Age-Related Differences in Arm and Trunk Responses to First and Repeated Exposure to Laterally Induced Imbalances


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. First and Last Trial Age-Related Differences
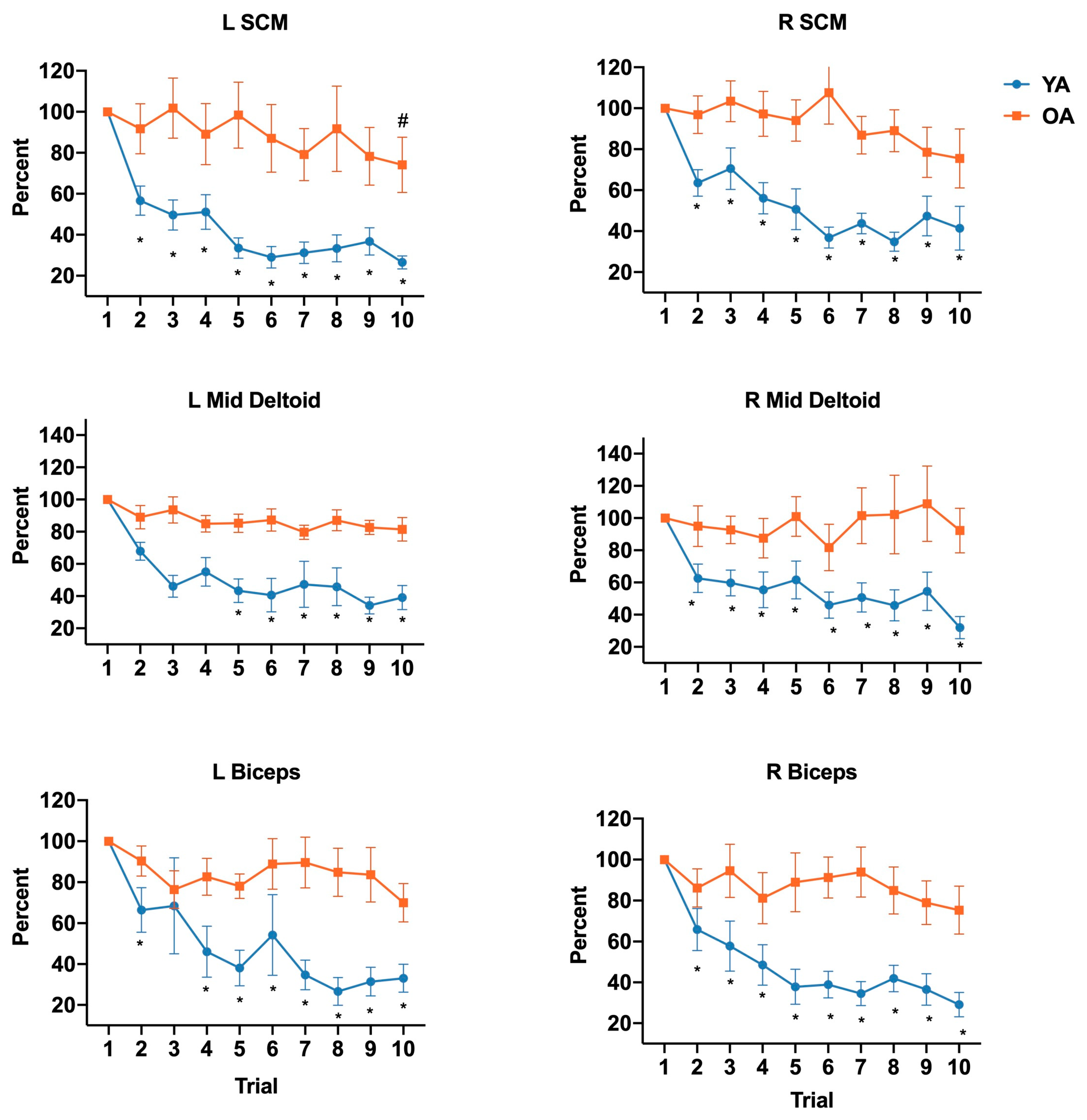
3.2. Habituation
3.3. Step Types
3.4. Harness Assistance and Balance Confidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dietz, V.; Fouad, K.; Bastiaanse, C.M. Neuronal coordination of arm and leg movements during human locomotion. Eur. J. Neurosci. 2001, 14, 1906–1914. [Google Scholar] [CrossRef]
- Misiaszek, J.E. Early activation of arm and leg muscles following pulls to the waist during walking. Exp. Brain Res. 2003, 151, 318–329. [Google Scholar] [CrossRef]
- Misiaszek, J.E.; Krauss, E.M. Restricting arm use enhances compensatory reactions of leg muscles during walking. Exp. Brain Res. 2004, 161, 474–485. [Google Scholar] [CrossRef]
- Marigold, D.S.; Misiaszek, J.E. Whole-Body Responses: Neural Control and Implications for Rehabilitation and Fall Prevention. Neuroscientist 2008, 15, 36–46. [Google Scholar] [CrossRef]
- Pijnappels, M.; Kingma, I.; Wezenberg, D.; Reurink, G.; Van Dieën, J.H.; Reurink, G. Armed against falls: The contribution of arm movements to balance recovery after tripping. Exp. Brain Res. 2009, 201, 689–699. [Google Scholar] [CrossRef] [Green Version]
- Grin, L.; Frank, J.; Allum, J.H.J. The effect of voluntary arm abduction on balance recovery following multidirectional stance perturbations. Exp. Brain Res. 2006, 178, 62–78. [Google Scholar] [CrossRef] [Green Version]
- Holliday, P.; Fernie, G.; Gryfe, C.; Griggs, G. Video Recording of Spontaneous Falls of the Elderly. In Slips, Stumbles, and Falls: Pedestrian Footwear and Surfaces; ASTM International: West Conshohocken, PA, USA, 2009; Volume 7. [Google Scholar] [CrossRef]
- Yang, Y.; Mackey, D.C.; Liu-Ambrose, T.; Leung, P.-M.; Feldman, F.; Robinovitch, S.N. Clinical Risk Factors for Head Impact During Falls in Older Adults. J. Head Trauma Rehabil. 2017, 32, 168–177. [Google Scholar] [CrossRef]
- Schonnop, R.; Yang, Y.; Feldman, F.; Robinson, E.; Loughin, M.; Robinovitch, S.N. Prevalence of and factors associated with head impact during falls in older adults in long-term care. Can. Med Assoc. J. 2013, 185, E803–E810. [Google Scholar] [CrossRef] [Green Version]
- Maki, B.E.; Edmondstone, M.A.; McIlroy, W.E.; Hagerman, F.C.; Walsh, S.J.; Staron, R.S.; Hikida, R.S.; Gilders, R.M.; Murray, T.F.; Toma, K.; et al. Age-Related Differences in Laterally Directed Compensatory Stepping Behavior. J. Gerontol. Ser. A: Boil. Sci. Med Sci. 2000, 55, M270–M277. [Google Scholar] [CrossRef]
