
Clinical Outcomes of Biportal Endoscopic Interlaminar Decompression with Oblique Lumbar Interbody Fusion (OLIF): Comparative Analysis with TLIF

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
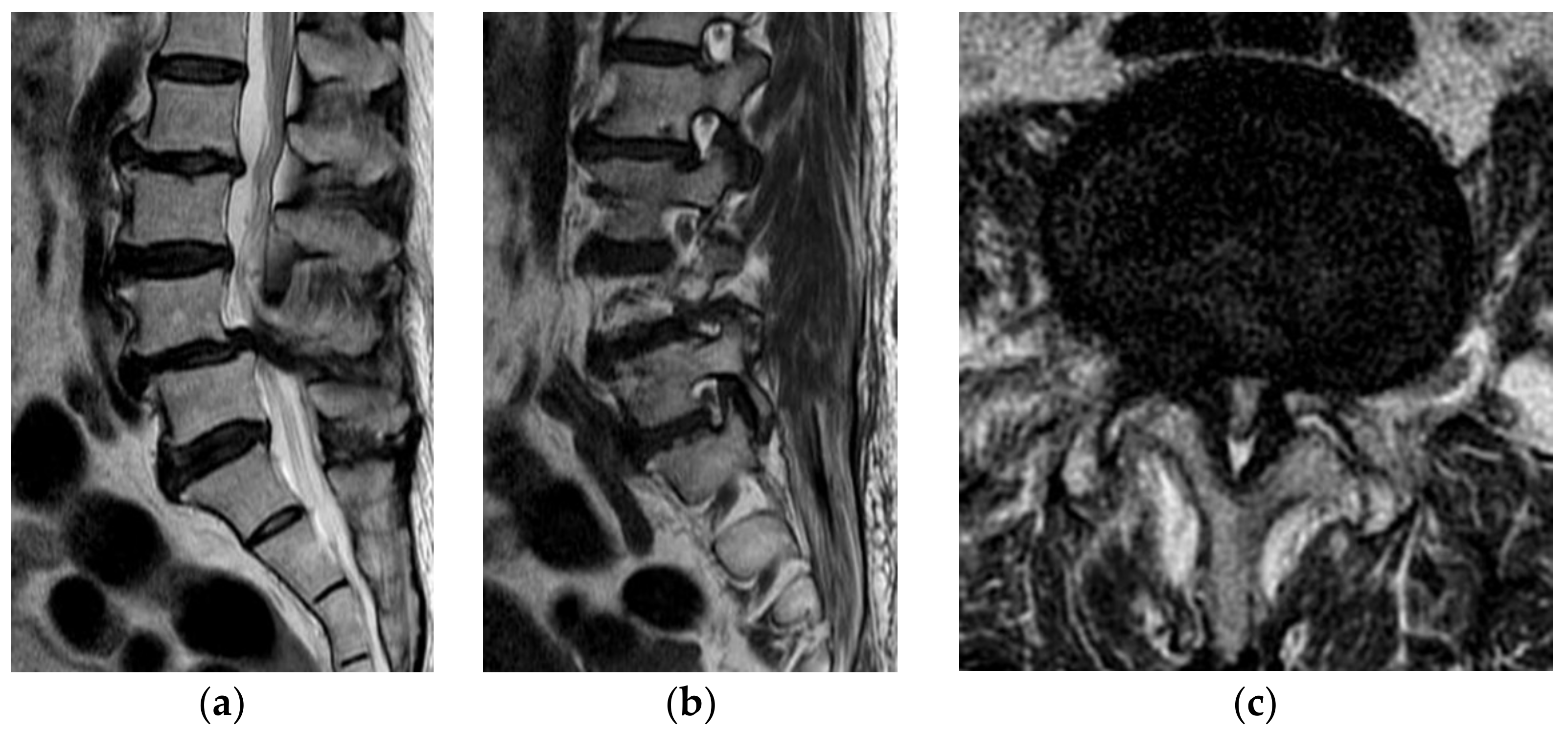
2.1. Indications for Operations
2.2. Surgical Procedures
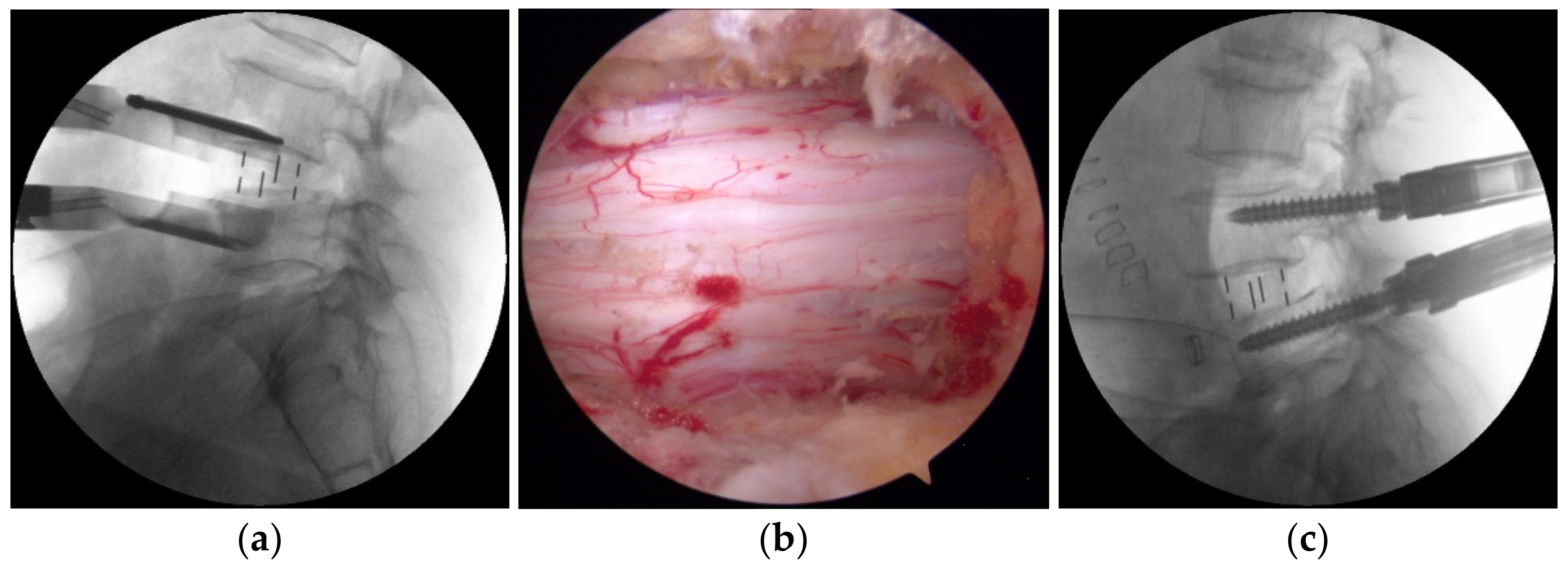
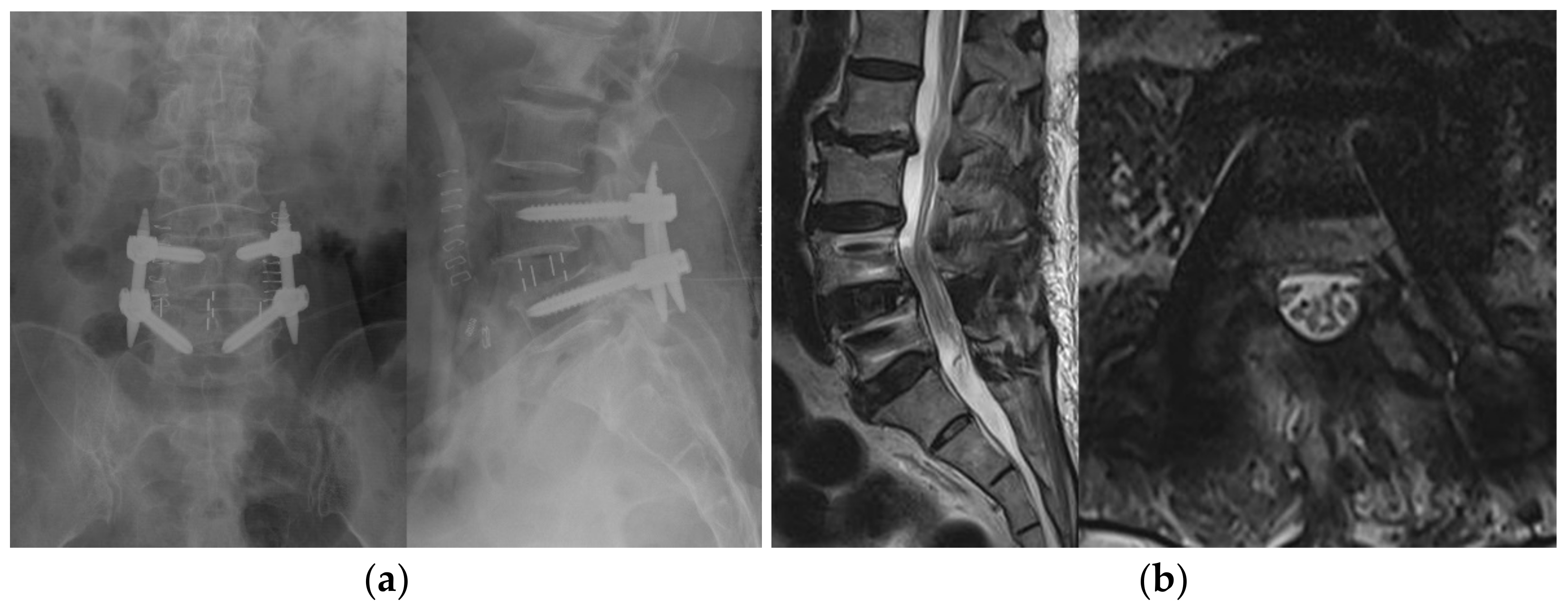
2.2.1. BESS with OLIF
2.2.2. Conventional Open TLIF
2.3. Clinical Assessment
2.4. Statistical Analyses
3. Results
3.1. Demographic Data, Disease Characteristics, and Operative Data
3.2. Clinical Outcomes
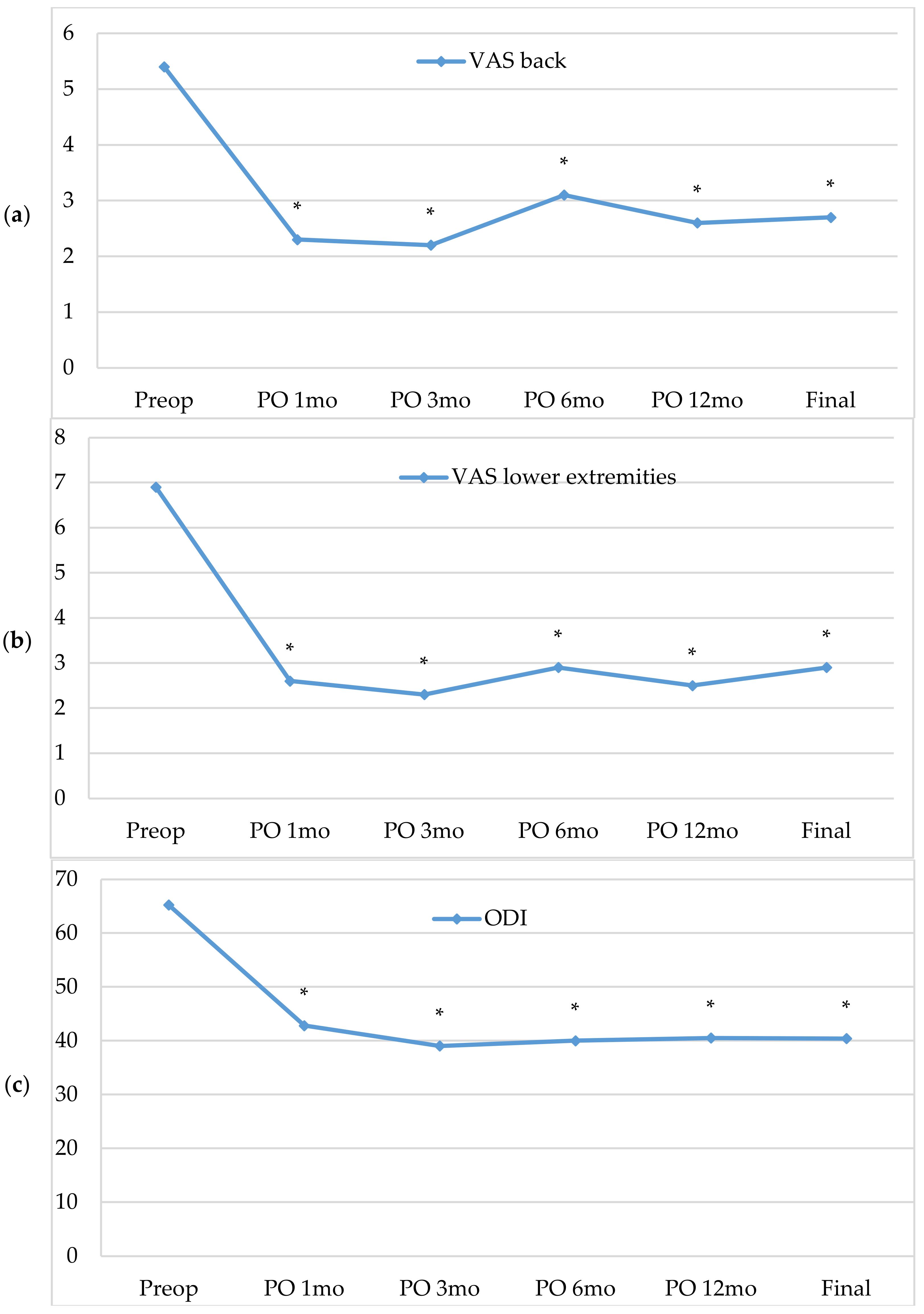
3.2.1. Intra-Group Analyses (Group A)
3.2.2. Inter-Group Analyses (Group A Versus Group B)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.-T.; Jo, D.-J.; Lee, S.-H.; Seo, E.-M. Oblique Retroperitoneal Approach for Lumbar Interbody Fusion from L1 to S1 in Adult Spinal Deformity. Neurosurg. Rev. 2018, 41, 355–363. [Google Scholar] [CrossRef]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme Lateral Interbody Fusion (XLIF): A Novel Surgical Technique for Anterior Lumbar Interbody Fusion. Spine J. 2006, 6, 435–443. [Google Scholar] [CrossRef]
- Silvestre, C.; Mac-Thiong, J.-M.; Hilmi, R.; Roussouly, P. Complications and Morbidities of Mini-Open Anterior Retroperitoneal Lumbar Interbody Fusion: Oblique Lumbar Interbody Fusion in 179 Patients. Asian Spine J. 2012, 6, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Fujibayashi, S.; Hynes, R.A.; Otsuki, B.; Kimura, H.; Takemoto, M.; Matsuda, S. Effect of Indirect Neural Decompression through Oblique Lateral Interbody Fusion for Degenerative Lumbar Disease. Spine (Phila Pa 1976) 2015, 40, E175–E182. