
The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
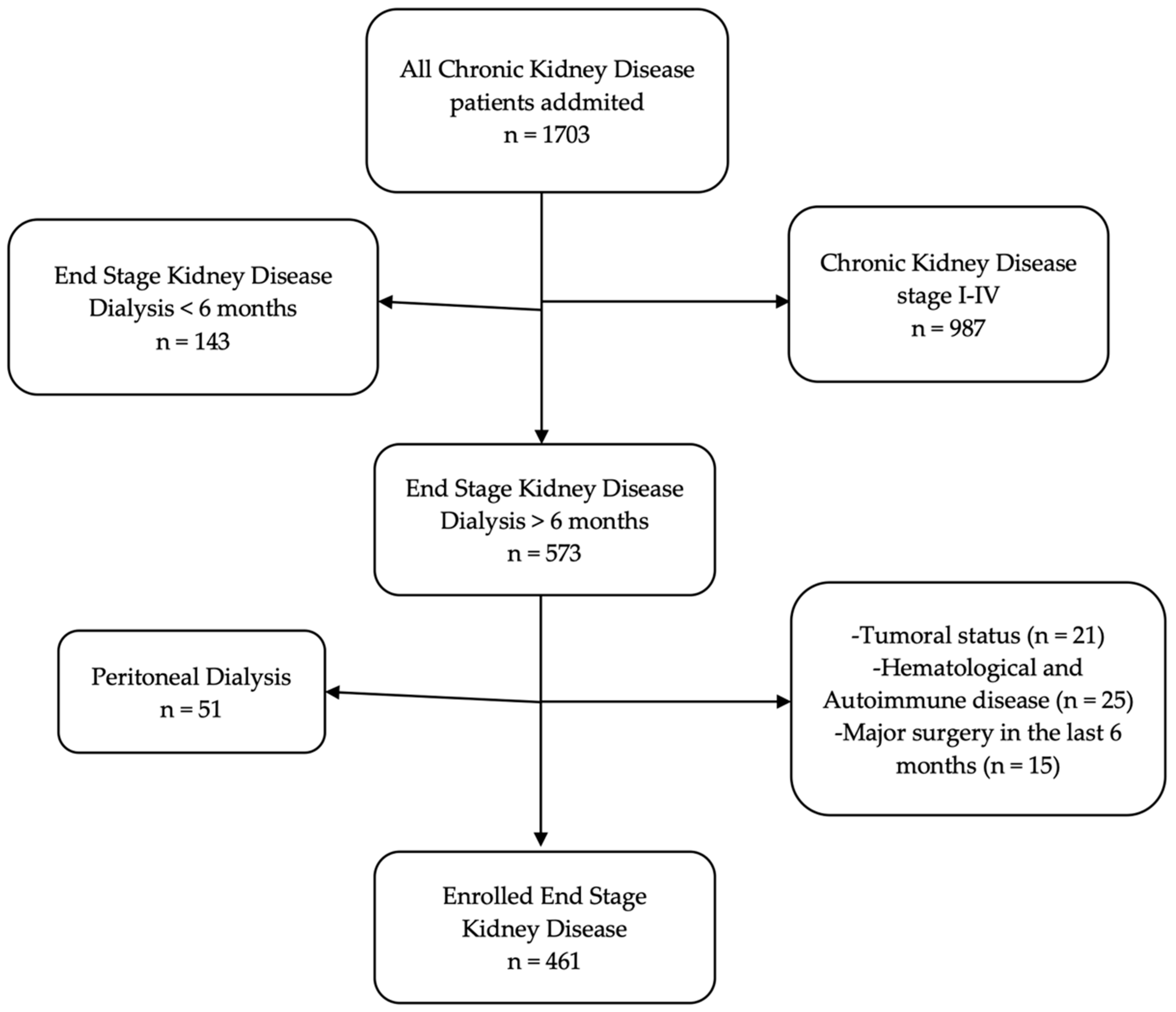
2.1. Study Design
2.2. Data Collection
2.3. Study Outcomes
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eknoyan, G.; Lameire, N.; Barsoum, R.; Eckardt, K.-U.; Levin, A.; Levin, N.; Locatelli, F.; Macleod, A.; Vanholder, R.; Walker, R.; et al. The Burden of Kidney Disease: Improving Global Outcomes. Kidney Int. 2004, 66, 1310–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 15 January 2022).
