Arteriovenous Fistula Flow Dysfunction Surveillance: Early Detection Using Pulse Radar Sensor and Machine Learning Classification


Abstract
:1. Introduction
2. Materials and Methods
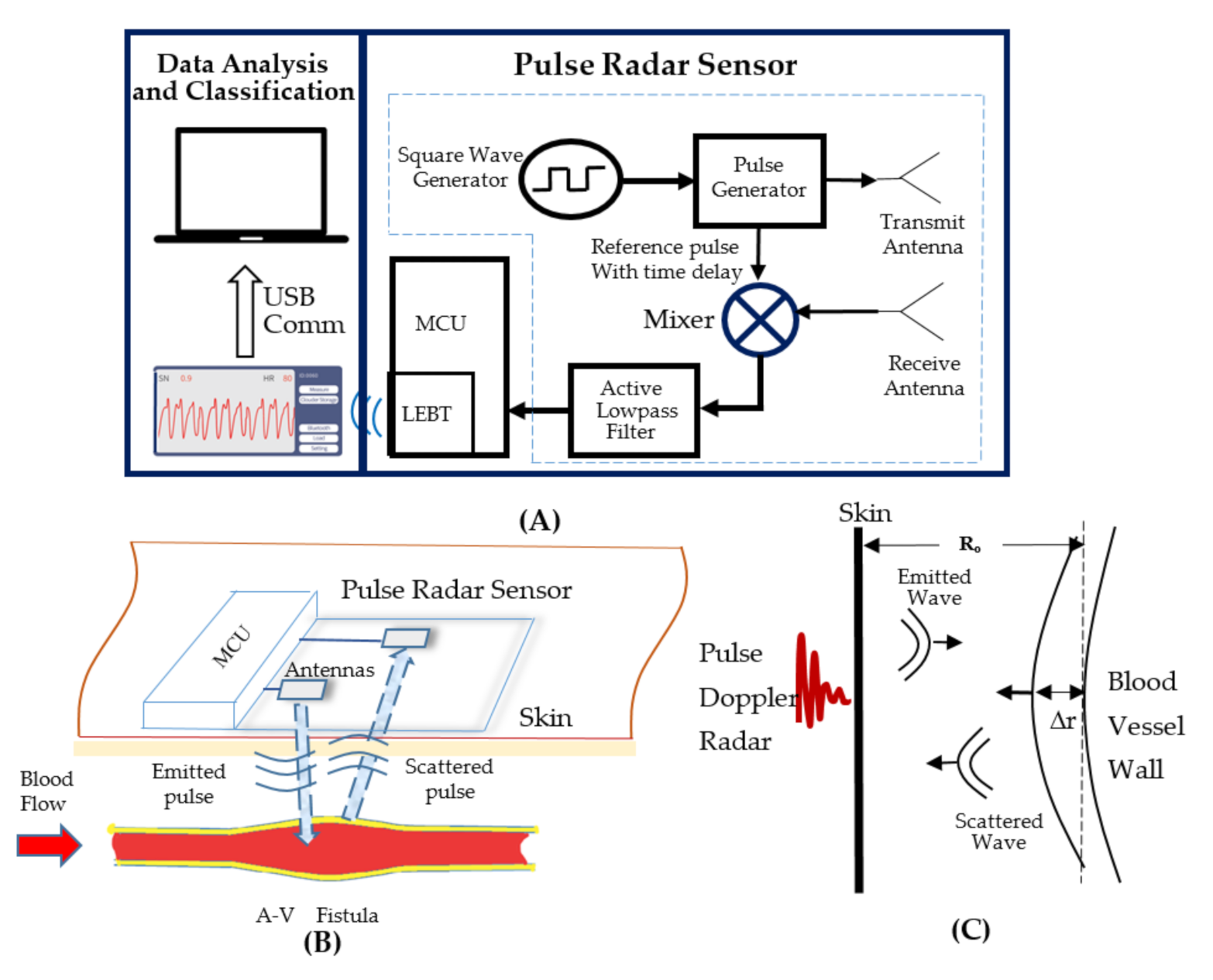
2.1. The Sensing Device and System
2.2. A Clinical Testing Protocol
2.3. Data Processing and SVM Classification