- Tang, P.-F.; Woollacott, M.H. Inefficient postural responses to unexpected slips during walking in older adults. J. Gerontol. Ser. A Boil. Sci. Med Sci. 1998, 53, M471–M480. [Google Scholar] [CrossRef]
- Allum, J.H.J.; Carpenter, M.G.; Honegger, F.; Adkin, A.L.; Bloem, B.R. Age-dependent variations in the directional sensitivity of balance corrections and compensatory arm movements in man. J. Physiol. 2002, 542, 643–663. [Google Scholar] [CrossRef]
- Roos, P.E.; McGuigan, M.P.; Kerwin, D.G.; Trewartha, G. The role of arm movement in early trip recovery in younger and older adults. Gait Posture 2008, 27, 352–356. [Google Scholar] [CrossRef] [Green Version]
- Nijhuis, L.B.O.; Allum, J.H.J.; Valls-Solé, J.; Overeem, S.; Bloem, B.R. First Trial Postural Reactions to Unexpected Balance Disturbances: A Comparison with the Acoustic Startle Reaction. J. Neurophysiol. 2010, 104, 2704–2712. [Google Scholar] [CrossRef] [Green Version]
- Blouin, J.-S.; Siegmund, G.P.; Inglis, J.T. Interaction between acoustic startle and habituated neck postural responses in seated subjects. J. Appl. Physiol. 2007, 102, 1574–1586. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.; Falls, W.A.; Campeau, S.; Kim, M. Fear-potentiated startle: A neural and pharmacological analysis. Behav. Brain Res. 1993, 58, 175–198. [Google Scholar] [CrossRef]
- Sanders, O.; Hsiao, H.Y.; Savin, D.N.; Creath, R.A.; Rogers, M. Aging changes in protective balance and startle responses to sudden drop perturbations. J. Neurophysiol. 2019, 122, 39–50. [Google Scholar] [CrossRef]
- Shelkey, M.; Wallace, M. Katz Index of Independence in Activities of Daily Living (ADL). Directories (Cincinnati Ohio) 2000, 8, 72–73. [Google Scholar]
- Cheng, K.C.; McKay, S.M.; King, E.C.; Maki, B.E. Reaching to recover balance in unpredictable circumstances: Is online visual control of the reach-to-grasp reaction necessary or sufficient? Exp. Brain Res. 2012, 218, 589–599. [Google Scholar] [CrossRef] [Green Version]
- Weaver, T.B.; Tokuno, C.D. The influence of handrail predictability on compensatory arm reactions in response to a loss of balance. Gait Posture 2013, 38, 293–298. [Google Scholar] [CrossRef]
- Mille, M.-L.; Johnson-Hilliard, M.; Martinez, K.M.; Zhang, Y.; Edwards, B.J.; Rogers, M.W. One Step, Two Steps, Three Steps More … Directional Vulnerability to Falls in Community-Dwelling Older People. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2013, 68, 1540–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilliard, M.J.; Martinez, K.M.; Janssen, I.; Edwards, B.J.; Mille, M.-L.; Zhang, Y.; Rogers, M.W. Lateral Balance Factors Predict Future Falls in Community-Living Older Adults. Arch. Phys. Med. Rehabil. 2008, 89, 1708–1713. [Google Scholar] [CrossRef] [Green Version]
