
The Urgent Threat of Clostridioides difficile Infection: A Glimpse of the Drugs of the Future, with Related Patents and Prospects


Abstract
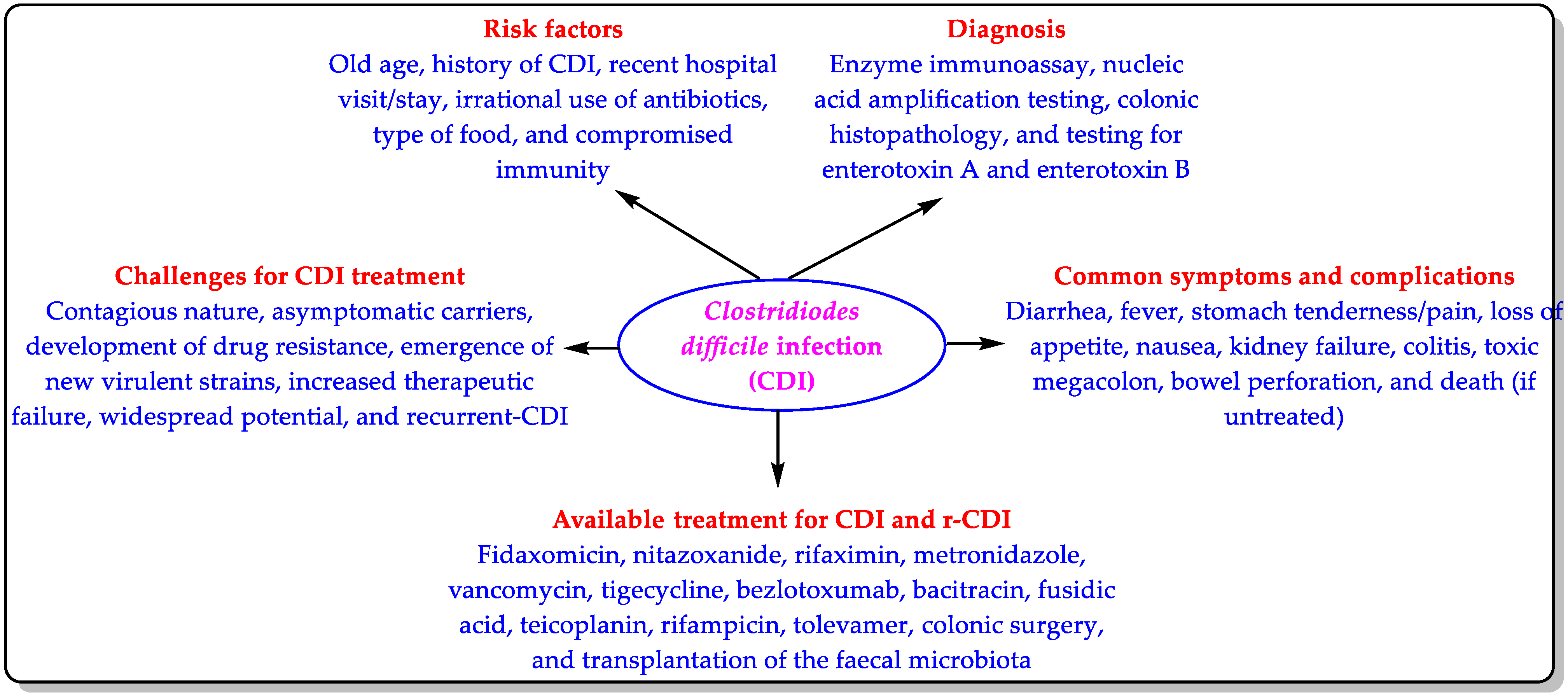
:1. Introduction
2. Methodology
3. Existing Treatments for CDI and Related Patents
4. Drugs of the Future for CDI
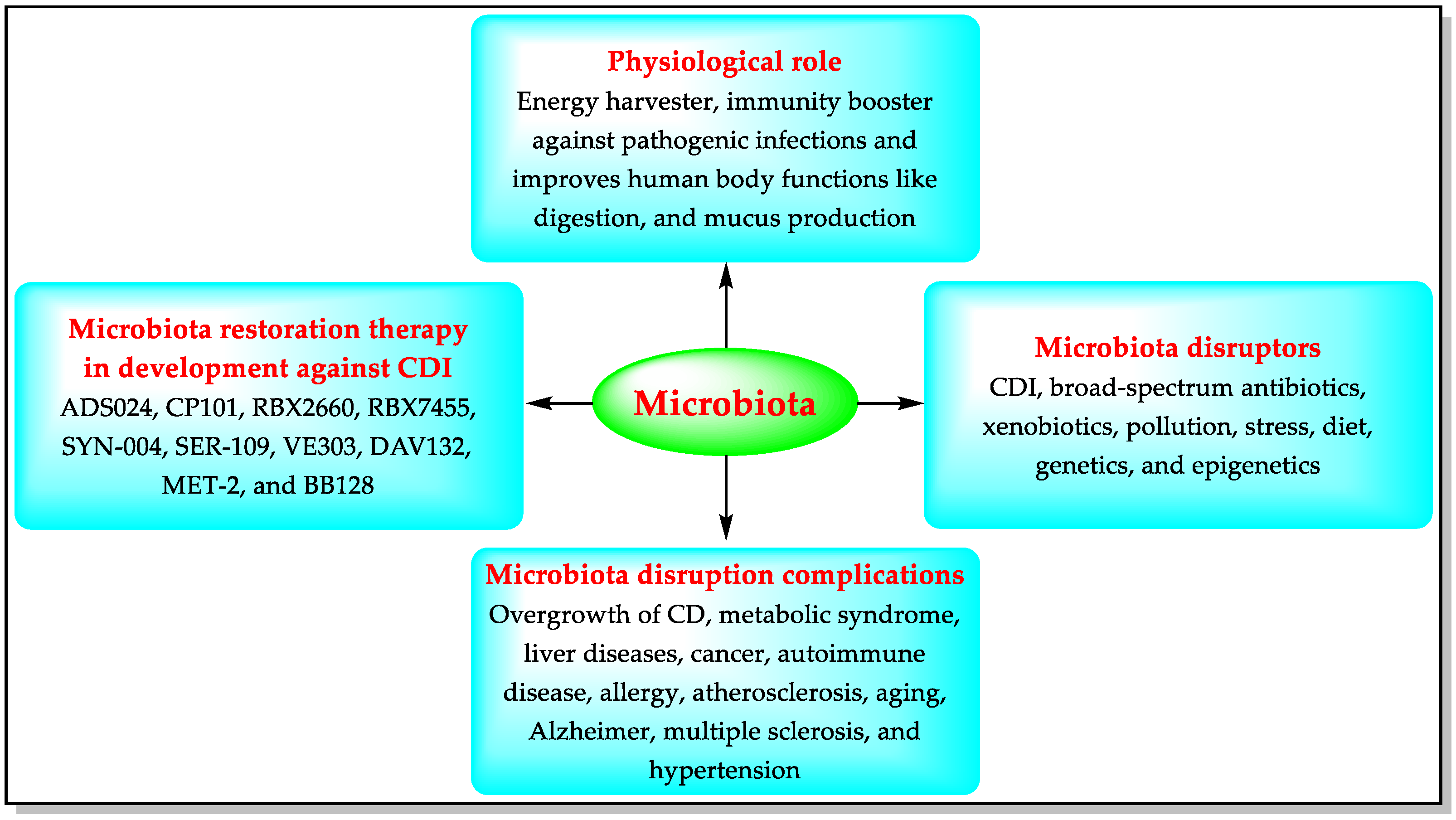
4.1. Microbiome-Modulating Agents (MMA)
4.1.1. ADS024 (ART24)
4.1.2. CP101
4.1.3. RBX2660
4.1.4. RBX7455
4.1.5. SYN-004 (Ribaxamase)
4.1.6. SER-109
4.1.7. VE303
4.1.8. DAV132
4.1.9. MET-2 (Microbial Ecosystem Therapeutic-2)
4.1.10. BB128
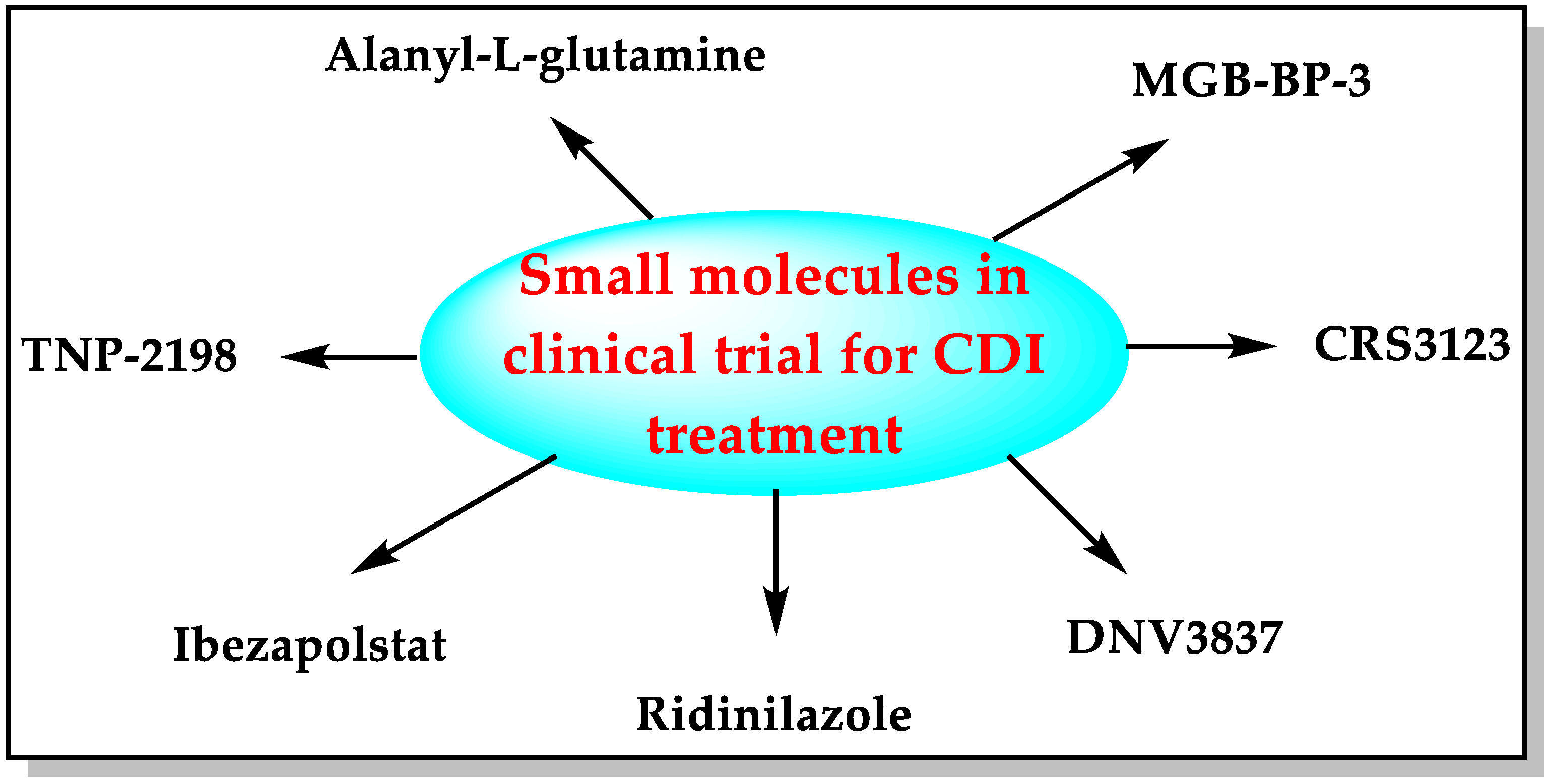
4.2. Small Molecules
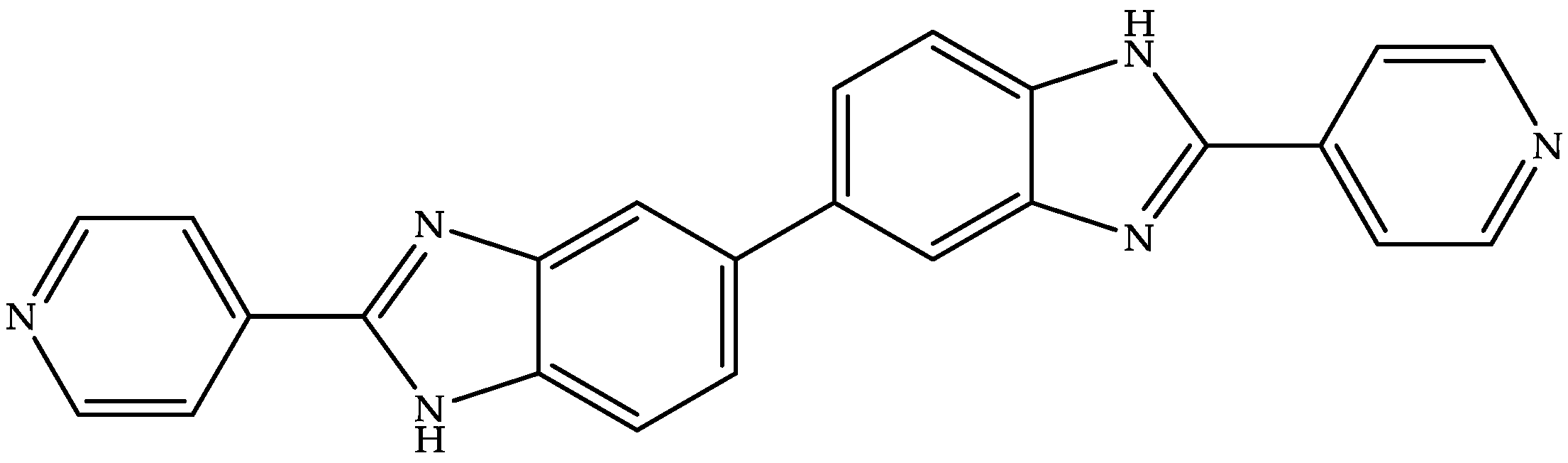
4.2.1. Ridinilazole (SMT19969)
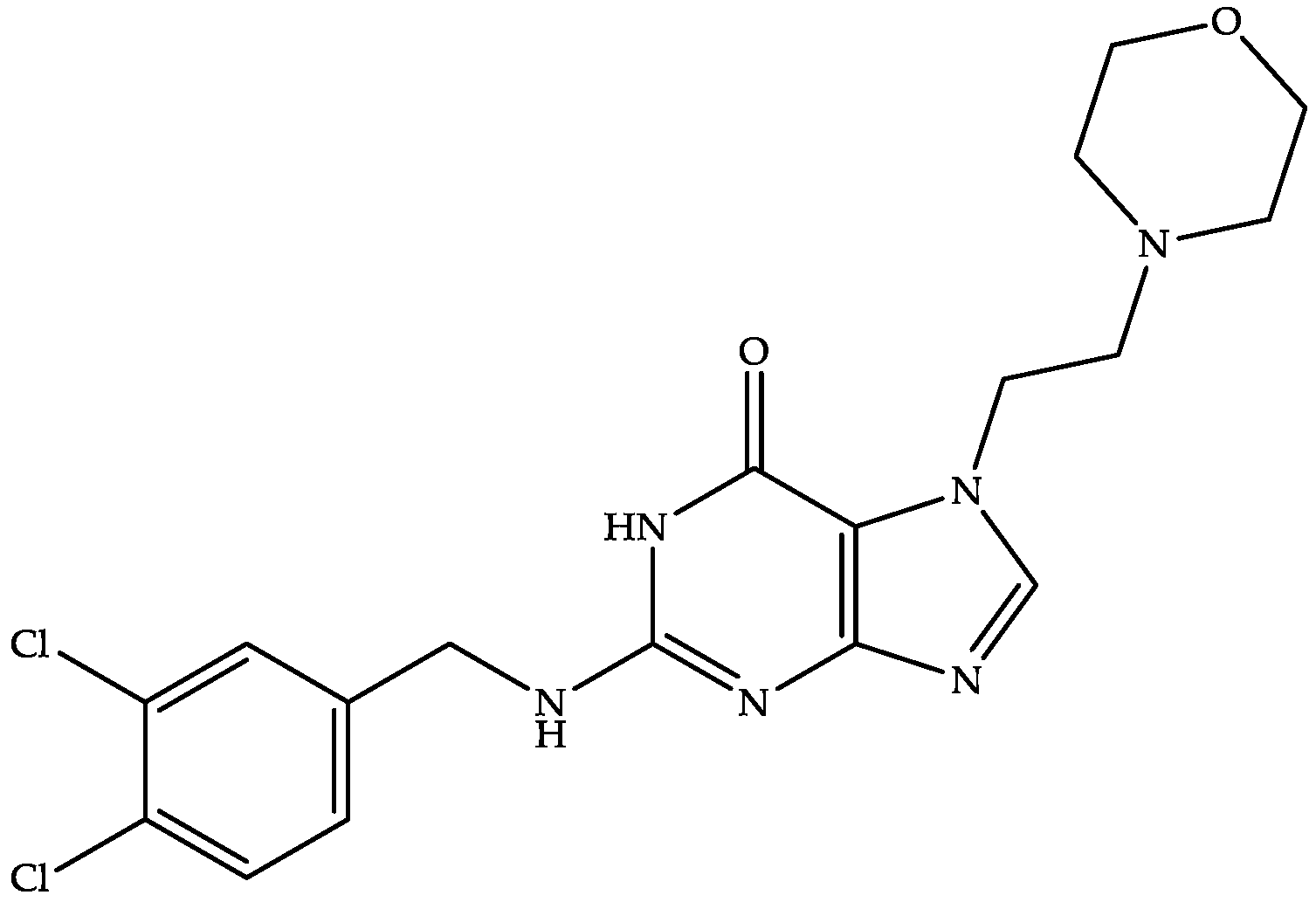
4.2.2. Ibezapolstat (ACX-362E)
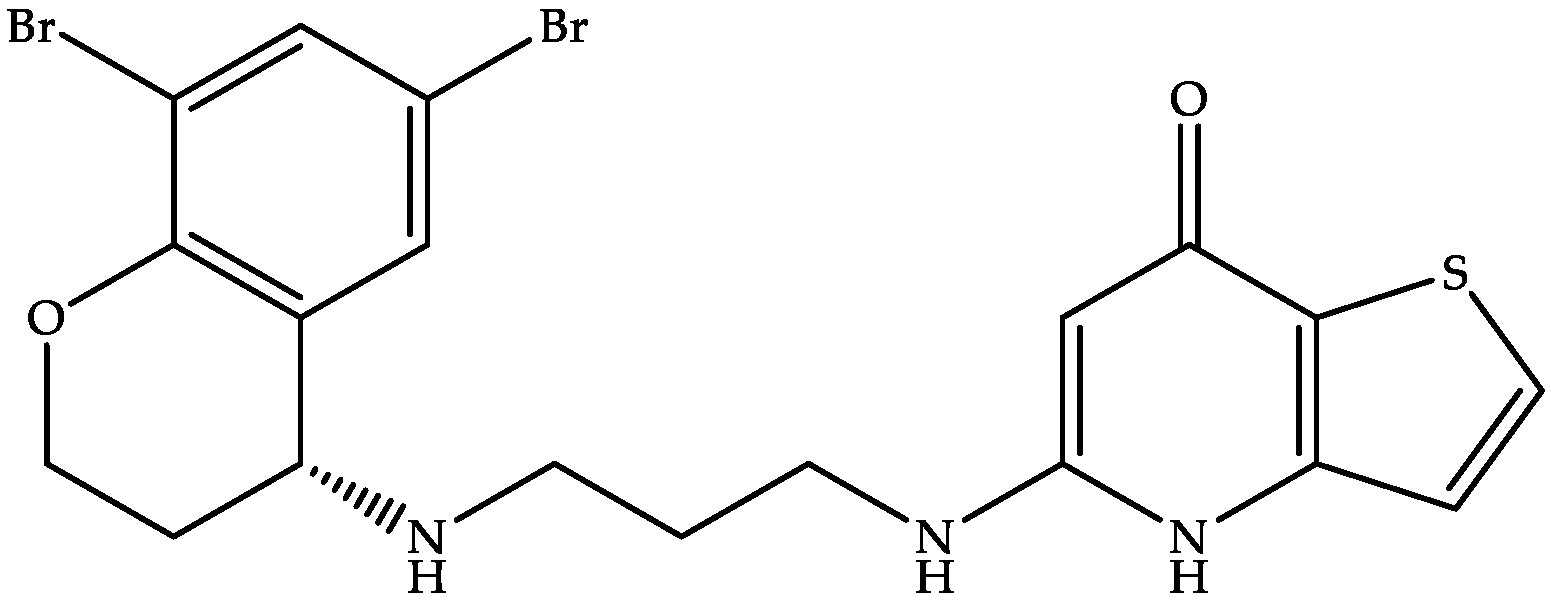
4.2.3. CRS3123
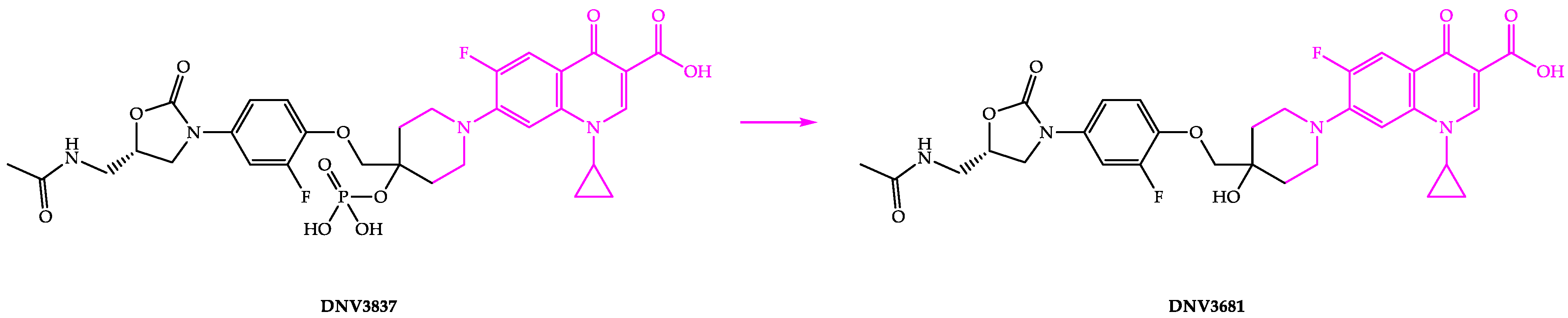
4.2.4. DNV3837
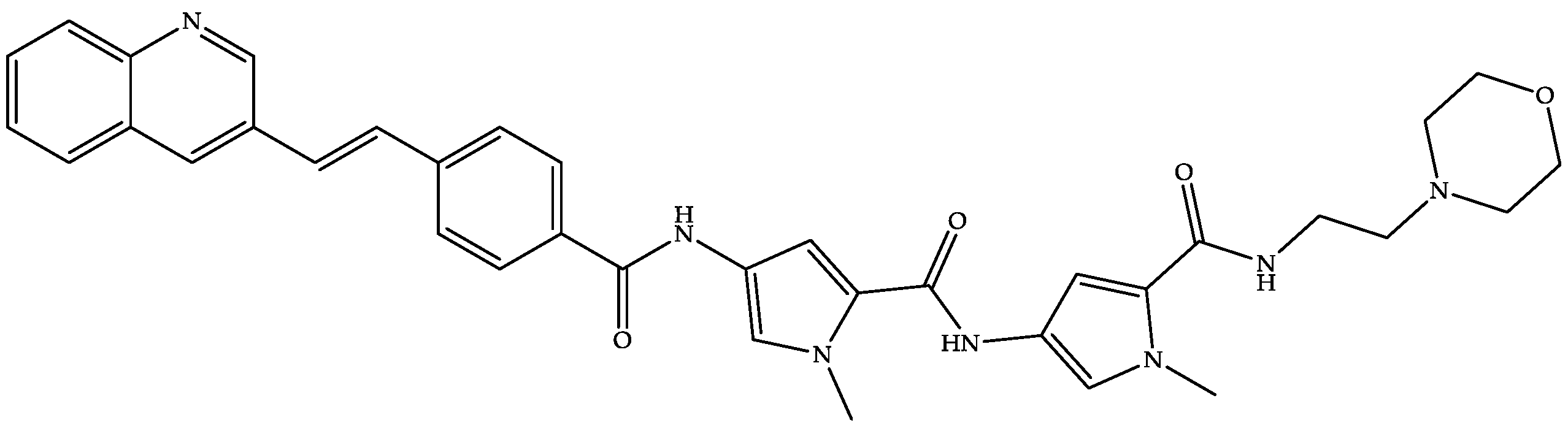
4.2.5. MGB-BP-3
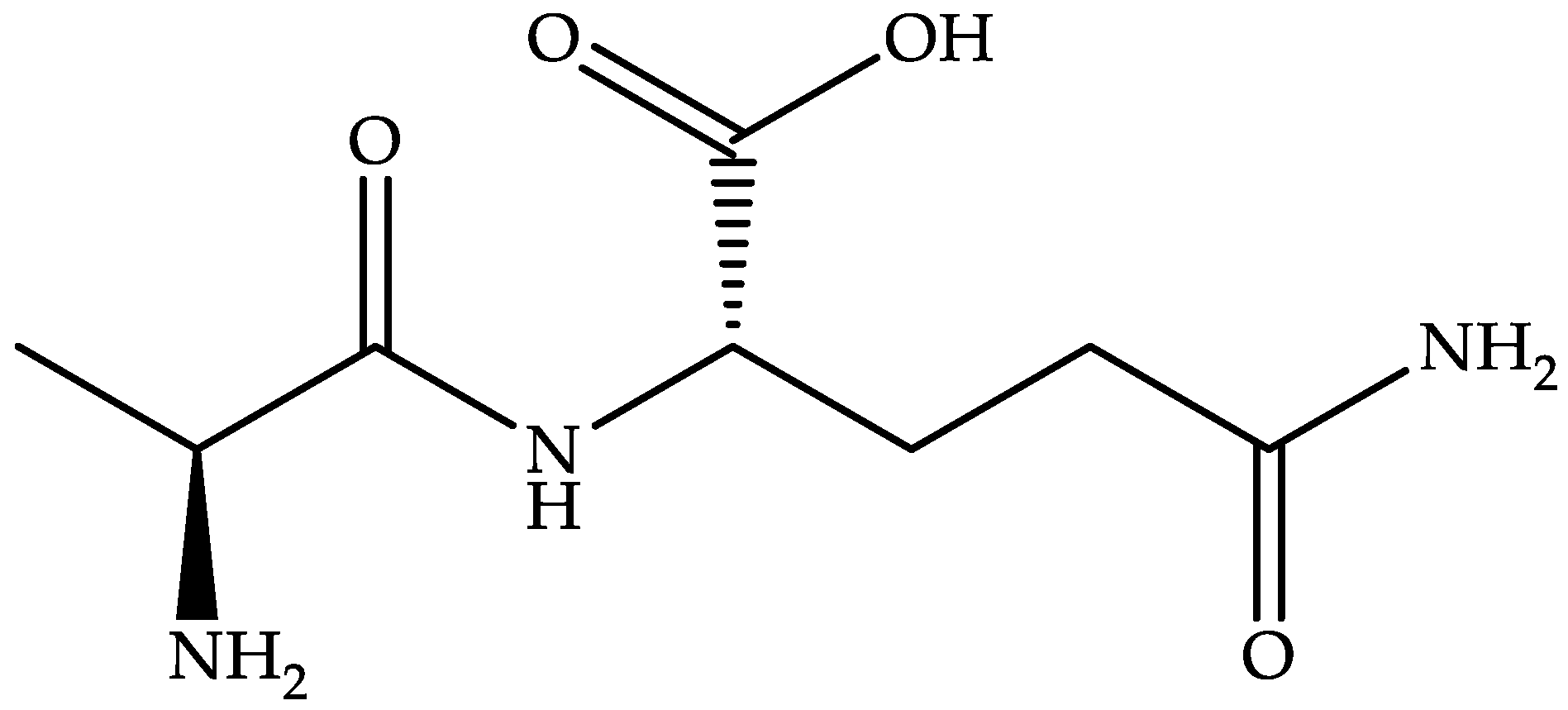
4.2.6. Alanyl-L-glutamine (DB11876)
4.2.7. TNP-2198 (Rifasutenizol)
4.3. Miscellaneous Therapies against CDI
4.3.1. IM-01
4.3.2. LMN-201
4.3.3. NTCD-M3
5. Drugs Not in Active Development
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moreno, M.A.; Furtner, F.; Rivara, F.P. Clostridium difficile: A cause of diarrhea in children. JAMA Pediatr. 2013, 167, 592. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Hagihara, M.; Asai, N.; Shibata, Y.; Yamagishi, Y.; Iwamoto, T.; Mikamo, H. A systematic review and meta-analysis of decontamination methods to prevent hospital environmental contamination and transmission of Clostridioides difficile. Anaerobe 2022, 73, 102478. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.A.; Smith, B.A.; Lewis, S.S. Novel and emerging sources of Clostridioides difficile infection. PLoS Pathog. 2019, 15, e1008125. [Google Scholar] [CrossRef] [PubMed]