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.; Marchi, L.; Coutinho, E.; Pimenta, L. A Radiographic Assessment of the Ability of the Extreme Lateral Interbody Fusion Procedure to Indirectly Decompress the Neural Elements. Spine (Phila Pa 1976) 2010, 35, S331–S337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, J.; Ohtori, S.; Orita, S.; Yamauchi, K.; Eguchi, Y.; Ochiai, N.; Kuniyoshi, K.; Aoki, Y.; Nakamura, J.; Miyagi, M.; et al. Radiographic Evaluation of Indirect Decompression of Mini-Open Anterior Retroperitoneal Lumbar Interbody Fusion: Oblique Lateral Interbody Fusion for Degenerated Lumbar Spondylolisthesis. Eur. Spine J. 2017, 26, 671–678. [Google Scholar] [CrossRef]
- Epstein, N.E. Extreme Lateral Lumbar Interbody Fusion: Do the Cons Outweigh the Pros? Surg. Neurol. Int. 2016, 7, S692–S700. [Google Scholar] [CrossRef] [Green Version]
- Heo, D.H.; Kim, J.-S. Clinical and Radiological Outcomes of Spinal Endoscopic Discectomy–Assisted Oblique Lumbar Interbody Fusion: Preliminary Results. Neurosurg. Focus 2017, 43, E13. [Google Scholar] [CrossRef]
- Nakashima, H.; Kanemura, T.; Satake, K.; Ishikawa, Y.; Ouchida, J.; Segi, N.; Yamaguchi, H.; Imagama, S. Unplanned Second-Stage Decompression for Neurological Deterioration Caused by Central Canal Stenosis after Indirect Lumbar Decompression Surgery. Asian Spine J. 2019, 13, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Heo, D.H.; Choi, W.S.; Park, C.-K.; Kim, J.-S. Minimally Invasive Oblique Lumbar Interbody Fusion with Spinal Endoscope Assistance: Technical Note. World Neurosurg. 2016, 96, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.-J.; Choi, C.