
Impact of Plasma Xanthine Oxidoreductase Activity on the Mechanisms of Distal Symmetric Polyneuropathy Development in Patients with Type 2 Diabetes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Clinical Parameters and Procedures
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Enrolled Patients
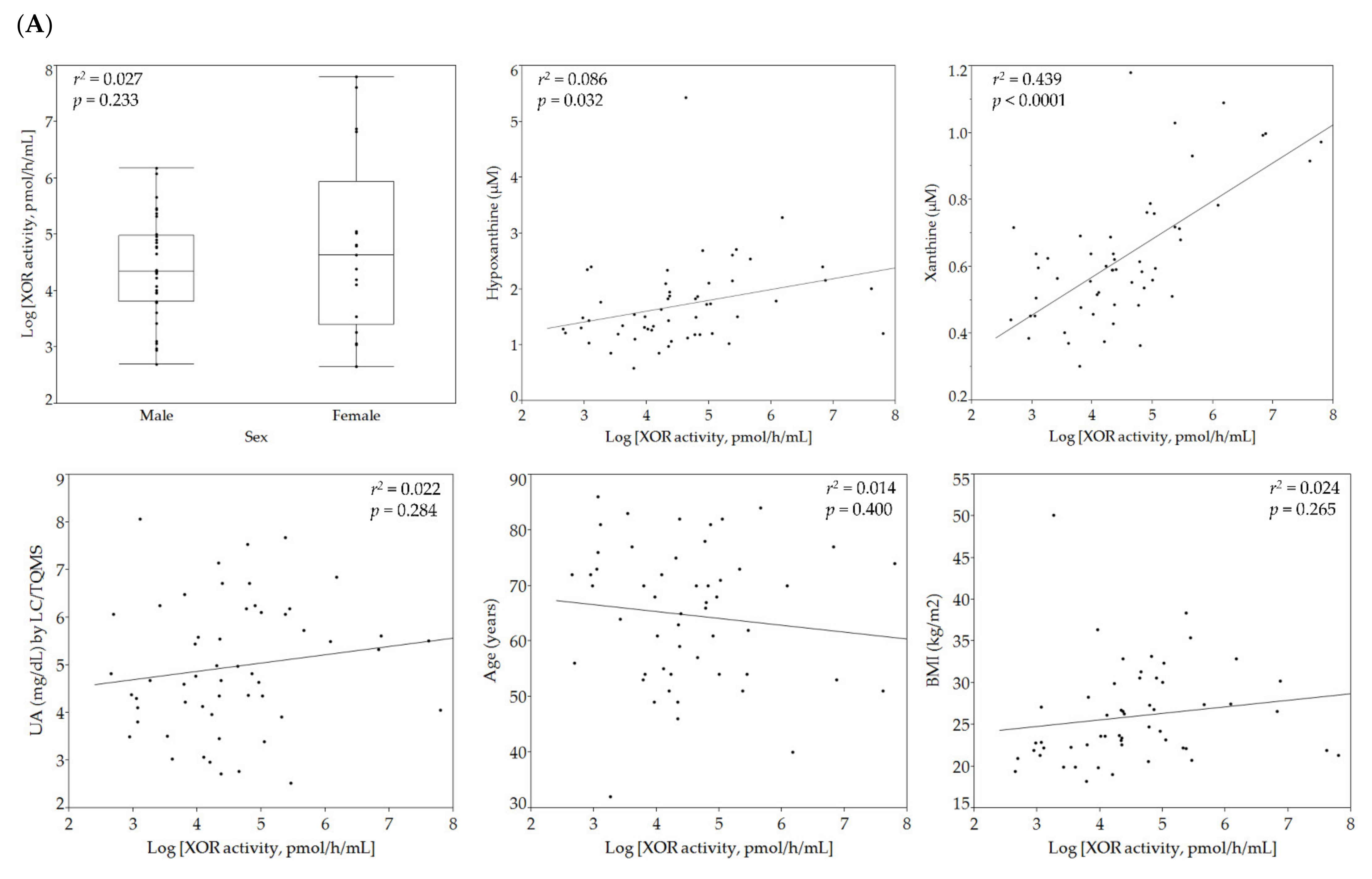
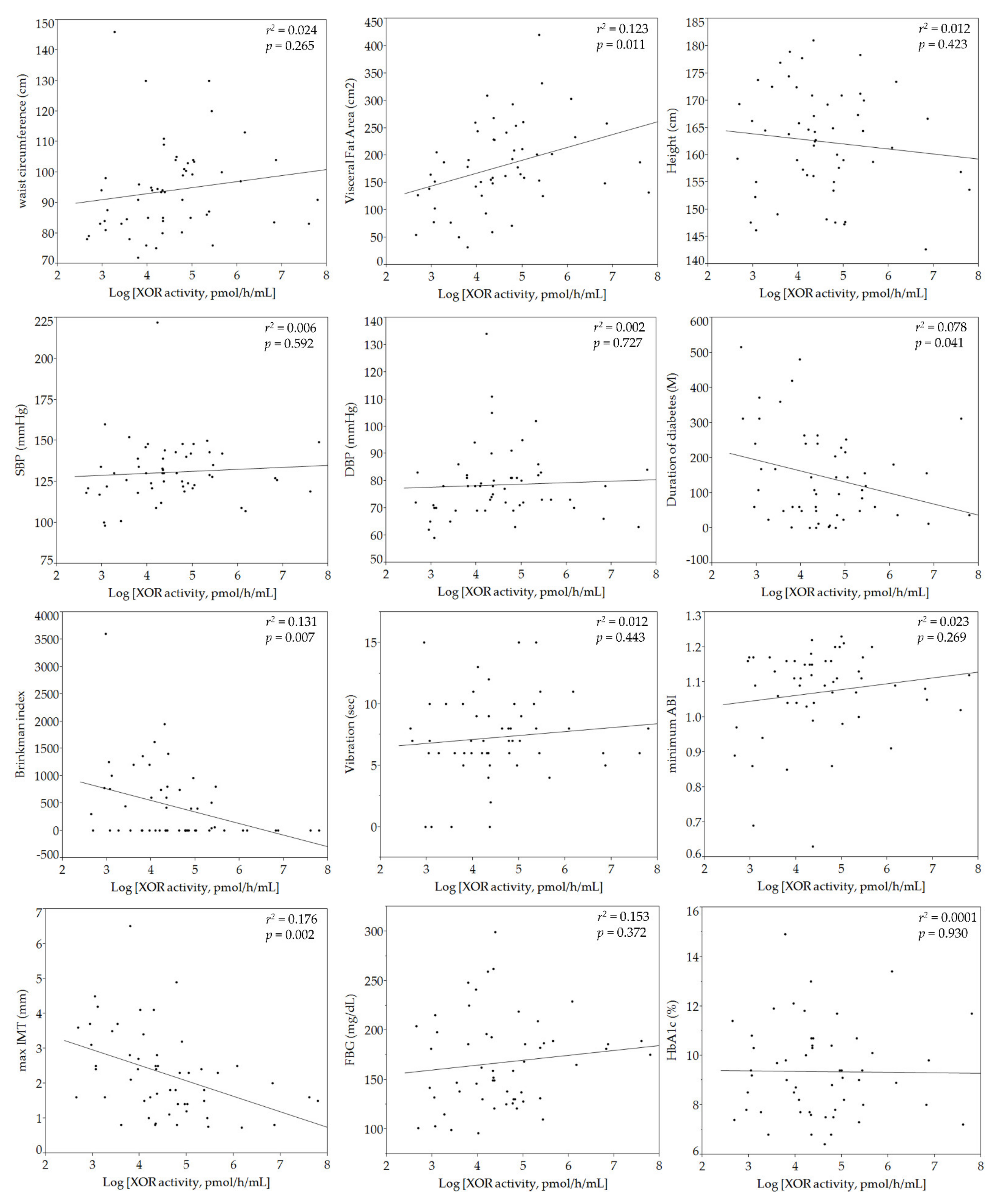
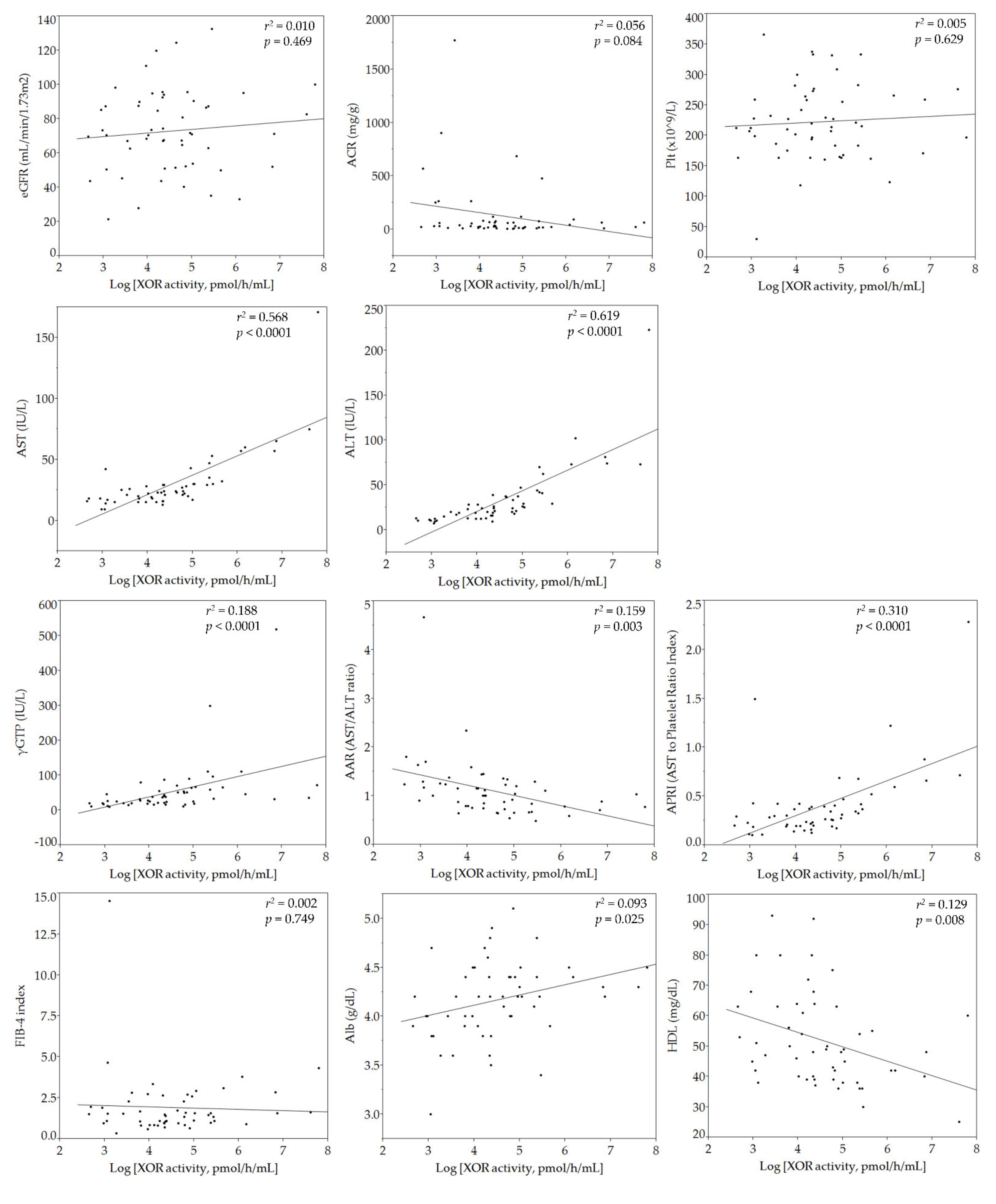
3.2. Relationships of Plasma XOR Activity with Individual Parameters
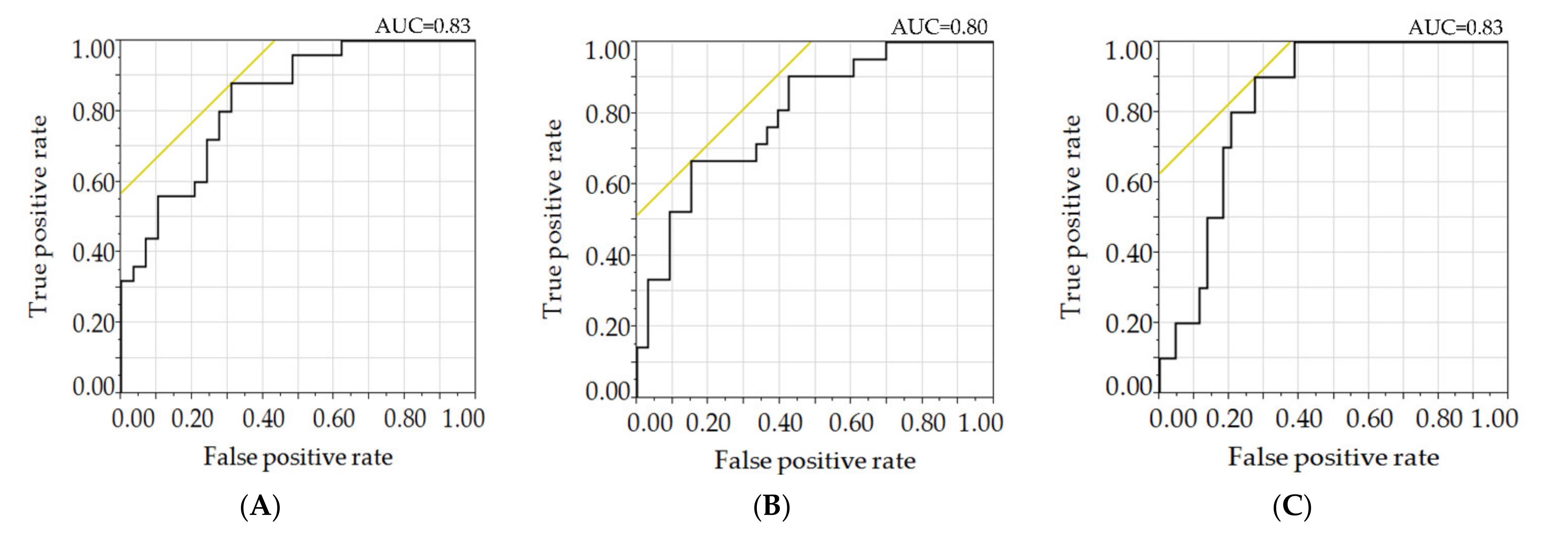
3.3. Relationships of Plasma XOR Activity with NCS Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABI | Ankle-Brachial Index |
| AST | Aspartate Aminotransferase |
| ALT | Alanine Aminotransferase |
| AAR | AST to ALT Ratio |
| APRI | AST to Platelet Ratio Index |
| BNP | B-Type Natriuretic Peptide |
| BMI | Body Mass Index |
| CRP | C-Reactive Protein |
| CVRR | Coefficient of Variation of RR Intervals |
| DR | Diabetic Retinopathy |
| DPN | Diabetic Polyneuropathy |
| DSP | Distal Symmetric Polyneuropathy |
| EPA/AA | Eicosapentaenoic Acid to Arachidonic Acid Ratio |
| eGFR | Estimated Glomerular Filtration Rate |
| FBG | Fasting Blood Glucose |
| γ-GTP | Gamma-Glutamyl Transferase |
| HDL-Cholesterol | High Density Lipoprotein-Cholesterol |
| IMT | Intima-Media Thickness |
| LC | Liquid Chromatography |
| ln-XOR | Logarithmically Transformed Plasma XOR Activity |
| LDL-Cholesterol | Low Density Lipoprotein-Cholesterol |
| NCS | Nerve Conduction Study |
| NDR | No Apparent Diabetic Retinopathy |
| PCA | Principal Component Analysis |
| PDR | Proliferative Diabetic Retinopathy |
| SDR | Simple Diabetic Retinopathy |
| TQMS | Triple Quadrupole Mass Spectrometry |
| T2DM | Type 2 Diabetes Mellitus |
| TG | Triglyceride |
| UA | Uric Acid |
| VFA | Visceral Fat Area |
| XOR | Xanthine Oxidoreductase |
References
- Rao Kondapally Seshasai, S.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [CrossRef] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Saeedi, P.; Salpea, P.; Karuranga, S.; Petersohn, I.; Malanda, B.; Gregg, E.W.; Unwin, N.; Wild, S.H.; Williams, R. Mortality attributable to diabetes in 20–79 years old adults, 2019 estimates: Results from the International Diabetes Federation Diabetes Atlas, 9th ed. Diabetes Res. Clin. Pract. 2020, 162, 108086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callaghan, B.C.; Cheng, H.T.; Stables, C.L.; Smith, A.L.; Feldman, E.L. Diabetic neuropathy: Clinical manifestations and current treatments. Lancet Neurol. 2012, 11, 521–534. [Google Scholar] [CrossRef] [Green Version]
