
The Impact of Neutrophil-to-Lymphocyte Ratio after Two Courses of Pembrolizumab for Oncological Outcomes in Patients with Metastatic Urothelial Carcinoma

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment Schedule
2.3. Patient Evaluation
2.4. Endpoints and Statistical Analysis
3. Results
3.1. Patient Characteristics
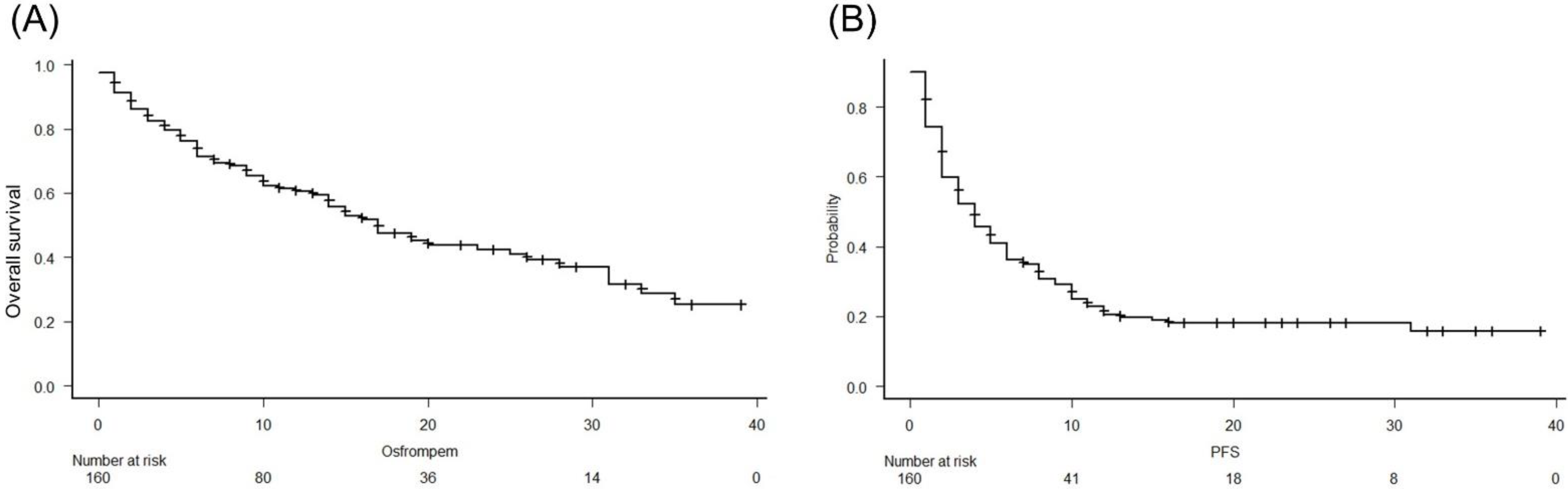
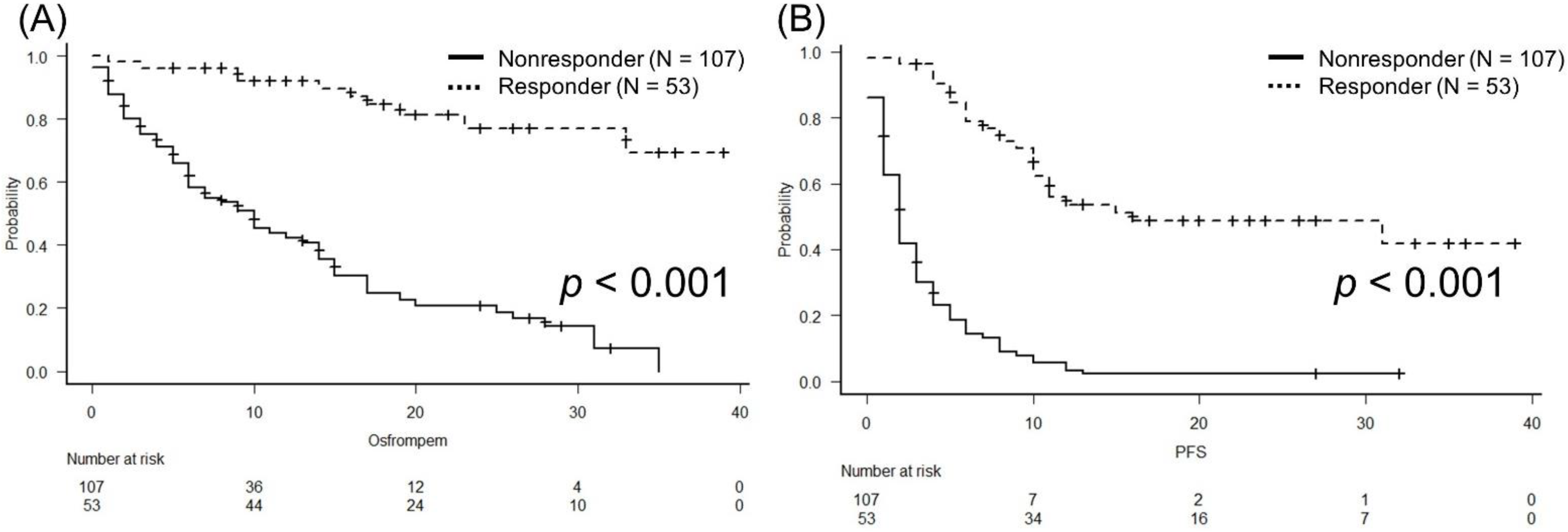
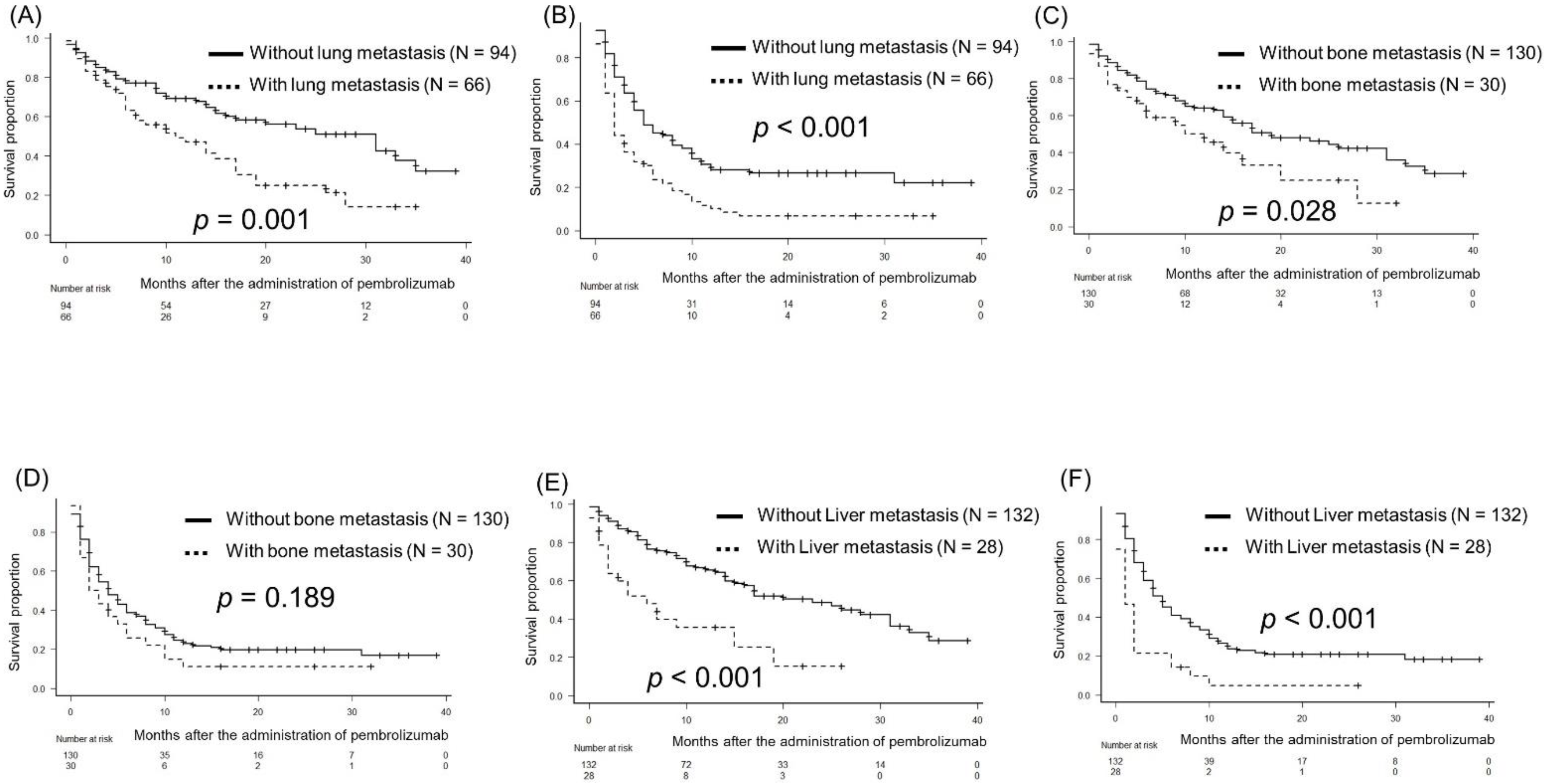
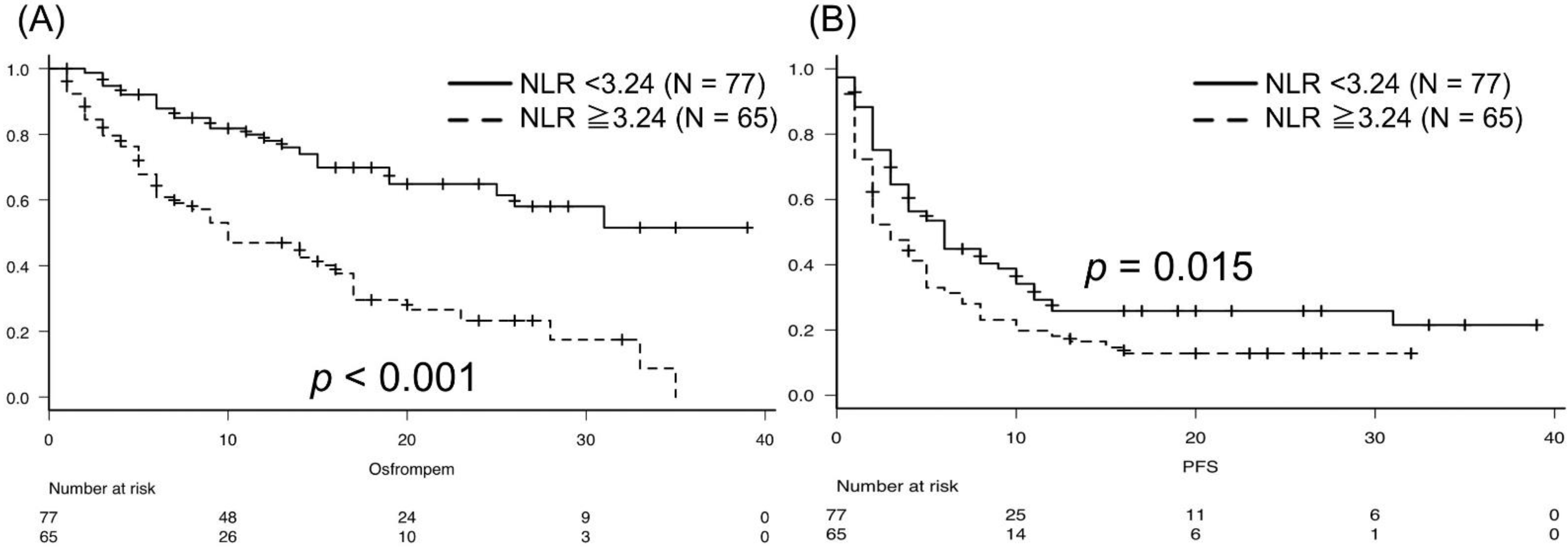
3.2. Oncological Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Deininger, S.; Törzsök, P.; Oswald, D.; Lusuardi, L. Current Systemic Treatment Options in Metastatic Urothelial Carcinoma after Progression on Checkpoint Inhibition Therapy-A Systemic Review Combined with Single-Group Meta-Analysis of Three Studies Testing Enfortumab Vedotin. Cancers 2021, 13, 3206. [Google Scholar] [CrossRef]
- Cathomas, R.; Lorch, A.; Bruins, H.M.; Compérat, E.M.; Cowan, N.C.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Hernández, V.; Espinós, E.L.; et al. The 2021 Updated European Association of Urology Guidelines on Metastatic Urothelial Carcinoma. Eur. Urol. 2022, 81, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Seront, E.; Machiels, J.P. Molecular