-M.; Jung, J.-T.; Lee, S.-J.; Kim, Y.-S. Learning Curve Associated with Complications in Biportal Endoscopic Spinal Surgery: Challenges and Strategies. Asian Spine J. 2016, 10, 624–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwa Eum, J.; Hwa Heo, D.; Son, S.K.; Park, C.K. Percutaneous Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Technical Note and Preliminary Clinical Results. J. Neurosurg. Spine 2017, 24, 602–607. [Google Scholar] [CrossRef]
- Soliman, H.M. Irrigation Endoscopic Decompressive Laminotomy. A New Endoscopic Approach for Spinal Stenosis Decompression. Spine J. 2015, 15, 2282–2289. [Google Scholar] [CrossRef]
- Choi, C.M.; Chung, J.T.; Lee, S.J.; Choi, D.J. How I Do It? Biportal Endoscopic Spinal Surgery (BESS) for Treatment of Lumbar Spinal Stenosis. Acta Neurochir. 2016, 158, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Komp, M.; Giannakopoulos, A.; Kasch, R.; Ruetten, S. Bilateral Spinal Decompression of Lumbar Central Stenosis with the Full-Endoscopic Interlaminar Versus Microsurgical Laminotomy Technique: A Prospective, Randomized, Controlled Study. Pain Physician 2015, 10, 61–70. [Google Scholar] [CrossRef]
- Min, W.-K.; Kim, J.-E.; Choi, D.-J.; Park, E.J.; Heo, J. Clinical and Radiological Outcomes between Biportal Endoscopic Decompression and Microscopic Decompression in Lumbar Spinal Stenosis. J. Orthop. Sci. 2020, 25, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Ahn, J.-S.; Park, E.J.; Kwon, Y.-S. Combination of Minimally Invasive Spinal Surgery: Oblique Lumbar Interbody Fusion And Biportal Endoscopic Spinal Surgery for Lumbar Spinal Stenosis—Pilot Study. JASS 2018, 8, 17–25. [Google Scholar]