- Tesfaye, S.; Boulton, A.J.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic neuropathies: Update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Chaturvedi, N.; Eaton, S.E.; Ward, J.D.; Manes, C.; Ionescu-Tirgoviste, C.; Witte, D.R.; Fuller, J.H. Vascular risk factors and diabetic neuropathy. N. Engl. J. Med. 2005, 352, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Y.; Scherer, P.E. Adipokines as novel biomarkers and regulators of the metabolic syndrome. Ann. NY Acad. Sci. 2010, 1212, E1–E19. [Google Scholar] [CrossRef] [PubMed]
- Facchini, F.; Chen, Y.D.; Hollenbeck, C.B.; Reaven, G.M. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA 1991, 266, 3008–3011. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.D.; Chiou, W.K.; Chang, H.Y.; Liu, F.H.; Weng, H.F. Serum uric acid and leptin levels in metabolic syndrome: A quandary over the role of uric acid. Metabolism 2007, 56, 751–756. [Google Scholar] [CrossRef]
- Bjornstad, P.; Laffel, L.; Lynch, J.; El Ghormli, L.; Weinstock, R.S.; Tollefsen, S.E.; Nadeau, K.J. Elevated Serum Uric Acid is Associated with Greater Risk for Hypertension and Diabetic Kidney Diseases in Obese Adolescents with Type 2 Diabetes: An Observational Analysis From the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) Study. Diabetes Care 2019, 42, 1120–1128. [Google Scholar] [CrossRef]
- Spatola, L.; Ferraro, P.M.; Gambaro, G.; Badalamenti, S.; Dauriz, M. Metabolic syndrome and uric acid nephrolithiasis: Insulin resistance in focus. Metabolism 2018, 83, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.D.; Wang, Y.Z.; Zou, C.; She, X.P.; Zheng, Z. The role of uric acid in the pathogenesis of diabetic retinopathy based on Notch pathway. Biochem. Biophys. Res. Commun. 2018, 503, 921–929. [Google Scholar] [CrossRef]
- Yu, S.; Chen, Y.; Hou, X.; Xu, D.; Che, K.; Li, C.; Yan, S.; Wang, Y.; Wang, B. Serum Uric Acid Levels and Diabetic Peripheral Neuropathy in Type 2 Diabetes: A Systematic Review and Meta-analysis. Mol. Neurobiol. 2016, 53, 1045–1051. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, C.; Zhao, Y.; Chen, Y. The significance of serum xanthine oxidoreductase in patients with nonalcoholic fatty liver disease. Clin. Lab. 2014, 60, 1301–1307. [Google Scholar] [CrossRef]
- Kuppusamy, U.R.; Indran, M.; Rokiah, P. Glycaemic control in relation to xanthine oxidase and antioxidant indices in Malaysian Type 2 diabetes patients. Diabet Med. 2005, 22, 1343–1346. [Google Scholar] [CrossRef] [PubMed]
- Parks, D.A.; Granger, D.N. Xanthine oxidase: Biochemistry, distribution and physiology. Acta Physiol Scand. Suppl. 1986, 548, 87–99. [Google Scholar] [PubMed]
- Nishino, T.; Okamoto, K.; Eger, B.T.; Pai, E.F.; Nishino, T. Mammalian xanthine oxidoreductase—Mechanism of transition from xanthine dehydrogenase to xanthine oxidase. FEBS J. 2008, 275, 3278–3289. [Google Scholar] [CrossRef] [PubMed]
- Nishino, T.; Okamoto, K.; Kawaguchi, Y.; Hori, H.; Matsumura, T.; Eger, B.T.; Pai, E.F.; Nishino, T. Mechanism of the conversion of xanthine dehydrogenase to xanthine oxidase: Identification of the two cysteine disulfide bonds and crystal structure of a non-convertible rat liver xanthine dehydrogenase mutant. J. Biol. Chem. 2005, 280, 24888–24894. [Google Scholar] [CrossRef] [Green Version]