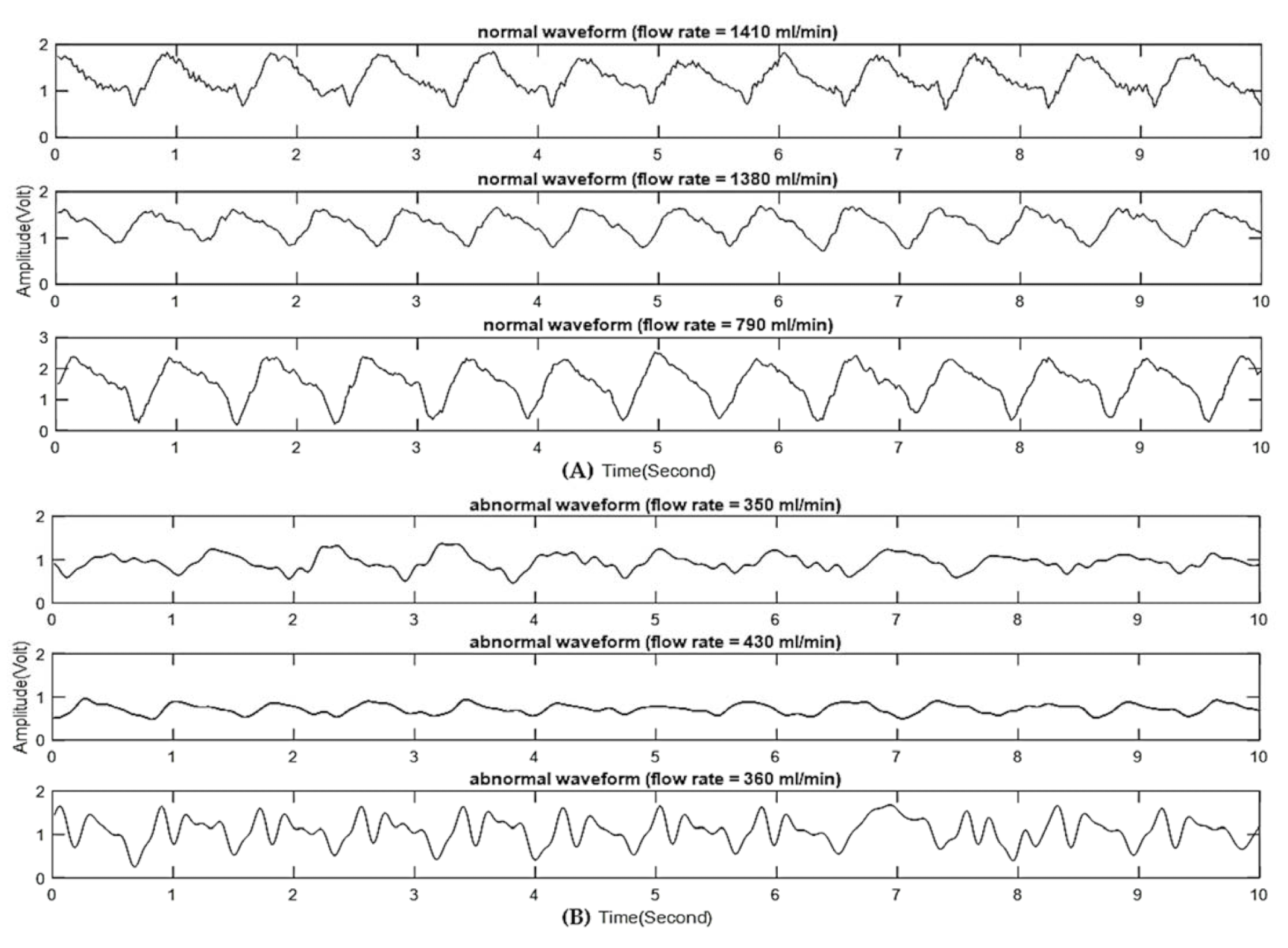
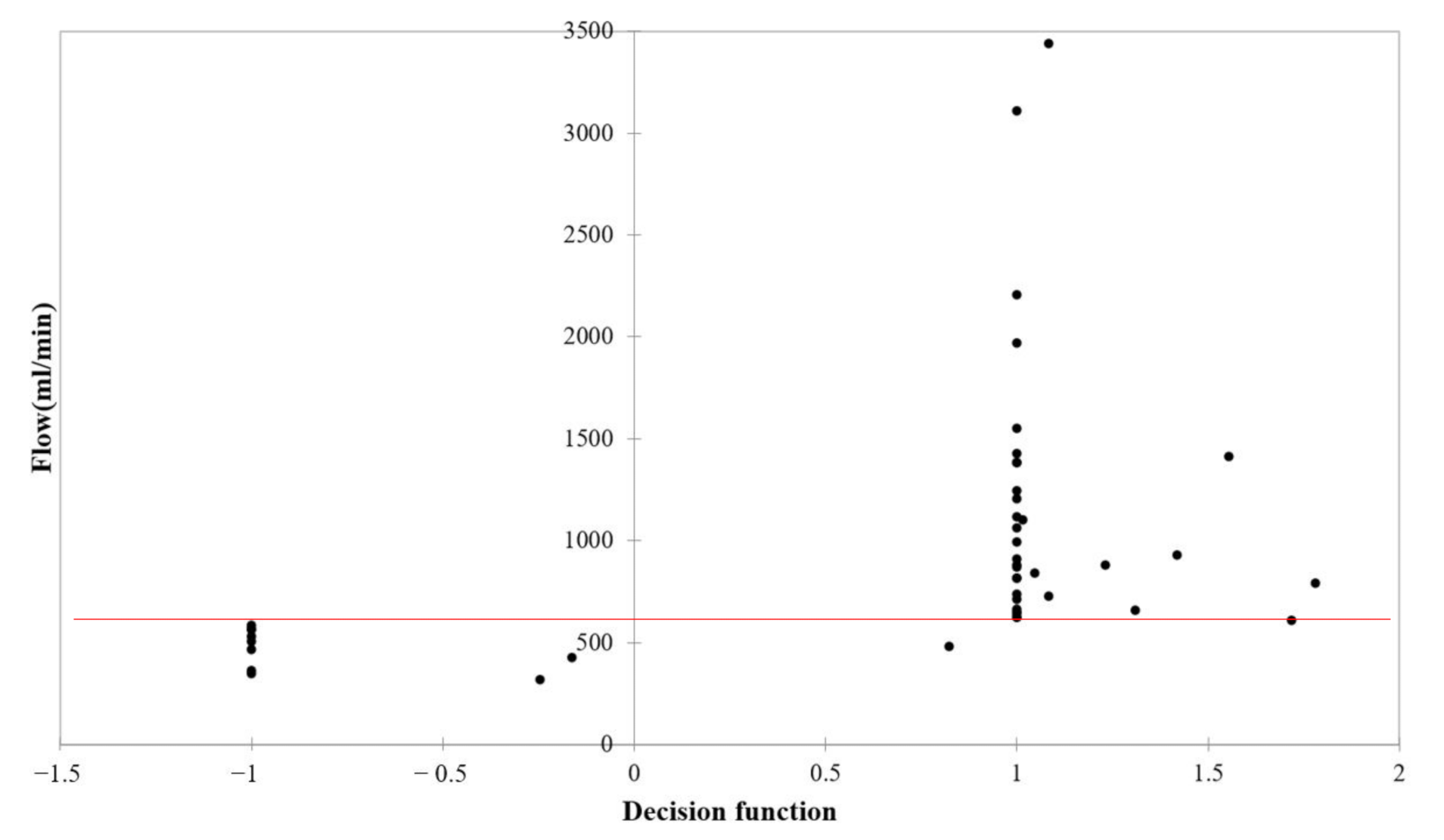
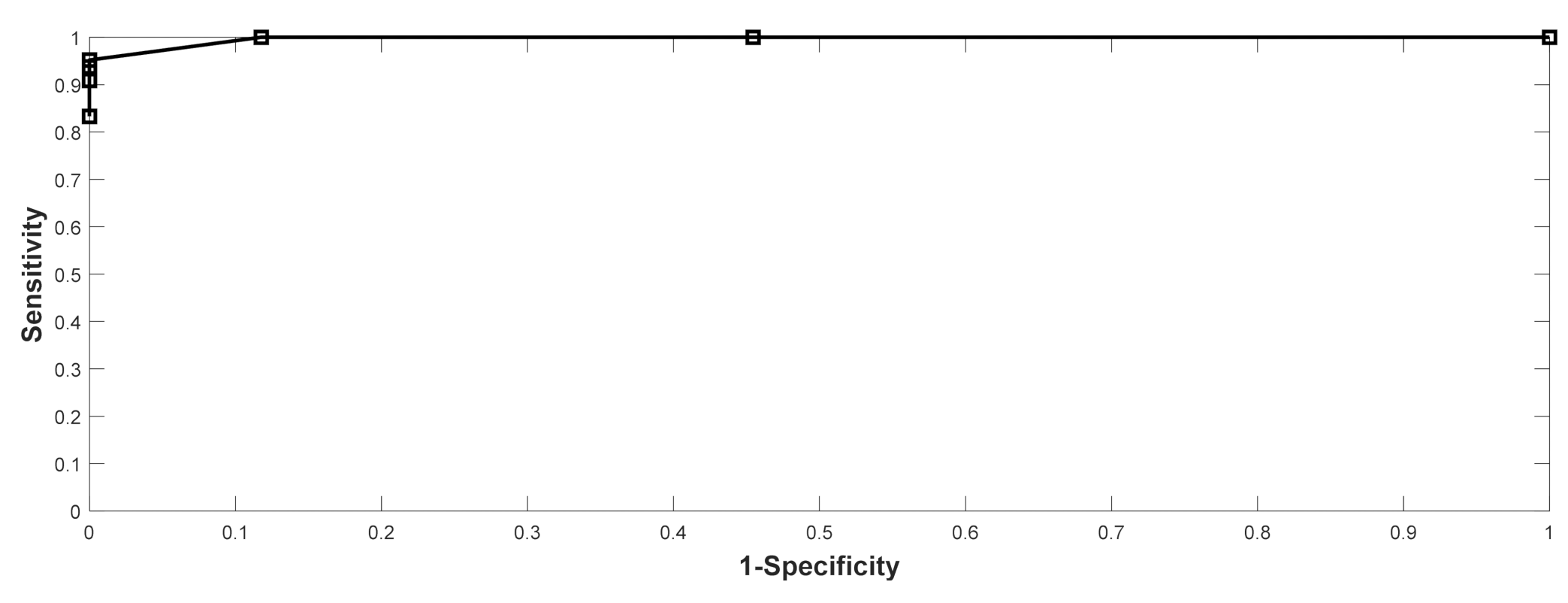
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
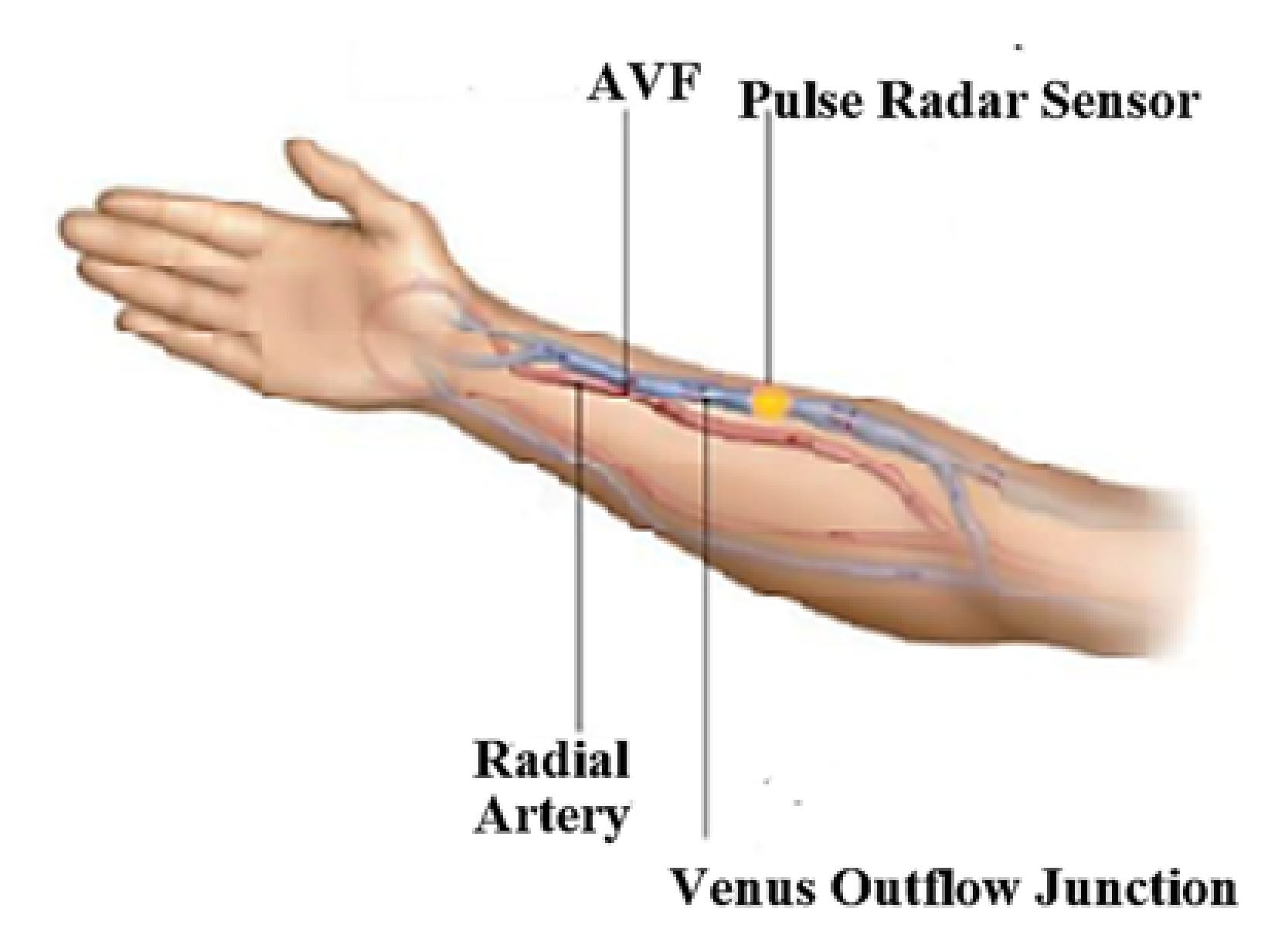
- Place the arm on the table top. Make sure that the side of the arm with AVF is in parallel with the table top and the weight of the arm should be fully supported by the table, as shown in Figure A1.
- Attach the pulse radar sensor to the skin using the soft cloth tape.
- Start the measurement while keeping the body still for 1 min.



