Deep Learning for Osteoporosis Classification Using Hip Radiographs and Patient Clinical Covariates

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
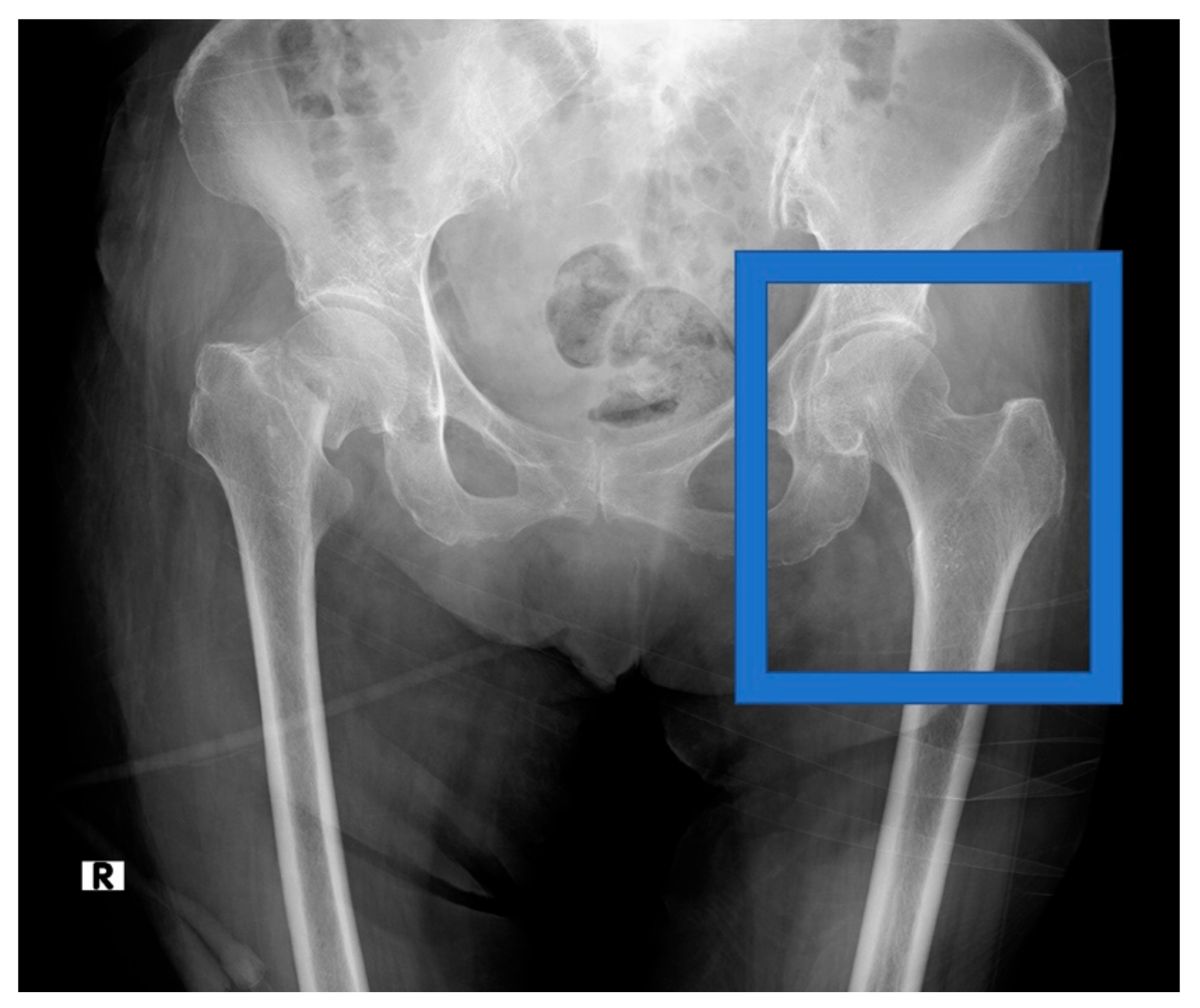
2.2. Data Acquisition
2.3. Data Preprocessing