biology and targeted therapies for urothelial carcinoma. Cancer Treat. Rev. 2015, 41, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Sonpavde, G.; Galsky, M.D.; Latini, D.; Chen, G.J. Cisplatin-ineligible and chemotherapy-ineligible patients should be the focus of new drug development in patients with advanced bladder cancer. Clin. Genitourin. Cancer 2014, 12, 71–73. [Google Scholar] [CrossRef]
- Plimack, E.R.; Bellmunt, J.; Gupta, S.; Berger, R.; Chow, L.Q.; Juco, J.; Lunceford, J.; Saraf, S.; Perini, R.F.; O’Donnell, P.H. Safety and activity of pembrolizumab in patients with locally advanced or metastatic urothelial cancer (KEYNOTE-012): A non-randomised, open-label, phase 1b study. Lancet Oncol. 2017, 18, 212–220. [Google Scholar] [CrossRef]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Fradet, Y.; Bellmunt, J.; Vaughn, D.J.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; Necchi, A.; et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: Results of >2 years of follow-up. Ann. Oncol. 2019, 30, 970–976. [Google Scholar] [CrossRef]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 244–258. [Google Scholar] [CrossRef]
- Bladder Cancer. NCCN guidelines® 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf (accessed on 2 May 2022).
- Ogihara, K.; Kikuchi, E.; Shigeta, K.; Okabe, T.; Hattori, S.; Yamashita, R.; Yoshimine, S.; Shirotake, S.; Nakazawa, R.; Matsumoto, K.; et al. The pretreatment neutrophil-to-lymphocyte ratio is a novel biomarker for predicting clinical responses to pembrolizumab in platinum-resistant metastatic urothelial carcinoma patients. Urol. Oncol. 2020, 38, 602.e1–602.e10. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Miyake, M.; Hori, S.; Ichikawa, K.; Omori, C.; Iemura, Y.; Owari, T.; Itami, Y.; Nakai, Y.; Anai, S.; et al. Clinical Impact of Sarcopenia and Inflammatory/Nutritional Markers in Patients with Unresectable Metastatic Urothelial Carcinoma Treated with Pembrolizumab. Diagnostics 2020, 10, 310. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, S.; Kawai, T.; Nakagawa, T.; Nakamura, Y.; Kamei, J.; Obinata, D.; Yamaguchi, K.; Kaneko, T.; Kakutani, S.; Tokunaga, M.; et al. Prognostic significance of the albumin-to-globulin ratio for advanced urothelial carcinoma treated with pembrolizumab: A multicenter retrospective study. Sci. Rep. 2021, 11, 15623. [Google Scholar] [CrossRef] [PubMed]