- Panjabi, M.M. Clinical Biomechanics of the Spine; JB Lippincott: Philadelphia, PA, USA, 1990. [Google Scholar]
- Wildermuth, S.; Zanetti, M.; Duewell, S.; Schmid, M.R.; Romanowski, B.; Benini, A.; Böni, T.; Hodler, J. Lumbar Spine: Quantitative and Qualitative Assessment of Positional (Upright Flexion and Extension) MR Imaging and Myelography. Radiology 1998, 207, 391–398. [Google Scholar] [CrossRef]
- Lee, G.Y.; Guen, Y.L.; Lee, J.W.; Joon, W.L.; Choi, H.S.; Hee, S.C.; Oh, K.-J.; Kyoung-Jin, O.; Kang, H.S.; Heung, S.K. A New Grading System of Lumbar Central Canal Stenosis on MRI: An Easy and Reliable Method. Skelet. Radiol. 2011, 40, 1033–1039. [Google Scholar] [CrossRef] [Green Version]
- Chin, K.R.; Furey, C.; Bohlman, H.H. Risk of Progression in de Novo Low-Magnitude Degenerative Lumbar Curves: Natural History and Literature Review. Am. J. Orthop. (Belle Mead NJ) 2009, 38, 404–409. [Google Scholar]
- Humphreys, S.C.; Hodges, S.D.; Patwardhan, A.G.; Eck, J.C.; Murphy, R.B.; Covington, L.A. Comparison of Posterior and Transforaminal Approaches to Lumbar Interbody Fusion. Spine (Phila Pa 1976) 2001, 26, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Harms, J.G.; Jeszenszky, D. Die Posteriore, Lumbale, Interkorporelle Fusion in Unilateraler Transforaminaler Technik. Orthop. Traumatol. 1998, 10, 90–102. [Google Scholar] [CrossRef]
- Mayer, H.M. A New Microsurgical Technique for Minimally Invasive Anterior Lumbar Interbody Fusion. Spine (Phila Pa 1976) 1997, 22, 691–699, discussion. [Google Scholar] [CrossRef] [PubMed]