- Gibbings, S.; Elkins, N.D.; Fitzgerald, H.; Tiao, J.; Weyman, M.E.; Shibao, G.; Fini, M.A.; Wright, R.M. Xanthine oxidoreductase promotes the inflammatory state of mononuclear phagocytes through effects on chemokine expression, peroxisome proliferator-activated receptor-{gamma} sumoylation, and HIF-1{alpha}. J. Biol. Chem. 2011, 286, 961–975. [Google Scholar] [CrossRef] [Green Version]
- Kushiyama, A.; Nakatsu, Y.; Matsunaga, Y.; Yamamotoya, T.; Mori, K.; Ueda, K.; Inoue, Y.; Sakoda, H.; Fujishiro, M.; Ono, H.; et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediat. Inflamm. 2016, 2016, 8603164. [Google Scholar] [CrossRef] [PubMed]
- Murase, T.; Nampei, M.; Oka, M.; Miyachi, A.; Nakamura, T. A highly sensitive assay of human plasma xanthine oxidoreductase activity using stable isotope-labeled xanthine and LC/TQMS. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2016, 1039, 51–58. [Google Scholar] [CrossRef]
- Yoshizumi, T.; Nakamura, T.; Yamane, M.; Islam, A.H.; Menju, M.; Yamasaki, K.; Arai, T.; Kotani, K.; Funahashi, T.; Yamashita, S.; et al. Abdominal fat: Standardized technique for measurement at CT. Radiology 1999, 211, 283–286. [Google Scholar] [CrossRef]
- Tanaka, K.; Hara, S.; Hattori, M.; Sakai, K.; Onishi, Y.; Yoshida, Y.; Kawazu, S.; Kushiyama, A. Role of elevated serum uric acid levels at the onset of overt nephropathy in the risk for renal function decline in patients with type 2 diabetes. J. Diabetes Investig. 2015, 6, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Haneda, M.; Utsunomiya, K.; Koya, D.; Babazono, T.; Moriya, T.; Makino, H.; Kimura, K.; Suzuki, Y.; Wada, T.; Ogawa, S.; et al. A new classification of Diabetic Nephropathy 2014: A report from Joint Committee on Diabetic Nephropathy. Clin. Exp. Nephrol. 2015, 19, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, Q.; Gillies, M.C.; Wong, T.Y. Management of diabetic retinopathy: A systematic review. JAMA 2007, 298, 902–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, A.; Miyamoto, M.; Kotani, K.; Okada, K.; Nagasaka, S.; Ishibashi, S. Cardio-Ankle Vascular Index and Indices of Diabetic Polyneuropathy in Patients with Type 2 Diabetes. J. Diabetes Res. 2017, 2017, 2810914. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, D.H.; Polak, J.F.; Wolfson, S.K., Jr.; Bond, M.G.; Bommer, W.; Sheth, S.; Psaty, B.M.; Sharrett, A.R.; Manolio, T.A. Use of sonography to evaluate carotid atherosclerosis in the elderly. The Cardiovascular Health Study. CHS Collaborative Research Group. Stroke 1991, 22, 1155–1163. [Google Scholar] [CrossRef] [Green Version]
