
Rupture Risk of Intracranial Aneurysm and Prediction of Hemorrhagic Stroke after Liver Transplant

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Unruptured Intracranial Aneurysm Evaluation
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Characteristics of Unruptured Intracranial Aneurysms
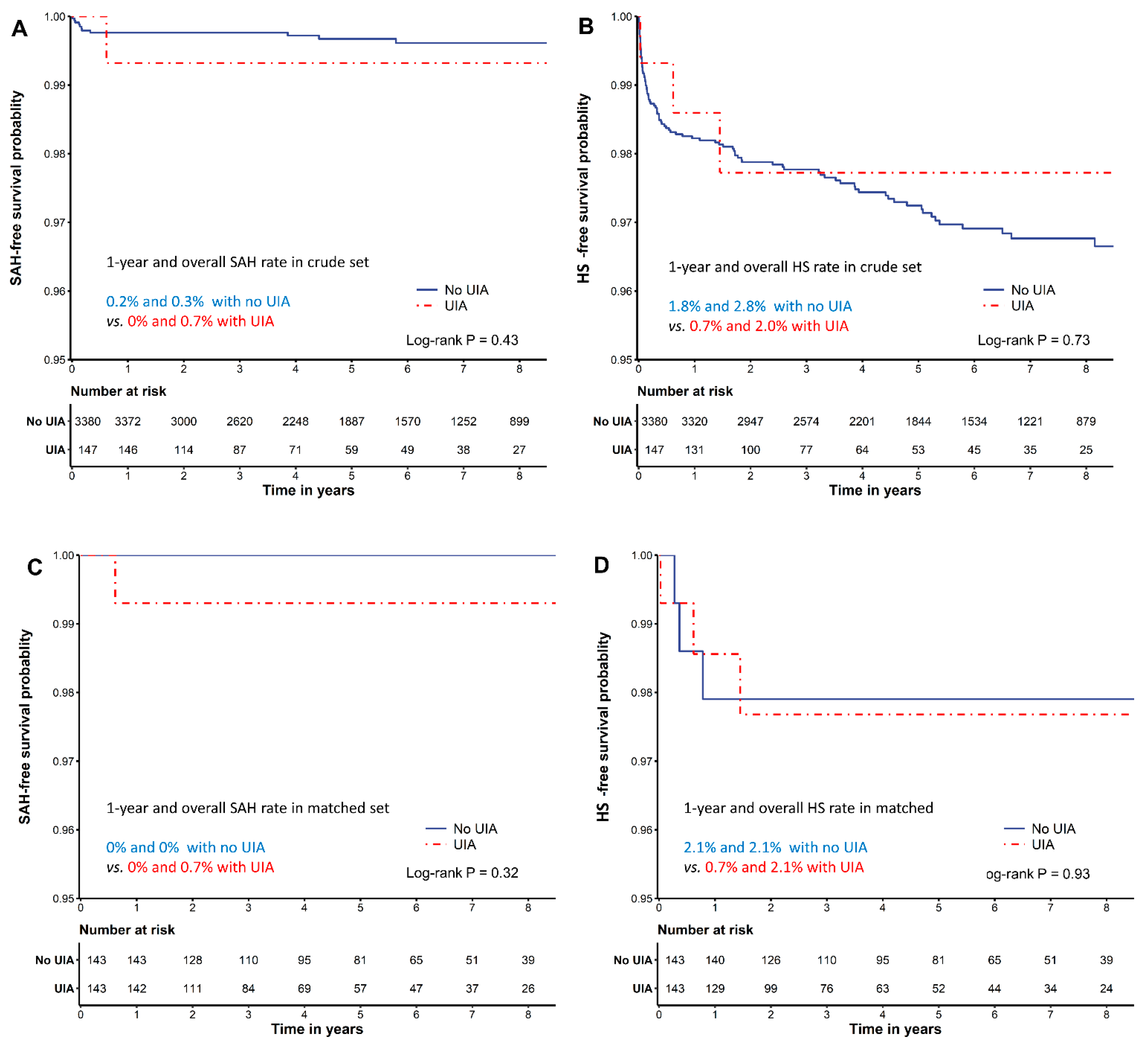
3.3. Postoperative Outcomes of Patients with and without Unruptured Intracranial Aneurysms
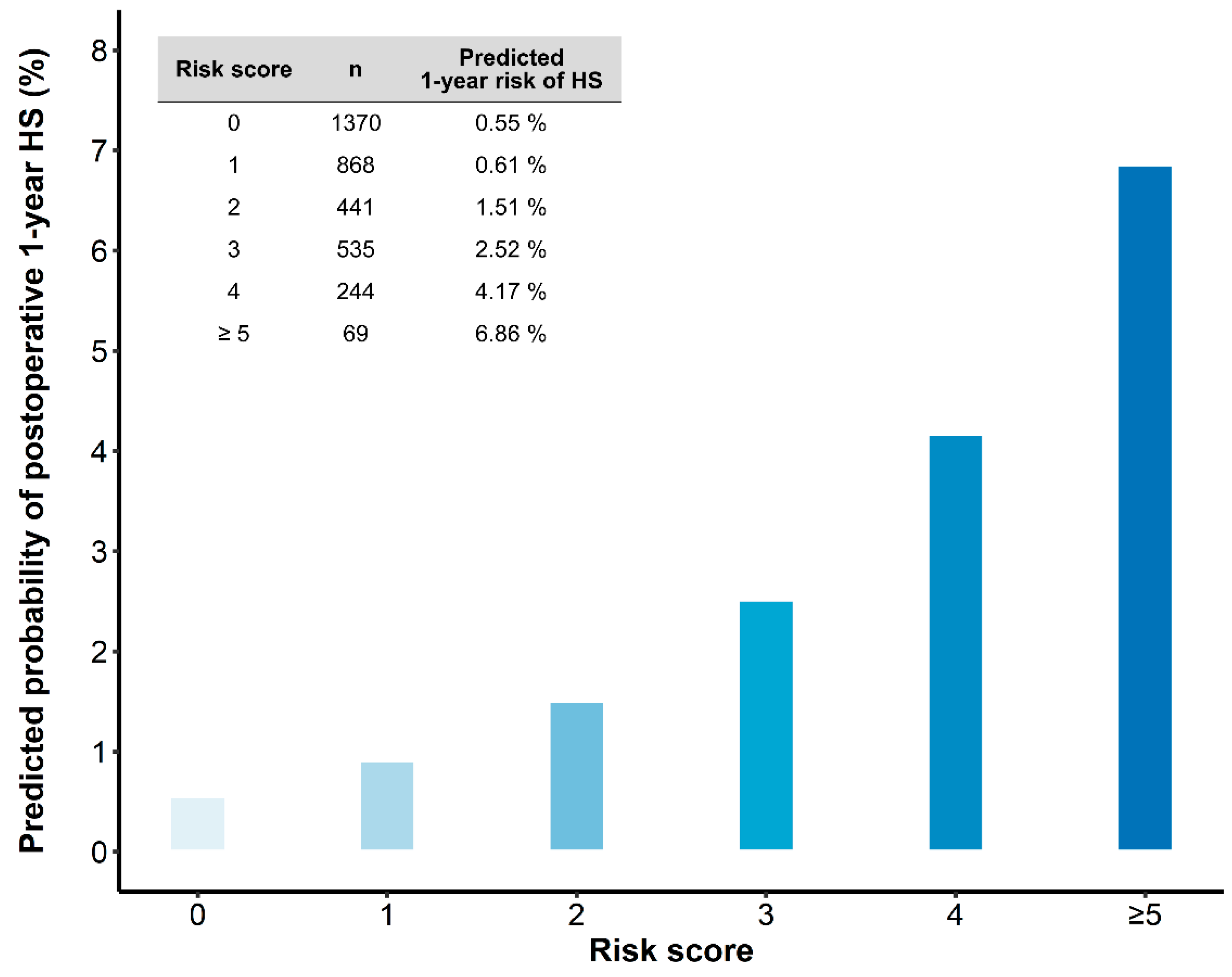
3.4. Risk Factors and Prediction Model of 1-Year Hemorrhagic Stroke
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gallagher, T.K.; Thomas, K.A.; Ladner, D.P.; Ganger, D.; Sorond, F.A.; Prabhakaran, S.; Abecassis, M.M.; Fryer, J.P.; Liotta, E.M. Incidence and Risk Factors of Intracranial Hemorrhage in Liver Transplant Recipients. Transplantation 2018, 102, 448–453. [Google Scholar] [CrossRef]
- Wang, W.L.; Yang, Z.F.; Lo, C.M.; Liu, C.L.; Fan, S.T. Intracerebral hemorrhage after liver transplantation. Liver Transplant. 2000, 6, 345–348. [Google Scholar] [CrossRef]
- Ghaus, N.; Bohlega, S.; Rezeig, M. Neurological complications in liver transplantation. J. Neurol. 2001, 248, 1042–1048. [Google Scholar] [CrossRef]
- Gronbaek, H.; Johnsen, S.P.; Jepsen, P.; Gislum, M.; Vilstrup, H.; Tage-Jensen, U.; Sorensen, H.T. Liver cirrhosis, other liver diseases, and risk of hospitalisation for intracerebral haemorrhage: A Danish population-based case-control study. BMC Gastroenterol. 2008, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Parikh, N.S.; Navi, B.B.; Schneider, Y.; Jesudian, A.; Kamel, H. Association Between Cirrhosis and Stroke in a Nationally Representative Cohort. JAMA Neurol. 2017, 74, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.S.; Navi, B.B.; Kumar, S.; Kamel, H. Association between Liver Disease and Intracranial Hemorrhage. J. Stroke Cerebrovasc. Dis. 2016, 25, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, R.A.; Kim, H.; Sidney, S.; McCulloch, C.E.; Singh, V.; Johnston, S.C.; Ko, N.U.; Achrol, A.S.; Zaroff, J.G.; Young, W.L. Ten-year detection