- Cummock, M.D.; Vanni, S.; Levi, A.D.; Yu, Y.; Wang, M.Y. An Analysis of Postoperative Thigh Symptoms after Minimally Invasive Transpsoas Lumbar Interbody Fusion. J. Neurosurg. Spine 2011, 15, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, L.; Oliveira, L.; Schaffa, T.; Coutinho, E.; Marchi, L. Lumbar Total Disc Replacement from an Extreme Lateral Approach: Clinical Experience with a Minimum of 2 Years’ Follow-Up. J. Neurosurg. Spine 2011, 14, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.-S.; Lee, H.-J.; Park, E.J.; Kim, S.B.; Choi, D.; Kwon, Y.-S.; Chung, H.-J. Multifidus Muscle Changes after Biportal Endoscopic Spinal Surgery (BESS): Magnetic Resonance Image Evaluation. World Neurosurg. 2019, 130, e525–e534. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.-J.; Jung, J.-T.; Lee, S.-J.; Kim, Y.-S.; Jang, H.-J.; Yoo, B. Biportal Endoscopic Spinal Surgery for Recurrent Lumbar Disc Herniations. Clin. Orthop. Surg. 2016, 8, 325–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria (All of 1–3): |
|---|
| 1. Lower back pain and/or leg pain with neurogenic intermittent claudication (NIC) and a progressive neurological deficit with: |
| - segmental instability |
| >4.5 mm of translation or 15° of angulation evident on a flexion-extension radiograph [18], |
| or |
| - foraminal stenosis |
| moderate to severe based on the Wildermuth grading system [19]. |
| 2. Concomitant, severe central canal stenosis |
| based on the Lumbar central canal stenosis (LCCS) grading system [20]. |
| 3. Failure of 3 months of conservative treatment. |
| Exclusion criteria (any of 1–4): |
| 1. Scoliosis with a Cobb angle > 30° [21] |
| 2. Coexisting pathological conditions |
| - infection,- tumor |
| 3. Trauma |
| 4. Revision surgery |
| Group A | Group B | p-Value | |
|---|---|---|---|