- Kordus, S.L.; Thomas, A.K.; Lacy, D.B. Clostridioides difficile toxins: Mechanisms of action and antitoxin therapeutics. Nat. Rev. Microbiol. 2022, 20, 285–298. [Google Scholar] [CrossRef] [PubMed]
- McMillen, T.; Kamboj, M.; Babady, N.E. Comparison of Multilocus Sequence Typing and the Xpert C. difficile/Epi Assay for Identification of Clostridium difficile 027/NAP1/BI. J. Clin. Microbiol. 2016, 54, 775–778. [Google Scholar] [CrossRef]
- Drewes, J.L.; Chen, J.; Markham, N.O.; Knippel, R.J.; Domingue, J.C.; Tam, A.J.; Chan, J.L.; Kim, L.; McMann, M.; Stevens, C.; et al. Human Colon Cancer-Derived Clostridioides difficile Strains Drive Colonic Tumorigenesis in Mice. Cancer Discov. 2022, 12, 1873–1885. [Google Scholar] [CrossRef]
- Al-Jashaami, L.S.; DuPont, H.L. Management of Clostridium difficile Infection. Gastroenterol. Hepatol. 2016, 12, 609–616. [Google Scholar]
- Lang, V.; Gunka, K.; Ortlepp, J.R.; Zimmermann, O.; Groß, U. Risk Factors of Patients With Diarrhea for Having Clostridioides (Clostridium) difficile Infection. Front. Microbiol. 2022, 13, 840846. [Google Scholar] [CrossRef]
- Antibiotic Resistance Threats in the United States. Available online: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf (accessed on 14 December 2022).
- Romero-Rodríguez, A.; Martínez de la, P.C.; Troncoso-Cotal, S.; Guzmán, C.; Sánchez, S. Emerging alternatives against Clostridioides difficile infection. Anaerobe 2022, 78, 102638. [Google Scholar] [CrossRef]
- Martínez-Meléndez, A.; Cruz-López, F.; Morfin-Otero, R.; Maldonado-Garza, H.J.; Garza-González, E. An Update on Clostridioides difficile Binary Toxin. Toxins 2022, 14, 305. [Google Scholar] [CrossRef]
- Taylor, K.N.; McHale, M.T.; Saenz, C.C.; Plaxe, S.C. Diagnosis and treatment of Clostridium difficile (C. diff) colitis: Review of the literature and a perspective in gynecologic oncology. Gynecol. Oncol. 2017, 144, 428–437. [Google Scholar] [CrossRef]