- Washio, K.W.; Kusunoki, Y.; Murase, T.; Nakamura, T.; Osugi, K.; Ohigashi, M.; Sukenaga, T.; Ochi, F.; Matsuo, T.; Katsuno, T.; et al. Xanthine oxidoreductase activity is correlated with insulin resistance and subclinical inflammation in young humans. Metabolism 2017, 70, 51–56. [Google Scholar] [CrossRef]
- Yanagida, H.A.A.; Kenta, O.; Nagasaka, S.; Ishibashi, S.; Kotani, K.; Hasegawa, O.; Taniguchi, N. Determination of reference ranges for nerve conduction studies: Influence of age, height and gender. Jichi Med. Univ. J. 2015, 38, 27–39. [Google Scholar]
- Weisman, A.; Bril, V.; Ngo, M.; Lovblom, L.E.; Halpern, E.M.; Orszag, A.; Perkins, B.A. Identification and prediction of diabetic sensorimotor polyneuropathy using individual and simple combinations of nerve conduction study parameters. PLoS ONE 2013, 8, e58783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, T.N.; Dale, A.M.; Al-Lozi, M.T.; Franzblau, A.; Evanoff, B.A. Median and ulnar nerve conduction studies at the wrist: Criterion validity of the NC-stat automated device. J. Occup. Environ. Med. 2008, 50, 758–764. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Kwon, H.K.; Kim, D.H.; Pyun, S.B. Nerve conduction studies of median motor nerve and median sensory branches according to the severity of carpal tunnel syndrome. Ann. Rehabil. Med. 2013, 37, 254–262. [Google Scholar] [CrossRef] [Green Version]
- Andersen, H.; Stålberg, E.; Falck, B. F-wave latency, the most sensitive nerve conduction parameter in patients with diabetes mellitus. Muscle Nerve 1997, 20, 1296–1302. [Google Scholar] [CrossRef]
- Furuhashi, M.; Koyama, M.; Higashiura, Y.; Murase, T.; Nakamura, T.; Matsumoto, M.; Sakai, A.; Ohnishi, H.; Tanaka, M.; Saitoh, S.; et al. Differential regulation of hypoxanthine and xanthine by obesity in a general population. J. Diabetes Investig. 2020, 11, 878–887. [Google Scholar] [CrossRef] [Green Version]
- Washio, K.; Kusunoki, Y.; Tsunoda, T.; Osugi, K.; Ohigashi, M.; Murase, T.; Nakamura, T.; Matsuo, T.; Konishi, K.; Katsuno, T.; et al. Xanthine oxidoreductase activity correlates with vascular endothelial dysfunction in patients with type 1 diabetes. Acta Diabetol. 2020, 57, 31–39. [Google Scholar] [CrossRef]
- Kawachi, Y.; Fujishima, Y.; Nishizawa, H.; Nagao, H.; Nakamura, T.; Akari, S.; Murase, T.; Taya, N.; Omori, K.; Miyake, A.; et al. Plasma xanthine oxidoreductase activity in Japanese patients with type 2 diabetes across hospitalized treatment. J. Diabetes Investig. 2020, 12, 1512–1520. [Google Scholar] [CrossRef]
- Watanabe, K.; Shishido, T.; Otaki, Y.; Watanabe, T.; Sugai, T.; Toshima, T.; Takahashi, T.; Yokoyama, M.; Kinoshita, D.; Murase, T.; et al. Increased plasma xanthine oxidoreductase activity deteriorates coronary artery spasm. Heart Vessels 2019, 34, 1–8. [Google Scholar] [CrossRef]
