Questioning Cause and Effect: Children with Severe Asthma Exhibit High Levels of Inflammatory Biomarkers Including Beta-Hexosaminidase, but Low Levels of Vitamin A and Immunoglobulins

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Sample Collection
2.2. Determination of β-HEX and Other Immune Mediators in the Plasma
2.3. Determination of Immunoglobulin Levels in Plasma
2.4. RBP Assay
2.5. Statistical Analyses
3. Results
3.1. Patient Demographics
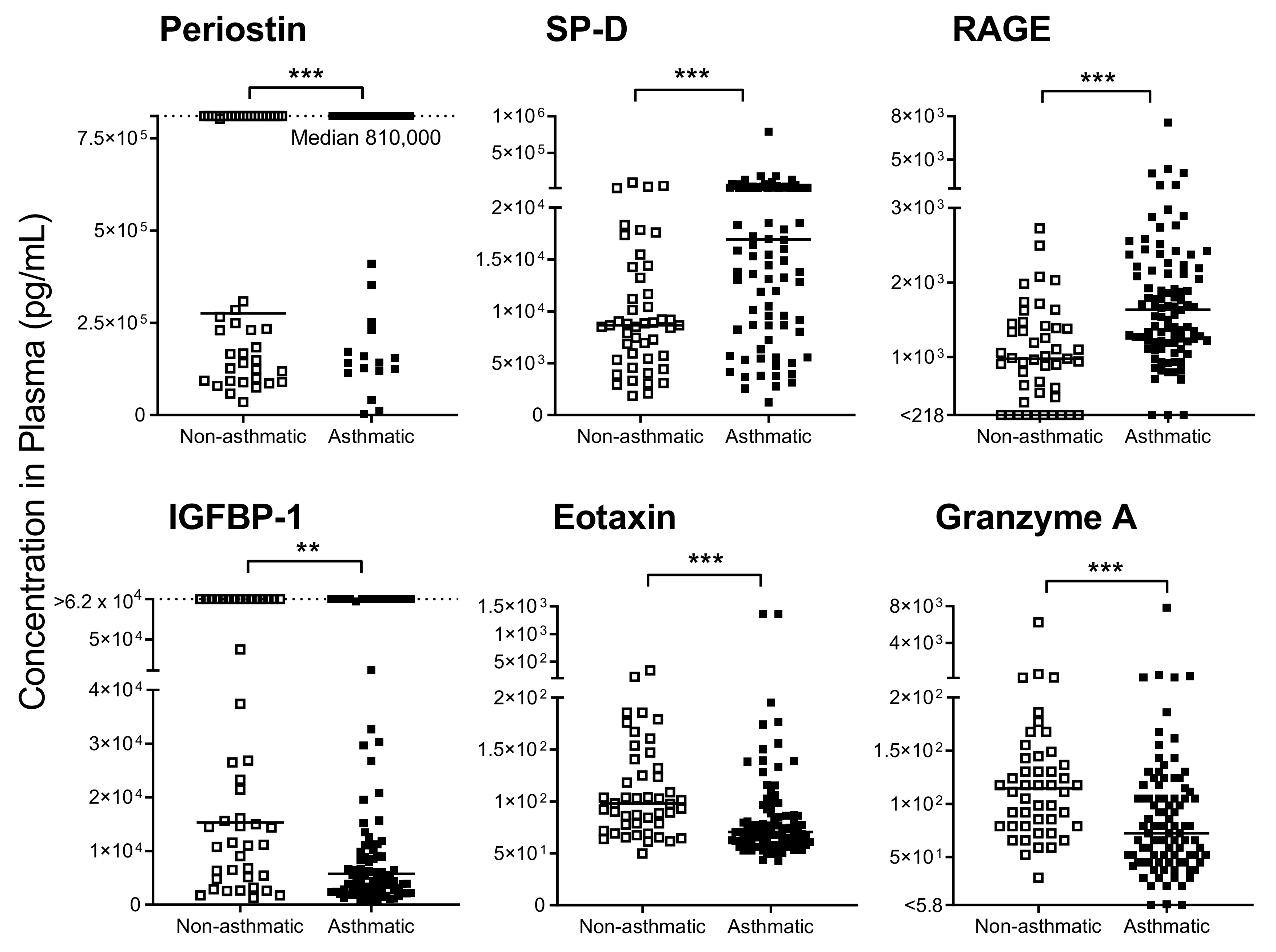
3.2. Cytokines/Chemokines Mark Severe Asthma in Children
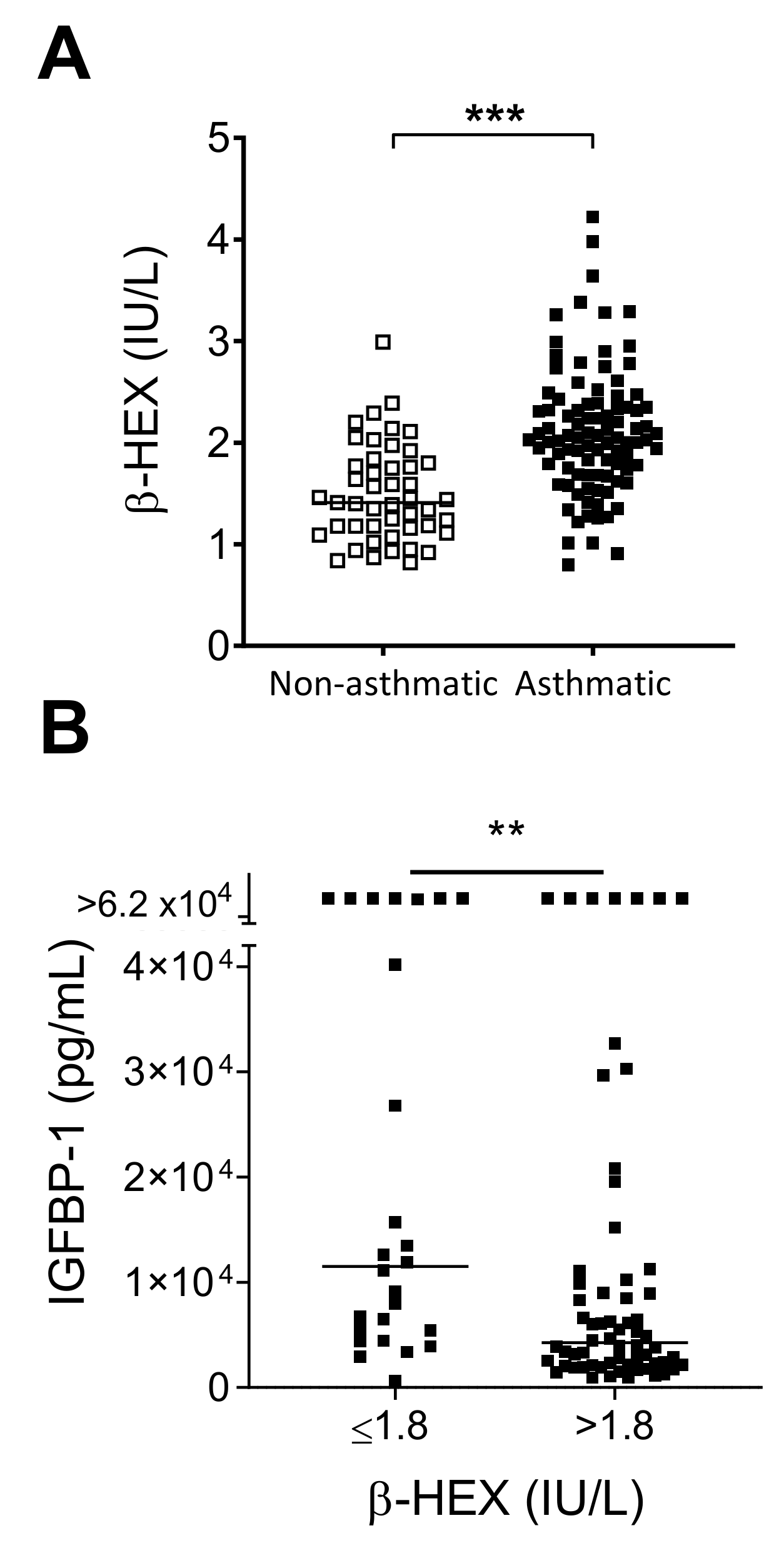
3.3. High β-HEX Levels in Severe Asthmatics
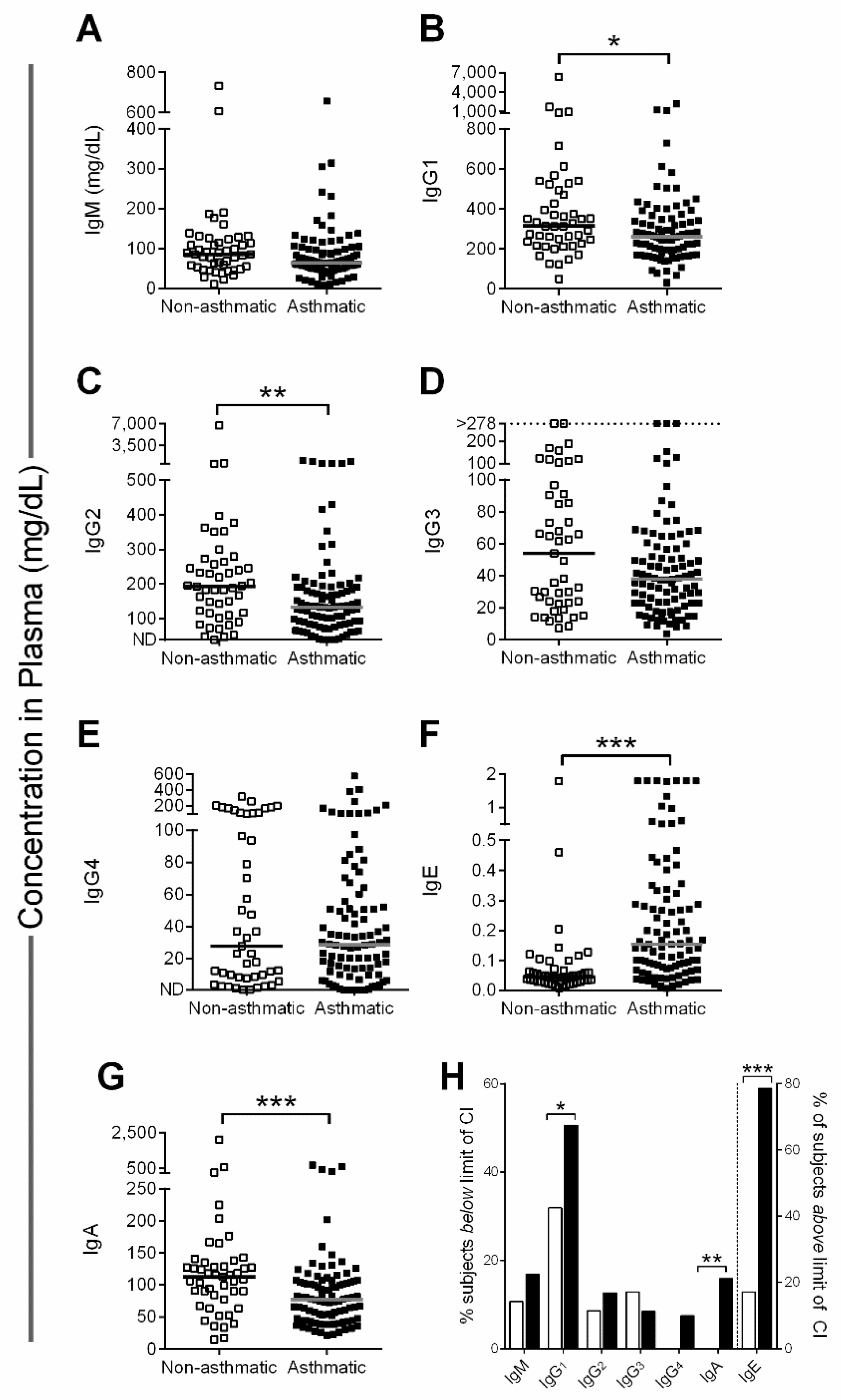
3.4. Children with Severe Asthma Have Low Plasma IgG and IgA Levels
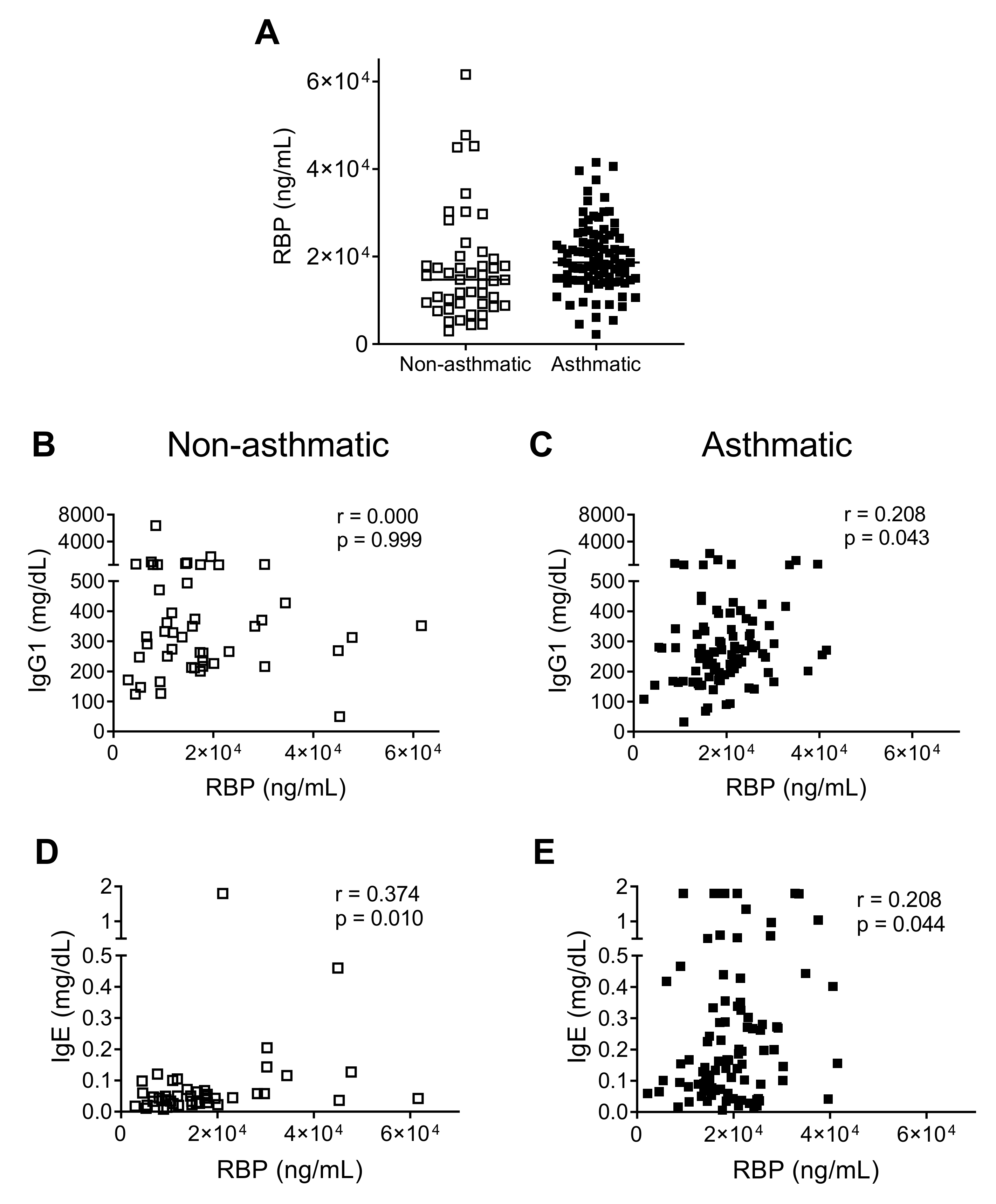