- Mizusawa, M.; Carroll, K.C. The future of Clostridioides difficile diagnostics. Curr. Opin. Infect. Dis. 2021, 34, 483–490. [Google Scholar] [CrossRef]
- Chaar, A.; Feuerstadt, P. Evolution of clinical guidelines for antimicrobial management of Clostridioides difficile infection. Therap. Adv. Gastroenterol. 2021, 14, 17562848211011953. [Google Scholar] [CrossRef]
- Gupta, A.; Ananthakrishnan, A.N. Economic burden and cost-effectiveness of therapies for Clostridiodes difficile infection: A narrative review. Therap. Adv. Gastroenterol. 2021, 14, 17562848211018654. [Google Scholar] [CrossRef]
- Dayananda, P.; Wilcox, M.H. A Review of Mixed Strain Clostridium difficile Colonization and Infection. Front. Microbiol. 2019, 10, 692. [Google Scholar] [CrossRef]
- Dai, J.; Gong, J.; Guo, R. Real-world comparison of fidaxomicin versus vancomycin or metronidazole in the treatment of Clostridium difficile infection: A systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2022, 78, 1727–1737. [Google Scholar] [CrossRef]
- Khanna, S.; Sims, M.; Louie, T.J.; Fischer, M.; LaPlante, K.; Allegretti, J.; Hasson, B.R.; Fonte, A.T.; McChalicher, C.; Ege, D.S.; et al. SER-109: An Oral Investigational Microbiome Therapeutic for Patients with Recurrent Clostridioides difficile Infection (rCDI). Antibiotics 2022, 11, 1234. [Google Scholar] [CrossRef]
- Chen, J.; Lu, Y.; Du, Y.; Wang, H.; Wu, Q. Recent development of small-molecular inhibitors against Clostridioides difficile infection. Bioorg. Chem. 2022, 125, 105843. [Google Scholar] [CrossRef]
- Chen, J.; Li, Y.; Wang, S.; Zhang, H.; Du, Y.; Wu, Q.; Wang, H. Targeting Clostridioides difficile: New uses for old drugs. Drug Discov Today. 2022, 27, 1862–1873. [Google Scholar] [CrossRef]