| Patients, no. | 20 | 20 | |
| Mean age ± SD, years | 68.4 ± 5.6 | 66.5 ± 6.8 | 0.34 |
| Male/female ratio | 9:11 | 8:12 | 1.0 |
| Diagnosis (SCCS with), no. (%) | |||
| Foraminal stenosis | 12 (60) | 11 (55) | 0.83 |
| Segmental instability | 3 (15) | 5 (25) | |
| Foraminal stenosis + segmental instability | 5 (25) | 4 (20) | |
| ASA classification ± SD, grade | 2.4 ± 0.5 | 2.2 ± 0.4 | 0.15 |
| Median LOS, days (range) | 14 (11–17) | 14 (13–18) | 0.48 |
| Mean FU ± SD, months | 17.6 ± 5.6 | 19.3 ± 4.5 | 0.30 |
| Mean operative time ± SD, min | 182 ± 42.9 | 167 ± 21.2 | 0.15 |
| Mean EBL ± SD*mL | 151 ± 60.9 | 435 ± 243.0 | 0.00 |
| Fusion segment, no. (%) | |||
| L2–3 | 1 | 0 | 0.74 |
| L3–4 | 2 | 4 | |
| L4–5 | 12 (60) | 10 (50) | |
| L5-S1 | 5 | 6 | |
| Complications, no. | 0 | 0 |
| Group A | p-Value (Compared to the Preoperative Value) | |
|---|---|---|
| VAS back scores | ||
| Preoperative | 5.4 ± 2.4 | |
| 1 month postoperative | 2.3 ± 2.0 | 0.000 |
| 3 months postoperative | 2.2 ± 2.1 | 0.000 |
| 6 months postoperative | 3.1 ± 2.2 | 0.030 |
| 12 months postoperative | 2.6 ± 2.1 | 0.002 |
| Final FU | 2.7 ± 2.2 | 0.003 |
| VAS lower extremity scores | ||
| Preoperative | 6.9 ± 2.1 | |
| 1 month postoperative | 2.6 ± 2.5 | 0.000 |
| 3 months postoperative | 2.3 ± 1.8 | 0.000 |
| 6 months postoperative | 2.9 ± 2.3 | 0.001 |
| 12 months postoperative | 2.5 ± 1.9 | 0.000 |
| Final FU | 2.9 ± 2.0 | 0.001 |
| ODI scores | ||
| Preoperative | 65.2 ± 15.2 | |
| 1 month postoperative | 42.8 ± 14.9 | 0.030 |
| 3 months postoperative | 39.0 ± 14.5 | 0.000 |
| 6 months postoperative | 40.0 ±17.7 | 0.001 |
| 12 months postoperative | 40.5 ± 17.6 | 0.000 |