3.5. Low Plasma RBP Levels Correlate with Low IgG1 in Severe Asthmatics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Network, G.A. The Global Asthma Report 2018; Global Asthma Network: Auckland, New Zealand, 2018. [Google Scholar]
- Busse, W.W.; Morgan, W.J.; Gergen, P.J.; Mitchell, H.E.; Gern, J.E.; Liu, A.H.; Gruchalla, R.S.; Kattan, M.; Teach, S.J.; Pongracic, J.A.; et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N. Engl. J. Med. 2011, 364, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.; Chupp, G.; Nagase, H.; Albers, F.C.; Doyle, S.; Shen, Q.; Bratton, D.J.; Gunsoy, N.B. Anti-IL-5 treatments in patients with severe asthma by blood eosinophil thresholds: Indirect treatment comparison. J. Allergy Clin. Immunol. 2019, 143, 190–200.e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poddighe, D.; Brambilla, I.; Licari, A.; Marseglia, G.L. Omalizumab in the Therapy of Pediatric Asthma. Recent Pat. Inflamm. Allergy Drug Discov. 2018, 12, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Farne, H.A.; Wilson, A.; Powell, C.; Bax, L.; Milan, S.J. Anti-IL5 therapies for asthma. Cochrane Database Syst. Rev. 2017, 9, CD010834. [Google Scholar] [CrossRef] [PubMed]
- Agache, I.; Rocha, C.; Beltran, J.; Song, Y.; Posso, M.; Sola, I.; Alonso-Coello, P.; Akdis, C.; Akdis, M.; Canonica, G.W.; et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab and omalizumab) for severe allergic asthma: A systematic review for the EAACI Guidelines—Recommendations on the use of biologicals in severe asthma. Allergy 2020, 75, 1043–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. Asthma in the US. Available online: http://www.cdc.gov/vitalsigns/asthma/ (accessed on 23 June 2014).