- Watanabe, K.; Watanabe, T.; Otaki, Y.; Shishido, T.; Murase, T.; Nakamura, T.; Kato, S.; Tamura, H.; Nishiyama, S.; Takahashi, H.; et al. Impact of plasma xanthine oxidoreductase activity in patients with heart failure with preserved ejection fraction. ESC Heart Fail. 2020, 7, 1735–1743. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Shirakabe, A.; Okazaki, H.; Matsushita, M.; Goda, H.; Shigihara, S.; Asano, K.; Kiuchi, K.; Tani, K.; Murase, T.; et al. Plasma xanthine oxidoreductase (XOR) activity in patients who require cardiovascular intensive care. Heart Vessels 2020, 35, 1390–1400. [Google Scholar] [CrossRef] [PubMed]
- Miric, D.J.; Kisic, B.M.; Filipovic-Danic, S.; Grbic, R.; Dragojevic, I.; Miric, M.B.; Puhalo-Sladoje, D. Xanthine Oxidase Activity in Type 2 Diabetes Mellitus Patients with and without Diabetic Peripheral Neuropathy. J. Diabetes Res. 2016, 2016, 4370490. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Wang, C.; Liu, F.; Lu, Y.; Cheng, J. Metabonomics revealed xanthine oxidase-induced oxidative stress and inflammation in the pathogenesis of diabetic nephropathy. Anal. Bioanal. Chem. 2015, 407, 2569–2579. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Wang, Z.; Zhang, F. Association between Related Purine Metabolites and Diabetic Retinopathy in Type 2 Diabetic Patients. Int. J. Endocrinol. 2014, 2014, 651050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feoli, A.M.; Macagnan, F.E.; Piovesan, C.H.; Bodanese, L.C.; Siqueira, I.R. Xanthine oxidase activity is associated with risk factors for cardiovascular disease and inflammatory and oxidative status markers in metabolic syndrome: Effects of a single exercise session. Oxid. Med. Cell Longev. 2014, 2014, 587083. [Google Scholar] [CrossRef] [PubMed]
- Honorat, J.A.; Kinoshita, M.; Okuno, T.; Takata, K.; Koda, T.; Tada, S.; Shirakura, T.; Fujimura, H.; Mochizuki, H.; Sakoda, S.; et al. Xanthine oxidase mediates axonal and myelin loss in a murine model of multiple sclerosis. PLoS ONE 2013, 8, e71329. [Google Scholar] [CrossRef] [Green Version]
- Battelli, M.G.; Bolognesi, A.; Polito, L. Pathophysiology of circulating xanthine oxidoreductase: New emerging roles for a multi-tasking enzyme. Biochim. Biophys. Acta 2014, 1842, 1502–1517. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, T.; Shirakawa, J.; Nakamura, T.; Murase, T.; Miyashita, D.; Inoue, R.; Kyohara, M.; Togashi, Y.; Terauchi, Y. Association of the plasma xanthine oxidoreductase activity with the metabolic parameters and vascular complications in patients with type 2 diabetes. Sci. Rep. 2021, 11, 3768. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Luo, P.; Wang, Y.; Li, W.; Wang, C.; Sun, D.; Zhang, R.; Su, T.; Ma, X.; Zeng, C.; et al. Glucagon-like peptide-1 protects against cardiac microvascular injury in diabetes via a cAMP/PKA/Rho-dependent mechanism. Diabetes 2013, 62, 1697–1708. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Park, M.S.; Choung, J.S.; Kim, S.S.; Oh, H.H.; Choi, C.S.; Ha, S.Y.; Kang, Y.; Kim, Y.; Jun, H.S. Glucagon-like peptide-1 inhibits adipose tissue macrophage infiltration and inflammation in an obese mouse model of diabetes. Diabetologia 2012, 55, 2456–2468. [Google Scholar] [CrossRef] [Green Version]