- Tomisaki, I.; Harada, M.; Tokutsu, K.; Minato, A.; Nagata, Y.; Kimuro, R.; Matsumoto, M.; Fujimoto, N. Impact of C-reactive Protein Flare Response in Patients with Advanced Urothelial Carcinoma Who Received Pembrolizumab. In Vivo 2021, 35, 3563–3568. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Tamura, D.; Jinnouchi, N.; Abe, M.; Ikarashi, D.; Matsuura, T.; Kato, R.; Maekawa, S.; Kato, Y.; Kanehira, M.; Takata, R.; et al. Prognostic outcomes and safety in patients treated with pembrolizumab for advanced urothelial carcinoma: Experience in real-world clinical practice. Int. J. Clin. Oncol. 2020, 25, 899–905. [Google Scholar] [CrossRef]
- Fukuokaya, W.; Kimura, T.; Yanagisawa, T.; Kimura, S.; Tsuzuki, S.; Koike, Y.; Iwamoto, Y.; Enei, Y.; Tanaka, M.; Urabe, F.; et al. Clinical benefit of continuing pembrolizumab treatment beyond progression in patients with metastatic urothelial carcinoma. Cancer Immunol. Immunother. 2022, 71, 229–236. [Google Scholar] [CrossRef]
- Paner, G.P.; Stadler, W.M.; Hansel, D.E.; Montironi, R.; Lin, D.W.; Amin, M.B. Updates in the eighth edition of the Tumor-Node-Metastasis staging classification for urologic cancers. Eur. Urol. 2018, 73, 560–569. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 13 May 2022).