2.4. Diagnosis of Osteoporosis
2.5. Clinical Covariates
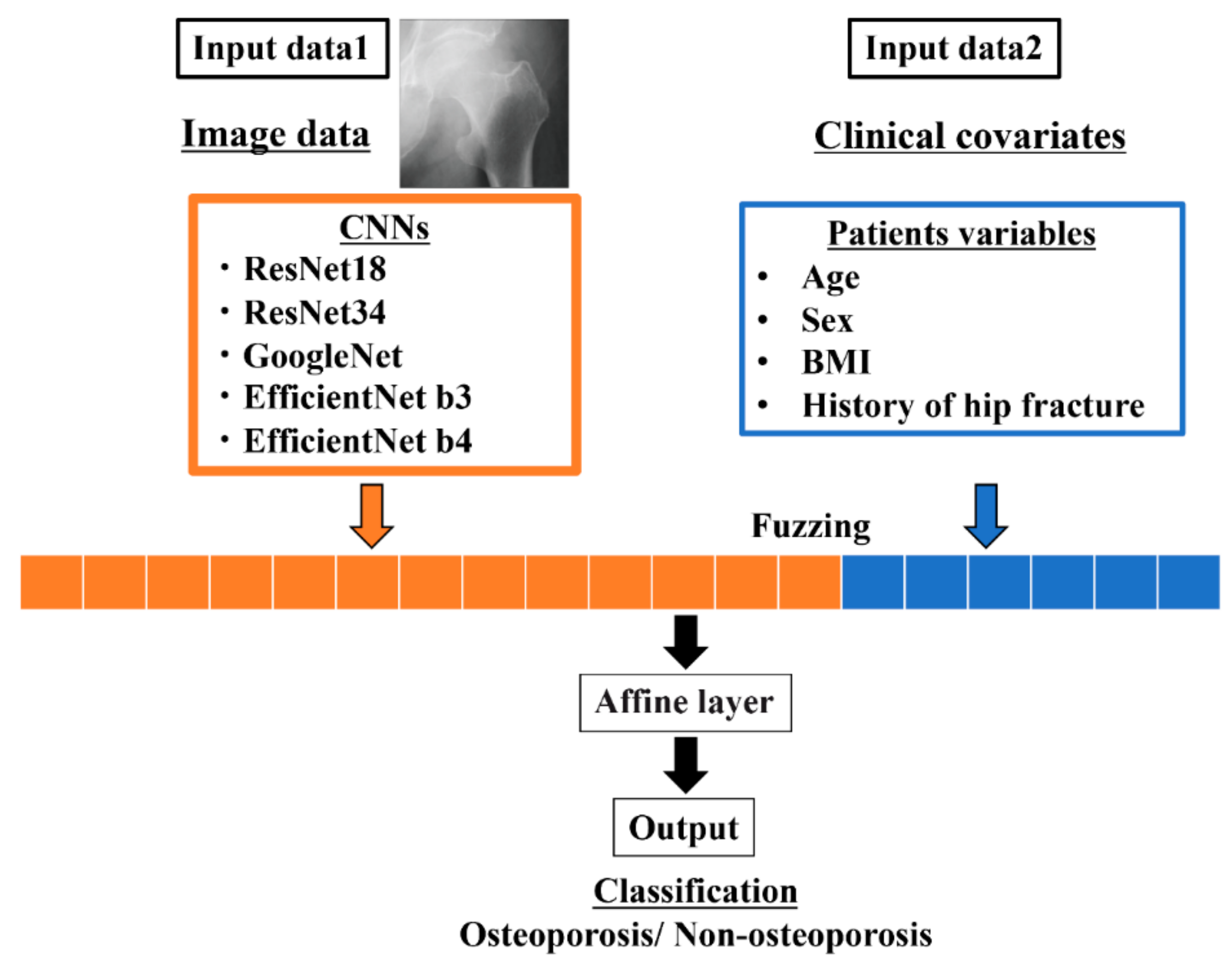
2.6. CNN Model Architecture
2.7. Architecture of the Ensemble Model
2.8. Performance Metrics
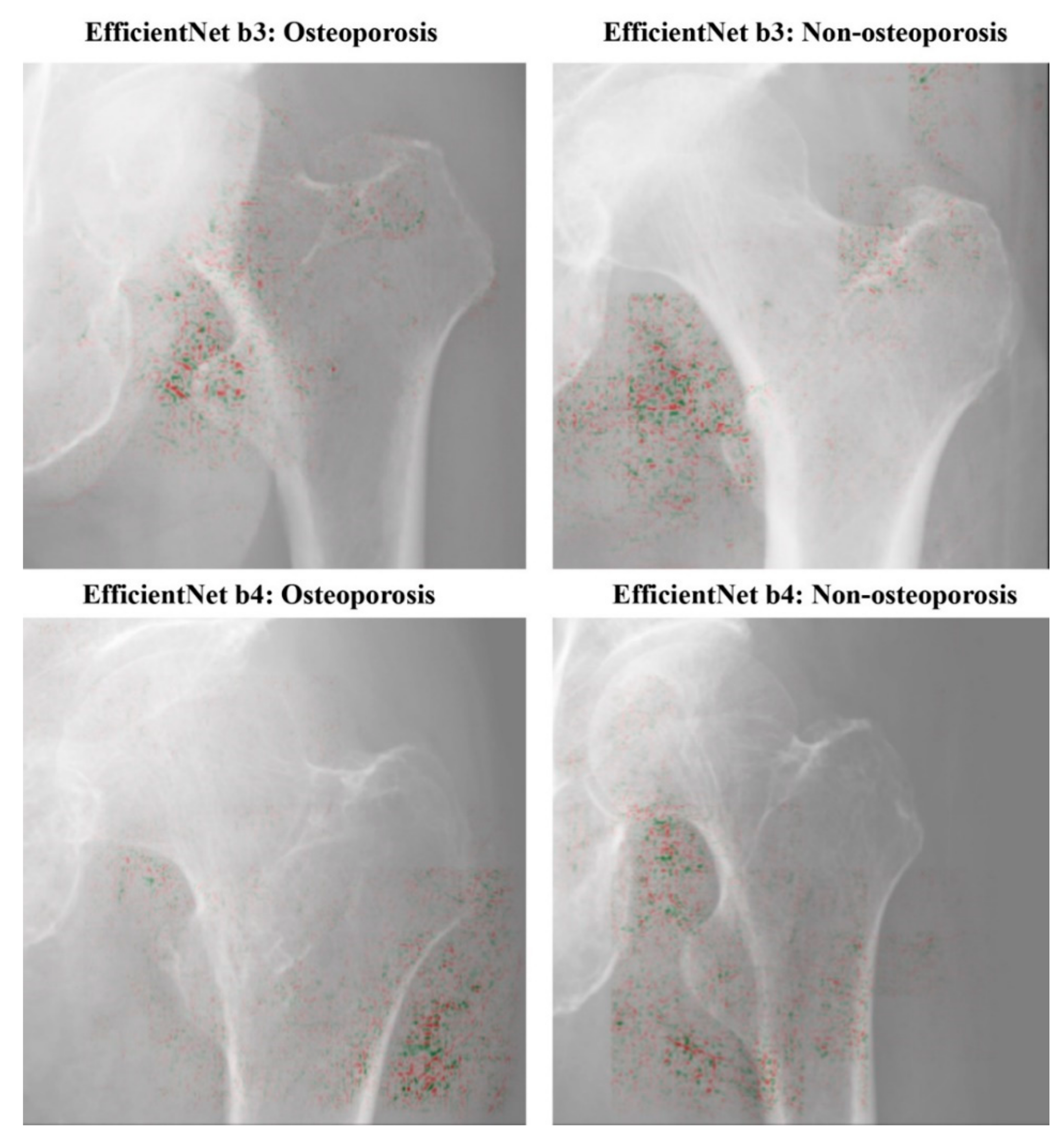