- Khanna, S. My Treatment Approach to Clostridioides difficile Infection. Mayo Clin. Proc. 2021, 96, 2192–2204. [Google Scholar] [CrossRef]
- Kullar, R.; Tran, M.N.; Goldstein, E.J.C. Investigational Treatment Agents for Recurrent Clostridioides difficile Infection (rCDI). J. Exp. Pharmacol. 2020, 12, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Sandiford, S.K. Current developments in lantibiotic discovery for treating Clostridium difficile infection. Expert Opin. Drug Discov. 2019, 14, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Cammarota, G.; Gallo, A.; Ianiro, G.; Montalto, M. Emerging drugs for the treatment of Clostridium difficile. Expert Opin. Emerg. Drugs 2019, 24, 17–28. [Google Scholar] [CrossRef] [PubMed]
- 2020 Antibacterial Agents in Clinical and Preclinical Development: An Overview and Analysis. Available online: https://www.who.int/publications/i/item/9789240021303 (accessed on 14 December 2022).
- Imran, M.; Alsharari, A.S.; Tauseef, M.; Khan, S.A.; Hudu, S.A.; Abida. Mucormycosis medications: A patent review. Expert Opin. Ther. Pat. 2021, 31, 1059–1074. [Google Scholar] [CrossRef]
- Imran, M.; Alsharari, A.S.; Thabet, H.K.; Bakht, M.A.; Abida. Synthetic molecules as DprE1 inhibitors: A patent review. Expert Opin. Ther. Pat. 2021, 31, 759–772. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.A.; Alsharari, A.S.; Eltahir, M.M.M.; Alshammari, M.K.; Harshan, A.A.; Alshammari, N.A.; Abida. Small molecules as kinetoplastid specific proteasome inhibitors for leishmaniasis: A patent review from 1998 to 2021. Expert Opin. Ther. Pat. 2022, 32, 591–604. [Google Scholar] [CrossRef]
- National Library of Medicine. Available online: https://www.clinicaltrials.gov/ (accessed on 14 December 2022).
- National Library of Medicine. Available online: https://pubchem.ncbi.nlm.nih.gov/ (accessed on 14 December 2022).