- Maki, B.E.; McIlroy, W.E. Control of rapid limb movements for balance recovery: Age-related changes and implications for fall prevention. Age Ageing 2006, 35, ii12–ii18. [Google Scholar] [CrossRef] [Green Version]
- Yang, F.; Pai, Y.-C. Automatic recognition of falls in gait-slip training: Harness load cell based criteria. J. Biomech. 2011, 44, 2243–2249. [Google Scholar] [CrossRef] [Green Version]
- Keshner, E.; Allum, J.; Pfaltz, C. Postural coactivation and adaptation in the sway stabilizing responses of normals and patients with bilateral vestibular deficit. Exp. Brain Res. 1987, 69, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, L.B.O.; Allum, J.H.J.; Borm, G.F.; Honegger, F.; Overeem, S.; Bloem, B.R. Directional Sensitivity of “First Trial” Reactions in Human Balance Control. J. Neurophysiol. 2009, 101, 2802–2814. [Google Scholar] [CrossRef] [PubMed]
- Merriaux, P.; Dupuis, Y.; Boutteau, R.; Vasseur, P.; Savatier, X. A Study of Vicon System Positioning Performance. Sensors 2017, 17, 1591. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. Ser. A Boil. Sci. Med Sci. 1995, M28–M34. [Google Scholar] [CrossRef]
- Ganesan, M.; Kanekar, N.; Aruin, A.S. Direction-specific impairments of limits of stability in individuals with multiple sclerosis. Ann. Phys. Rehabil. Med. 2015, 58, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Dreissen, Y.E.; Bakker, M.J.; Koelman, J.H.; Tijssen, M.A. Exaggerated startle reactions. Clin. Neurophysiol. 2012, 123, 34–44. [Google Scholar] [CrossRef]
- Mille, M.-L.; Johnson, M.E.; Martinez, K.M.; Rogers, M.W. Age-dependent differences in lateral balance recovery through protective stepping. Clin. Biomech. 2005, 20, 607–616. [Google Scholar] [CrossRef]
- Maki, B.E. Gait Changes in Older Adults: Predictors of Falls or Indicators of Fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. A structural equation model relating impaired sensorimotor function, fear of falling and gait patterns in older people. Gait Posture 2007, 25, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, M.G.; Frank, J.S.; Silcher, C.P. Surface height effects on postural control: A hypothesis for a stiffness strategy for stance. J. Vestib. Res. 1999, 9, 277–286. [Google Scholar] [PubMed]
- Carpenter, M.G.; Frank, J.S.; Adkin, A.L.; Paton, A.; Allum, J. Influence of Postural Anxiety on Postural Reactions to Multi-Directional Surface Rotations. J. Neurophysiol. 2004, 92, 3255–3265. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.C.; Landis, C.; Hunt, W.A. The Startle Pattern. Am. J. Psychol. 1941, 54, 148. [Google Scholar] [CrossRef]