References
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Vascular Access, update 2019. Am. J. Kidney Dis. 2019, 75 (Suppl. 2), 80–88. [Google Scholar]
- Salman, L.; Rizvi, A.; Contreras, G.; Manning, C.; Feustel, P.J.; Machado, I.; Briones, P.L.; Jamal, A.; Bateman, N.; Martinez, L.; et al. A Multicenter Randomized Clinical Trial of Hemodialysis Access Blood Flow Surveillance Compared to Standard of Care: The Hemodialysis Access Surveillance Evaluation (HASE) Study. Kidney Int. Rep. 2020, 5, 1937–1944. [Google Scholar] [CrossRef] [PubMed]
- Mccarley, P.; Wingard, R.L.; Shyr, Y.; Pettus, W.; Hakim, R.M.; Ikizler, T.A. Vascular access blood flow monitoring reduces access morbidity and costs. Kidney Int. 2001, 60, 1164–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, C.; Mitterbauer, C.; Boczula, M.; Maca, T.; Funovics, M.; Heinze, G.; Matthias, M.; Kovarik, J.; Oberbauer, R. Flow Monitoring: Performance Characteristics of Ultrasound Dilution Versus Color Doppler Ultrasound Compared with Fistulography. Am. J. Kidney Dis. 2003, 42, 539–545. [Google Scholar] [CrossRef]
- Tessitore, N.; Bedogna, V.; Gammaro, L.; Lipari, G.; Poli, A.; Baggio, E.; Firpo, M.; Morana, G.; Mansueto, G.; Maschio, G. Diagnostic Accuracy of Ultrasound Dilution Access Blood Flow Measurement in Detecting Stenosis and Predicting Thrombosis in Native Forearm Arteriovenous Fistulae for Hemodialysis. Am. J. Kidney Dis. 2003, 42, 331–341. [Google Scholar] [CrossRef]
- Du, Y.-C.; Stephanus, A. A Novel Classification Technique of Arteriovenous Fistula Stenosis Evaluation Using Bilateral PPG Analysis. Micromachines 2016, 7, 147. [Google Scholar] [CrossRef] [PubMed]
- Chiang, P.Y.; Chao, P.C.P.; Tarng, D.C.; Yang, C.Y. A Novel Wireless Photoplethysmography Blood-Flow Volume Sensor for Assessing Arteriovenous Fistula of Hemodialysis Patients. IEEE Trans. Ind. Electron. 2017, 64, 9626–9635. [Google Scholar] [CrossRef]
- Chiang, P.Y.; Chao, P.C.P.; Tu, T.Y.; Kao, Y.H.; Yang, C.Y.; Tarng, D.C.; Wey, C.L. Machine Learning Classification for Assessing the Degree of Stenosis and Blood Flow Volume at Arteriovenous Fistulas of Hemodialysis Patients Using a New Photoplethysmography Sensor Device. Sensors 2019, 19, 3422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.L.; Lin, C.H.; Chen, T.; Chen, P.J.; Kan, C.D. Stenosis Detection using Burg Method with Autoregressive Model for Hemodialysis Patients. J. Med. Biol. Eng. 2013, 33, 356–362. [Google Scholar] [CrossRef]