rate of brain arteriovenous malformations in a large, multiethnic, defined population. Stroke 2010, 41, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernooij, M.W.; Ikram, M.A.; Tanghe, H.L.; Vincent, A.J.; Hofman, A.; Krestin, G.P.; Niessen, W.J.; Breteler, M.M.; van der Lugt, A. Incidental findings on brain MRI in the general population. N. Engl. J. Med. 2007, 357, 1821–1828. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.G.; Brown, R.D., Jr.; Amin-Hanjani, S.; Broderick, J.P.; Cockroft, K.M.; Connolly, E.S., Jr.; Duckwiler, G.R.; Harris, C.C.; Howard, V.J.; Johnston, S.C.; et al. Guidelines for the Management of Patients With Unruptured Intracranial Aneurysms: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2368–2400. [Google Scholar] [CrossRef] [Green Version]
- Darsaut, T.E.; Estrade, L.; Jamali, S.; Bojanowski, M.W.; Chagnon, M.; Raymond, J. Uncertainty and agreement in the management of unruptured intracranial aneurysms. J. Neurosurg. 2014, 120, 618–623. [Google Scholar] [CrossRef]
- Kim, Y.W.; Neal, D.; Hoh, B.L. Cerebral aneurysms in pregnancy and delivery: Pregnancy and delivery do not increase the risk of aneurysm rupture. Neurosurgery 2013, 72, 143–149; discussion 150. [Google Scholar] [CrossRef]
- Etminan, N.; Rinkel, G.J. Cerebral aneurysms: Cerebral aneurysm guidelines-more guidance needed. Nat. Rev. Neurol. 2015, 11, 490–491. [Google Scholar] [CrossRef] [PubMed]
- Perrini, P.; Montemurro, N.; Caniglia, M.; Lazzarotti, G.; Benedetto, N. Wrapping of intracranial aneurysms: Single-center series and systematic review of the literature. Br. J. Neurosurg. 2015, 29, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Choudhari, K.A. Wrapping and coating of cerebral aneurysms: History, evolution and surgical management after a re-bleed. Br. J. Neurosurg. 2004, 18, 259–267. [Google Scholar] [CrossRef]
- Etminan, N.; Rinkel, G.J. Unruptured intracranial aneurysms: Development, rupture and preventive management. Nat. Rev. Neurol. 2016, 12, 699–713. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.D., Jr.; Broderick, J.P. Unruptured intracranial aneurysms: Epidemiology, natural history, management options, and familial screening. Lancet Neurol. 2014, 13, 393–404. [Google Scholar] [CrossRef]