- Pop-Busui, R.; Boulton, A.J.; Feldman, E.L.; Bril, V.; Freeman, R.; Malik, R.A.; Sosenko, J.M.; Ziegler, D. Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 2017, 40, 136–154. [Google Scholar] [CrossRef] [Green Version]
- Binns-Hall, O.; Selvarajah, D.; Sanger, D.; Walker, J.; Scott, A.; Tesfaye, S. One-stop microvascular screening service: An effective model for the early detection of diabetic peripheral neuropathy and the high-risk foot. Diabet. Med. 2018, 35, 887–894. [Google Scholar] [CrossRef]
- Alam, U.; Jeziorska, M.; Petropoulos, I.N.; Asghar, O.; Fadavi, H.; Ponirakis, G.; Marshall, A.; Tavakoli, M.; Boulton, A.J.M.; Efron, N.; et al. Diagnostic utility of corneal confocal microscopy and intra-epidermal nerve fibre density in diabetic neuropathy. PLoS ONE 2017, 12, e0180175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvarajah, D.; Cash, T.; Davies, J.; Sankar, A.; Rao, G.; Grieg, M.; Pallai, S.; Gandhi, R.; Wilkinson, I.D.; Tesfaye, S. SUDOSCAN: A Simple, Rapid, and Objective Method with Potential for Screening for Diabetic Peripheral Neuropathy. PLoS ONE 2015, 10, e0138224. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (n = 54) * | n or Mean ± SD | (Median) |
| Sex (male/female) | 37/17 | |
| Age (years) | 64.7 ± 12.2 | (66.5) |
| Height (cm) | 162.5 ± 9.6 | (163.3) |
| BMI (kg/m2) | 26.0 ± 5.9 | (24.0) |
| Waist circumference (cm) | 94.1 ± 14.8 | (93.5) |
| VFA (cm2) | 180.8 ± 78.3 | (171.4) |
| SBP (mmHg) | 131 ± 19 | (130) |
| DBP (mmHg) | 79 ± 13 | (78) |
| Pulse Rate (bpm) | 76 ± 12 | (77) |
| Duration of diabetes (M) | 146 ± 130 | (108) |
| Brinkman index | 443 ± 677 | (0) |
| Vibration (sec) | 7.3 ± 3.5 | (7.0) |
| CVRR (%) | 148 ± 130 | (106) |
| Minimum ABI | 1.07 ± 0.13 | (1.11) |
| Maximum IMT (mm) | 2.3 ± 1.2 | (2.2) |
| Laboratory measurements | ||
| XOR activity (pmol/h/mL) | 216 ± 441 | (78.3) |
| Hypoxanthine (μM) | 1.7 ± 0.8 | (1.5) |
| Xanthine (μM) | 0.63 ± 0.30 | (0.49) |
| UA by LC/TQMS (mg/dL) | 5.0 ± 1.4 | (4.8) |
| FBG (mg/dL) | 168 ± 46 | (161) |
| HbA1c (%) | 9.4 ± 1.9 | (9.2) |
| Cre (mg/dL) | 0.9 ± 0.4 | (0.8) |
| eGFR (mL/min/1.73 m2) | 72.9 ± 24.1 | (71.1) |
| ACR (mg/g) | 127 ± 288 | (30.3) |
| Plt (×109/L) | 223 ± 63 | (215) |
| AST (IU/L) | 30 ± 24 | (23) |
| ALT (IU/L) | 33 ± 34 | (24) |
| γGTP (IU/L) | 54 ± 78 | (34) |
| AAR | 1.11 ± 0.61 | (1.00) |
| APRI | 0.40 ± 0.37 | (0.29) |
| FIB-4 index | 1.92 ± 1.99 | (1.50) |
| Albumin (g/dL) | 4.2 ± 0.4 | (4.2) |
| HDL-Chol (mg/dL) | 52 ± 15 | (49) |
| LDL-Chol (mg/dL) | 122 ± 40 | (120) |
| TG (mg/dL) | 136 ± 51 | (133) |
| EPA/AA | 0.34 ± 0.31 | (0.21) |
| CRP (mg/dL) | 0.3 ± 0.9 | (0.1) |