- Ota, K.; Nishiura, Y.; Ishihara, S.; Adachi, H.; Yamamoto, T.; Hamano, T. Evaluation of Hemodialysis Arteriovenous Bruit by Deep Learning. Sensors 2020, 20, 4852. [Google Scholar] [CrossRef] [PubMed]
- Ku, D.N. Blood Flow in Arteries. Annu. Rev. Fluid Mech. 1997, 29, 399–434. [Google Scholar] [CrossRef]
- Jahangiri, M.; Saghafia, M.; Sadeghi, M.R. Numerical Simulation of Hemodynamic Parameters of Turbulent and Pulsatile Blood Flow in Flexible Artery with Single and Double Stenoses. J. Mech. Sci. Technol. 2015, 29, 3549–3560. [Google Scholar] [CrossRef]
- Ramnarine, K.V.; Hartshorne, T.; Sensier, Y.; Naylor, M.; Walker, J.; Naylor, A.R.; Panerai, R.B.; Evans, D.H. Tissue Doppler imaging of carotid plaque wall motion: A pilot study. Cardiovasc. Ultrasound 2003, 1, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, T.H.; Hu, S.J.; Peng, J.H.; Kuo, S.C. An Ultrawideband Radar Based Pulse Sensor for Arterial Stiffness Measurement. In Proceedings of the 29th Annual International Conference of the IEEE EMBS 2007, Lyon, France, 22–26 August 2007; pp. 1679–1682. [Google Scholar]
- Hellbrück, H.; Ardelt, G.; Wegerich, P.; Gehring, H. Brachialis Pulse Wave Measurements with Ultra-Wide Band and Continuous Wave Radar, Photoplethysmography and Ultrasonic Doppler Sensors. Sensors 2021, 21, 165. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: Hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am. J. Kidney Dis. 2006, 48 (Suppl. 1), S1–S322. [Google Scholar]
- Giannattasio, C.; Vincenti, A.; Failla, M.; Capra, A.; Cirò, A.; Ceglia, S.D.; Gentile, G.; Brambilla, R.; Mancia, G. Effects of Heart Rate Changes on Arterial Distensibility in Humans. Hypertension 2003, 42, 253–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brovoll, S.; Aardal, Ø.; Paichard, Y.; Berger, T.; Lande, T.S.; Hamran, S.-E. Optimal frequency range for medical radar Measurements of human heartbeats using body-contact radar. In Proceedings of the 35th Annual International Conference of the IEEE EMBS 2013, Osaka, Japan, 3–7 July 2013; pp. 1752–1755. [Google Scholar]
- Merli, F.; Fuchs, B.; Mosig, J.R.; Skrivervik, A.K. The Effect of Insulating Layers on the Performance of Implanted Antennas. IEEE Trans. Antennas Propag. 2011, 59, 21–31. [Google Scholar]