- Parikh, N.S.; Merkler, A.E.; Jesudian, A.; Kamel, H. Association between cirrhosis and aneurysmal subarachnoid hemorrhage. Ann. Clin. Transl. Neurol. 2019, 6, 27–32. [Google Scholar] [CrossRef]
- Cebral, J.R.; Mut, F.; Weir, J.; Putman, C.M. Association of hemodynamic characteristics and cerebral aneurysm rupture. AJNR Am. J. Neuroradiol. 2011, 32, 264–270. [Google Scholar] [CrossRef]
- Al-Hamoudi, W.K.; Alqahtani, S.; Tandon, P.; Ma, M.; Lee, S.S. Hemodynamics in the immediate post-transplantation period in alcoholic and viral cirrhosis. World J. Gastroenterol. 2010, 16, 608–612. [Google Scholar] [CrossRef]
- Weiss, N.; Thabut, D. Neurological Complications Occurring After Liver Transplantation: Role of Risk Factors, Hepatic Encephalopathy, and Acute (on Chronic) Brain Injury. Liver Transplant. 2019, 25, 469–487. [Google Scholar] [CrossRef]
- Greving, J.P.; Wermer, M.J.; Brown, R.D., Jr.; Morita, A.; Juvela, S.; Yonekura, M.; Ishibashi, T.; Torner, J.C.; Nakayama, T.; Rinkel, G.J.; et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: A pooled analysis of six prospective cohort studies. Lancet Neurol. 2014, 13, 59–66. [Google Scholar] [CrossRef]
- Tominari, S.; Morita, A.; Ishibashi, T.; Yamazaki, T.; Takao, H.; Murayama, Y.; Sonobe, M.; Yonekura, M.; Saito, N.; Shiokawa, Y.; et al. Prediction model for 3-year rupture risk of unruptured cerebral aneurysms in Japanese patients. Ann. Neurol. 2015, 77, 1050–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byoun, H.S.; Huh, W.; Oh, C.W.; Bang, J.S.; Hwang, G.; Kwon, O.K. Natural History of Unruptured Intracranial Aneurysms: A Retrospective Single Center Analysis. J. Korean Neurosurg. Soc. 2016, 59, 11–16. [Google Scholar] [CrossRef]
- Demler, O.V.; Paynter, N.P.; Cook, N.R. Tests of calibration and goodness-of-fit in the survival setting. Stat. Med. 2015, 34, 1659–1680. [Google Scholar] [CrossRef] [Green Version]