- Nieuwenhuijzen, P.; Schillings, A.M.; Van Galen, G.P.; Duysens, J. Modulation of the startle response during human gait. J. Neurophysiol. 2000, 84, 65–74. [Google Scholar] [CrossRef]
- Brown, P.; Day, B.L.; Rothwell, J.C.; Thompson, P.D.; Marsden, C.D. The effect of posture on the normal and pathological auditory startle reflex. J. Neurol. Neurosurg. Psychiatry 1991, 54, 892–897. [Google Scholar] [CrossRef] [Green Version]
- Westlake, K.P.; Wu, Y.; Culham, E.G. Velocity discrimination: Reliability and construct validity in older adults. Hum. Mov. Sci. 2007, 26, 443–456. [Google Scholar] [CrossRef]
- Westlake, K.P.; Culham, E.G. Sensory-Specific Balance Training in Older Adults: Effect on Proprioceptive Reintegration and Cognitive Demands. Phys. Ther. 2007, 87, 1274–1283. [Google Scholar] [CrossRef]
- Allum, J.H.J.; Nijhuis, L.B.O.; Carpenter, M.G. Differences in coding provided by proprioceptive and vestibular sensory signals may contribute to lateral instability in vestibular loss subjects. Exp. Brain Res. 2007, 184, 391–410. [Google Scholar] [CrossRef] [Green Version]
- Thelen, D.; Wojcik, L.A.; Schultz, A.B.; Ashton-Miller, J.A.; Alexander, N.B. Age Differences in Using a Rapid Step to Regain Balance during a Forward Fall. J. Gerontol. Ser. A Boil. Sci. Med Sci. 1997, 52, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.W.; Mille, M.-L. Lateral Stability and Falls in Older People. Exerc. Sport Sci. Rev. 2003, 31, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Lattimer, L.J.; Lanovaz, J.L.; Farthing, J.P.; Madill, S.J.; Kim, S.; Arnold, C. Upper limb and trunk muscle activation during an unexpected descent on the outstretched hands in young and older women. J. Electromyogr. Kinesiol. 2016, 30, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E.; Holliday, P.J.; Topper, A.K. Fear of Falling and Postural Performance in the Elderly. J. Gerontol. 1991, 46, M123–M131. [Google Scholar] [CrossRef] [PubMed]
- Allum, J.H.J.; Tang, K.-S.; Carpenter, M.; Nijhuis, L.O.; Bloem, B. Review of first trial responses in balance control: Influence of vestibular loss and Parkinson’s disease. Hum. Mov. Sci. 2011, 30, 279–295. [Google Scholar] [CrossRef]
- Inacio, M.; Creath, R.; Rogers, M.W. Effects of aging on hip abductor-adductor neuromuscular and mechanical performance during the weight transfer phase of lateral protective stepping. J. Biomech. 2019, 82, 244–250. [Google Scholar] [CrossRef]