- Pybus, D.A. Real-time, spectral analysis of the arterial pressure waveform using a wirelessly-connected, tablet computer: A pilot study. J. Clin. Monit. Comput. 2019, 33, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanber, B.; Hartshorne, T.C.; Horsfield, M.A.; Naylor, A.R.; Robinson, T.G. and Ramnarine, K.V. Wall Motion in the Stenotic Carotid Artery: Association with Greyscale Plaque Characteristics, the Degree of Stenosis and Cerebrovascular Symptoms. Cardiovasc. Ultrasound 2013, 11, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
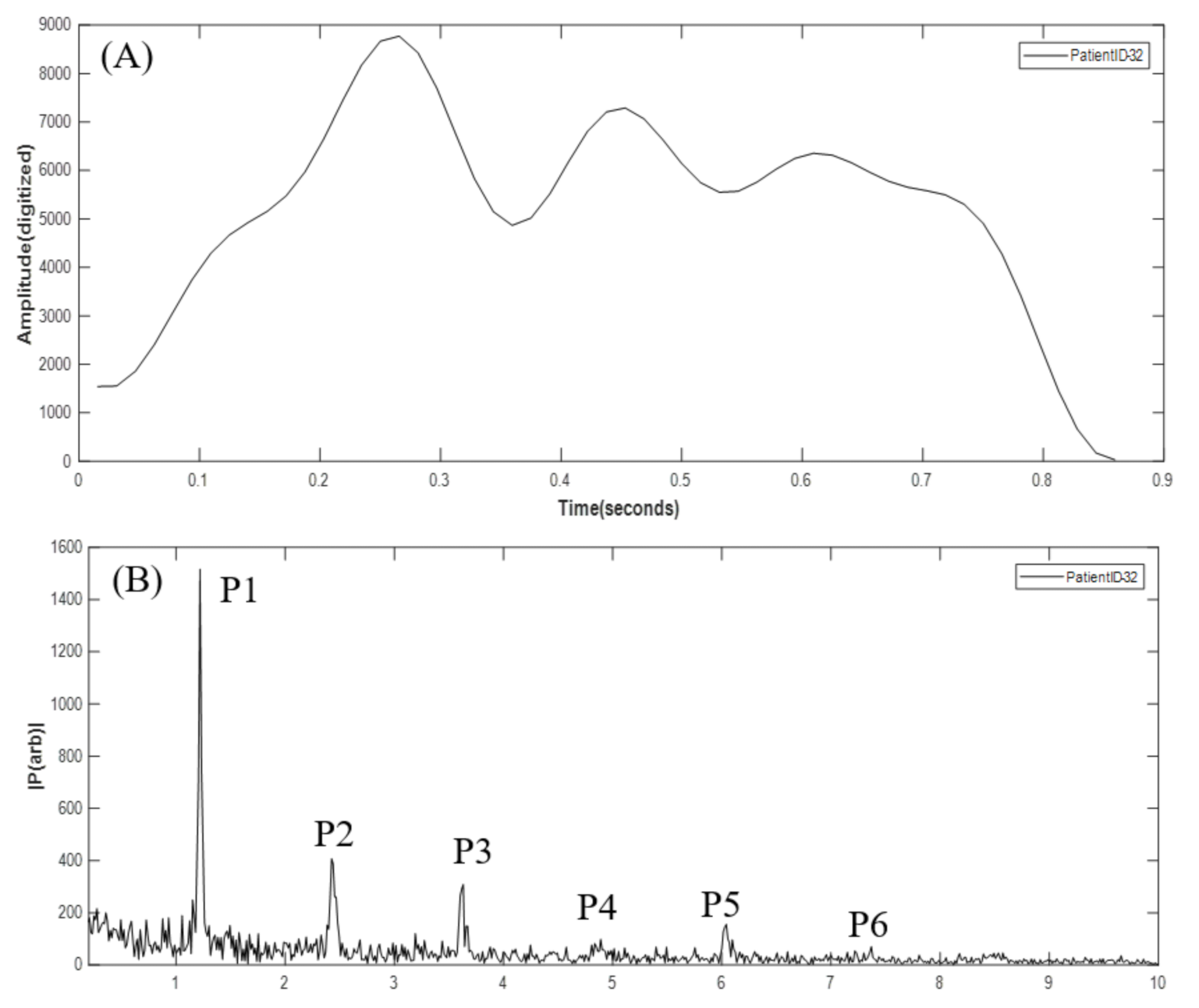
| Harmonic Ratio | ≤600 (n = 11) | >600 (n = 34) | Difference | p-Value | ≤750 (n = 21) | >750 (n = 24) | Difference | p-Value |
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||||
| P2/P1 | 0.357 (0.203) | 0.380 (0.178) | −0.023 | 0.722 | 0.347 (0.168) | 0.398 (0.195) | −0.051 | 0.356 |
| P3/P2 | 0.665 (0.313) | 0.491 (0.285) | 0.174 | 0.093 | 0.630 (0.277) | 0.449 (0.296) | 0.181 | 0.041 * |
| P4/P3 | 0.591 (0.289) | 0.785 (0.456) | −0.193 | 0.195 | 0.774 (0.475) | 0.705 (0.387) | 0.069 | 0.591 |
| P5/P4 | 1.075 (0.601) | 0.711 (0.273) | 0.365 | 0.008 * | 0.818 (0.510) | 0.784 (0.293) | 0.035 | 0.777 |
| P6/P5 | 0.659 (0.235) | 0.751 (0.347) | −0.092 | 0.417 | 0.696 (0.352) | 0.758 (0.300) | −0.062 | 0.529 |
| Ground Truth | ||||||
|---|---|---|---|---|---|---|
| Threshold | Prediction | Flow ≤ 600 | Flow > 600 | Total | %Correct | Index |
| 600 | Flow ≤ 600 | 10 | 0 | 10 | 90.9 | Sensitivity |
| Flow > 600 | 1 | 34 | 35 | 100.0 | Specificity | |
| Total | 11 | 34 | 45 | 97.8 | Accuracy | |
| Threshold | Prediction | Flow ≤ 750 | Flow > 750 | Total | %Correct | Index |
| 750 | Flow ≤ 750 | 20 | 1 | 21 | 95.2 | Sensitivity |
| Flow > 750 | 0 | 24 | 24 | 100.0 | Specificity | |
| Total | 20 | 25 | 45 | 97.8 | Accuracy | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Tao, T.-H.; Chou, Y.-H.; Chuang, Y.-W.; Chen, T.-B. Arteriovenous Fistula Flow Dysfunction Surveillance: Early Detection Using Pulse Radar Sensor and Machine Learning Classification. Biosensors 2021, 11, 297. https://doi.org/10.3390/bios11090297
Chen C-H, Tao T-H, Chou Y-H, Chuang Y-W, Chen T-B. Arteriovenous Fistula Flow Dysfunction Surveillance: Early Detection Using Pulse Radar Sensor and Machine Learning Classification. Biosensors. 2021; 11(9):297. https://doi.org/10.3390/bios11090297
Chicago/Turabian StyleChen, Cheng-Hsu, Teh-Ho Tao, Yi-Hua Chou, Ya-Wen Chuang, and Tai-Been Chen. 2021. "Arteriovenous Fistula Flow Dysfunction Surveillance: Early Detection Using Pulse Radar Sensor and Machine Learning Classification" Biosensors 11, no. 9: 297. https://doi.org/10.3390/bios11090297