- Nurmagambetov, T.; Kuwahara, R.; Garbe, P. The Economic Burden of Asthma in the United States, 2008–2013. Ann. Am. Thorac. Soc. 2018, 15, 348–356. [Google Scholar] [CrossRef]
- Hurwitz, J.L.; Penkert, R.R.; Xu, B.; Fan, Y.; Partridge, J.F.; Maul, R.W.; Gearhart, P.J. Hotspots for Vitamin-Steroid-Thyroid Hormone Response Elements Within Switch Regions of Immunoglobulin Heavy Chain Loci Predict a Direct Influence of Vitamins and Hormones on B Cell Class Switch Recombination. Viral. Immunol. 2016, 29, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Kakoti, G.; Dewan, H. Childhood Asthma in Tennessee 2003–2012; Tennessee Department of Health: Nashville, TN, USA, 2014. [Google Scholar]
- Penkert, R.R.; Iverson, A.; Rosch, J.W.; Hurwitz, J.L. Prevnar-13 vaccine failure in a mouse model for vitamin A deficiency. Vaccine 2017, 35, 6264–6268. [Google Scholar] [CrossRef]
- Holben, D.H.; Marshall, M.B. Position of the Academy of Nutrition and Dietetics: Food Insecurity in the United States. J. Acad. Nutr. Diet 2017, 117, 1991–2002. [Google Scholar] [CrossRef] [Green Version]
- CDC. National Center for Chronic Disease Prevention and Health Promotion, Division of Population Health. BRFSS Prevalence & Trends Data. Available online: https://www.cdc.gov/brfss/brfssprevalence/ (accessed on 11 January 2019).
- Bureau, U.C. US Census Bureau Quick Facts. Available online: https://www.census.gov/quickfacts/fact/table/memphiscitytennessee,tn,US/PST045218 (accessed on 11 January 2019).
- Lan, J.; Chung, H.S.; Maltby, K.; Stewart, S.; Vickery, J.; Michael, C.; Lew, D.B. High Prevalence of Atopy in Severe Persistent Pediatric Asthmatics in Memphis, Tennessee. Insights Allerg. Asthma Bronchitis 2016, 2. [Google Scholar] [CrossRef]
- Patel, N.; Penkert, R.R.; Jones, B.G.; Sealy, R.E.; Surman, S.L.; Sun, Y.; Tang, L.; DeBeauchamp, J.; Webb, A.; Richardson, J.; et al. Baseline Serum Vitamin A and D Levels Determine Benefit of Oral Vitamin A&D Supplements to Humoral Immune Responses Following Pediatric Influenza Vaccination. Viruses 2019, 11, 907. [Google Scholar] [CrossRef] [Green Version]
- Hurwitz, J.L.; Jones, B.G.; Penkert, R.R.; Gansebom, S.; Sun, Y.; Tang, L.; Bramley, A.M.; Jain, S.; McCullers, J.A.; Arnold, S.R. Low Retinol-Binding Protein and Vitamin D Levels Are Associated with Severe Outcomes in Children Hospitalized with Lower Respiratory Tract Infection and Respiratory Syncytial Virus or Human Metapneumovirus Detection. J. Pediatr. 2017, 187, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Mantzouranis, E.; Cruz, A.A.; Ait-Khaled, N.; Baena-Cagnani, C.E.; Bleecker, E.R.; Brightling, C.E.; Burney, P.; Bush, A.; Busse, W.W.; et al. Uniform definition of asthma severity, control, and exacerbations: Document presented for the World Health Organization Consultation on Severe Asthma. J. Allergy Clin. Immunol. 2010, 126, 926–938. [Google Scholar] [CrossRef] [PubMed]
- Tomasiak, M.M.; Tomasiak, M.; Zietkowski, Z.; Skiepko, R.; Bodzenta-Lukaszyk, A. N-acetyl-beta-hexosaminidase activity in asthma. Int. Arch. Allergy Immunol. 2008, 146, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Almekinder, J.; Manda, W.; Soko, D.; Lan, Y.; Hoover, D.R.; Semba, R.D. Evaluation of plasma retinol-binding protein as a surrogate measure for plasma retinol concentrations. Scand. J. Clin. Lab. Investig. 2000, 60, 199–203. [Google Scholar] [CrossRef]
- Baeten, J.M.; Richardson, B.A.; Bankson, D.D.; Wener, M.H.; Kreiss, J.K.; Lavreys, L.; Mandaliya, K.; Bwayo, J.J.; McClelland, R.S. Use of serum retinol-binding protein for prediction of vitamin A deficiency: Effects of HIV-1 infection, protein malnutrition, and the acute phase response. Am. J. Clin. Nutr. 2004, 79, 218–225. [Google Scholar] [CrossRef]
- Kanai, M.; Raz, A.; Goodman, D.S. Retinol-binding protein: The transport protein for vitamin A in human plasma. J. Clin. Invest. 1968, 47, 2025–2044. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.C. Vitamin A supplementation and retinoic acid treatment in the regulation of antibody responses in vivo. Vitam. Horm. 2007, 75, 197–222. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, P.; Gaston, B.; Bonfield, T.; Grabski, T.; Fletcher, D.; Shein, S.L. Periostin levels in children without respiratory disease. Pediatr. Pulmonol. 2019, 54, 200–204. [Google Scholar] [CrossRef]
- Decker, M.L.; Grobusch, M.P.; Ritz, N. Influence of Age and Other Factors on Cytokine Expression Profiles in Healthy Children-A Systematic Review. Front. Pediatr. 2017, 5, 255. [Google Scholar] [CrossRef]
- Kleiner, G.; Marcuzzi, A.; Zanin, V.; Monasta, L.; Zauli, G. Cytokine levels in the serum of healthy subjects. Mediat. Inflamm. 2013, 2013, 434010. [Google Scholar] [CrossRef] [PubMed]