2.9. Visualization of Computer-Assisted Diagnostic System
3. Results
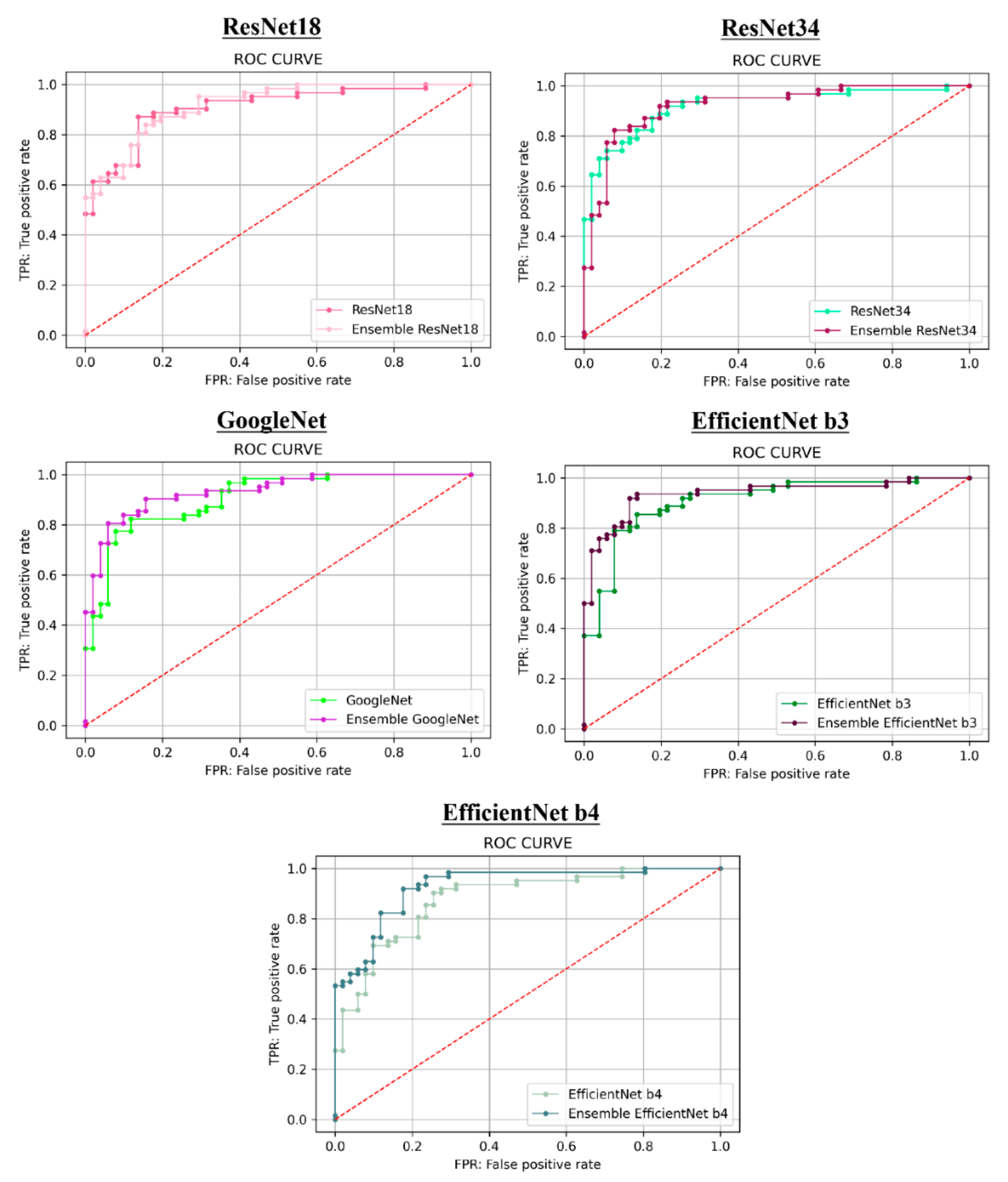
3.1. Prediction Performance
3.1.1. Hip Radiographic Image
3.1.2. Hip Radiographic Image-Connected Clinical Covariates
3.2. Visualization of Model Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bone Health and Osteoporosis: A Report of the Surgeon General; US Department of Health and Human Services: Washington, DC, USA, 2004; Volume 87, pp. 15–25.