- Murakami, Y.; Saito, H. Composition of Tiacumicin Compounds. U.S. Patent US9808530B2, 7 November 2017. [Google Scholar]
- Karas, A.J.; Longshaw, C.M.; Delgado-Herrera, L.; Zeiher, B.G. Dosage Regimen for a Tiacumicin Compound. U.S. Patent US10548912B2, 4 February 2020. [Google Scholar]
- Purandare, S.M.; Malhotra, G. Pharmaceutical Compositions for Rectal Administration. PCT Patent WO2014135891A1, 12 September 2014. [Google Scholar]
- Guang, B.; Yang, T.; Dong, R.; Liu, J.; Zhan, W.; Qin, C.; Xie, J.; Huang, S.; Peng, X.; Lai, Y.; et al. Novel Nitrothiazole Derivative and Application Thereof. Chinese Patent CN114044761B, 14 May 2022. [Google Scholar]
- Malhotra, G.; Joshi, K.; Ghosalkar, J. Pharmaceutical Compositions Comprising Rifaximin. U.S. Patent US11224591B2, 18 January 2022. [Google Scholar]
- Jahagirdar, H.A.; Kulkarni, R.; Kulkarni, S. Pharmaceutical Compositions of Rifaximin. U.S. Patent US8383151B2, 26 February 2013. [Google Scholar]
- Viscomi, G.C.; Chelazzi, L.; Grepioni, F.; Braga, D.; Kindt, M. Pharmaceutical Compositions Comprising Rifaximin and Amino Acids, Preparation Methods and Use Thereof. U.S. Patent US9452157B2, 27 September 2016. [Google Scholar]
- Angel, A.J.; Pawar, K.R.; Pillai, R.S. Rifaximin Liquid Formulations. PCT Patent WO2021058656A1, 1 April 2021. [Google Scholar]
- Reddy, V.M.; Prensky, W.; VedBrat, S. Synergistic Clofazimine/Metronidazole Combination for Treating Clostridium Difficile. U.S. Patent US2017143707A1, 25 May 2017. [Google Scholar]
- van der Aart, L.T.; Lemmens, N.A.; van Wamel, W.J.B.; van Wezel, G.P. Composition and Method for Treating Infections Caused by Vancomycin-Resistant Infectious Agents in a Subject. U.S. Patent US2019000789A1, 3 January 2019. [Google Scholar]
- Fujita, I.; Taguchi, N. Treatment of Clostridium Difficile Diarrhoea and Pseudomembranous Colitis. European Patent EP0456418B1, 25 September 1996. [Google Scholar]
- Diorio, C.R.; Shah, S.M.; Ali, K.A. Oral Formulations Comprising Tigecycline. PCT Patent WO2007075794A2, 5 July 2007. [Google Scholar]
- Crowe, S.; West, M.; Roberts, K.; Carlton, T.; Strokappe, N.; Verrips, T. Polypeptide Comprising an Immunoglobulin Chain Variable Domain Which Binds to Clostridium Difficile Toxin B. U.S. Patent US2018100008A1, 12 April 2018. [Google Scholar]
- Crowe, S.; West, M.; Roberts, K.; Carlton, T.; Strokappe, N.; Verrips, T. Polypeptide Comprising an Immunoglobulin Chain Variable Domain Which Binds to Clostridium Difficile Toxin A. U.S. Patent US2018100009A1, 12 April 2018. [Google Scholar]
- Aronoff, D. Treatment and Prevention of Clostridium Difficile Colitis Using Misoprostol. PCT Patent WO2018009789A1, 8 January 2017. [Google Scholar]
- Dong, S. Injection Suitable for Treating Clostridium Difficile Infection and Preparation Method Thereof. Chinese Patent CN106511266A, 22 March 2017. [Google Scholar]
- Bostwick, E.F.; Hoerr, R.A. Therapeutic Treatment of Clostridium Difficile Associated Diseases. U.S. Patent US5773000A, 30 June 1998. [Google Scholar]
- Jones, R. Fusidic Acid Dosing Regimens for Treatment of Bacterial Infections. Canadian Patent CA2767614C, 15 January 2019. [Google Scholar]
- Ma, Z.; Gregory, R. Novel Application of Rifamycin-Nitroimidazole Coupling Molecule. Chinese Patent CN104971061B, 7 November 2017. [Google Scholar]
- Chiu, C.W.; Tsai, P.J.; Lee, C.C.; Ko, W.C.; Hung, Y.P. Application of Microbiome Management in Therapy for Clostridioides difficile Infections: From Fecal Microbiota Transplantation to Probiotics to Microbiota-Preserving Antimicrobial Agents. Pathogens 2021, 10, 649. [Google Scholar] [CrossRef]
- Appanna, V.D. Dysbiosis, Probiotics, and Prebiotics: In Diseases and Health. In Human Microbes-The Power Within; Springer: Singapore, 2018; pp. 7684–7688. [Google Scholar]
- O’Donnell, M.M.; Hegarty, J.W.; Healy, B.; Schulz, S.; Walsh, C.J.; Hill, C.; Ross, R.P.; Rea, M.C.; Farquhar, R.; Chesnel, L. Identification of ADS024, a newly characterized strain of Bacillus velezensis with direct Clostridiodes difficile killing and toxin degradation bio-activities. Sci. Rep. 2022, 12, 9283. [Google Scholar] [CrossRef]
- Adiso Therapeutics. Available online: https://adisotx.com/science-and-pipeline/#pipeline (accessed on 14 December 2022).
- Farquhar, R.; Murphy, C.K.; Hill, C.; Ross, P.; Rea, M.; O’Donnell, M.; Healy, B.; Chesnel, L. Methods and Compositions for the Treatment of C. Difficile. U.S. Patent US11419900B2, 23 August 2022. [Google Scholar]
- Farquhar, R.; Chesnel, L.; Hill, C.; Ross, P.; Rea, M.; O’donnell, M.; Hagerty, J.; Schulz, S. Edible Products Comprising Bacterial Strains and Methods of Use. PCT Patent WO2021116983A1, 17 June 2021. [Google Scholar]
- Shin, J.H.; Warren, C.A. Prevention and treatment of recurrent Clostridioides difficile infection. Curr. Opin. Infect. Dis. 2019, 32, 482–489. [Google Scholar] [CrossRef]
- Khanna, S.; Kelly, C.R.; Louie, T.; Fisher, M.; Hota, S.; Misra, B.; Van Hise, N.W.; Yen, E.F.; Bullock, J.S.; Pullman, J.; et al. CP101, an Investigational Orally Administered Microbiome Therapeutic, Increases Intestinal Microbiome Diversity and Prevents Recurrent C. difficile Infection: Results From a Randomized, Placebo-Controlled Trial. American J. Gastroent. 2021, 116, S57. [Google Scholar] [CrossRef]
- Finch Therapeutics. Available online: https://www.finchtherapeutics.com/pipeline/ (accessed on 14 December 2022).
- Finch Therapeutics. Available online: https://www.finchtherapeutics.com/platform/#portfolio (accessed on 14 December 2022).
- RBX2660 Clinical Trials. Available online: https://www.rebiotix.com/clinical-trials/rbx2660-clinical-trials/ (accessed on 14 December 2022).
- Khanna, S.; Assi, M.; Lee, C.; Yoho, D.; Louie, T.; Knapple, W.; Aguilar, H.; Garcia-Diaz, J.; Wang, G.P.; Berry, S.M.; et al. Efficacy and Safety of RBX2660 in PUNCH CD3, a Phase III, Randomized, Double-Blind, Placebo-Controlled Trial with a Bayesian Primary Analysis for the Prevention of Recurrent Clostridioides difficile Infection. Drugs 2022, 82, 1527–1538. [Google Scholar] [CrossRef]
- Khanna, S.; Gerding, D.; Jones, C.; Blount, K. Altering the Microbiome: Patients With a Successful Outcome Following Microbiota-Based RBX2660 Treatment Trend Toward Human Microbiome Project Healthy Subjects’ Profile. Off. J. Am. Coll. Gastroent. 2017, 112, S86. [Google Scholar] [CrossRef]
- Jones, L.A.; Jones, C.R.; Sobcinski, M.K. Microbiota Restoration Therapy (MRT), Compositions and Methods of Manufacture. U.S. Patent US9782445B2, 10 October 2017. [Google Scholar]
- RBX7455. Available online: https://www.rebiotix.com/clinical-trials/rbx7455-oral-c-diff-prevention/ (accessed on 14 December 2022).
- Khanna, S.; Pardi, D.S.; Jones, C.; Shannon, W.D.; Gonzalez, C.; Blount, K. RBX7455, a non-frozen, orally administered investigational live biotherapeutic, is safe, effective, and shifts patients’ microbiomes in a phase 1 study for recurrent clostridioides difficile infections. Clin. Infect. Dis. 2021, 73, e1613–e1620. [Google Scholar] [CrossRef]
- Jones, L.A.; Jones, L.A. Microbiota Restoration Therapy (MRT) Compositions and Methods of Manufacture. PCT Patent WO2022051610A1, 10 March 2022. [Google Scholar]
- Theriva Biologics. Available online: https://therivabio.com/ (accessed on 14 December 2022).