- Caswell-Smith, R.; Hosking, A.; Cripps, T.; Holweg, C.; Matthews, J.; Holliday, M.; Maillot, C.; Fingleton, J.; Weatherall, M.; Braithwaite, I.; et al. Reference ranges for serum periostin in a population without asthma or chronic obstructive pulmonary disease. Clin. Exp. Allergy 2016, 46, 1303–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuishi, N.; Murakami, S.; Ohno, A.; Yamanaka, N.; Matsui, N.; Fukutsuji, K.; Yamada, S.; Itoh, K.; Akagi, M. Does beta-hexosaminidase function only as a degranulation indicator in mast cells? The primary role of beta-hexosaminidase in mast cell granules. J. Immunol. 2014, 193, 1886–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudraraju, R.; Surman, S.L.; Jones, B.G.; Sealy, R.; Woodland, D.L.; Hurwitz, J.L. Reduced frequencies and heightened CD103 expression among virus-induced CD8(+) T cells in the respiratory tract airways of vitamin A-deficient mice. Clin. Vaccine Immunol. 2012, 19, 757–765. [Google Scholar] [CrossRef]
- Sealy, R.; Jones, B.G.; Surman, S.L.; Hurwitz, J.L. Robust IgA and IgG-producing antibody forming cells in the diffuse-NALT and lungs of Sendai virus-vaccinated cotton rats associate with rapid protection against human parainfluenza virus-type 1. Vaccine 2010, 28, 6749–6756. [Google Scholar] [CrossRef] [Green Version]
- Surman, S.L.; Jones, B.G.; Rudraraju, R.; Sealy, R.E.; Hurwitz, J.L. Intranasal administration of retinyl palmitate with a respiratory virus vaccine corrects impaired mucosal IgA response in the vitamin A-deficient host. Clin. Vaccine Immunol. 2014, 21, 598–601. [Google Scholar] [CrossRef] [Green Version]
- Surman, S.L.; Jones, B.G.; Sealy, R.E.; Rudraraju, R.; Hurwitz, J.L. Oral retinyl palmitate or retinoic acid corrects mucosal IgA responses toward an intranasal influenza virus vaccine in vitamin A deficient mice. Vaccine 2014, 32, 2521–2524. [Google Scholar] [CrossRef] [Green Version]
- Surman, S.L.; Penkert, R.R.; Jones, B.G.; Sealy, R.E.; Hurwitz, J.L. Vitamin Supplementation at the Time of Immunization with a Cold-Adapted Influenza Virus Vaccine Corrects Poor Mucosal Antibody Responses in Mice Deficient for Vitamins A and D. Clin. Vaccine Immunol. 2016, 23, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Surman, S.L.; Rudraraju, R.; Sealy, R.; Jones, B.; Hurwitz, J.L. Vitamin A deficiency disrupts vaccine-induced antibody-forming cells and the balance of IgA/IgG isotypes in the upper and lower respiratory tract. Viral Immunol. 2012, 25, 341–344. [Google Scholar] [CrossRef]
- Kim, H.; Ellis, A.K.; Fischer, D.; Noseworthy, M.; Olivenstein, R.; Chapman, K.R.; Lee, J. Asthma biomarkers in the age of biologics. Allergy Asthma Clin. Immunol. Off. J. Can. Soc. Allergy Clin. Immunol. 2017, 13, 48. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Gao, P.; Zhi, Y.; Xu, W.; Wu, Y.; Yin, J.; Zhang, J. Periostin: Its role in asthma and its potential as a diagnostic or therapeutic target. Respir. Res. 2015, 16, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hol, B.E.; van de Graaf, E.A.; Out, T.A.; Hische, E.A.; Jansen, H.M. IgM in the airways of asthma patients. Int. Arch. Allergy Appl. Immunol. 1991, 96, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Loftus, B.G.; Price, J.F.; Lobo-Yeo, A.; Vergani, D. IgG subclass deficiency in asthma. Arch. Dis. Child. 1988, 63, 1434–1437. [Google Scholar] [CrossRef] [PubMed]
- Nouri-Aria, K.T.; Wachholz, P.A.; Francis, J.N.; Jacobson, M.R.; Walker, S.M.; Wilcock, L.K.; Staple, S.Q.; Aalberse, R.C.; Till, S.J.; Durham, S.R. Grass pollen immunotherapy induces mucosal and peripheral IL-10 responses and blocking IgG activity. J. Immunol. 2004, 172, 3252–3259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lúdvíksson, B.R.; Eiríksson, T.H.; Ardal, B.; Sigfússon, A.; Valdimarsson, H. Correlation between serum immunoglobulin A concentrations and allergic manifestations in infants. J. Pediatr. 1992, 121, 23–27. [Google Scholar] [CrossRef]
- Lew, D.B.; Rattazzi, M.C. Mitogenic effect of lysosomal hydrolases on bovine tracheal myocytes in culture. J. Clin. Investig. 1991, 88, 1969–1975. [Google Scholar] [CrossRef] [Green Version]
- Lew, D.B.; Michael, C.F.; Overbeck, T.; Robinson, W.S.; Rohman, E.L.; Lehman, J.M.; Patel, J.K.; Eiseman, B.; LeMessurier, K.S.; Samarasinghe, A.E.; et al. Beneficial effects of prebiotic Saccharomyces cerevisiae mannan on allergic asthma mouse models. J. Immunol. Res. 2017, 2017, 3432701. [Google Scholar] [CrossRef] [Green Version]
- Lew, D.B.; Songu-Mize, E.; Pontow, S.E.; Stahl, P.D.; Rattazzi, M.C. A mannose receptor mediates mannosyl-rich glycoprotein-induced mitogenesis in bovine airway smooth muscle cells. J. Clin. Investig. 1994, 94, 1855–1863. [Google Scholar] [CrossRef] [Green Version]