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Perkins, N.J.; Schisterman, E.F. The inconsistency of “optimal” cutpoints obtained using two criteria based on the receiver operating characteristic curve. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef] [Green Version]
- Bellmunt, J.; Necchi, A.; De Wit, R.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent Durán, M.A.; Petrylak, D.P.; Choueiri, T.K.; Gerritsen, W.R.; et al. Pembrolizumab (pembro) versus investigator’s choice of paclitaxel, docetaxel, or vinflunine in recurrent, advanced urothelial cancer (UC): 5-year follow-up from the phase 3 KEYNOTE-045 trial. J. Clin. Oncol. 2021, 39, 4532. [Google Scholar] [CrossRef]
- Narita, T.; Hatakeyama, S.; Numakura, K.; Kobayashi, M.; Muto, Y.; Saito, M.; Narita, S.; Tanaka, T.; Noro, D.; Tokui, N.; et al. Comparison of pembrolizumab with conventional chemotherapy after first-line platinum-based chemotherapy for advanced urothelial carcinoma in real-world practice: A multicenter retrospective study. Int. J. Urol. 2021, 28, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Marchioni, M.; Primiceri, G.; Ingrosso, M.; Filograna, R.; Castellan, P.; De Francesco, P.; Schips, L. The Clinical Use of the Neutrophil to Lymphocyte Ratio (NLR) in Urothelial Cancer: A Systematic Review. Clin. Genitourin. Cancer 2016, 14, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Suh, K.J.; Kim, S.H.; Kim, Y.J.; Kim, M.; Keam, B.; Kim, T.M.; Kim, D.W.; Heo, D.S.; Lee, J.S. Post-treatment neutrophil-to-lymphocyte ratio at week 6 is prognostic in patients with advanced non-small cell lung cancers treated with anti-PD-1 antibody. Cancer Immunol. Immunother. 2018, 67, 459–470. [Google Scholar] [CrossRef]
- Lalani, A.A.; Xie, W.; Martini, D.J.; Steinharter, J.A.; Norton, C.K.; Krajewski, K.M.; Duquette, A.; Bossé, D.; Bellmunt, J.; Van Allen, E.M.; et al. Change in Neutrophil-to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma. J. Immunother. Cancer 2018, 6, 5. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Responder | Non-Responder | p |
|---|---|---|---|
| Number | 53 | 107 | |
| Age (year, median, IQR) | 72 (70–78) | 72 (68–78) | 0.707 |
| Sex (n, %) | 0.845 | ||
| Male | 41 (77.4) | 80 (74.8) | |
| Female | 12 (22.6) | 27 (25.2) | |
| BMI (kg/m2, median, IQR) | 22.2 (19.4–24.2) | 22.0 (19.5–24.5) | 0.988 |
| ECOG-PS | |||
| 0 | 38 (71.7) | 56 (52.3) | 0.026 |
| 1 | 12 (22.6) | 29 (27.1) | |
| 2 | 1 (1.9) | 16 (15.0) | |
| 3 | 2 (3.8) | 6 (5.6) | |
| Primary site (number, %) | 0.485 | ||
| Upper urinary tract | 19 (35.8) | 30 (28.0) | |
| Bladder | 26 (49.1) | 63 (58.9) | |