| BNP (pg/mL) | 48.5 ± 28.3 | (14.3) |
| NCS Parameters | □ | Median (Q1, Q3) |
| Sural Amp (μV) | ND (ND, 3.3) | |
| Sural CV (m/s) | ND (ND, 43.3) | |
| Peroneal Amp (mV) | 4.6 (1.4, 6.7) | |
| Peroneal CV (m/s) | 43.8 (37.7, 47.0) | |
| Peroneal F-wave (ms) | 49.2 (45.8, 52.6) | |
| Tibial Amp (mV) | 10.6 (6.4, 17.1) | |
| Tibial CV (m/s) | 41.4 (37.7, 45.0) | |
| Tibial F-wave (ms) | 51.6 (47.3, 55.4) | |
| Incidence of Diabetic Microangiopathy | n | |
| Nephropathy Stage 1 Stage 2 Stage 3 Stage 4 | 27 21 4 2 | |
| Retinopathy NDR SDR PDR | 32 8 14 | |
| Use of Antidiabetic Drugs or Other Medications | n (%) | |
| Insulins | 13 (24) | |
| SU/Glinides | 9 (17) | |
| GLP1RAs/DPP4is | 27 (50) | |
| SGLT2is | 12 (22) | |
| Biguanides | 15 (28) | |
| TZDs | 2 (4) | |
| αGIs | 5 (9) | |
| Epalrestat | 1 (2) | |
| Statins | 22 (41) | |
| EPAs | 6 (11) | |
| ACEI/ARBs | 17 (31) | |
| CCBs | 15 (28) | |
| Diuretics | 3 (6) | |
| β-blockers | 6 (11) | |
| Univariate Analysis | ||||
| Objective Variable | Explanatory Variable | OR | <95% CI> | p-value |
| Peroneal Amp (<6.2 mV) | Ln-XOR | 0.78 | <0.46–1.31> | 0.349 |
| Peroneal CV (<42.4 m/s) | 0.48 | <0.24–0.83> | 0.007 | |
| Peroneal F-wave (>51.8 ms) | 0.39 | <0.18–0.73> | 0.002 | |
| Tibial Amp (<8.4 mV) | 0.63 | <0.34–1.07> | 0.087 | |
| Tibial CV (<41.4 m/s) | 0.84 | <0.51–1.34> | 0.454 | |
| Tibial F-wave (>57.6 ms) | 0.23 | <0.07–0.58> | 0.001 | |
| Multivariate Analysis | ||||
| Objective Variable | Explanatory Variable | OR | <95% CI> | p-value |
| Peroneal CV (<42.4 m/s) | Ln-XOR | 0.47 | <0.22–0.86> | 0.013 |
| Age | 0.93 | <0.87–0.99> | 0.027 | |
| Waist circumference | 0.92 | <0.86–0.96> | 0.0004 | |
| Peroneal F-wave (>51.8 ms) | Ln-XOR | 0.48 | <0.21–0.89> | 0.017 |
| BMI | 0.83 | <0.69–0.96> | 0.007 | |
| Tibial F-wave (>57.6 ms) | Ln-XOR | 0.23 | <0.07–0.58> | 0.001 |
| Factor Loadings for PC1 to PC11 | |||||||||||
| Variables | PC1 | PC2 | PC3 | PC4 | PC5 | PC6 | PC7 | PC8 | PC9 | PC10 | PC11 |
| Log [XOR activity, pmol/h/mL] | 0.75 | 0.49 | |||||||||
| Peroneal F-wave (ms) | −0.69 | −0.34 | |||||||||
| Peroneal CV (m/s) | 0.65 | −0.3 | |||||||||
| Xanthine (μM) | 0.63 | 0.51 | |||||||||
| BMI (kg/m2) | 0.62 | −0.35 | 0.48 | ||||||||
| Hepatic steatosis (Without0/Wth1) | 0.61 | 0.35 | |||||||||
| ALT (IU/L) | 0.6 | 0.64 | |||||||||
| Tibial F-wave (ms) | −0.6 | −0.51 | |||||||||
| Visceral Fat Area (cm2) | 0.6 | 0.52 | |||||||||
| max IMT (mm) | −0.6 | 0.32 | |||||||||
| Waist circumference (cm) | 0.58 | 0.52 | |||||||||
| γGTP (IU/L) | 0.51 | ||||||||||
| AST (IU/L) | 0.49 | 0.72 | |||||||||
| Tibial Amp (mV) | 0.49 | −0.34 | 0.38 | −0.43 | |||||||
| Peroneal Amp (mV) | 0.48 | −0.38 | 0.46 | ||||||||
| Duration of diabetes (M) | −0.48 | −0.48 | 0.35 | ||||||||
| Hypoxanthine (μM) | 0.46 | 0.31 | −0.36 | −0.35 | |||||||