- Boenink, R.; Astley, M.E.; Huijben, J.A.; Stel, V.S.; Kerschbaum, J.; Rosenberg-Ots, M.; Åsberg, A.A.; Lopot, F.; Golan, E.; Castro de la Nuez, P.; et al. The ERA Registry Annual Report 2019: Summary and Age Comparisons. Clin. Kidney J. 2021, 15, 452–472. [Google Scholar] [CrossRef] [PubMed]
- Raportul Registrului Renal Român 2019–2020. Available online: http://registrulrenal.ro/resurse_statistica/Raport_RRR_2019_2020.pdf (accessed on 15 January 2022).
- Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Arbănași, E.M.; Kovács, I.; Horváth, E.; Suciu, B.A.; Hosu, I.; Russu, E. Uncommon Surgical Management by AVF between the Great Saphenous Vein and Anterior Tibial Artery for Old Radiocephalic AVF Failure. Life 2022, 12, 529. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Am. J. Kidney Dis. 2002, 39, S1–S266.
- Wen, C.P.; Cheng, T.Y.D.; Tsai, M.K.; Chang, Y.C.; Chan, H.T.; Tsai, S.P.; Chiang, P.H.; Hsu, C.C.; Sung, P.K.; Hsu, Y.H.; et al. All-Cause Mortality Attributable to Chronic Kidney Disease: A Prospective Cohort Study Based on 462,293 Adults in Taiwan. Lancet 2008, 371, 2173–2182. [Google Scholar] [CrossRef]
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.F.; Levy, D. Predictors of New-Onset Kidney Disease in a Community-Based Population. JAMA 2004, 291, 844–850. [Google Scholar] [CrossRef] [Green Version]
- Xu, R.; Zhang, L.-X.; Zhang, P.-H.; Wang, F.; Zuo, L.; Wang, H.-Y. Gender Differences in Age-Related Decline in Glomerular Filtration Rates in Healthy People and Chronic Kidney Disease Patients. BMC Nephrol. 2010, 11, 20. [Google Scholar] [CrossRef] [Green Version]
- Imig, J.D.; Ryan, M.J. Immune and Inflammatory Role in Renal Disease. Compr. Physiol. 2013, 3, 957–976. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Sacks, F.; Pfeffer, M.; Jhangri, G.S.; Curhan, G. Cholesterol and Recurrent Events (CARE) Trial Investigators Biomarkers of Inflammation and Progression of Chronic Kidney Disease. Kidney Int. 2005, 68, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.-C.; Hung, C.-C.; Kuo, M.-C.; Tsai, J.-C.; Yeh, S.-M.; Hwang, S.-J.; Chiu, Y.-W.; Kuo, H.-T.; Chang, J.-M.; Chen, H.-C. Association of HsCRP, White Blood Cell Count and Ferritin with Renal Outcome in Chronic Kidney Disease Patients. PLoS ONE 2012, 7, e52775. [Google Scholar] [CrossRef] [Green Version]
- Tamhane, U.U.; Aneja, S.; Montgomery, D.; Rogers, E.-K.; Eagle, K.A.; Gurm, H.S. Association between Admission Neutrophil to Lymphocyte Ratio and Outcomes in Patients with Acute Coronary Syndrome. Am. J. Cardiol. 2008, 102, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Erturk, M.; Cakmak, H.A.; Surgit, O.; Celik, O.; Aksu, H.U.; Akgul, O.; Gurdogan, M.; Bulut, U.; Ozalp, B.; Akbay, E.; et al. Predictive Value of Elevated Neutrophil to Lymphocyte Ratio for Long-Term Cardiovascular Mortality in Peripheral Arterial Occlusive Disease. J. Cardiol. 2014, 64, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-S.; Seo, K.-W.; Choi, B.-J.; Choi, S.-Y.; Yoon, M.-H.; Hwang, G.-S.; Tahk, S.-J.; Shin, J.-H. Importance of Prognostic Value of Neutrophil to Lymphocyte Ratio in Patients with ST-Elevation Myocardial Infarction. Medicine 2018, 97, e13471. [Google Scholar] [CrossRef] [PubMed]