- Investigators, U.J.; Morita, A.; Kirino, T.; Hashi, K.; Aoki, N.; Fukuhara, S.; Hashimoto, N.; Nakayama, T.; Sakai, M.; Teramoto, A.; et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N. Engl. J. Med. 2012, 366, 2474–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.C.; Hsu, P.W.; Lee, S.T.; Chang, C.N.; Wei, K.C.; Wu, C.T.; Hsu, Y.H.; Lin, T.K.; Lee, S.C.; Huang, Y.C. Brain surgery in patients with liver cirrhosis. J. Neurosurg. 2012, 117, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Marrocco-Trischitta, M.M.; Kahlberg, A.; Astore, D.; Tshiombo, G.; Mascia, D.; Chiesa, R. Outcome in cirrhotic patients after elective surgical repair of infrarenal aortic aneurysm. J. Vasc. Surg. 2011, 53, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlak, M.H.; Algra, A.; Brandenburg, R.; Rinkel, G.J. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011, 10, 626–636. [Google Scholar] [CrossRef]
- Nam, J.S.; Jeon, S.B.; Jo, J.Y.; Joung, K.W.; Chin, J.H.; Lee, E.H.; Chung, C.H.; Choi, I.C. Perioperative rupture risk of unruptured intracranial aneurysms in cardiovascular surgery. Brain 2019, 142, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.M.; Hwang, G.S. Cardiovascular dysfunction and liver transplantation. Korean J. Anesthesiol. 2018, 71, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.D.; Song, D.; Heo, J.H.; Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, K.J.; Han, K.H. Relationship between Cerebral Microbleeds and Liver Stiffness Determined by Transient Elastography. PLoS ONE 2015, 10, e0139227. [Google Scholar] [CrossRef]
- Lee, S.G. A complete treatment of adult living donor liver transplantation: A review of surgical technique and current challenges to expand indication of patients. Am. J. Transplant. 2015, 15, 17–38. [Google Scholar] [CrossRef]
- Ariesen, M.J.; Claus, S.P.; Rinkel, G.J.; Algra, A. Risk factors for intracerebral hemorrhage in the general population: A systematic review. Stroke 2003, 34, 2060–2065. [Google Scholar] [CrossRef]