- Nordin, C. Screening for osteoporosis: U.S. preventive services task force recommendation statement. Ann. Intern. Med. 2011, 155, 276. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.J. Fracture Liaison Services: The UK experience. Osteoporos. Int. 2011, 22, 487. [Google Scholar] [CrossRef]
- Svendsen, O.L.; Hassager, C.; Skødt, V.; Christiansen, C. Impact of soft tissue on in vivo accuracy of bone mineral measurements in the spine, hip, and forearm: A human cadaver study. J. Bone Miner. Res. 1995, 10, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Lochmüller, E.M.; Krefting, N.; Bürklein, D.; Eckstein, F. Effect of fixation, soft-tissues, and scan projection on bone mineral measurements with dual energy, X-ray absorptiometry (DXA). Calcif. Tissue Int. 2001, 68, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Mueller, D.; Econ, H.; Gandjour, A. Cost-effectiveness of using clinical risk factors with and without DXA for osteoporosis screening in postmenopausal women. Value Health 2009, 12, 1106–1117. [Google Scholar] [CrossRef] [Green Version]
- Victor Sim, M.F.; Stone, M.; Johansen, A.; Evans, W. Cost effectiveness analysis of BMD referral for DXA using ultrasound as a selective pre-screen in a group of women with low trauma Colles’ fractures. Technol. Health Care 2000, 8, 277–284. [Google Scholar]
- Wani, I.M.; Arora, S. Computer-aided diagnosis systems for osteoporosis detection: A comprehensive survey. Med. Biol. Eng. Comput. 2020, 58, 1873–1917. [Google Scholar] [CrossRef]
- Singh, M.; Nagrath, A.R.; Maini, P.S. Changes in trabecular pattern of the upper end of the femur as an index of osteoporosis. J. Bone Joint Surg. Am. 1970, 52, 457–467. [Google Scholar] [CrossRef]
- Exton-Smith, A.N.; Millard, P.H.; Payne, P.R.; Wheeler, E.F. Method for measuring quantity of bone. Lancet 1969, 294, 1153–1154. [Google Scholar] [CrossRef]
- Nguyen, B.N.T.; Hoshino, H.; Togawa, D.; Matsuyama, Y. Cortical thickness index of the proximal femur: A radiographic parameter for preliminary assessment of bone mineral density and osteoporosis status in the age 50 years and over population. CiOS Clin. Orthop. Surg. 2018, 10, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Sah, A.P.; Thornhill, T.S.; LeBoff, M.S.; Glowacki, J. Correlation of plain radiographic indices of the hip with quantitative bone mineral density. Osteoporos. Int. 2007, 18, 1119–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, Y.; Chiu, K.Y.; Yau, W.P.; Tang, W.M.; Cheung, W.Y.; Ng, T.P. Assessment of the Proximal Femoral Morphology Using Plain Radiograph-Can it Predict the Bone Quality? J. Arthroplasty 2006, 21, 508–513. [Google Scholar] [CrossRef]
- Lee, S.; Choe, E.K.; Kang, H.Y.; Yoon, J.W.; Kim, H.S. The exploration of feature extraction and machine learning for predicting bone density from simple spine X-ray images in a Korean population. Skeletal Radiol. 2020, 49, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Ferizi, U.; Honig, S.; Chang, G. Artificial intelligence, osteoporosis and fragility fractures. Curr. Opin. Rheumatol. 2019, 31, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.J.; Lee, J.H.; Han, S.S.; Kim, Y.H.; Jeong, H.G.; Choi, Y.J.; Park, W. Strut analysis for osteoporosis detection model using dental panoramic radiography. Dentomaxillofac. Radiol. 2017, 46, 20170006. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.-S.; Jung, S.-K.; Ryu, J.-J.; Shin, S.-W.; Choi, J. Evaluation of Transfer Learning with Deep Convolutional Neural Networks for Screening Osteoporosis in Dental Panoramic Radiographs. J. Clin. Med. 2020, 9, 392. [Google Scholar] [CrossRef] [Green Version]