| Upper urinary tract and Bladder | 8 (15.1) | 14 (13.1) | |
| Location of metastases (number, %) | |||
| Lung | 13 (24.5) | 53 (49.5) | 0.004 |
| Liver | 5 (9.4) | 23 (21.5) | 0.077 |
| Bone | 5 (9.4) | 25 (23.4) | 0.051 |
| Lymph node | 36 (67.9) | 80 (74.8) | 0.452 |
| Smoking history (number, %) | |||
| Never | 18 (34.0) | 43 (40.2) | 0.239 |
| Current | 5 (9.4) | 18 (16.8) | |
| Former | 30 (56.6) | 46 (43.0) | |
| Definitive therapy for primary site (number, %) | 47 (88.7) | 83 (77.6) | 0.131 |
| Histological subtype (number, %) | 0.322 | ||
| Pure urothelial carcinoma | 43 (82.7) | 95 (88.8) | |
| Sarcomatoid variant | 3 (5.7) | 3 (2.8) | |
| other variants | 7 (13.2) | 9 (17.3) | |
| Follow-up period | 19 (12–26) | 6 (3–13) | <0.001 |
| (months, median, IQR) |
| Variables | Responder | Non-Responder | p |
|---|---|---|---|
| Number | 53 | 107 | |
| Before the administration of pembrolizumab | |||
| CRP (mg/dL, median, IQR) | 0.20 (0.10–1.40) | 1.14 (0.23–2.77) | 0.002 |
| Albumin (g/dL, median, IQR) | 3.90 (3.50–4.12) | 3.60 (3.20–3.95) | 0.006 |
| Hemoglobin (g/dL, IQR) | 11.10 (9.20- 12.60) | 10.50 (9.12–12.00) | 0.133 |
| NLR (median, IQR) | 2.94 (2.07–4.47) | 2.96 (2.08–4.96) | 0.843 |
| After two courses of pembrolizumab | |||
| CRP (mg/dL, IQR) | 0.14 (0.07–0.46) | 1.05 (0.42–3.83) | <0.001 |
| Albumin (g/dL, IQR) | 3.90 (3.68–4.23) | 3.60 (3.23–3.98) | <0.001 |
| Hemoglobin (g/dL, IQR) | 11.90 (10.88- 13.40) | 10.80 (9.50–12.30) | 0.003 |
| NLR (median, IQR) | 2.13 (1.60–3.50) | 3.30 (2.50–5.80) | <0.001 |
| Best of response | ||||||
| Variables | CR | PR | SD | PD | p | |
| Number | 23 | 30 | 33 | 74 | ||
| Before pembrolizumab administration | ||||||
| CRP, <0.63 mg/dL | 19 (82.6) | 18 (60.0) | 17 (51.5) | 26 (35.1) | 0.001 | |
| CRP, ≥0.63 mg/dL | 4 (17.4) | 12 (40.0) | 16 (48.5) | 48 (64.9) | ||
| Albumin, <3.7 g/dL | 6 (26.1) | 11 (37.9) | 16 (48.5) | 44 (59.5) | 0.024 | |
| Albumin, ≥3.7 g/dL | 17 (73.9) | 18 (62.1) | 17 (51.5) | 30 (40.5) | ||
| Hemoglobin, <10.6 g/dL | 6 (26.1) | 14 (46.7) | 16 (48.5) | 40 (54.8) | 0.122 | |
| Hemoglobin, ≥10.6 g/dL | 17 (73.9) | 16 (53.3) | 17 (51.5) | 33 (45.2) | ||
| NLR, <4.89 | 19 (82.6) | 21 (70.0) | 28 (84.8) | 51 (68.9) | 0.243 | |
| NLR, ≥4.89 | 4 (17.4) | 9 (30.0) | 5 (15.2) | 23 (31.1) | ||
| After pembrolizumab administration | ||||||
| CRP, <0.67 mg/dL | 20 (90.9) | 23 (79.3) | 18 (58.1) | 15 (25.0) | <0.001 | |
| CRP, ≥0.67 mg/dL | 2 (9.1) | 6 (20.7) | 13 (41.9) | 45 (75.0) | ||
| Albumin, <3.7 g/dL | 5 (21.7) | 8 (27.6) | 13 (40.6) | 40 (64.5) | <0.001 | |
| Albumin, ≥3.7 g/dL | 18 (78.3) | 21 (72.4) | 19 (59.4) | 22 (35.5) | ||
