
The Use of Dynamic Contrast-Enhanced Magnetic Resonance Imaging for the Evaluation of Blood-Brain Barrier Disruption in Traumatic Brain Injury: What Is the Evidence?

 , ,
, ,
Abstract
:1. Introduction
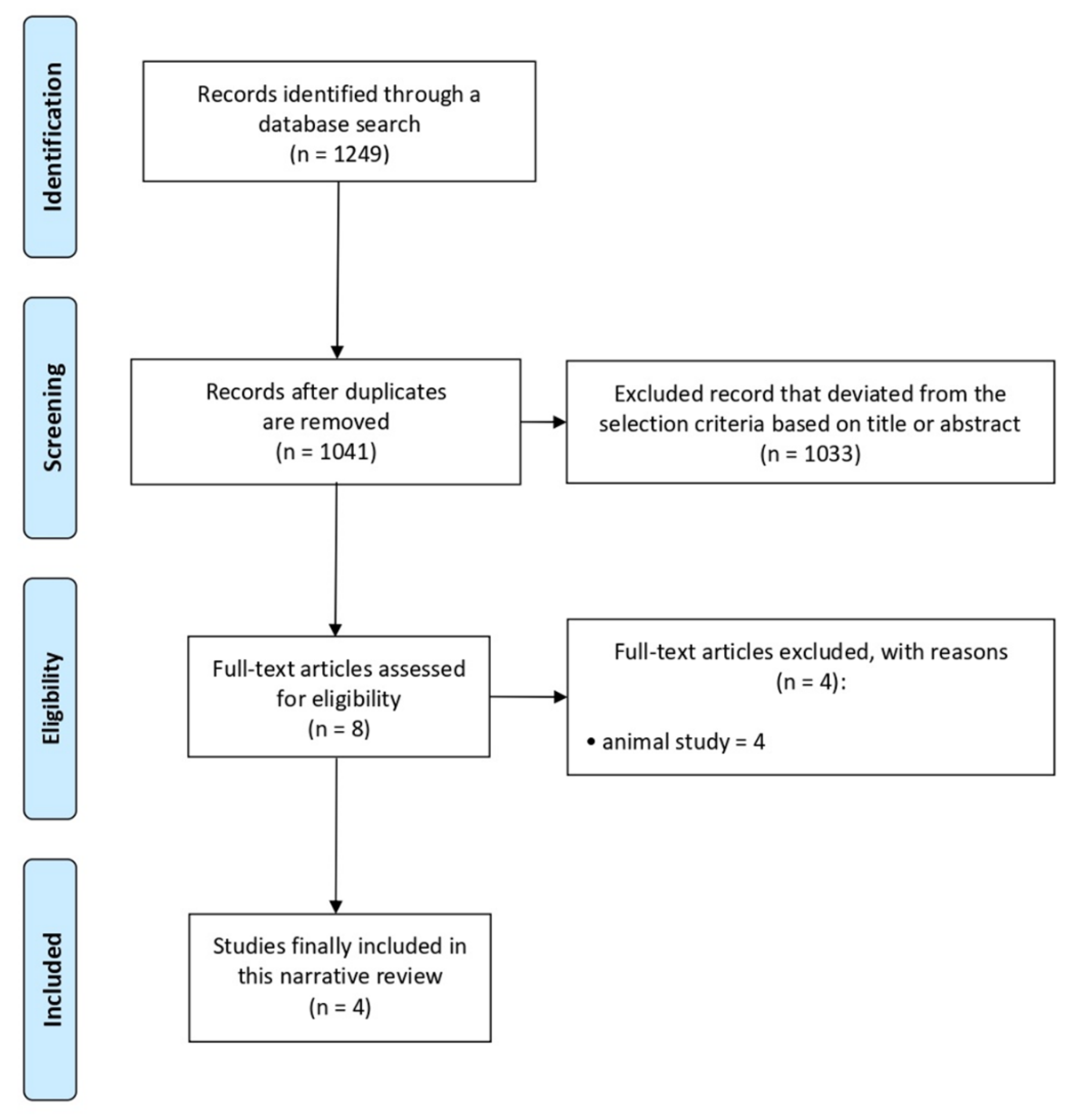
2. Methods
3. Results
3.1. Study Selection
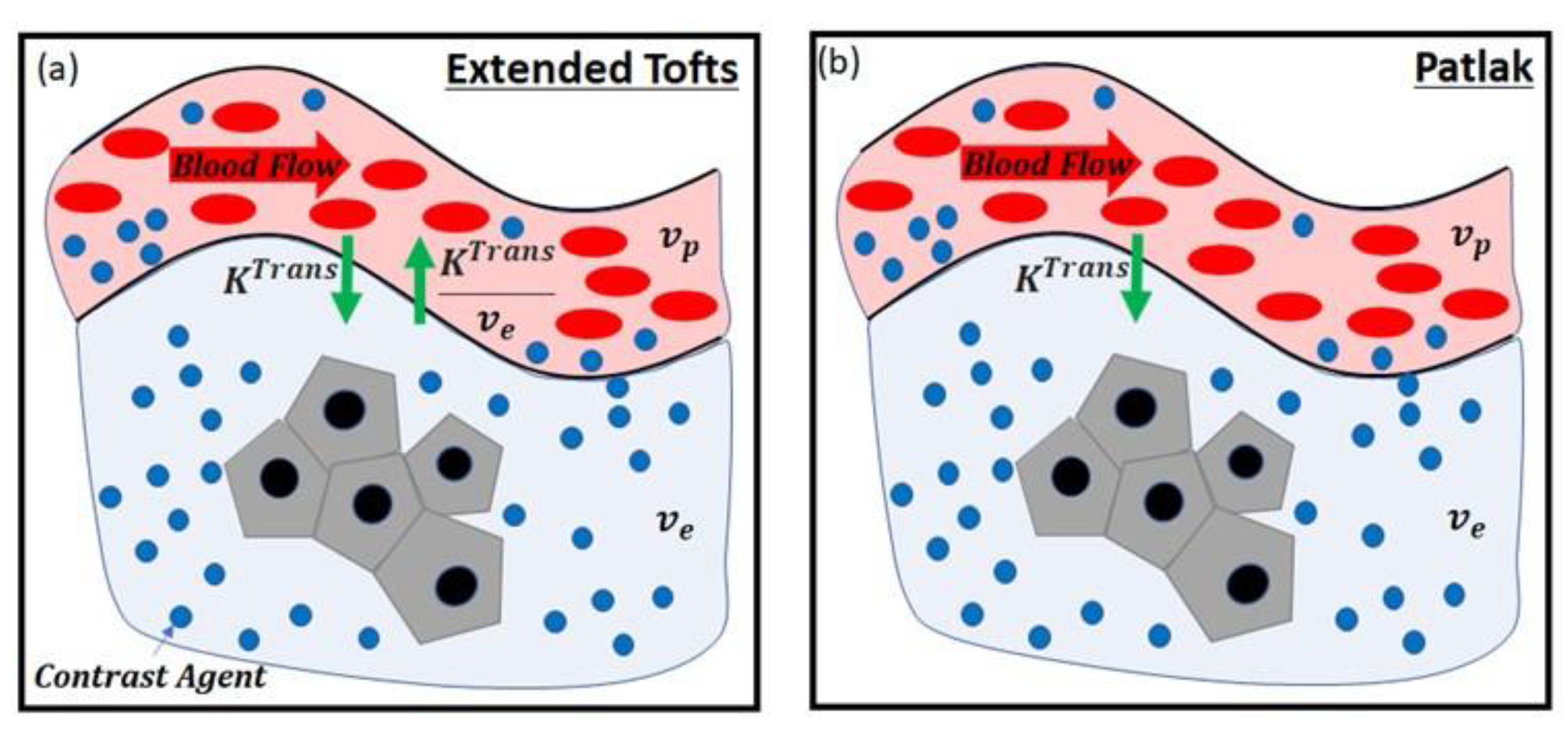
3.2. Parameters Used in DCE-MRI Studies
3.3. Review of Previous Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ling, H.; Hardy, J.; Zetterberg, H. Neurological consequences of traumatic brain injuries in sports. Mol. Cell. Neurosci. 2015, 66, 114–122. [Google Scholar] [CrossRef]
- Kaur, P.; Sharma, S. Recent Advances in Pathophysiology of Traumatic Brain Injury. Curr. Neuropharmacol. 2018, 16, 1224–1238. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The Blood-Brain Barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef] [Green Version]
- Chodobski, A.; Zink, B.J.; Szmydynger-Chodobska, J. Blood–Brain Barrier Pathophysiology in Traumatic Brain Injury. Transl. Stroke Res. 2011, 2, 492–516. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Hussain, B.; Chang, J. Peripheral inflammation and blood–brain barrier disruption: Effects and mechanisms. CNS Neurosci. Ther. 2021, 27, 36–47. [Google Scholar] [CrossRef]
- Varatharaj, A.; Liljeroth, M.; Darekar, A.; Larsson, H.B.; Galea, I.; Cramer, S.P. Blood-brain barrier permeability measured using dynamic contrast-enhanced magnetic resonance imaging: A validation study. J. Physiol. 2018, 597, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Jin, T.; Zhang, H.; Liu, X.; Kong, X.; Makamure, J.; Chen, Z.; Alwalid, O.; Yao, Z.; Wang, J. Enhancement degree of brain metastases: Correlation analysis between enhanced T2 FLAIR and vascular permeability parameters of dynamic contrast-enhanced MRI. Eur. Radiol. 2021, 1–10. [Google Scholar] [CrossRef]
- Raja, R.; Rosenberg, G.A.; Caprihan, A. MRI measurements of Blood-Brain Barrier function in dementia: A review of recent studies. Neuropharmacology 2018, 134, 259–271. [Google Scholar] [CrossRef]
