importance of specialization.
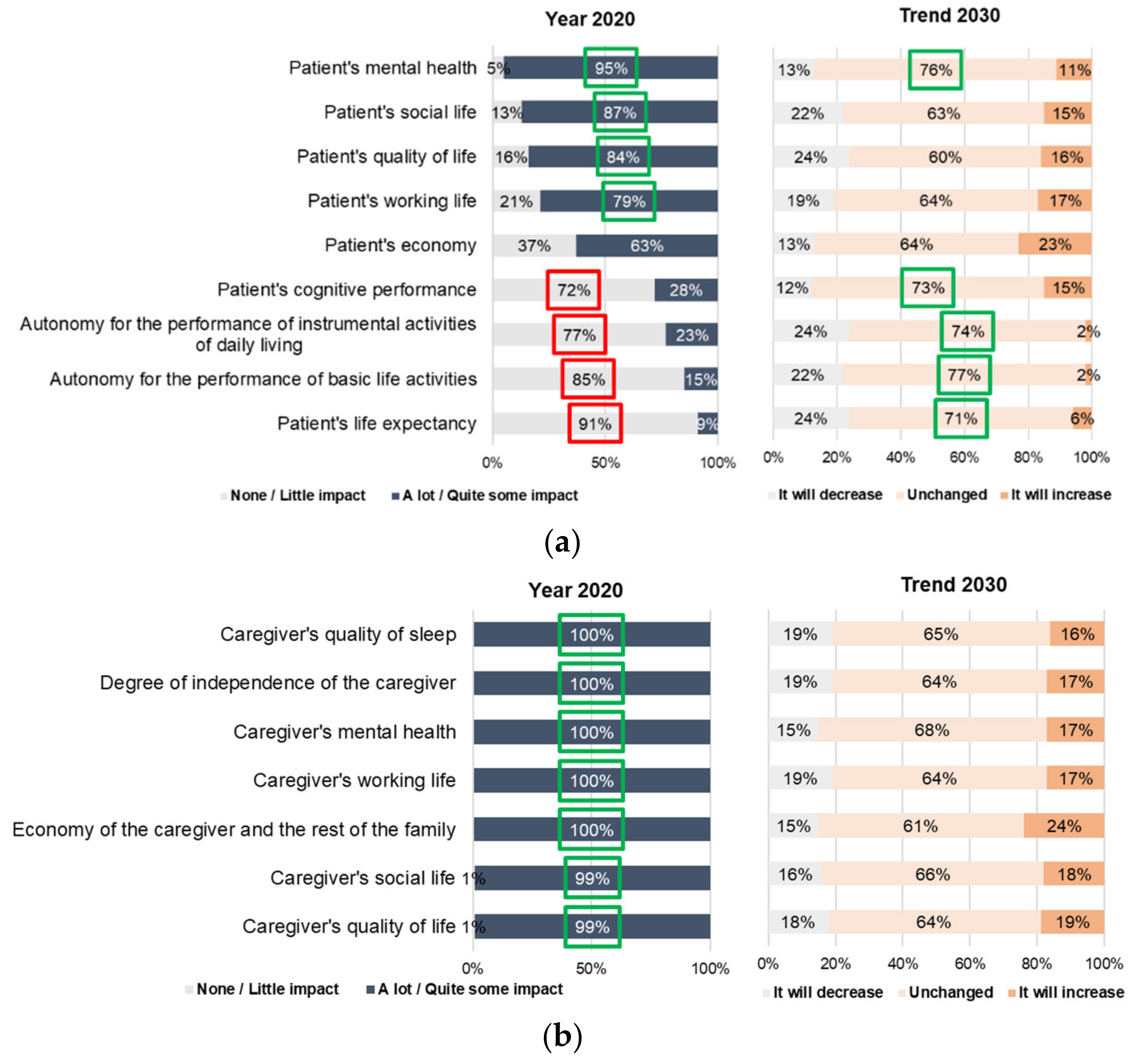
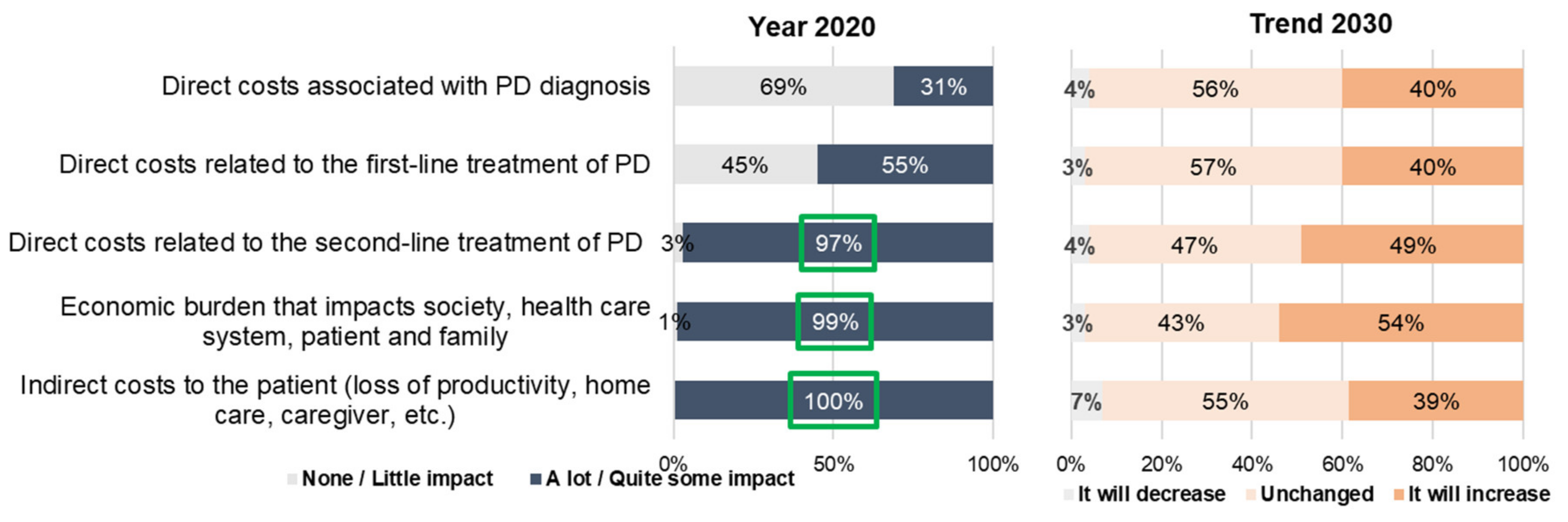
As with many other neurologic conditions, PD has a great impact on quality of life and increases mortality among PD patients [
35]. As the disability increases, PD symptoms and the disease course affect not only patients, but also their families and caregivers. Furthermore, it entails high economic burden with an estimated cost of €17,000 per patient per year in Spain [
13]. Pharmacological treatment was identified as the main driver (34% of direct costs), and as the disease progresses, the need for symptomatic treatment grows.
PD unmet needs can be addressed through a comprehensive approach including physical, psychological, social and financial aspects. Early actions on diagnosis, follow-up and care planning can allow patients and caregivers to hamper the disease course and to develop anticipatory strategies. In this vein, a recent study identified a desire of PD patients and care partners to establish roadmaps as a guide for decision-making and planning [
36].
Limitations
The panelists participating in the study were representative of the clinical practice across Spain, and provided detailed information regarding PD clinical management. Consequently, results reflect the current management of PD and the vision for the future in a populous European country; however, the conclusions of this study cannot be extrapolated to other countries or cultural settings.
It has to be noted that the COVID-19 outbreak may have had an impact on the results, given that the project was truncated by this pandemic and carried out in two different scenarios. Besides, as with all Delphi studies, the results derived from the panel express an opinion and do not analyze prospective or retrospective data. Finally, the questionnaire was long, and bias due to tiredness cannot be excluded.