| Final FU | 40.4 ± 16.5 | 0.001 |
| Modified Macnab criteria (cases, %) | ||
| Excellent | 7 (35) | |
| Good | 10 (50) | |
| Fair | 3 (15) | |
| Poor | 0 (0) |
| Group A | Group B | p-Value | |
|---|---|---|---|
| VAS back scores | |||
| Preoperative | 5.4 ± 2.4 | 4.7 ± 2.3 | 0.35 |
| Final FU | 2.7 ± 2.2 | 3.4 ± 2.2 | 0.36 |
| VAS lower extremity scores | |||
| Preoperative | 6.9 ± 2.1 | 5.8 ± 1.7 | 0.06 |
| Final FU | 2.9 ± 1.9 | 4.2 ± 2.3 | 0.07 |
| ODI scores | |||
| Preoperative* | 65.2 ± 15.2 | 51.9 ± 16.9 | 0.01 |
| Final FU | 40.4 ± 16.5 | 38.2 ± 15.2 | 0.66 |
| Modified Macnab criteria (cases, %) | |||
| Excellent | 7 (35) | 3 (15) | 0.28 |
| Good | 10 (50) | 10 (50) | |
| Fair | 3 (15) | 6 (30) | |
| Poor | 0 (0) | 1 (5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-J.; Park, E.J.; Ahn, J.-S.; Kim, S.B.; Kwon, Y.-S.; Park, Y.-C. Clinical Outcomes of Biportal Endoscopic Interlaminar Decompression with Oblique Lumbar Interbody Fusion (OLIF): Comparative Analysis with TLIF. Brain Sci. 2021, 11, 630. https://doi.org/10.3390/brainsci11050630
Lee H-J, Park EJ, Ahn J-S, Kim SB, Kwon Y-S, Park Y-C. Clinical Outcomes of Biportal Endoscopic Interlaminar Decompression with Oblique Lumbar Interbody Fusion (OLIF): Comparative Analysis with TLIF. Brain Sciences. 2021; 11(5):630. https://doi.org/10.3390/brainsci11050630
Chicago/Turabian StyleLee, Ho-Jin, Eugene J. Park, Jae-Sung Ahn, Sang Bum Kim, Youk-Sang Kwon, and Young-Cheol Park. 2021. "Clinical Outcomes of Biportal Endoscopic Interlaminar Decompression with Oblique Lumbar Interbody Fusion (OLIF): Comparative Analysis with TLIF" Brain Sciences 11, no. 5: 630. https://doi.org/10.3390/brainsci11050630