- Ulas, C.; Das, D.; Thrippleton, M.J.; Hernández, M.D.C.V.; Armitage, P.A.; Makin, S.; Wardlaw, J.M.; Menze, B.H. Convolutional Neural Networks for Direct Inference of Pharmacokinetic Parameters: Application to Stroke Dynamic Contrast-Enhanced MRI. Front. Neurol. 2019, 9, 1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Golob, E.J.; Su, M.-Y. Vascular volume and blood-brain barrier permeability measured by dynamic contrast enhanced MRI in hippocampus and cerebellum of patients with MCI and normal controls. J. Magn. Reson. Imaging 2006, 24, 695–700. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, E.; Kelly, E.; Liu, Y.; Giordano, C.; Wallace, E.; Hynes, M.; Tiernan, S.; Meagher, A.; Greene, C.; Hughes, S.; et al. Dynamic Blood–Brain Barrier Regulation in Mild Traumatic Brain Injury. J. Neurotrauma 2020, 37, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Winter, C.; Bell, C.; Whyte, T.; Cardinal, J.; Macfarlane, D.; Rose, S. Blood–brain barrier dysfunction following traumatic brain injury: Correlation of K trans (DCE-MRI) and SUVR (99mTc-DTPA SPECT) but not serum S100B. Neurol. Res. 2015, 37, 599–606. [Google Scholar] [CrossRef]
- Yoen, H.; Yoo, R.-E.; Choi, S.H.; Kim, E.; Oh, B.-M.; Yang, D.; Hwang, I.; Kang, K.M.; Yun, T.J.; Kim, J.-H.; et al. Blood-Brain Barrier Disruption in Mild Traumatic Brain Injury Patients with Post-Concussion Syndrome: Evaluation with Region-Based Quantification of Dynamic Contrast-Enhanced MR Imaging Parameters Using Automatic Whole-Brain Segmentation. Korean J. Radiol. 2021, 22, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Yoo, R.-E.; Choi, S.H.; Oh, B.-M.; Shin, S.D.; Lee, E.J.; Shin, D.J.; Jo, S.W.; Kang, K.M.; Yun, T.J.; Kim, J.-H.; et al. Quantitative dynamic contrast-enhanced MR imaging shows widespread blood-brain barrier disruption in mild traumatic brain injury patients with post-concussion syndrome. Eur. Radiol. 2019, 29, 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Tofts, P.; Berkowitz, B.; Schnall, M.D. Quantitative Analysis of Dynamic Gd-DTPA Enhancement in Breast Tumors Using a Permeability Model. Magn. Reson. Med. 1995, 33, 564–568. [Google Scholar] [CrossRef]