- Dimai, H.P.; Ljuhar, R.; Ljuhar, D.; Norman, B.; Nehrer, S.; Kurth, A.; Fahrleitner-Pammer, A. Assessing the effects of long-term osteoporosis treatment by using conventional spine radiographs: Results from a pilot study in a sub-cohort of a large randomized controlled trial. Skeletal Radiol. 2019, 48, 1023–1032. [Google Scholar] [CrossRef] [Green Version]
- Areeckal, A.S.; Kamath, J.; Zawadynski, S.; Kocher, M. Combined radiogrammetry and texture analysis for early diagnosis of osteoporosis using Indian and Swiss data. Comput. Med. Imaging Graph. 2018, 68, 25–39. [Google Scholar] [CrossRef]
- Areeckal, A.S.; Jayasheelan, N.; Kamath, J.; Zawadynski, S.; Kocher, M.; David, S.S. Early diagnosis of osteoporosis using radiogrammetry and texture analysis from hand and wrist radiographs in Indian population. Osteoporos. Int. 2018, 29, 665–673. [Google Scholar] [CrossRef]
- Schreiber, J.J.; Kamal, R.N.; Yao, J. Simple Assessment of Global Bone Density and Osteoporosis Screening Using Standard Radiographs of the Hand. J. Hand Surg. Am. 2017, 42, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Tecle, N.; Teitel, J.; Morris, M.R.; Sani, N.; Mitten, D.; Hammert, W.C. Convolutional Neural Network for Second Metacarpal Radiographic Osteoporosis Screening. J. Hand Surg. Am. 2020, 45, 175–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, D.; Han, S.M. Computer-aided osteoporosis detection from DXA imaging. Comput. Methods Programs Biomed. 2019, 173, 87–107. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, G.Y.; Hwang, Y.N.; Park, S.Y.; Kim, S.M. Classification of osteoporosis by extracting the microarchitectural properties of trabecular bone from DXA scans based on thresholding technique. J. Med. Imaging Health Inform. 2015, 5, 1782–1789. [Google Scholar] [CrossRef]
- Germán, G.; George, R.W.; Raúl, S.J.E. Deep learning for biomarker regression: Application to osteoporosis and emphysema on chest CT scans. In Medical Imaging 2018: Image Processing; International Society for Optics and Photonics: Houston, TX, USA, 2018; Volume 10574. [Google Scholar] [CrossRef]
- Valentinitsch, A.; Trebeschi, S.; Kaesmacher, J.; Lorenz, C.; Löffler, M.T.; Zimmer, C.; Baum, T.; Kirschke, J.S. Opportunistic osteoporosis screening in multi-detector CT images via local classification of textures. Osteoporos. Int. 2019, 30, 1275–1285. [Google Scholar] [CrossRef] [Green Version]
- Sapthagirivasan, V.; Anburajan, M. Diagnosis of osteoporosis by extraction of trabecular features from hip radiographs using support vector machine: An investigation panorama with DXA. Comput. Biol. Med. 2013, 43, 1910–1919. [Google Scholar] [CrossRef]
- Rastegar, S.; Vaziri, M.; Qasempour, Y.; Akhash, M.R.; Abdalvand, N.; Shiri, I.; Abdollahi, H.; Zaidi, H. Radiomics for classification of bone mineral loss: A machine learning study. Diagn. Interv. Imaging 2020, 101, 599–610. [Google Scholar] [CrossRef] [Green Version]
- Badgeley, M.A.; Zech, J.R.; Oakden-Rayner, L.; Glicksberg, B.S.; Liu, M.; Gale, W.; McConnell, M.V.; Percha, B.; Snyder, T.M.; Dudley, J.T. Deep learning predicts hip fracture using confounding patient and healthcare variables. NPJ Digit. Med. 2019, 2, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Watts, N.B. Fundamentals and pitfalls of bone densitometry using dual-energy X-ray absorptiometry (DXA). Osteoporos. Int. 2004, 15, 847–854. [Google Scholar] [CrossRef]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [Green Version]
- Chiu, J.S.; Li, Y.C.; Yu, F.C.; Wang, Y.F. Applying an artificial neural network to predict osteoporosis in the elderly. Stud. Health Technol. Inform. 2006, 124, 609–614. [Google Scholar] [PubMed]