- He, S.H.; Zhang, H.Y.; Zeng, X.N.; Chen, D.; Yang, P.C. Mast cells and basophils are essential for allergies: Mechanisms of allergic inflammation and a proposed procedure for diagnosis. Acta Pharm. Sin. 2013, 34, 1270–1283. [Google Scholar] [CrossRef] [Green Version]
- Izuhara, K.; Ohta, S.; Ono, J. Using Periostin as a Biomarker in the Treatment of Asthma. Allergy Asthma Immunol. Res. 2016, 8, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Benfante, A.; Battaglia, S.; Principe, S.; Di Mitri, C.; Paterno, A.; Spatafora, M.; Scichilone, N. Asthmatics with high levels of serum surfactant protein D have more severe disease. Eur. Respir. J. 2016, 47, 1864–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benfante, A.; Battaglia, S.; Scichilone, N. Serum Surfactant Protein D as a Marker of Asthma Severity. Chest 2016, 150, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Imbalzano, E.; Quartuccio, S.; Di Salvo, E.; Crea, T.; Casciaro, M.; Gangemi, S. Association between HMGB1 and asthma: A literature review. Clin. Mol. Allergy 2017, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, P.G.; Boushey, H.A.; Dolganov, G.M.; Barker, C.S.; Yang, Y.H.; Donnelly, S.; Ellwanger, A.; Sidhu, S.S.; Dao-Pick, T.P.; Pantoja, C.; et al. Genome-wide profiling identifies epithelial cell genes associated with asthma and with treatment response to corticosteroids. Proc. Natl. Acad. Sci. USA 2007, 104, 15858–15863. [Google Scholar] [CrossRef] [Green Version]
- Milutinovic, P.S.; Alcorn, J.F.; Englert, J.M.; Crum, L.T.; Oury, T.D. The receptor for advanced glycation end products is a central mediator of asthma pathogenesis. Am. J. Pathol. 2012, 181, 1215–1225. [Google Scholar] [CrossRef] [Green Version]
- Oczypok, E.A.; Milutinovic, P.S.; Alcorn, J.F.; Khare, A.; Crum, L.T.; Manni, M.L.; Epperly, M.W.; Pawluk, A.M.; Ray, A.; Oury, T.D. Pulmonary receptor for advanced glycation end-products promotes asthma pathogenesis through IL-33 and accumulation of group 2 innate lymphoid cells. J. Allergy Clin. Immunol. 2015, 136, 747–756.e4. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, A.; Miyahara, N.; Waseda, K.; Kurimoto, E.; Fujii, U.; Tanimoto, Y.; Kataoka, M.; Yamamoto, Y.; Gelfand, E.W.; Yamamoto, H.; et al. Contrasting roles for the receptor for advanced glycation end-products on structural cells in allergic airway inflammation vs. airway hyperresponsiveness. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 309, L789–L800. [Google Scholar] [CrossRef] [Green Version]
- Hancock, D.B.; Eijgelsheim, M.; Wilk, J.B.; Gharib, S.A.; Loehr, L.R.; Marciante, K.D.; Franceschini, N.; van Durme, Y.M.; Chen, T.H.; Barr, R.G.; et al. Meta-analyses of genome-wide association studies identify multiple loci associated with pulmonary function. Nat. Genet. 2010, 42, 45–52. [Google Scholar] [CrossRef]
- Repapi, E.; Sayers, I.; Wain, L.V.; Burton, P.R.; Johnson, T.; Obeidat, M.; Zhao, J.H.; Ramasamy, A.; Zhai, G.; Vitart, V.; et al. Genome-wide association study identifies five loci associated with lung function. Nat. Genet. 2010, 42, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Ying, S.; Meng, Q.; Zeibecoglou, K.; Robinson, D.S.; Macfarlane, A.; Humbert, M.; Kay, A.B. Eosinophil chemotactic chemokines (eotaxin, eotaxin-2, RANTES, monocyte chemoattractant protein-3 (MCP-3), and MCP-4), and C-C chemokine receptor 3 expression in bronchial biopsies from atopic and nonatopic (Intrinsic) asthmatics. J. Immunol. 1999, 163, 6321–6329. [Google Scholar]
- Ying, S.; Robinson, D.S.; Meng, Q.; Rottman, J.; Kennedy, R.; Ringler, D.J.; Mackay, C.R.; Daugherty, B.L.; Springer, M.S.; Durham, S.R.; et al. Enhanced expression of eotaxin and CCR3 mRNA and protein in atopic asthma. Association with airway hyperresponsiveness and predominant co-localization of eotaxin mRNA to bronchial epithelial and endothelial cells. Eur. J. Immunol. 1997, 27, 3507–3516. [Google Scholar] [CrossRef] [PubMed]
- Zeibecoglou, K.; Macfarlane, A.J.; Ying, S.; Meng, Q.; Pavord, I.; Barnes, N.C.; Robinson, D.S.; Kay, A.B. Increases in eotaxin-positive cells in induced sputum from atopic asthmatic subjects after inhalational allergen challenge. Allergy 1999, 54, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Yamaguchi, M.; Yamamoto, K.; Nakajima, T.; Hirai, K.; Morita, Y.; Sano, Y.; Yamada, H. Eotaxin in induced sputum of asthmatics: Relationship with eosinophils and eosinophil cationic protein in sputum. Allergy 2000, 55, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Feltis, B.N.; Reid, D.W.; Ward, C.; Walters, E.H. BAL eotaxin and IL-5 in asthma, and the effects of inhaled corticosteroid and beta2 agonist. Respirology 2004, 9, 507–513. [Google Scholar] [CrossRef]