To our knowledge, this is the first study aiming to shed light on planning for future PD management in Spain. This study highlights the unmet needs in diagnosis and treatment and how crucial it is to establish recommendations on the diagnostic-therapeutic management of PD to optimize and design future management strategies.
5. Conclusions
The global and, in particular, socio-economic impact of PD will continue to be very important in all life dimensions of patients, family, caregivers, and in society in general, especially for patients in more advanced stages.
The experts considered that there will be an improvement in diagnostic capacity, follow-up and the development of innovative treatments, with fewer diagnostic errors and earlier diagnosis. This will be due to improved access of patients to movement disorder experts, and future studies on biomarkers will probably contribute to this improvement. In prognosis, the use of certain biomarkers will be important; in monitoring, new technologies will have an impact; and in treatment, depending on the evolutionary stage of the disease, the growing roles of expert nurses, neurologists, and other professionals (e.g., physiotherapists) will be very important, forming multidisciplinary teams that will move towards a more individualized and technological medicine. In summary, this work offers information that can help healthcare professionals to reflect individually on the care of PD in their area and propose future strategies to improve the management of patients and their environment (e.g., protocols, national plans, research management, social measures, etc.), as well as advance in knowledge and research.


 ,
, 



{kind=link}
{kind=link}
{kind=link}