- Nanhoe-Mahabier, W.; Allum, J.H.J.; Overeem, S.; Borm, G.; Nijhuis, L.O.; Bloem, B.R. First trial reactions and habituation rates over successive balance perturbations in Parkinson’s disease. Neuroscientist 2012, 217, 123–129. [Google Scholar] [CrossRef]
- Siegmund, G.P.; Blouin, J.-S.; Inglis, J.T. Does Startle Explain the Exaggerated First Response to a Transient Perturbation? Exerc. Sport Sci. Rev. 2008, 36, 76–82. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Muscle | Older Adults | Younger Adults | p-Value | ||
|---|---|---|---|---|---|
| Trial 1 | Trial 1 0 | Trial 1 | Trial 10 | ||
| Left SCM | 140.9 ± 12.89 | 122.8 ± 9.00 | 127.8 ± 15.18 | 128.4 ± 12.69 | 0.79 |
| Right SCM | 144.4 ± 14.43 | 141.9 ± 8.57 | 124.3 ± 11.53 | 147.8 ± 12.80 | 0.61 |
| Left Mid Deltoid | 139.6 ± 13.06 | 131.0 ± 6.74 | 125.8 ± 10.58 | 132.5 ± 10.61 | 0.59 |
| Right Mid Deltoid | 142.7 ± 12.37 | 125.3 ± 8.37 | 120.6 ± 10.94 | 125.5 ± 10.37 | 0.36 |
| Left Biceps | 149.6 ± 12.61 | 129.3 ± 9.42 | 126.9 ± 11.12 | 140.9 ± 13.08 | 0.68 |
| Right Biceps | 147.7 ± 13.89 | 144.7 ± 8.43 | 128.6 ± 10.95 | 140.0 ± 11.00 | 0.36 |
| FFLO Onset Latency | 263.6 ± 19.55 | 226.4 ± 9.17 | 216.4 ± 8.45 | 214.5 ± 9.28 | 0.03 * |
| Muscle | Older Adults | Younger Adults | p-Value | ||
|---|---|---|---|---|---|
| Trial 1 | Trial 10 | Trial 1 | Trial 10 | ||
| Left SCM | 272.9 ± 21.27 | 167.6 ± 1.16 | 127.8 ± 1.10 | 135.6 ± 1.11 | 0.01 * |
| Right SCM | 161.1 ± 1.24 | 129.9 ± 1.06 | 148.2 ± 1.15 | 122.0 ± 3.59 | 0.66 |
| Left Mid Deltoid | 199.5 ± 8.31 | 126.0 ± 2.05 | 122.9 ± 1.06 | 117.0 ± 1.11 | 0.03 * |
| Right Mid Deltoid | 307.3 ± 1.25 | 137.9 ± 1.19 | 128.3 ± 1.06 | 137.9 ± 1.13 | 0.04 † |
| Left Biceps | 221.9 ± 1.22 | 151.9 ± 1.07 | 124.8 ± 1.08 | 136.6 ± 1.13 | 0.02 * |
| Right Biceps | 319.2 ± 1.25 | 124.8 ± 1.08 | 122.7 ± 1.05 | 147.9 ± 1.19 | 0.01 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akinlosotu, R.Y.; Alissa, N.; Sorkin, J.D.; Wittenberg, G.F.; Westlake, K.P. Age-Related Differences in Arm and Trunk Responses to First and Repeated Exposure to Laterally Induced Imbalances. Brain Sci. 2020, 10, 574. https://doi.org/10.3390/brainsci10090574
Akinlosotu RY, Alissa N, Sorkin JD, Wittenberg GF, Westlake KP. Age-Related Differences in Arm and Trunk Responses to First and Repeated Exposure to Laterally Induced Imbalances. Brain Sciences. 2020; 10(9):574. https://doi.org/10.3390/brainsci10090574
Chicago/Turabian StyleAkinlosotu, Ruth Y., Nesreen Alissa, John D. Sorkin, George F. Wittenberg, and Kelly P. Westlake. 2020. "Age-Related Differences in Arm and Trunk Responses to First and Repeated Exposure to Laterally Induced Imbalances" Brain Sciences 10, no. 9: 574. https://doi.org/10.3390/brainsci10090574