- Kokai-Kun, J.F.; Roberts, T.; Coughlin, O.; Sicard, E.; Rufiange, M.; Fedorak, R.; Carter, C.; Adams, M.H.; Longstreth, J.; Whalen, H.; et al. The Oral β-Lactamase SYN-004 (Ribaxamase) Degrades Ceftriaxone Excreted into the Intestine in Phase 2a Clinical Studies. Antimicrob. Agents Chemother. 2017, 61, e02197-16. [Google Scholar] [CrossRef]
- Kaleko, M.; Connelly, S.; Van, D.B.; Marcel, R.M.; Peled, J.; Da Silva, M.B. Beta-Lactamase Compositions for Treatment of Graft Versus Host Disease. U.S. Patent US2022218800A1, 14 July 2022. [Google Scholar]
- Connelly, S.; Kaleko, M. Methods And Compositions For Attenuating Antibiotic Resistance. U.S. Patent US2019275120A1, 12 September 2019. [Google Scholar]
- Seres Therapeutics. Available online: https://www.serestherapeutics.com/our-programs/ (accessed on 14 December 2022).
- Vedanta Biosciences. Available online: https://www.vedantabio.com/pipeline/ve303 (accessed on 14 December 2022).
- Dsouza, M.; Menon, R.; Crossette, E.; Bhattarai, S.K.; Schneider, J.; Kim, Y.G.; Reddy, S.; Caballero, S.; Felix, C.; Cornacchione, L.; et al. Colonization of the live biotherapeutic product VE303 and modulation of the microbiota and metabolites in healthy volunteers. Cell Host Microbe. 2022, 30, 583–598.e8. [Google Scholar] [CrossRef]
- Norman, J.; Olle, B.; Roberts, B.; Menon, R. Methods of Decreasing Dysbiosis and Restoring a Microbiome. U.S. Patent US2022143108A1, 12 May 2022. [Google Scholar]
- Available online: https://www.who.int/publications/i/item/9789240047655 (accessed on 14 December 2022).
- Kampouri, E.; Croxatto, A.; Prod’hom, G.; Guery, B. Clostridioides difficile Infection, Still a Long Way to Go. J. Clin. Med. 2021, 10, 389. [Google Scholar] [CrossRef]
- Guk, J.; Guedj, J.; Burdet, C.; Andremont, A.; de Gunzburg, J.; Ducher, A.; Mentré, F. Modeling the Effect of DAV132, a Novel Colon-Targeted Adsorbent, on Fecal Concentrations of Moxifloxacin and Gut Microbiota Diversity in Healthy Volunteers. Clin. Pharmacol. Ther. 2021, 109, 1045–1054. [Google Scholar] [CrossRef]
- Bristol, A.; Kaleko, M.; Connelly, S. Beta-Lactamase Formulations and Uses Thereof. U.S. Patent US10105322B2, 23 October 2018. [Google Scholar]
- Nubiyota. Available online: https://nubiyota.com/pipeline/ (accessed on 14 December 2022).
- Chinna, A.M.; Sgarbossa, C.; Vazquez, G.; Bond, D.; Müller, D.; Milev, R. The Safety and Efficacy of Microbial Ecosystem Therapeutic-2 in People With Major Depression: Protocol for a Phase 2, Double-Blind, Placebo-Controlled Study. JMIR Res. Protoc. 2021, 10, e31439-e. [Google Scholar] [CrossRef]
- Kao, D.; Wong, K.; Franz, R.; Cochrane, K.; Sherriff, K.; Chui, L.; Lloyd, C.; Roach, B.; Bai, A.D.; Petrof, E.O.; et al. The effect of a microbial ecosystem therapeutic (MET-2) on recurrent Clostridioides difficile infection: A phase 1, open-label, single-group trial. Lancet Gastroenterol. Hepatol. 2021, 6, 282–291. [Google Scholar] [CrossRef]
- Allen-Vercoe, E. Compositions Comprising Co-Selected Microbiota and Methods for Use Thereof. U.S. Patent US2021069262A1, 11 March 2021. [Google Scholar]
- Summit Therapeutics. Available online: https://www.summittxinc.com/our-programmes/c-difficile-infection/ (accessed on 14 December 2022).
- Collins, D.A.; Riley, T.V. Ridinilazole: A novel, narrow-spectrum antimicrobial agent targeting Clostridium (Clostridioides) difficile. Lett. Appl. Microbiol. 2022, 75, 526–536. [Google Scholar] [CrossRef]
- Collins, D.A.; Wu, Y.; Tateda, K.; Kim, H.J.; Vickers, R.J.; Riley, T.V. Evaluation of the antimicrobial activity of ridinilazole and six comparators against Chinese, Japanese and South Korean strains of Clostridioides difficile. J. Antimicrob. Chemother. 2021, 76, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.X.; Trespidi, L.; Carniaux, J.F.; Timmins, P. Solid Tablet Dosage form of Ridinilazole. U.S. Patent US2022226249A1, 21 July 2022. [Google Scholar]
- Ibezapolstat. Available online: https://www.acurxpharma.com/pipeline/ibezapolstat (accessed on 14 December 2022).
- Murray, B.; Wolfe, C.; Marra, A.; Pillar, C.; Shinabarger, D. In vitro activity of the novel antibacterial agent ibezapolstat (ACX-362E) against Clostridioides difficile. J. Antimicrob. Chemother. 2020, 75, 2149–2155. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.Y. Deuterium-Substituted 7-Substituted-2-(Benzylamino)-6-Ozopurine Compounds and Uses Thereof. U.S. Patent US2022024925A1, 27 January 2022. [Google Scholar]
- CRS3123. Available online: https://crestonepharma.com/pipeline/crs3123-for-c-difficile/ (accessed on 14 December 2022).
- Lomeli, B.K.; Galbraith, H.; Schettler, J.; Saviolakis, G.A.; El-Amin, W.; Osborn, B.; Ravel, J.; Hazleton, K.; Lozupone, C.A.; Evans, R.J.; et al. Multiple-Ascending-Dose Phase 1 Clinical Study of the Safety, Tolerability, and Pharmacokinetics of CRS3123, a Narrow-Spectrum Agent with Minimal Disruption of Normal Gut Microbiota. Antimicrob. Agents Chemother. 2019, 64, e01395-19. [Google Scholar] [CrossRef] [PubMed]
- Aronoff, D. Treatment and Prevention of Clostridium Difficile Colitis Using Misoprostol. U.S. Patent US2022000884A1, 6 January 2022. [Google Scholar]
- Freeman, J.; Pilling, S.; Vernon, J.; Wilcox, M.H. In vitro activities of MCB3681 and eight comparators against Clostridium difficile isolates with known ribotypes and diverse geographical spread. Antimicrob. Agents Chemother. 2017, 61, e02077-16. [Google Scholar] [CrossRef]
- DNV3837. Available online: https://www.deinove.com/en/pipeline/dnv3837#7 (accessed on 14 December 2022).
- Carlson, T.J.; Gonzales-Luna, A.J.; Garey, K.W. Recent developments in antimicrobial therapy for gastrointestinal infections. Curr. Opinion Gastroent. 2021, 37, 30–36. [Google Scholar] [CrossRef]
- Antibacterials. Available online: https://www.mgb-biopharma.com/antibacterials/ (accessed on 14 December 2022).
- Monaghan, T.M.; Seekatz, A.M.; Mullish, B.H.; Moore-Gillon, C.C.E.R.; Dawson, L.F.; Ahmed, A.; Kao, D.; Chan, W.C. Clostridioides difficile: Innovations in target discovery and potential for therapeutic success. Expert Opin. Ther. Targets. 2021, 25, 949–963. [Google Scholar] [CrossRef]
- Carlson, T.J.; Gonzales-Luna, A.J. Antibiotic treatment pipeline for Clostridioides difficile infection (CDI): A wide array of narrow-spectrum agents. Curr. Infect. Dis. Rep. 2020, 22, 20. [Google Scholar] [CrossRef]
- Nova, M.V.; Nothnagel, L.; Thurn, M.; Travassos, P.B.; Herculano, L.S.; Bittencourt, P.R.S.; Novello, C.R.; Bazotte, R.B.; Wacker, M.G.; Bruschi, M.L. Development study of pectin/Surelease® solid microparticles for the delivery of L-alanyl-L-glutamine dipeptide. Food Hydrocolloids 2019, 89, 921–932. [Google Scholar] [CrossRef]
- Klaenhammer, T.R.; Guerrant, R.L.; Kolling, G.L.; Durmaz, E.; Timko, M.P.; Warren, C.A. Compositions and Methods for the Delivery of Therapeutic Peptides. Chinese Patent CN103221420A, 24 July 2013. [Google Scholar]
- TNP-2198 PO. Available online: http://www.tennorx.com/en/h-col-157.html (accessed on 14 December 2022).
- Ma, Z.; He, S.; Yuan, Y.; Zhuang, Z.; Liu, Y.; Wang, H.; Chen, J.; Xu, X.; Ding, C.; Molodtsov, V.; et al. Design, Synthesis, and Characterization of TNP-2198, a Dual-Targeted Rifamycin-Nitroimidazole Conjugate with Potent Activity against Microaerophilic and Anaerobic Bacterial Pathogens. J. Med. Chem. 2022, 65, 4481–4495. [Google Scholar] [CrossRef]
- Ma, Z.; Yuan, Y.; Liu, Y.; Wang, X. New Use of Rifamycin-Nitroimidazole Coupling Molecule. Chinese Patent CN106822119A, 13 June 2017. [Google Scholar]
- Immunimed. Available online: https://immunimed.com/vaccine-therapy (accessed on 14 December 2022).