- Fukakusa, M.; Bergeron, C.; Tulic, M.K.; Fiset, P.O.; Al Dewachi, O.; Laviolette, M.; Hamid, Q.; Chakir, J. Oral corticosteroids decrease eosinophil and CC chemokine expression but increase neutrophil, IL-8, and IFN-gamma-inducible protein 10 expression in asthmatic airway mucosa. J. Allergy Clin. Immunol. 2005, 115, 280–286. [Google Scholar] [CrossRef]
- Tateno, H.; Nakamura, H.; Minematsu, N.; Nakajima, T.; Takahashi, S.; Nakamura, M.; Fukunaga, K.; Asano, K.; Lilly, C.M.; Yamaguchi, K. Plasma eotaxin level and severity of asthma treated with corticosteroid. Respir. Med. 2004, 98, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kim, S.R.; Oh, Y.; Cho, S.H.; Schleimer, R.P.; Lee, Y.C. Targeting insulin-like growth factor-I and insulin-like growth factor-binding protein-3 signaling pathways. A novel therapeutic approach for asthma. Am. J. Respir. Cell Mol. Biol. 2014, 50, 667–677. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Li, W.; Guo, Q.; Wang, Y.; Ma, L.; Zhang, X. Insulin-Like Growth Factor-1 Signaling in Lung Development and Inflammatory Lung Diseases. Biomed. Res. Int. 2018, 2018, 6057589. [Google Scholar] [CrossRef] [Green Version]
- Arora, P.; Kumar, V.; Batra, S. Vitamin A status in children with asthma. Pediatr. Allergy Immunol. Off. Publ. Eur. Soc. Pediatr. Allergy Immunol. 2002, 13, 223–226. [Google Scholar] [CrossRef]
- Gonzalez Barcala, F.J.; Pertega, S.; Bamonde, L.; Garnelo, L.; Perez Castro, T.; Sampedro, M.; Sanchez Lastres, J.; San Jose Gonzalez, M.A.; Lopez Silvarrey, A. Mediterranean diet and asthma in Spanish schoolchildren. Pediatr. Allergy Immunol. Off. Publ. Eur. Soc. Pediatr. Allergy Immunol. 2010, 21, 1021–1027. [Google Scholar] [CrossRef]
- Bai, Y.J.; Dai, R.J. Serum levels of vitamin A and 25-hydroxyvitamin D3 (25OHD3) as reflectors of pulmonary function and quality of life (QOL) in children with stable asthma: A case-control study. Medicine 2018, 97, e9830. [Google Scholar] [CrossRef] [PubMed]
- Cui, W.; Zhang, P.; Gu, J.; Tian, Y.; Gao, X.; Liu, Y.; Jin, Z.; Yan, D.; Zhu, X.; Li, D. Vitamin A Deficiency Promotes Inflammation by Induction of Type 2 Cytokines in Experimental Ovalbumin-Induced Asthma Murine Model. Inflammation 2016, 39, 1798–1804. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Britton, J.R.; Leonardi-Bee, J.A. Association between antioxidant vitamins and asthma outcome measures: Systematic review and meta-analysis. Thorax 2009, 64, 610–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassano, P.A. Nutritional effects on asthma aetiology and progression. Thorax 2009, 64, 560. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Akashi, K.; Watanabe, M.; Ikeda, Y.; Ashizuka, S.; Motoki, T.; Suzuki, R.; Sagara, N.; Yanagida, N.; Sato, S.; et al. Periostin as a biomarker for the diagnosis of pediatric asthma. Pediatr. Allergy Immunol. 2016, 27, 521–526. [Google Scholar] [CrossRef]
- Liao, S.C.; Cheng, Y.C.; Wang, Y.C.; Wang, C.W.; Yang, S.M.; Yu, C.K.; Shieh, C.C.; Cheng, K.C.; Lee, M.F.; Chiang, S.R.; et al. IL-19 induced Th2 cytokines and was up-regulated in asthma patients. J. Immunol. 2004, 173, 6712–6718. [Google Scholar] [CrossRef] [Green Version]
- Pukelsheim, K.; Stoeger, T.; Kutschke, D.; Ganguly, K.; Wjst, M. Cytokine profiles in asthma families depend on age and phenotype. PLoS ONE 2010, 5, e14299. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.G.; Oshansky, C.M.; Bajracharya, R.; Tang, L.; Sun, Y.; Wong, S.S.; Webby, R.; Thomas, P.G.; Hurwitz, J.L. Retinol binding protein and vitamin D associations with serum antibody isotypes, serum influenza virus-specific neutralizing activities and airway cytokine profiles. Clin. Exp. Immunol. 2016, 183, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Poddighe, D.; Vangelista, L. Effects of omalizumab on basophils: Potential biomarkers in asthma and chronic spontaneous urticaria. Cell. Immunol. 2020. [Google Scholar] [CrossRef]
- Bousquet, J.; Wahn, U.; Meltzer, E.O.; Fox, H.; Hedgecock, S.; Thomas, K.; Fowler-Taylor, A. Omalizumab: An anti-immunoglobulin E antibody for the treatment of allergic respiratory diseases. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2008, 17, 1–9. [Google Scholar] [CrossRef]
- Nimmagadda, S.R.; Spahn, J.D.; Leung, D.Y.; Szefler, S.J. Steroid-resistant asthma: Evaluation and management. Ann. Allergy Asthma Immunol. 1996, 77, 345–355. [Google Scholar] [CrossRef]