- Bhat, T.; Teli, S.; Rijal, J.; Bhat, H.; Raza, M.; Khoueiry, G.; Meghani, M.; Akhtar, M.; Costantino, T. Neutrophil to Lymphocyte Ratio and Cardiovascular Diseases: A Review. Expert Rev. Cardiovasc. Ther. 2013, 11, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Garza, E.; Jerjes-Sanchez, C.; Navarrete, A.; Joya-Harrison, J.; Rodriguez, D. Venous Thromboembolism: Thrombosis, Inflammation, and Immunothrombosis for Clinicians. J. Thromb. Thrombolysis 2017, 44, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Galliazzo, S.; Nigro, O.; Bertù, L.; Guasti, L.; Grandi, A.M.; Ageno, W.; Dentali, F. Prognostic Role of Neutrophils to Lymphocytes Ratio in Patients with Acute Pulmonary Embolism: A Systematic Review and Meta-Analysis of the Literature. Intern. Emerg. Med. 2018, 13, 603–608. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Solid Tumors: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Li, M.-X.; Liu, X.-M.; Zhang, X.-F.; Zhang, J.-F.; Wang, W.-L.; Zhu, Y.; Dong, J.; Cheng, J.-W.; Liu, Z.-W.; Ma, L.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Colorectal Cancer: A Systematic Review and Meta-Analysis. Int. J. Cancer 2014, 134, 2403–2413. [Google Scholar] [CrossRef]
- Ethier, J.-L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Breast Cancer: A Systematic Review and Meta-Analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.-T.; Yang, Y.; Xu, S.; Zhang, X.-P.; Wang, H.-E.; Zhang, H.; Wang, Z.-K.; Yuan, Z.; Duan, G.-C. Prognostic Role of Neutrophil to Lymphocyte Ratio in Lung Cancers: A Meta-Analysis Including 7054 Patients. OncoTargets Ther. 2015, 8, 2731–2738. [Google Scholar] [CrossRef] [Green Version]
- Takenaka, Y.; Oya, R.; Kitamiura, T.; Ashida, N.; Shimizu, K.; Takemura, K.; Yamamoto, Y.; Uno, A. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Head and Neck Cancer: A Meta-Analysis. Head Neck 2018, 40, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Xiao, Y.; Li, F.; Qi, S.; Yin, Z.; Gao, J. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Prostate Cancer. Medicine 2016, 95, e2544. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhu, L.; Yang, Y.; Long, Y.; Li, X.; Wang, Y. Prognostic Role of Neutrophil to Lymphocyte Ratio in Ovarian Cancer: A Meta-Analysis. Technol. Cancer Res. Treat. 2018, 17, 1533033818791500. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ren, Q.; Song, Y.; He, M.; Zeng, Y.; Liu, Z.; Xu, J. Prognostic Role of Neutrophil–Lymphocyte Ratio in Patients with Acute Ischemic Stroke. Medicine 2017, 96, e8624. [Google Scholar] [CrossRef] [PubMed]