| Hemoglobin, <10.0 g/dL | 0 (0) | 6 (20.7) | 12 (37.5) | 22 (36.1) | 0.004 | |
| Hemoglobin, ≥10.0 g/dL | 23 (100.0) | 23 (79.3) | 20 (62.5) | 39 (63.9) | ||
| NLR, <3.24 | 18 (81.8) | 19 (65.5) | 16 (51.6) | 24 (40.0) | 0.004 | |
| NLR, ≥3.24 | 4 (18.2) | 10 (34.5) | 15 (48.4) | 36 (60.0) | ||
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age, ≥75 vs. <75 | 0.91 | 0.57–1.44 | 0.705 | |||
| Sex, Female vs. Male | 0.87 | 0.51–1.48 | 0.610 | |||
| ECOG-PS, ≥2 vs. ≤1 | 1.37 | 1.07–1.75 | 0.013 | 1.88 | 0.95–3.72 | 0.068 |
| BMI, <21.9 vs. ≥21.9 | 0.82 | 0.53–1.27 | 0.378 | |||
| Smoking history, yes vs. no | 0.74 | 0.47–1.16 | 0.201 | |||
| Lung metastasis, yes vs. no | 1.98 | 1.28–3.07 | 0.002 | 2.02 | 1.15–3.55 | 0.014 |
| Liver metastasis, yes vs. no | 2.56 | 1.55–4.24 | <0.001 | 2.65 | 1.35–5.17 | 0.004 |
| Bone metastasis, yes vs. no | 1.82 | 1.1–3.03 | 0.021 | 1.11 | 0.61–2.00 | 0.720 |
| Lymph node metastasis, yes vs. no | 0.95 | 0.6–1.51 | 0.830 | |||
| Surgery of the primary site, yes vs. no | 0.63 | 0.37–1.07 | 0.084 | |||
| Radiation therapy of the primary site, yes vs. no | 1.17 | 0.43–3.21 | 0.760 | |||
| Albumin, ≥3.7 vs. <3.7 | 0.28 | 0.23–0.56 | <0.001 | 0.59 | 0.30–1.15 | 0.126 |
| CRP, ≥0.67 vs. <0.67 | 1.08 | 1.04–1.11 | <0.001 | 2.28 | 1.13–4.57 | 0.020 |
| Hemoglobin, ≥10.0 vs. <10.0 | 0.29 | 0.18–0.48 | <0.001 | 1.08 | 0.58–2.02 | 0.790 |
| NLR, ≥3.24 vs. <3.24 | 3.21 | 1.94–5.33 | <0.001 | 2.82 | 1.50–5.31 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomioka-Inagawa, R.; Nakane, K.; Enomoto, T.; Tomioka, M.; Taniguchi, T.; Ishida, T.; Ozawa, K.; Takagi, K.; Ito, H.; Takeuchi, S.; et al. The Impact of Neutrophil-to-Lymphocyte Ratio after Two Courses of Pembrolizumab for Oncological Outcomes in Patients with Metastatic Urothelial Carcinoma. Biomedicines 2022, 10, 1609. https://doi.org/10.3390/biomedicines10071609
Tomioka-Inagawa R, Nakane K, Enomoto T, Tomioka M, Taniguchi T, Ishida T, Ozawa K, Takagi K, Ito H, Takeuchi S, et al. The Impact of Neutrophil-to-Lymphocyte Ratio after Two Courses of Pembrolizumab for Oncological Outcomes in Patients with Metastatic Urothelial Carcinoma. Biomedicines. 2022; 10(7):1609. https://doi.org/10.3390/biomedicines10071609
Chicago/Turabian StyleTomioka-Inagawa, Risa, Keita Nakane, Torai Enomoto, Masayuki Tomioka, Tomoki Taniguchi, Takashi Ishida, Kaori Ozawa, Kimiaki Takagi, Hiroki Ito, Shinichi Takeuchi, and et al. 2022. "The Impact of Neutrophil-to-Lymphocyte Ratio after Two Courses of Pembrolizumab for Oncological Outcomes in Patients with Metastatic Urothelial Carcinoma" Biomedicines 10, no. 7: 1609. https://doi.org/10.3390/biomedicines10071609