- Tofts, P. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J. Magn. Reson. Imaging 1997, 7, 91–101. [Google Scholar] [CrossRef]
- Patlak, C.S.; Blasberg, R.G.; Fenstermacher, J.D. Graphical Evaluation of Blood-to-Brain Transfer Constants from Multiple-Time Uptake Data. Br. J. Pharmacol. 1983, 3, 1–7. [Google Scholar] [CrossRef]
- Chang, M.C.; Kim, S.H.; Kim, O.L.; Bai, D.S.; Jang, S.H. The relation between fornix injury and memory impairment in patients with diffuse axonal injury: A diffusion tensor imaging study. Neurorehabilitation 2010, 26, 347–353. [Google Scholar] [CrossRef]
- Gennarelli, T.A. Mechanisms of brain injury. J. Emerg. Med. 1993, 11, 5–11. [Google Scholar]
- Chang, M.C.; Seo, J.P. Injury of the dentato-rubro-thalamic tract in a patient with intentional tremor after mild traumatic brain injury: A case report. Brain Inj. 2020, 34, 1283–1286. [Google Scholar] [CrossRef]
- Yeo, S.S.; Chang, M.C.; Kim, S.H.; Son, S.M.; Jang, S.H. Neural connection between injured cingulum and pedunculopontine nucleus in a patient with traumatic brain injury. Neurorehabilitation 2012, 31, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Calamante, F. The Seven Deadly Sins of Measuring Brain Structural Connectivity Using Diffusion MRI Streamlines Fibre-Tracking. Diagnostics 2019, 9, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| First Author, Year | Study Design | Number of Patients (E/C) | Parameters for Analysis | Summary of the Outcome |
|---|---|---|---|---|
| Winter, 2015 [12] | Single-arm prospective study | 14 (7 mild, 4 moderate, and 3 severe TBI) | Although there was no statistical significance, as TBI severity became more severe, the value increased. value was significantly correlated with the SPECT findings. | |