- Russu, E.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Voidăzan, S.; Arbănași, E.M.; Coșarcă, C.M. The Predictive Role of NLR and PLR in Outcome and Patency of Lower Limb Revascularization in Patients with Femoropopliteal Disease. J. Clin. Med. 2022, 11, 2620. [Google Scholar] [CrossRef]
- Szor, D.J.; Dias, A.R.; Pereira, M.A.; Ramos, M.F.K.P.; Zilberstein, B.; Cecconello, I.; Ribeiro-Júnior, U. Prognostic Role of Neutrophil/Lymphocyte Ratio in Resected Gastric Cancer: A Systematic Review and Meta-Analysis. Clinics 2018, 73, e360. [Google Scholar] [CrossRef]
- Yuan, Q.; Wang, J.; Peng, Z.; Zhou, Q.; Xiao, X.; Xie, Y.; Wang, W.; Huang, L.; Tang, W.; Sun, D.; et al. Neutrophil-to-Lymphocyte Ratio and Incident End-Stage Renal Disease in Chinese Patients with Chronic Kidney Disease: Results from the Chinese Cohort Study of Chronic Kidney Disease (C-STRIDE). J. Transl. Med. 2019, 17, 86. [Google Scholar] [CrossRef] [Green Version]
- MacIsaac, R.J.; Ekinci, E.I.; Jerums, G. Markers of and Risk Factors for the Development and Progression of Diabetic Kidney Disease. Am. J. Kidney Dis. 2014, 63, S39–S62. [Google Scholar] [CrossRef]
- Soehnlein, O. Multiple Roles for Neutrophils in Atherosclerosis. Circ. Res. 2012, 110, 875–888. [Google Scholar] [CrossRef] [Green Version]
- Hotchkiss, R.S.; Karl, I.E. The Pathophysiology and Treatment of Sepsis. N. Engl. J. Med. 2003, 348, 138–150. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Fu, Z.; Huang, W.; Huang, K. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Sepsis: A Meta-Analysis. Am. J. Emerg. Med. 2020, 38, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Balta, S.; Celik, T.; Mikhailidis, D.P.; Ozturk, C.; Demirkol, S.; Aparci, M.; Iyisoy, A. The Relation Between Atherosclerosis and the Neutrophil–Lymphocyte Ratio. Clin. Appl. Thromb. 2016, 22, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Cognasse, F.; Garraud, O.; Pozzetto, B.; Laradi, S.; Hamzeh-Cognasse, H. How Can Non-Nucleated Platelets Be so Smart? J. Thromb. Haemost. 2016, 14, 794–796. [Google Scholar] [CrossRef]
- Sut, C.; Tariket, S.; Aubron, C.; Aloui, C.; Hamzeh-Cognasse, H.; Berthelot, P.; Laradi, S.; Greinacher, A.; Garraud, O.; Cognasse, F. The Non-Hemostatic Aspects of Transfused Platelets. Front. Med. 2018, 5, 42. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-J.; Davis, R.P.; Jenne, C.N. Platelets as Modulators of Inflammation. Semin. Thromb. Hemost. 2018, 44, 91–101. [Google Scholar] [CrossRef]
- Reddan, D.N.; Klassen, P.S.; Szczech, L.A.; Coladonato, J.A.; O’Shea, S.; Owen, W.F.; Lowrie, E.G. White Blood Cells as a Novel Mortality Predictor in Haemodialysis Patients. Nephrol. Dial. Transplant. 2003, 18, 1167–1173. [Google Scholar] [CrossRef]
- Kim, K.M.; Oh, H.J.; Choi, H.Y.; Lee, H.; Ryu, D.-R. Impact of Chronic Kidney Disease on Mortality: A Nationwide Cohort Study. Kidney Res. Clin. Pract. 2019, 38, 382–390. [Google Scholar] [CrossRef] [Green Version]