- Robinson, C.M.; Royds, M.; Abraham, A.; McQueen, M.M.; Court-Brown, C.M.; Christie, J. Refractures in patients at least forty-five years old: A prospective analysis of twenty-two thousand and sixty patients. J. Bone Jt. Surg. Ser. A 2002, 84, 1528–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. Proc. IEEE Comput. Soc. Conf. Comput. Vis. Pattern Recognit. 2016, 2016, 770–778. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015. [Google Scholar] [CrossRef] [Green Version]
- Tan, M.; Le, Q.V. EfficientNet: Rethinking model scaling for convolutional neural networks. In Proceedings of the ICML 2019: 36th International Conference on Machine Learning, San Diego, CA, USA, 9–15 June 2019. [Google Scholar]
- Sukegawa, S.; Yoshii, K.; Hara, T.; Yamashita, K.; Nakano, K.; Yamamoto, N.; Nagatsuka, H.; Furuki, Y. Deep neural networks for dental implant system classification. Biomolecules 2020, 10, 984. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. Int. J. Comput. Vis. 2020, 128, 336–359. [Google Scholar] [CrossRef] [Green Version]
- Springenberg, J.T.; Dosovitskiy, A.; Brox, T.; Riedmiller, M. Striving for simplicity: The all convolutional net. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Liu, L.; Shen, C.; Van Den Hengel, A. Cross-Convolutional-Layer Pooling for Image Recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2305–2313. [Google Scholar] [CrossRef] [Green Version]
- Urakawa, T.; Tanaka, Y.; Goto, S.; Matsuzawa, H.; Watanabe, K.; Endo, N. Detecting intertrochanteric hip fractures with orthopedist-level accuracy using a deep convolutional neural network. Skeletal Radiol. 2019, 48, 239–244. [Google Scholar] [CrossRef]
- Adams, M.; Chen, W.; Holcdorf, D.; McCusker, M.W.; Howe, P.D.L.; Gaillard, F. Computer vs. human: Deep learning versus perceptual training for the detection of neck of femur fractures. J. Med. Imaging Radiat. Oncol. 2019, 63, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.T.; Ho, T.Y.; Lee, T.Y.; Chang, C.C.; Chou, C.C.; Chen, C.C.; Chung, I.F.; Liao, C.H. Application of a deep learning algorithm for detection and visualization of hip fractures on plain pelvic radiographs. Eur. Radiol. 2019, 29, 5469–5477. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.; Giannoudis, P.V. Fragility fractures: A complex interaction of the health care system- the patient and the bone: Can we do better? Injury 2017, 48, S1–S3. [Google Scholar] [CrossRef]
- Lekamwasam, S.; Lenora, R.S.J. Effect of Leg Rotation on Hip Bone Mineral Density Measurements. J. Clin. Densitom. 2003, 6, 331–336. [Google Scholar] [CrossRef]
- Rosenthall, L. Range of change of measured BMD in the femoral neck and total hip with rotation in women. J. Bone Miner. Metab. 2004, 22, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Morin, S.; Tsang, J.F.; Leslie, W.D. Weight and body mass index predict bone mineral density and fractures in women aged 40 to 59 years. Osteoporos. Int. 2009, 20, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Ye, C.; Xiang, L. Application of artificial neural network in the diagnostic system of osteoporosis. Neurocomputing 2016, 214, 376–381. [Google Scholar] [CrossRef]
- Cruz, A.S.; Lins, H.C.; Medeiros, R.V.A.; Filho, J.M.F.; Silva, S.G. Artificial intelligence on the identification of risk groups for osteoporosis, a general review. Biomed. Eng. Online 2018, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.; Wang, M.; Wu, H.; Jiang, K.; Iwahori, Y. A novel LiDAR data classification algorithm combined capsnet with resnet. Sensors 2020, 20, 1151. [Google Scholar] [CrossRef] [Green Version]