- Aronowski, J.; Hall, C.E. New horizons for primary intracerebral hemorrhage treatment: Experience from preclinical studies. Neurol. Res. 2005, 27, 268–279. [Google Scholar] [CrossRef]
- Di Napoli, M.; Slevin, M.; Popa-Wagner, A.; Singh, P.; Lattanzi, S.; Divani, A.A. Monomeric C-Reactive Protein and Cerebral Hemorrhage: From Bench to Bedside. Front. Immunol. 2018, 9, 1921. [Google Scholar] [CrossRef]
- Prelipcean, C.C.; Fierbinteanu-Braticevici, C.; Drug, V.L.; Lacatusu, C.; Mihai, B.; Mihai, C. Liver cirrhosis--procoagulant stasis. Rev. Med. Chir. Soc. Med. Nat. Iasi 2011, 115, 678–685. [Google Scholar] [PubMed]
- Strauss, G.I.; Hansen, B.A.; Herzog, T.; Larsen, F.S. Cerebral autoregulation in patients with end-stage liver disease. Eur. J. Gastroenterol. Hepatol. 2000, 12, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Pere, P.; Hockerstedt, K.; Isoniemi, H.; Lindgren, L. Cerebral blood flow and oxygenation in liver transplantation for acute or chronic hepatic disease without venovenous bypass. Liver Transplant. 2000, 6, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; de Groen, P.C.; Wiesner, R.H.; Krom, R.A. Intracerebral hemorrhage in liver transplant recipients. Mayo Clin. Proc. 1995, 70, 443–446. [Google Scholar] [CrossRef]
- Zheng, K.; Yoshida, E.M.; Tacke, F.; Li, Y.; Guo, X.; Qi, X. Risk of Stroke in Liver Cirrhosis: A Systematic Review and Meta-Analysis. J. Clin. Gastroenterol. 2020, 54, 96–105. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Crude Cohort | PS-Matched Cohort | ||||||
|---|---|---|---|---|---|---|---|
| No UIA | UIA | p Value | No UIA | UIA | p Value | SMD | |
| n = 3382 (95.4%) | n = 162 (4.6%) | n = 143 | n = 143 | ||||
| Age, years | 52.7 ± 9.1 | 54.1 ± 7.9 | 0.028 | 54.0 ± 8.1 | 54.4 ± 8.1 | 0.683 | 0.048 |
| Sex, (men) | 2492 (73.7) | 99 (60.4) | <0.001 | 82 (57.3) | 86 (60.1) | 0.719 | 0.057 |
| Body mass index, kg m−² | 24.1 (21.9–26.5) | 24.0 (21.7–26.4) | 0.798 | 23.5 (21.7–26.0) | 24.0 (21.6–26.4) | 0.671 | 0.005 |
| MELDs | 15 (10–25) | 13 (10–24) | 0.300 | 13 (9–20) | 13 (10–23) | 0.343 | 0.071 |
| <20 | 2193 (64.9) | 109 (66.5) | 105 (73.4) | 97 (67.8) | |||