- Altunoren, O.; Akkus, G.; Sezal, D.T.; Ciftcioglu, M.; Guzel, F.B.; Isiktas, S.; Torun, G.I.; Uyan, M.; Sokmen, M.F.; Sevim, H.A.; et al. Does Neutrophyl to Lymphocyte Ratio Really Predict Chronic Kidney Disease Progression? Int. Urol. Nephrol. 2019, 51, 129–137. [Google Scholar] [CrossRef]
- Solak, Y.; Yilmaz, M.I.; Sonmez, A.; Saglam, M.; Cakir, E.; Unal, H.U.; Gok, M.; Caglar, K.; Oguz, Y.; Yenicesu, M.; et al. Neutrophil to Lymphocyte Ratio Independently Predicts Cardiovascular Events in Patients with Chronic Kidney Disease. Clin. Exp. Nephrol. 2013, 17, 532–540. [Google Scholar] [CrossRef]
- Kato, S.; Abe, T.; Lindholm, B.; Maruyama, S. Neutrophil/Lymphocyte Ratio: A Promising Prognostic Marker in Patients with Chronic Kidney Disease. Inflamm. Cell Signal. 2015, 2, 132–137. [Google Scholar]
- Woziwodzka, K.; Dziewierz, A.; Pawica, M.; Panek, A.; Krzanowski, M.; Gołasa, P.; Latacz, P.; Burkat, M.; Kuźniewski, M.; Krzanowska, K. Neutrophil-to-Lymphocyte Ratio Predicts Long-Term All-Cause Mortality in Patients with Chronic Kidney Disease Stage 5. Folia Med. Cracov. 2019, 59, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, X.; Wang, S.; Li, H. High Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Are Associated with Poor Survival in Patients with Hemodialysis. BioMed Res. Int. 2021, 2021, e9958081. [Google Scholar] [CrossRef] [PubMed]
- Umeres-Francia, G.; Rojas-Fernández, M.; Añazco, P.H.; Benites-Zapata, V. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as a Risk Factor for Mortality in Peruvian Adults with Chronic Kidney Disease. Authorea 2021. [Google Scholar] [CrossRef]
- Duan, S.; Sun, L.; Zhang, C.; Wu, L.; Nie, G.; Huang, Z.; Xing, C.; Zhang, B.; Yuan, Y. Association of Platelet-to-Lymphocyte Ratio with Kidney Clinicopathologic Features and Renal Outcomes in Patients with Diabetic Kidney Disease. Int. Immunopharmacol. 2021, 93, 107413. [Google Scholar] [CrossRef] [PubMed]
- Brito, G.M.C.; Fontenele, A.M.M.; Carneiro, E.C.R.L.; Nogueira, I.A.L.; Cavalcante, T.B.; Vale, A.A.M.; Monteiro, S.C.M.; Salgado Filho, N. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in Nondialysis Chronic Kidney Patients. Int. J. Inflamm. 2021, 2021, e6678960. [Google Scholar] [CrossRef] [PubMed]
- Catabay, C.; Obi, Y.; Streja, E.; Soohoo, M.; Park, C.; Rhee, C.M.; Kovesdy, C.P.; Hamano, T.; Kalantar-Zadeh, K. Lymphocyte Cell Ratios and Mortality among Incident Hemodialysis Patients. Am. J. Nephrol. 2017, 46, 408–416. [Google Scholar] [CrossRef]