| Yoo, 2019 [14] | Retrospective study | 44 (mild TBI)/32 | , | and values at dorsolateral midbrain and at bilateral frontal gray-white matter were significantly higher in the TBI patients. Delayed recall scores were significantly correlated with values. |
| O’Keeffe, 2020 [11] | Single-arm prospective study | 5 professional MMA fighters and 19 adolescent rugby players | Slope of contrast agent concentration | MMA fighters: the degree of BBB disruption was correlated with the duration and repeatability of the strike. Rugby players: BBB disruption was found in the periventricular regions. |
| Yoen, 2021 [13] | Retrospective study | 42 (mild TBI)/29 | , | value in the bilateral cerebral cortex was significantly higher in mild TBI patients. values in the bilateral cerebellar white matter and brainstem were significantly lower in mild TBI patients. |
| Pharmacokinetic Model | Parameters | Study | |
|---|---|---|---|
| Tofts | , | Winter (2015), Yoo (2018) [12,14] | |
| Extended Tofts | , , | Yoen (2021) [13] | |
| Patlak | , | Yoen (2021) [13] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, S.S.; Lee, E.-H.; Kim, J.-H.; Seo, Y.B.; Choo, Y.J.; Park, J.; Chang, M.C. The Use of Dynamic Contrast-Enhanced Magnetic Resonance Imaging for the Evaluation of Blood-Brain Barrier Disruption in Traumatic Brain Injury: What Is the Evidence? Brain Sci. 2021, 11, 775. https://doi.org/10.3390/brainsci11060775
Oh SS, Lee E-H, Kim J-H, Seo YB, Choo YJ, Park J, Chang MC. The Use of Dynamic Contrast-Enhanced Magnetic Resonance Imaging for the Evaluation of Blood-Brain Barrier Disruption in Traumatic Brain Injury: What Is the Evidence? Brain Sciences. 2021; 11(6):775. https://doi.org/10.3390/brainsci11060775
Chicago/Turabian StyleOh, Sung Suk, Eun-Hee Lee, Jong-Hoon Kim, Young Beom Seo, Yoo Jin Choo, Juyoung Park, and Min Cheol Chang. 2021. "The Use of Dynamic Contrast-Enhanced Magnetic Resonance Imaging for the Evaluation of Blood-Brain Barrier Disruption in Traumatic Brain Injury: What Is the Evidence?" Brain Sciences 11, no. 6: 775. https://doi.org/10.3390/brainsci11060775