| 20–39 | 938 (27.8) | 49 (29.9) | 32 (22.4) | 41 (28.7) | |||
| ≥40 | 249 (7.4) | 6 (3.7) | 6 (4.2) | 5 (3.5) | |||
| Diabetes | 794 (23.5) | 43 (26.2) | 0.478 | 39 (27.3) | 36 (25.2) | 0.788 | 0.048 |
| Hypertension | 588 (17.4) | 41 (25.0) | 0.017 | 28 (19.6) | 33 (23.1) | 0.564 | 0.085 |
| Systolic blood pressure (SBP) | 109 (101–119) | 111 (101–120) | 0.509 | 108 (100–117) | 110 (101–118) | 0.560 | 0.032 |
| SBP > 130 mmHg | 316 (9.3) | 13 (7.9) | 0.635 | 11 (7.7) | 8 (5.6) | 0.635 | 0.084 |
| Current smoker | 343 (10.1) | 20 (12.2) | 0.476 | 16 (11.2) | 16 (11.2) | 1.000 | <0.001 |
| Dyslipidemia | 608 (18.0) | 32 (19.5) | 0.695 | 29 (20.3) | 28 (19.6) | 1.000 | 0.018 |
| History of SAH | 21 (0.6) | 15 (9.1) | <0.001 | 3 (2.1) | 5 (3.5) | 0.720 | 0.085 |
| Etiology of cirrhosis | 0.903 | 0.745 | 0.091 | ||||
| Viral cirrhosis | 2165 (64.1) | 104 (63.4) | 97 (67.8) | 96 (67.1) | |||
| Alcoholic cirrhosis | 661 (19.6) | 31 (18.9) | 17 (11.9) | 21 (14.7) | |||
| Others | 554 (16.4) | 29 (17.7) | 29 (20.3) | 26 (18.2) | |||
| Combined HCC | 1516 (44.9) | 76 (46.3) | 0.769 | 72 (50.3) | 67 (46.9) | 0.636 | 0.070 |
| No SAH | SAH | Treated | Total | ||
|---|---|---|---|---|---|
| n = 128 | n = 1 | n = 18 | n = 147 | ||
| Modality | DSA | 5 (3.9) | 0 (0.0) | 1 (5.6) | 6 (4.1) |
| CT | 18 (14.1) | 0 (0.0) | 9 (50.0) | 27 (18.4) | |
| MRI | 105 (82.0) | 1 (100.0) | 8 (44.4) | 114 (77.6) | |
| Multiple UIAs | 18 (14.1) | 0 (0.0) | 4 (22.2) | 22 (15.0) | |
| Daughter sac | 6 (4.7) | 0 (0.0) | 2 (11.1) | 8 (5.4) | |
| Size, mm * | <3 mm | 78 (60.9) | 1 (100.0) | 2 (11.1) | 81 (55.1) |
| 3–6.9 mm | 42 (32.8) | 0 (0.0) | 9 (50.0) | 51 (34.7) | |
| 7–9.9 mm | 4 (3.1) | 0 (0.0) | 4 (22.2) | 8 (5.4) | |
| 10–19.9 mm | 3 (2.3) | 0 (0.0) | 3 (16.7) | 6 (4.1) | |
| ≥20 mm | 1 (0.8) | 0 (0.0) | 0 (0.0) | 1 (0.7) | |
| Location | Anterior cerebral artery | 6 (4.7) | 0 (0.0) | 1 (5.6) | 7 (4.8) |
| Anterior communicating artery | 13 (10.2) | 0 (0.0) | 6 (33.3) | 19 (12.9) | |
| Basilar artery | 4 (3.1) | 0 (0.0) | 1 (5.6) | 5 (3.4) | |