- Yoshitomi, R.; Nakayama, M.; Sakoh, T.; Fukui, A.; Katafuchi, E.; Seki, M.; Tsuda, S.; Nakano, T.; Tsuruya, K.; Kitazono, T. High Neutrophil/Lymphocyte Ratio Is Associated with Poor Renal Outcomes in Japanese Patients with Chronic Kidney Disease. Ren. Fail. 2019, 41, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Neuen, B.L.; Leather, N.; Greenwood, A.M.; Gunnarsson, R.; Cho, Y.; Mantha, M.L. Neutrophil–Lymphocyte Ratio Predicts Cardiovascular and All-Cause Mortality in Hemodialysis Patients. Ren. Fail. 2016, 38, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Wang, S.; Zhang, G.; Xiong, R.; Li, H. High Neutrophil-to-Lymphocyte Ratio Is a Significant Predictor of Cardiovascular and All-Cause Mortality in Patients Undergoing Peritoneal Dialysis. Kidney Blood Press. Res. 2018, 43, 490–499. [Google Scholar] [CrossRef]
- Zhang, L.; Nie, Y.; Guo, M.; Wang, L.; Shi, Y.; Jiang, X.; Ding, X.; Xu, X.; Ji, J. Neutrophil to Lymphocyte Ratio as a Predictor of Long-Term Outcome in Peritoneal Dialysis Patients: A 5-Year Cohort Study. Blood Purif. 2021, 50, 772–778. [Google Scholar] [CrossRef]
- Erdem, E.; Kaya, C.; Karataş, A.; Dilek, M.; Akpolat, T. Neutrophil to Lymphocyte Ratio in Predicting Short-Term Mortality in Hemodialysis Patients. J. Exp. Clin. Med. 2013, 30, 129–132. [Google Scholar] [CrossRef] [Green Version]
- An, X.; Mao, H.-P.; Wei, X.; Chen, J.-H.; Yang, X.; Li, Z.-B.; Yu, X.-Q.; Li, Z.-J. Elevated Neutrophil to Lymphocyte Ratio Predicts Overall and Cardiovascular Mortality in Maintenance Peritoneal Dialysis Patients. Int. Urol. Nephrol. 2012, 44, 1521–1528. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Li, G.; Li, S.; Gong, Z.; Liu, J.; Song, S. Neutrophil-to-lymphocyte Ratio and Red Blood Cell Distribution Width-to-platelet Ratio Predict Cardiovascular Events in Hemodialysis Patients. Exp. Ther. Med. 2020, 20, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Xiang, F.; Chen, R.; Cao, X.; Shen, B.; Liu, Z.; Tan, X.; Ding, X.; Zou, J. Monocyte/Lymphocyte Ratio as a Better Predictor of Cardiovascular and All-Cause Mortality in Hemodialysis Patients: A Prospective Cohort Study. Hemodial. Int. Int. Symp. Home Hemodial. 2018, 22, 82–92. [Google Scholar] [CrossRef]
- Yaprak, M.; Turan, M.N.; Dayanan, R.; Akın, S.; Değirmen, E.; Yıldırım, M.; Turgut, F. Platelet-to-Lymphocyte Ratio Predicts Mortality Better than Neutrophil-to-Lymphocyte Ratio in Hemodialysis Patients. Int. Urol. Nephrol. 2016, 48, 1343–1348. [Google Scholar] [CrossRef]
- Ao, G.; Wang, Y.; Qi, X.; Wang, F.; Wen, H. Association of Neutrophil-to-Lymphocyte Ratio and Risk of Cardiovascular or All-Cause Mortality in Chronic Kidney Disease: A Meta-Analysis. Clin. Exp. Nephrol. 2021, 25, 157–165. [Google Scholar] [CrossRef]
- Zhao, W.-M.; Tao, S.-M.; Liu, G.-L. Neutrophil-to-Lymphocyte Ratio in Relation to the Risk of All-Cause Mortality and Cardiovascular Events in Patients with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Ren. Fail. 2020, 42, 1059–1066. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | All Patients n = 461 |
|---|---|
| Age mean ± SD (min–max) | 64.36 ± 12.14 (19–98) |
| Male sex no. (%) | 279 (60.52%) |
| Comorbidities and Risk factors | |
| AH, no. (%) | 388 (84.16%) |
| AF, no. (%) | 95 (20.6%) |
| CHF, no. (%) | 213 (46.2%) |
| IHD, no. (%) | 303 (65.72%) |