| AAR (AST/ALT ratio) | −0.43 | 0.42 | −0.39 | ||||||||
| HDL-Chol (mg/dL) | −0.43 | 0.44 | |||||||||
| GLP1RAs/DPP4is (Without0/Wth1) | −0.41 | 0.51 | −0.34 | ||||||||
| TG (mg/dL) | 0.41 | 0.56 | |||||||||
| Age (years) | −0.38 | 0.36 | 0.5 | 0.36 | |||||||
| ACR (mg/g) | −0.37 | 0.37 | −0.41 | ||||||||
| Retinopathy (Without0/Wth1) | −0.35 | 0.46 | −0.33 | −0.32 | |||||||
| Brinkman index | −0.34 | 0.43 | 0.37 | ||||||||
| APRI (AST to Platelet Ratio Index) | 0.82 | ||||||||||
| Nephropathy (Without0/Wth1) | 0.44 | 0.32 | |||||||||
| eGFR (mL/min/1.73 m2) | −0.43 | −0.35 | −0.38 | −0.34 | 0.34 | ||||||
| UA (mg/dL) by LC/TQMS | 0.36 | 0.67 | −0.32 | ||||||||
| Alb (g/dL) | 0.3 | 0.52 | 0.35 | ||||||||
| BNP (pg/mL) | 0.58 | 0.58 | |||||||||
| Height (cm) | −0.58 | −0.31 | |||||||||
| CRP (mg/dL) | 0.52 | −0.34 | 0.64 | ||||||||
| Sex (Male0/Female1) | 0.45 | −0.48 | −0.32 | ||||||||
| FBG (mg/dL) | −0.45 | 0.65 | |||||||||
| min ABI | −0.37 | −0.45 | 0.49 | ||||||||
| Tibial CV (m/s) | 0.36 | −0.42 | |||||||||
| EPA/AA | 0.51 | 0.41 | 0.41 | ||||||||
| HbA1c (%) | −0.51 | 0.39 | 0.36 | ||||||||
| Vibration (sec) | −0.33 | 0.5 | 0.31 | ||||||||
| Eigenvalues of PCs | |||||||||||
| Eigenvalues | Proportion of Variance | Cumulative Proportion | |||||||||
| PC1 | 7.63 | 0.191 | 0.191 | ||||||||
| PC2 | 3.69 | 0.092 | 0.283 | ||||||||
| PC3 | 3.61 | 0.09 | 0.373 | ||||||||
| PC4 | 3.22 | 0.081 | 0.454 | ||||||||
| PC5 | 2.67 | 0.067 | 0.521 | ||||||||
| PC6 | 2.21 | 0.055 | 0.576 | ||||||||
| PC7 | 1.81 | 0.045 | 0.621 | ||||||||
| PC8 | 1.71 | 0.043 | 0.664 | ||||||||
| PC9 | 1.33 | 0.033 | 0.697 | ||||||||
| PC10 | 1.26 | 0.031 | 0.729 | ||||||||
| PC11 | 1.13 | 0.028 | 0.757 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujishiro, M.; Ishihara, H.; Ogawa, K.; Murase, T.; Nakamura, T.; Watanabe, K.; Sakoda, H.; Ono, H.; Yamamotoya, T.; Nakatsu, Y.; et al. Impact of Plasma Xanthine Oxidoreductase Activity on the Mechanisms of Distal Symmetric Polyneuropathy Development in Patients with Type 2 Diabetes. Biomedicines 2021, 9, 1052. https://doi.org/10.3390/biomedicines9081052
Fujishiro M, Ishihara H, Ogawa K, Murase T, Nakamura T, Watanabe K, Sakoda H, Ono H, Yamamotoya T, Nakatsu Y, et al. Impact of Plasma Xanthine Oxidoreductase Activity on the Mechanisms of Distal Symmetric Polyneuropathy Development in Patients with Type 2 Diabetes. Biomedicines. 2021; 9(8):1052. https://doi.org/10.3390/biomedicines9081052
Chicago/Turabian StyleFujishiro, Midori, Hisamitsu Ishihara, Katsuhiko Ogawa, Takayo Murase, Takashi Nakamura, Kentaro Watanabe, Hideyuki Sakoda, Hiraku Ono, Takeshi Yamamotoya, Yusuke Nakatsu, and et al. 2021. "Impact of Plasma Xanthine Oxidoreductase Activity on the Mechanisms of Distal Symmetric Polyneuropathy Development in Patients with Type 2 Diabetes" Biomedicines 9, no. 8: 1052. https://doi.org/10.3390/biomedicines9081052