- Maiti, P.K. Use of Polyclonal Antibodies Against Clostridium Difficile for Treatment of Inflammatory Bowel Disease. U.S. Patent US10513552B2, 24 December 2019. [Google Scholar]
- Maiti, P.K. Polyclonal Antibodies Against Clostridium Difficile and Uses Thereof. U.S. Patent US9873732B2, 23 January 2018. [Google Scholar]
- Lumen Bioscience. Available online: https://www.lumen.bio/news/lumen-bioscience-announces-clinical-advancement-lmn-201-c-difficile-infection (accessed on 14 December 2022).
- Hui, Z.; Michael, D.; Michael, T.; Mesfin, G.; Anissa, M.; Melanie, H.; Kristie, K.; Alex, P.; Benjamin, W.J.; Nhi, K.; et al. Using synthetic activity to design ultra-potent antibody cocktails. bioRxiv 2021. [Google Scholar] [CrossRef]
- Roberts, J.; Tasch, M.; Gewe, M.; Jester, B.; Saveria, T. Arthrospira Platensis Non-Parenteral Therapeutic Delivery Platform. U.S. Patent US2021338751A1, 4 November 2021. [Google Scholar]
- NTCD-M3. Available online: https://www.destinypharma.com/pipeline/clostridioides-difficile-infections/ (accessed on 14 December 2022).
- Sambol, S.P.; Johnson, S.; Cheknis, A.; Gerding, D.N. Absence of toxin gene transfer from Clostridioides difficile strain 630Δ erm to nontoxigenic C. difficile strain NTCD-M3r in filter mating experiments. PLoS ONE 2022, 17, e0270119. [Google Scholar] [CrossRef]
- Gerding, D.N.; Meyer, T.; Lee, C.; Cohen, S.H.; Murthy, U.K.; Poirier, A.; Van Schooneveld, T.C.; Pardi, D.S.; Ramos, A.; Barron, M.A.; et al. Administration of spores of nontoxigenic Clostridium difficile strain M3 for prevention of recurrent C. difficile infection: A randomized clinical trial. JAMA 2015, 313, 1719–1727. [Google Scholar] [CrossRef]
- Aires, J.; Barbut, F.; Ferraris, L. Non-Toxicogenic Strain of Clostridioides Difficile for Use in the Prevention and/or Treatment of an Infection Associated with Clostridioides Difficile and/or Associated Recurrences. European Patent EP3871683A1, 1 September 2021. [Google Scholar]
- Barman, T.K.; Kumar, M.; Mathur, T.; Namba, E.; Singh, D.; Chaira, T.; Kurosaka, Y.; Yamada, M.; Upadhyay, D.J.; Masuda, N. In Vitro and In Vivo Activities of DS-2969b, a Novel GyrB Inhibitor, and Its Water-Soluble Prodrug, DS11960558, against Methicillin-Resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2018, 62, e02556-17. [Google Scholar] [CrossRef]
- Oka, D.; Yamaya, N.; Kuno, T.; Asakawa, Y.; Shiragiku, T.; Chen, L.; Xue, J.; Mamuti, A.; Ye, F.; Sun, J.; et al. In Vitro and In Vivo Antibacterial Activities of a Novel Quinolone Compound, OPS-2071, against Clostridioides difficile. Antimicrob. Agents Chemother. 2021, 65, e01170-20. [Google Scholar] [CrossRef]
- Aronoff, D. Treatment and Prevention of Clostridium Difficile Colitis Using Misoprostol. U.S. Patent US2019298735A1, 3 October 2019. [Google Scholar]
- Hubschwerlen, C.; Panchaud, P.; Rager, T.; Specklin, J. Crystalline Forms of Cadazolid. U.S. Patent US10087171B2, 2 October 2018. [Google Scholar]
- Zackular, J.P.; Kirk, L.; Trindade, B.C.; Skaar, E.P.; Aronoff, D.M. Misoprostol protects mice against severe Clostridium difficile infection and promotes recovery of the gut microbiota after antibiotic perturbation. Anaerobe 2019, 58, 89–94. [Google Scholar] [CrossRef]
- McCafferty, D.G.; Cudic, P.; Frankel, B.A.; Barkallah, S.; Kruger, R.G.; Li, W. Chemistry and biology of the ramoplanin family of peptide antibiotics. Biopolymers 2002, 66, 261–284. [Google Scholar] [CrossRef]
- Petrosillo, N.; Granata, G.; Cataldo, M.A. Novel Antimicrobials for the Treatment of Clostridium difficile Infection. Front. Med. 2018, 5, 96. [Google Scholar] [CrossRef]
- Talton, J.D.; Kraus, C.N. Methods of Treatment of C. Difficile Spores with Ramoplanin. U.S. Patent US2017028016A1, 2 February 2017. [Google Scholar]
- Butler, M.S.; Gigante, V.; Sati, H.; Paulin, S.; Al-Sulaiman, L.; Rex, J.H.; Fernandes, P.; Arias, C.A.; Paul, M.; Thwaites, G.E.; et al. Analysis of the Clinical Pipeline of Treatments for Drug-Resistant Bacterial Infections: Despite Progress, More Action Is Needed. Antimicrob. Agents Chemother. 2022, 66, e0199121. [Google Scholar] [CrossRef]
- Leeds, J.; Sachdeva, M.; Mullin, S.; Dzink-Fox, J.; LaMarche, M. Mechanism of action of and mechanism of reduced susceptibility to the novel anti-Clostridium difficile compound LFF571. Antimicrob. Agents Chemother. 2012, 56, 4463–4465. [Google Scholar] [CrossRef]
- Iscla, I.; Wray, R.; Blount, P.; Larkins-Ford, J.; Conery, A.L.; Ausubel, F.M.; Ramu, S.; Kavanagh, A.; Huang, J.X.; Blaskovich, M.A.; et al. A new antibiotic with potent activity targets MscL. J Antibiot. 2015, 68, 453–462. [Google Scholar] [CrossRef]
- Nayak, S.U.; Griffiss, J.M.; Blumer, J.; O’Riordan, M.A.; Gray, W.; McKenzie, R.; Jurao, R.A.; An, A.T.; Le, M.; Bell, S.J.; et al. Safety, Tolerability, Systemic Exposure, and Metabolism of CRS3123, a Methionyl-tRNA Synthetase Inhibitor Developed for Treatment of Clostridium difficile, in a Phase 1 Study. Antimicrob. Agents Chemother. 2017, 61, e02760-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imran, M.; Khan, S.A.; Alshammari, M.K.; Alqahtani, A.M.; Alanazi, T.A.; Kamal, M.; Jawaid, T.; Ghoneim, M.M.; Alshehri, S.; Shakeel, F. Discovery, Development, Inventions and Patent Review of Fexinidazole: The First All-Oral Therapy for Human African Trypanosomiasis. Pharmaceuticals 2022, 15, 128. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Khan, S.A.; Alshammari, M.K.; Alreshidi, M.A.; Alreshidi, A.A.; Alghonaim, R.S.; Alanazi, F.A.; Alshehri, S.; Ghoneim, M.M.; Shakeel, F. Discovery, Development, Inventions, and Patent Trends on Mobocertinib Succinate: The First-in-Class Oral Treatment for NSCLC with EGFR Exon 20 Insertions. Biomedicines 2021, 9, 1938. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Kumar, A.M.; Asdaq, S.M.B.; Khan, S.A.; Alaqel, S.I.; Alshammari, M.K.; Alshehri, M.M.; Alshrari, A.S.; Mateq, A.A.; Al-Shammeri, A.M.; et al. Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19. Molecules 2021, 26, 5795. [Google Scholar] [CrossRef]
- Li, J.; Zhao, H.; Peng, Y.; Xio, P.M.; Nickel, D.; Shen, J. Clostridium Difficile Drug-Resistant/Low-Sensitivity Evolutionary Branch SNP Marker as well as Strain Category Identification Method and Application Thereof. Chinese Patent CN112481395A, 12 March 2021. [Google Scholar]
- Ko, G.P.; You, H.J.; Yu, J.S.; Choe, S.E. Composition for Treating or Preventing Clostridium Difficile Infection. PCT Patent WO2022039561A1, 24 February 2022. [Google Scholar]
- Sun, X.; Chen, Z.; Li, L. DNA Aptamer Capable of Being Specifically Combined with Clostridium Difficile Toxin TcdB as well as Preparation Method and Application of DNA Aptamer. Chinese Patent CN114736906A, 12 July 2022. [Google Scholar]
- Ward, B.; Winter, K. Vaccine, Method of Vaccination against Clostridium Difficile. PCT Patent WO2020061357A1, 26 March 2020. [Google Scholar]
- Laub, G.W. Foam Compositions for Treating Clostridioides Difficile infections. PCT Patent WO2022226300A1, 27 October 2022. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patent/Application Number (Applicant) | Summary |
|---|---|
| Fidaxomicin | |
| US9808530B2 (Astellas Pharma) | A pharmaceutical composition (a dry powder for an aqueous suspension, a dry granulate for an aqueous suspension, or a dispersible tablet for an aqueous suspension) to treat CDI comprising fidaxomicin and xanthan gum as an excipient, wherein the excipient is present in an amount to prevent foaming of the tiacumicin B compound in water [31]. |
| US10548912B2 (Astellas Pharma) | A patient-compliant novel dosage regimen of fidaxomicin (initial course, monitoring, assessment, and drug switching for specified days) with improved efficacy for CDI, r-CDI, and CD toxins [32]. The proposed regimen is also supposed to reduce the chances of r-CDI to <5% and be cost-effective. |