| MI, no. (%) | 97 (21.04%) |
| T2D, no. (%) | 164 (35.57%) |
| COPD, no. (%) | 133 (28.85%) |
| CVA, no. (%) | 117 (25.37%) |
| PAD, no. (%) | 143 (31.01%) |
| Tobacco, no. (%) | 199 (43.16%) |
| Obesity, no. (%) | 139 (30.15%) |
| Dyslipidemia, no. (%) | 217 (47.07%) |
| Type of dialysis access | |
| AVF, no. (%) | 191 (41.43%) |
| CVC, no. (%) | 270 (58.56%) |
| outcomes | |
| Hospital stay, day median [Q1–Q3] | 6 [4–11] |
| Dialysis session on patient, no. median [Q1–Q3] | 4 [2–6] |
| 30-day mortality, no. (%) | 69 (14.96%) |
| Survivors n = 392 | Deaths n = 69 | p Value (OR; CI 95%) | |
|---|---|---|---|
| Age mean ± SD (min–max) | 63.58 ± 12.04 (19–89) | 68.82 ± 11.83 (46–98) | 0.001 # |
| Male sex no. (%) | 234 (59.69%) | 45 (65.21%) | 0.38 ¥ (0.79; 0.46–1.34) |
| Comorbidities and Risk factors | |||
| AH, no. (%) | 341 (86.98%) | 47 (68.11%) | 0.0001 ¥ (3.12; 1.74–5.62) |
| AF, no. (%) | 71 (18.11%) | 24 (34.78%) | 0.002 ¥ (0.41; 0.23–0.72) |
| CHF, no. (%) | 176 (44.89%) | 37 (53.62%) | 0.18 ¥ (0.7; 0.42–1.17) |
| IHD, no. (%) | 261 (66.58%) | 42 (60.86%) | 0.35 ¥ (1.28; 0.75–2.16) |
| MI, no. (%) | 69 (17.6%) | 28 (40.57%) | <0.0001 ¥ (0.31; 0.18–0.54) |
| T2D, no. (%) | 144 (36.73%) | 20 (28.98%) | 0.21 ¥ (0.81; 0.7–2.48) |
| COPD, no. (%) | 109 (27.8%) | 24 (34.78%) | 0.23 ¥ (0.72; 0.41–1.24) |
| CVA, no. (%) | 92 (23.46%) | 25 (36.23%) | 0.02 ¥ (0.53; 0.31–0.92) |
| PAD, no. (%) | 118 (30.1%) | 25 (36.23%) | 0.31 ¥ (0.75; 0.44–1.29) |
| Tobacco, no. (%) | 153 (39.03%) | 46 (66.67%) | <0.0001 ¥ (0.32; 0.18–0.54) |
| Obesity, no. (%) | 119 (30.35%) | 20 (28.98%) | 0.81 ¥ (1.06; 0.6–1.87) |
| Dyslipidemia, no. (%) | 183 (46.68%) | 35 (49.27%) | 0.69 ¥ (0.9; 0.54–1.5) |
| Type of dialysis access | |||
| AVF, no. (%) | 177 (45.15%) | 14 (20.28%) | 0.01 ¥ (0.46; 0.25–0.87) |
| CVC, no. (%) | 215 (54.84%) | 55 (79.71%) | |
| Survivors n = 392 | Deaths n = 69 | p Value § | |
|---|---|---|---|
| Haemoglobin g/dL median [Q1–Q3] | 9.81 [8.41–11.3] | 9.6 [8.2–11.3] | 0.28 |
| Haematocrit % median [Q1–Q3] | 30.76 [26.2–34.4] | 31.19 [25.3–35.72] | 0.41 |
| Neutrophils ×10³/uL median [Q1–Q3] | 6.45 [4.57–8.25] | 11.29 [8.49–14.8] | <0.0001 |
| Lymphocytes ×10³/uL median [Q1–Q3] | 1.31 [0.94–1.83] | 0.62 [0.4–1.0] | <0.0001 |
| Monocyte ×10³/uL median [Q1–Q3] | 0.62 [0.45–0.88] | 0.64 [0.46–1.0] | 0.24 |
| PLT ×10³/uL median [Q1–Q3] | 216.95 [170.17–272.0] | 172 [125–235] | <0.0001 |
| Glucose mg/dL median [Q1–Q3] | 112 [95.0–143.25] | 116 [93–165] | 0.23 |
| BUN mg/dL median [Q1–Q3] | 137.5 [99.45–191.9] | 141.3 [98.95–220.1] | 0.2 |
| Creatinine mg/dL median [Q1–Q3] | 7.45 [5.87–9.63] | 7.41 [6.29–9.74] | 0.29 |
| Potassium mmol/L median [Q1–Q3] | 5.2 [4.65–6.06] | 5.1 [4.5–6.48] | 0.35 |
| NLR median [Q1–Q3] | 4.63 [2.87–7.89] | 17.91 [11.53–24.54] | <0.0001 |
| MLR median [Q1–Q3] | 0.45 [0.32–0.68] | 1 [0.7–1.63] | <0.0001 |