- Barnes, P.J. Corticosteroid resistance in airway disease. Proc. Am. Thorac. Soc. 2004, 1, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Heffler, E.; Madeira, L.N.G.; Ferrando, M.; Puggioni, F.; Racca, F.; Malvezzi, L.; Passalacqua, G.; Canonica, G.W. Inhaled Corticosteroids Safety and Adverse Effects in Patients with Asthma. J. Allergy Clin. Immunol. Pract. 2018, 6, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Dahl, R. Systemic side effects of inhaled corticosteroids in patients with asthma. Respir. Med. 2006, 100, 1307–1317. [Google Scholar] [CrossRef] [Green Version]
- Settipane, G.A.; Pudupakkam, R.K.; McGowan, J.H. Corticosteroid effect on immunoglobulins. J. Allergy Clin. Immunol. 1978, 62, 162–166. [Google Scholar] [CrossRef]
- Hershenson, M.B. Rhinovirus-Induced Exacerbations of Asthma and COPD. Scientifica 2013, 2013, 405876. [Google Scholar] [CrossRef] [Green Version]
- Feldman, A.S.; He, Y.; Moore, M.L.; Hershenson, M.B.; Hartert, T.V. Toward primary prevention of asthma. Reviewing the evidence for early-life respiratory viral infections as modifiable risk factors to prevent childhood asthma. Am. J. Respir. Crit. Care Med. 2015, 191, 34–44. [Google Scholar] [CrossRef]
- Takahashi, Y.; Miura, T.; Takahashi, K. Vitamin A is involved in maintenance of epithelial cells on the bronchioles and cells in the alveoli of rats. J. Nutr. 1993, 123, 634–641. [Google Scholar] [CrossRef]
- Ruuskanen, O.; Nurkka, A.; Helminen, M.; Viljanen, M.K.; Kayhty, H.; Kainulainen, L. Specific antibody deficiency in children with recurrent respiratory infections: A controlled study with follow-up. Clin. Exp. Immunol. 2013, 172, 238–244. [Google Scholar] [CrossRef]
- Ochs, H.D.; Wedgwood, R.J. IgG subclass deficiencies. Annu. Rev. Med. 1987, 38, 325–340. [Google Scholar] [CrossRef]
- Fauroux, B.; Simoes, E.A.F.; Checchia, P.A.; Paes, B.; Figueras-Aloy, J.; Manzoni, P.; Bont, L.; Carbonell-Estrany, X. The Burden and Long-term Respiratory Morbidity Associated with Respiratory Syncytial Virus Infection in Early Childhood. Infect. Dis. 2017, 6, 173–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irvin, C.; Zafar, I.; Good, J.; Rollins, D.; Christianson, C.; Gorska, M.M.; Martin, R.J.; Alam, R. Increased frequency of dual-positive TH2/TH17 cells in bronchoalveolar lavage fluid characterizes a population of patients with severe asthma. J. Allergy Clin. Immunol. 2014, 134, 1175–1186.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Smith, A.D.; Cheung, L.; Pham, Q.; Urban, J.F., Jr.; Dawson, H.D. Potentiation of IL-4 Signaling by Retinoic Acid in Intestinal Epithelial Cells and Macrophages-Mechanisms and Targets. Front. Immunol. 2020, 11, 605. [Google Scholar] [CrossRef] [PubMed]
- Mora, J.R.; Iwata, M.; Von Andrian, U.H. Vitamin effects on the immune system: Vitamins A and D take centre stage. Nat. Rev. Immunol. 2008, 8, 685–698. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Asthmatics | Nonasthmatics | |
|---|---|---|
| (Total n = 95) | (Total n = 47) | |
| Age (years) | ||
| 3–6 | 25 | 13 |
| 7–12 | 42 | 13 |
| 13–18 | 28 | 21 |
| Mean age (±SD) | 9.86 (±4.09) | 10.43 (±4.28) |
| Gender | ||
| Male | 70 | 22 |
| Female | 25 | 25 |
| Race | ||
| African American | 82 | 30 |
| White | 9 | 15 |
| Hispanic | 2 | 0 |
| Asian | 1 | 1 |
| Other | 0 | 1 |
| Undeclared | 1 | 0 |
| Therapy at Enrollment | ||
| Chronic Oral Steroids | 11 | 0 |
| High Dose ICS (LABA) | 84 (45) | 0 |
| Montelukast | 59 | 0 |
| Omalizumab | 6 | 0 |
| Allergen Immunotherapy | 16 | 0 |
| Anticholinergic | 1 | 0 |
| Other | 0 | ATB, Insulin, anti-epileptic |
| History of ICU Admission | 62 | 0 |
| #Asthma-Related Emergency Room Visits | ||
| 0–4 | 76 | 0 |
| 5–10 | 12 | 0 |
| >10 | 7 | 0 |
| Reported Smoke Exposure | 22 | Unknown |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samarasinghe, A.E.; Penkert, R.R.; Hurwitz, J.L.; Sealy, R.E.; LeMessurier, K.S.; Hammond, C.; Dubin, P.J.; Lew, D.B. Questioning Cause and Effect: Children with Severe Asthma Exhibit High Levels of Inflammatory Biomarkers Including Beta-Hexosaminidase, but Low Levels of Vitamin A and Immunoglobulins. Biomedicines 2020, 8, 393. https://doi.org/10.3390/biomedicines8100393
Samarasinghe AE, Penkert RR, Hurwitz JL, Sealy RE, LeMessurier KS, Hammond C, Dubin PJ, Lew DB. Questioning Cause and Effect: Children with Severe Asthma Exhibit High Levels of Inflammatory Biomarkers Including Beta-Hexosaminidase, but Low Levels of Vitamin A and Immunoglobulins. Biomedicines. 2020; 8(10):393. https://doi.org/10.3390/biomedicines8100393
Chicago/Turabian StyleSamarasinghe, Amali E., Rhiannon R. Penkert, Julia L. Hurwitz, Robert E. Sealy, Kim S. LeMessurier, Catherine Hammond, Patricia J. Dubin, and D. Betty Lew. 2020. "Questioning Cause and Effect: Children with Severe Asthma Exhibit High Levels of Inflammatory Biomarkers Including Beta-Hexosaminidase, but Low Levels of Vitamin A and Immunoglobulins" Biomedicines 8, no. 10: 393. https://doi.org/10.3390/biomedicines8100393