| WO2014135891A1 (Cipla Limited) | A pharmaceutical composition for rectal administration in the form of a foam comprising fidaxomicin and a suitable pharmaceutically acceptable excipient (e.g., propellants, emollient, humectants, pH-adjusting agent, surfactants, foaming agents, antioxidants, lubricants, etc.) for the treatment or maintenance of remission of infections caused by CD. The advantages of the claimed invention include targeted delivery, treatment of a large surface area, and bypassing the first-pass metabolism [33]. |
| Nitazoxanide | |
| CN114044761B (Chengdu Biobel Biotechnology) | Nitazoxanide-based small molecules, which can effectively inhibit CD growth, have lower toxicity than nitazoxanide, and have a low impact on the intestinal flora [34]. |
| Rifaximin | |
| US11224591B2 (Cipla) | A pharmaceutical composition of rifaximin for CDI comprising at least one bioavailability-enhancing agent (piperine). The experiments of this patent demonstrate a relative bioavailability of 189% when rifaximin is administered with piperine [35]. |
| US8383151B2 (Lupin) | A more patient-compliant controlled-release pharmaceutical composition of rifaximin (administered once a day) than Xifaxan (200 mg tablet of rifaximin, administered three times a day) to treat CDI [36]. The experimental results also establish similar efficacy of Xifaxan and the claimed controlled-release composition of rifaximin. |
| US9452157B2 (Alfa Wassermann) | A pharmaceutical composition for CDI comprising rifaximin and an amino acid (e.g., histidine, phenylalanine, proline, valine, leucine, etc.). The amino acids synergize the effect of rifaximin by allowing the release of higher rifaximin concentrations in the intestinal tract [37]. |
| WO2021058656A1 (Bausch Health Ireland) | A stable pharmaceutical composition with improved availability of rifaximin to the stomach and intestine, comprising rifaximin, castor oil, and a solubilizing excipient for treating CDI [38]. |
| Metronidazole | |
| US2017143707A1 (Kamtek) | A method of treating CDI with a synergistic combination of clofazimine, wherein the administration of said combination is synergistic compared with the administration of either clofazimine or metronidazole alone [39]. |
| Vancomycin | |
| US2019000789A1 (Universiteit Leiden) | A method of treating CDI with a combination of vancomycin and D-alanine amino acid. This patent application states that D-alanine lowers the vancomycin resistance of a vancomycin-resistant microorganism and helps improve and prolong the effect of vancomycin [40]. |
| EP0456418B1 (Kabushiki Kaisha Miyarisan Seibutsu Igaku Kenkyusho) | A composition comprising cells or spores of a butyric acid bacterium MIYAIRI 588 (CbM) and vancomycin to treat CDI. The short-term therapy with the claimed invention effectively prevented germination and propagation of CD in the intestine without impairing the intestinal microflora, thereby providing a complete cure for the disease, including preventing the recurrence of the disease [41]. |
| Tigecycline | |
| WO2007075794A2 (Wyeth Corporation) | Use of enteric-coated tigecycline for treating CDI-associated colitis. The enteric coating reduced the blood bioavailability of tigecycline and kept tigecycline within the stomach for local action against CD [42]. |
| Immunoglobulin | |
| US2018100008A1 (Vhsquared) | A polypeptide-based immunoglobulin that binds and neutralizes CD toxin B [43]. |
| US2018100009A1 (Vhsquared) | A polypeptide-based immunoglobulin that binds and neutralizes CD toxin A [44]. |
| Bezlotoxumab | |
| WO2018009789A1 (Vanderbilt University) | A method for treating or preventing CDI with a combination of misoprostol and bezlotoxumab. However, this patent application is silent about the experimental details of the claimed invention [45]. |
| CN106511266A (Dong Shuqing) | An injection dosage form of bezlotoxumab to treat CDI [46]. |
| Bacitracin | |
| US5773000A (Galagen) | A method of CDI with a combination of anti-CD bovine immunoglobulin, vancomycin, bacitracin, or metronidazole [47]. |
| Fusidic acid | |
| CA2767614C (Cempra Pharmaceuticals) | A method of treating various bacterial infections, including CDI, with a loading dose (1200 mg) and maintenance dose (600 mg) of fusidic acid [48]. However, this patent is silent about the experimental details of the claimed invention against CD. |
| Rifampicin | |
| CN104971061B (Dannuo Pharmaceutical) | The use of a rifamycin–nitroimidazole coupling molecule to treat CDI, H. pylori tuberculosis, etc. [49]. |
| Drug (USFDA Designation) | Developer | Mechanism of Action | Phase |
|---|---|---|---|
| ADS024 (Fast-track) | Adiso Therapeutics | MAA | Phase I completed |
| CP101 (Breakthrough and fast-track) | Finch Therapeutics | MAA | Phase III |
| RBX2660 (Fast-track, breakthrough, and orphan drug) | Rebiotix | MAA | Phase III |
| RBX7455 | Rebiotix | MAA | Phase I completed |
| SYN-004 | Theriva Biologics | MAA | Phase II completed |
| SER-109 (Breakthrough and orphan drug) | Seres Therapeutics | MAA | Phase III completed |
| VE303 | Vedanta Biosciences | MAA | Phase II completed |
| DAV132 | Da Volterra | MAA | Phase II completed |
| MET-2 | NuBiyota | MAA | Phase I completed |
| BB128 | BiomeBank | MAA | Marketing authorization application submitted in Australia |
| Ridinilazole (Fast-track, breakthrough, and QIPD) | Summit Therapeutics | Prevents cell division | Phase III completed |
| Ibezapolstat (QIDP and fast-track) | Acurx Pharmaceuticals | Inhibitor of DNA polymerase IIIC | Phase III |
| CRS3123 | Crestone Pharma | Methionyl-tRNA synthase inhibitor | Phase II |
| DNV3837 (Fast track and QIDP) | Deinove | Inhibits bacterial DNA gyrase and protein synthesis | Phase II |
| MGB-BP-3 (QIPD and fast-track) | MGB Biopharma | Transcription inhibitor | Phase III |
| Alanyl-L-glutamine | University of Virginia | Blocks caspase-8 activation | Phase II |
| TNP-2198 | TenNor Therapeutics | RNA polymerase inhibitor | Phase Ib/IIa |
| IM-01 | ImmuniMed | Neutralizes the CD toxins | Phase II |
| LMN-201 | Lumen Bioscience | Neutralizes CD toxins and destroys the cell wall of CD | Phase II/III |
| NTCD-M3 | Destiny Pharma | A non-toxic strain of CD that makes a “ground cover” in the colon | Phase III |
| Drug | Developer | Mechanism of Action | Reference |
|---|---|---|---|
| DS-2969b | Daiichi Sankyo | GyrB antagonist | [75,114] |
| OPS-2071 | Otsuka Pharmaceutical | DNA gyrase inhibitor | [75,115,116] |
| Cadazolid | Actelion Pharmaceuticals | Protein synthesis inhibitor | [22,75,117] |
| Misoprostol | Vanderbilt University and the National Institutes of Health | Prostaglandin analog | [92,118] |
| Ramoplanin | Nanotherapeutics | Cell wall synthesis inhibitor | [75,119,120,121] |
| KB109 | Kaleido Biosciences | Microbiome metabolic therapeutic | [75,122] |
| LFF571 | Novartis | Protein synthesis inhibitor | [22,123] |
| Ramizol | Boulos & Cooper Pharmaceuticals | Inhibits mechanosensitive ion channels of large conductance (MscL) | [22,124] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshrari, A.S.; Hudu, S.A.; Elmigdadi, F.; Imran, M. The Urgent Threat of Clostridioides difficile Infection: A Glimpse of the Drugs of the Future, with Related Patents and Prospects. Biomedicines 2023, 11, 426. https://doi.org/10.3390/biomedicines11020426
Alshrari AS, Hudu SA, Elmigdadi F, Imran M. The Urgent Threat of Clostridioides difficile Infection: A Glimpse of the Drugs of the Future, with Related Patents and Prospects. Biomedicines. 2023; 11(2):426. https://doi.org/10.3390/biomedicines11020426
Chicago/Turabian StyleAlshrari, Ahmed S., Shuaibu Abdullahi Hudu, Fayig Elmigdadi, and Mohd. Imran. 2023. "The Urgent Threat of Clostridioides difficile Infection: A Glimpse of the Drugs of the Future, with Related Patents and Prospects" Biomedicines 11, no. 2: 426. https://doi.org/10.3390/biomedicines11020426