| PLR median [Q1–Q3] | 163.57 [115.22–238.23] | 273.25 [161.87–411.11] | <0.0001 |
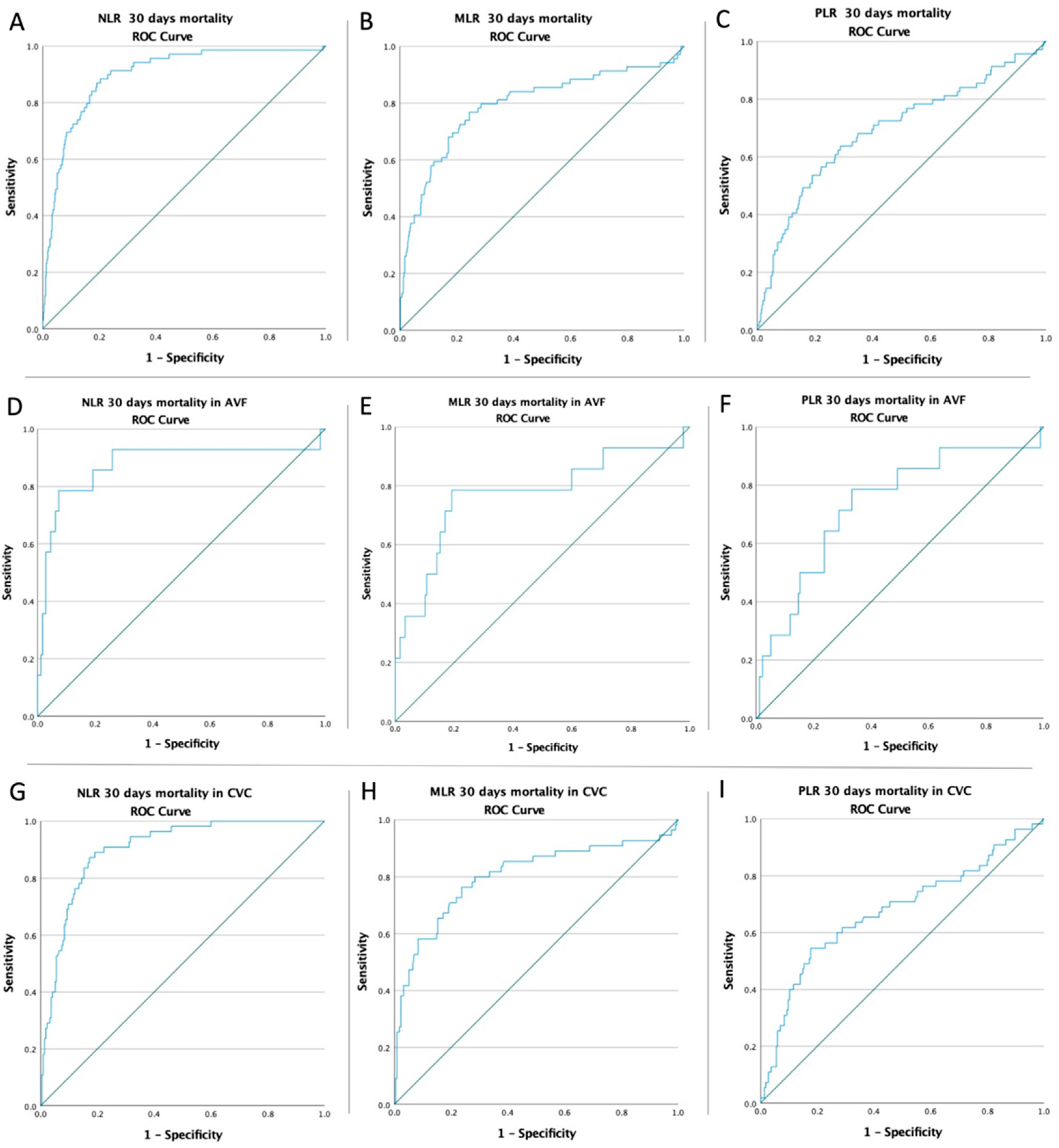
| Variable | Cut-Off | AUC | Std. Error | 95% CI | Sensitivity | Specificity | p Value |
|---|---|---|---|---|---|---|---|
| Mortality rate in all patients | |||||||
| NLR | 8.19 | 0.897 | 0.020 | 0.857–0.937 | 91.3% | 76% | <0.0001 |
| MLR | 0.63 | 0.792 | 0.035 | 0.724–0.860 | 79.7% | 71.4% | <0.0001 |
| PLR | 199.05 | 0.692 | 0.038 | 0.617–0.767 | 68.1% | 65.1% | <0.0001 |
| Mortality rate in AVF patients | |||||||
| NLR | 13.78 | 0.875 | 0.067 | 0.743–1.000 | 78.6% | 92.7% | <0.0001 |
| MLR | 0.809 | 0.772 | 0.080 | 0.615–0.928 | 78.6% | 80.8% | 0.001 |
| PLR | 198.19 | 0.734 | 0.074 | 0.589–0.879 | 78.6% | 67% | 0.004 |
| Mortality rate in CVC patients | |||||||
| NLR | 8.07 | 0.902 | 0.020 | 0.862–0.942 | 90.9% | 77.7% | <0.0001 |
| MLR | 0.69 | 0.802 | 0.039 | 0.725–0.879 | 76.4% | 76.3% | <0.0001 |
| PLR | 224.46 | 0.675 | 0.045 | 0.587–0.763 | 61.8% | 71.2% | <0.0001 |
| Low-NLR n = 304 | High-NLR n = 157 | p Value | |
|---|---|---|---|
| Hospital stay, day median [Q1–Q3] | 5 [4–9] | 10 [6–14] | <0.0001 § |
| Dialysis session on patient, no. median [Q1–Q3] | 2 [3–5] | 5 [3–7] | <0.0001 § |
| 30-day mortality, no. (%) | 6 (1.97%) | 63 (40.12%) | <0.0001 ¥ |
| low-MLR n = 291 | high-MLR n = 170 | p value | |
| Hospital stay, day median [Q1–Q3] | 5 [3.5–9] | 8 [5–12] | <0.0001 § |
| Dialysis session on patient, no. median [Q1–Q3] | 3 [2–5] | 4 [3–7] | <0.0001 § |
| 30-day mortality, no. (%) | 14 (4.81%) | 55 (32.35%) | <0.0001 ¥ |
| low-PLR n = 277 | high-PLR n = 184 | p value | |
| Hospital stay, day median [Q1–Q3] | 5 [3–9] | 9 [5–12] | <0.0001 § |
| Dialysis session on patient, no. median [Q1–Q3] | 3 [2–5] | 5 [3–7] | <0.0001 § |
| 30-day mortality, no. (%) | 22 (7.94%) | 47 (25.54%) | <0.0001 ¥ |
| 30 Days Mortality | |||
|---|---|---|---|
| OR | 95% CI | p Value | |
| AF | 2.41 | 1.38–4.21 | 0.002 |
| MI | 3.19 | 1.85–5.52 | <0.001 |
| CHF | 1.41 | 0.84–2.37 | 0.18 |
| T2D | 0.70 | 0.40–1.23 | 0.21 |
| PAD | 1.31 | 0.77–2.25 | 0.31 |
| Tobacco | 3.12 | 1.82–5.36 | <0.001 |
| AVF | 0.30 | 0.16–0.57 | <0.001 |
| CVC | 3.23 | 1.76–6.01 | <0.001 |
| high-NLR | 33.28 | 13.96–79.36 | <0.001 |
| high-MLR | 9.46 | 5.06–17.69 | <0.001 |
| high-PLR | 3.97 | 2.30–6.87 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. https://doi.org/10.3390/biomedicines10061272
Mureșan AV, Russu E, Arbănași EM, Kaller R, Hosu I, Arbănași EM, Voidăzan ST. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines. 2022; 10(6):1272. https://doi.org/10.3390/biomedicines10061272
Chicago/Turabian StyleMureșan, Adrian Vasile, Eliza Russu, Emil Marian Arbănași, Réka Kaller, Ioan Hosu, Eliza Mihaela Arbănași, and Septimiu Toader Voidăzan. 2022. "The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients" Biomedicines 10, no. 6: 1272. https://doi.org/10.3390/biomedicines10061272