| Internal carotid artery | 72 (56.2) | 1 (100.0) | 1 (5.6) | 74 (50.3) | |
| Posterior communicating artery | 6 (4.7) | 0 (0.0) | 2 (11.1) | 8 (5.4) | |
| Middle cerebral artery | 25 (19.5) | 0 (0.0) | 6 (33.3) | 31 (21.1) | |
| Vertebral artery | 0 (0.0) | 0 (0.0) | 1 (5.6) | 1 (0.7) | |
| Other | 2 (1.6) | 0 (0.0) | 0 (0.0) | 2 (1.4) | |
| PHASES score † | ≤4 | 70 (54.7) | 1 (100.0) | 1 (5.6) | 72 (49.0) |
| 5–7 | 47 (36.7) | 0 (0.0) | 12 (66.7) | 59 (40.1) | |
| 8–11 | 11 (8.6) | 0 (0.0) | 5 (27.8) | 16 (10.9) | |
| UCAS Japan score ‡ | ≤3 | 109 (85.2) | 1 (100.0) | 11 (61.1) | 121 (82.3) |
| 4–5 | 18 (14.1) | 0 (0.0) | 6 (33.3) | 24 (16.3) | |
| 6–8 | 1 (0.8) | 0 (0.0) | 1 (5.6) | 2 (1.4) |
| Risk Factors | Points * | β Coefficient | Adjusted HR [95% CI] | p-Value |
|---|---|---|---|---|
| MELDs | ||||
| <20 | 0 | 1 | ||
| 20–39 | 2 | 1.26 | 3.51 (1.88–6.53) | 0.001 |
| ≥40 | 3 | 1.74 | 5.69 (2.62–12.33) | <0.001 |
| History of SAH | ||||
| No | 0 | 1 | ||
| Yes | 3 | 1.63 | 5.09 (1.24–20.98) | 0.024 |
| Platelets | ||||
| >50,000 dL−1 | 0 | 1 | ||
| ≤50,000 dL−1 | 1 | 0.57 | 1.78 (1.07–2.94) | 0.026 |
| C-reactive protein | ||||
| <1.8 mg dL−1 | 0 | 1 | ||
| ≥1.8 mg dL−1 | 1 | 0.51 | 1.67 (0.94–2.96) | 0.080 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.-M.; Jun, I.-G.; Kim, K.-S.; Moon, Y.-J.; Huh, I.Y.; Lee, J.; Song, J.-G.; Hwang, G.-S. Rupture Risk of Intracranial Aneurysm and Prediction of Hemorrhagic Stroke after Liver Transplant. Brain Sci. 2021, 11, 445. https://doi.org/10.3390/brainsci11040445
Kwon H-M, Jun I-G, Kim K-S, Moon Y-J, Huh IY, Lee J, Song J-G, Hwang G-S. Rupture Risk of Intracranial Aneurysm and Prediction of Hemorrhagic Stroke after Liver Transplant. Brain Sciences. 2021; 11(4):445. https://doi.org/10.3390/brainsci11040445
Chicago/Turabian StyleKwon, Hye-Mee, In-Gu Jun, Kyoung-Sun Kim, Young-Jin Moon, In Young Huh, Jungmin Lee, Jun-Gol Song, and Gyu-Sam Hwang. 2021. "Rupture Risk of Intracranial Aneurysm and Prediction of Hemorrhagic Stroke after Liver Transplant" Brain Sciences 11, no. 4: 445. https://doi.org/10.3390/brainsci11040445