- Yoo, T.K.; Kim, S.K.; Kim, D.W.; Choi, J.Y.; Lee, W.H.; Oh, E.; Park, E.C. Osteoporosis risk prediction for bone mineral density assessment of postmenopausal women using machine learning. Yonsei Med. J. 2013, 54, 1321–1330. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.H.; Chang, Y.F.; Chen, C.H.; Lewiecki, E.M.; Wüster, C.; Reid, I.; Tsai, K.S.; Matsumoto, T.; Mercado-Asis, L.B.; Chan, D.C.; et al. Consensus Statement on the Use of Bone Turnover Markers for Short-Term Monitoring of Osteoporosis Treatment in the Asia-Pacific Region. J. Clin. Densitom. 2019. [Google Scholar] [CrossRef]
- Kim, K.M.; Brown, J.K.; Kim, K.J.; Choi, H.S.; Kim, H.N.; Rhee, Y.; Lim, S.K. Differences in femoral neck geometry associated with age and ethnicity. Osteoporos. Int. 2011, 22, 2165–2174. [Google Scholar] [CrossRef]
- Kanis, J.A.; Burlet, N.; Cooper, C.; Delmas, P.D.; Reginster, J.Y.; Borgstrom, F.; Rizzoli, R. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2008, 19, 399–428. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Osteoporosis | Non-Osteoporosis | p Value | |
|---|---|---|---|
| (T-score ≤ −2.5) | (T-score > −2.5) | ||
| Number of patients | 598 | 535 | |
| Sex | <0.0001 | ||
| Female (%) | 506 (84.6) | 371 (69.3) | |
| Male (%) | 92 (15.4) | 164 (30.7) | |
| Mean age (SD, min-max) | 82.7 (8.3, 60, 100) | 77.7 (9.0, 60–98) | <0.0001 |
| BMI (SD, min-max) | 20.1 (3.1, 13.3–29.0) | 23.3 (9.0, 14.1–39.2) | <0.0001 |
| History of hip fracture (%) | 250 (41.8) | 157 (29.3) | <0.0001 |
| Accuracy | Precision | Recall | Specificity | npv | F1 Score | AUC Score | |
|---|---|---|---|---|---|---|---|
| ResNet18 | 0.7876 | 0.8654 | 0.7258 | 0.8627 | 0.7213 | 0.7895 | 0.9089 |
| ResNet34 | 0.8407 | 0.8793 | 0.8226 | 0.8627 | 0.8000 | 0.8500 | 0.9203 |
| GoogleNet | 0.8407 | 0.8929 | 0.8065 | 0.8824 | 0.7895 | 0.8475 | 0.9064 |
| EfficientNet b3 | 0.8407 | 0.8929 | 0.8065 | 0.8824 | 0.7895 | 0.8475 | 0.9089 |
| EfficientNet b4 | 0.8053 | 0.8030 | 0.8548 | 0.7451 | 0.8085 | 0.8281 | 0.8786 |
| Accuracy | Precision | Recall | Specificity | npv | F1 Score | AUC Score | |
|---|---|---|---|---|---|---|---|
| ResNet18 | 0.8407 | 0.8667 | 0.8387 | 0.8431 | 0.8113 | 0.8525 | 0.9190 |
| ResNet34 | 0.8673 | 0.9273 | 0.8226 | 0.9216 | 0.8103 | 0.8718 | 0.9219 |
| GoogleNet | 0.8584 | 0.8966 | 0.8387 | 0.8824 | 0.8182 | 0.8667 | 0.9330 |
| EfficientNet b3 | 0.8850 | 0.9016 | 0.8871 | 0.8824 | 0.8654 | 0.8943 | 0.9374 |
| EfficientNet b4 | 0.8584 | 0.8594 | 0.8871 | 0.8235 | 0.8571 | 0.8730 | 0.9282 |
| Accuracy | Precision | Recall | Specificity | npv | F1 Score | AUC Score | |
|---|---|---|---|---|---|---|---|
| ResNet18 | 106.7 | 100.2 | 115.6 | 97.7 | 112.5 | 108.0 | 101.1 |
| ResNet34 | 103.2 | 105.5 | 100.0 | 106.8 | 101.3 | 102.6 | 100.2 |
| GoogleNet | 102.1 | 100.4 | 104.0 | 100.0 | 103.6 | 102.3 | 102.9 |
| EfficientNet b3 | 105.3 | 101.0 | 110.0 | 100.0 | 109.6 | 105.5 | 103.1 |
| EfficientNet b4 | 106.6 | 107.0 | 103.8 | 110.5 | 106.0 | 105.4 | 105.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, N.; Sukegawa, S.; Kitamura, A.; Goto, R.; Noda, T.; Nakano, K.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; Kawasaki, K.; et al. Deep Learning for Osteoporosis Classification Using Hip Radiographs and Patient Clinical Covariates. Biomolecules 2020, 10, 1534. https://doi.org/10.3390/biom10111534
Yamamoto N, Sukegawa S, Kitamura A, Goto R, Noda T, Nakano K, Takabatake K, Kawai H, Nagatsuka H, Kawasaki K, et al. Deep Learning for Osteoporosis Classification Using Hip Radiographs and Patient Clinical Covariates. Biomolecules. 2020; 10(11):1534. https://doi.org/10.3390/biom10111534
Chicago/Turabian StyleYamamoto, Norio, Shintaro Sukegawa, Akira Kitamura, Ryosuke Goto, Tomoyuki Noda, Keisuke Nakano, Kiyofumi Takabatake, Hotaka Kawai, Hitoshi Nagatsuka, Keisuke Kawasaki, and et al. 2020. "Deep Learning for Osteoporosis Classification Using Hip Radiographs and Patient Clinical Covariates" Biomolecules 10, no. 11: 1534. https://doi.org/10.3390/biom10111534