
Effects of Tai-Chi and Running Exercises on Cardiorespiratory Fitness and Biomarkers in Sedentary Middle-Aged Males: A 24-Week Supervised Training Study


Abstract
:Simple Summary
Abstract
1. Introduction
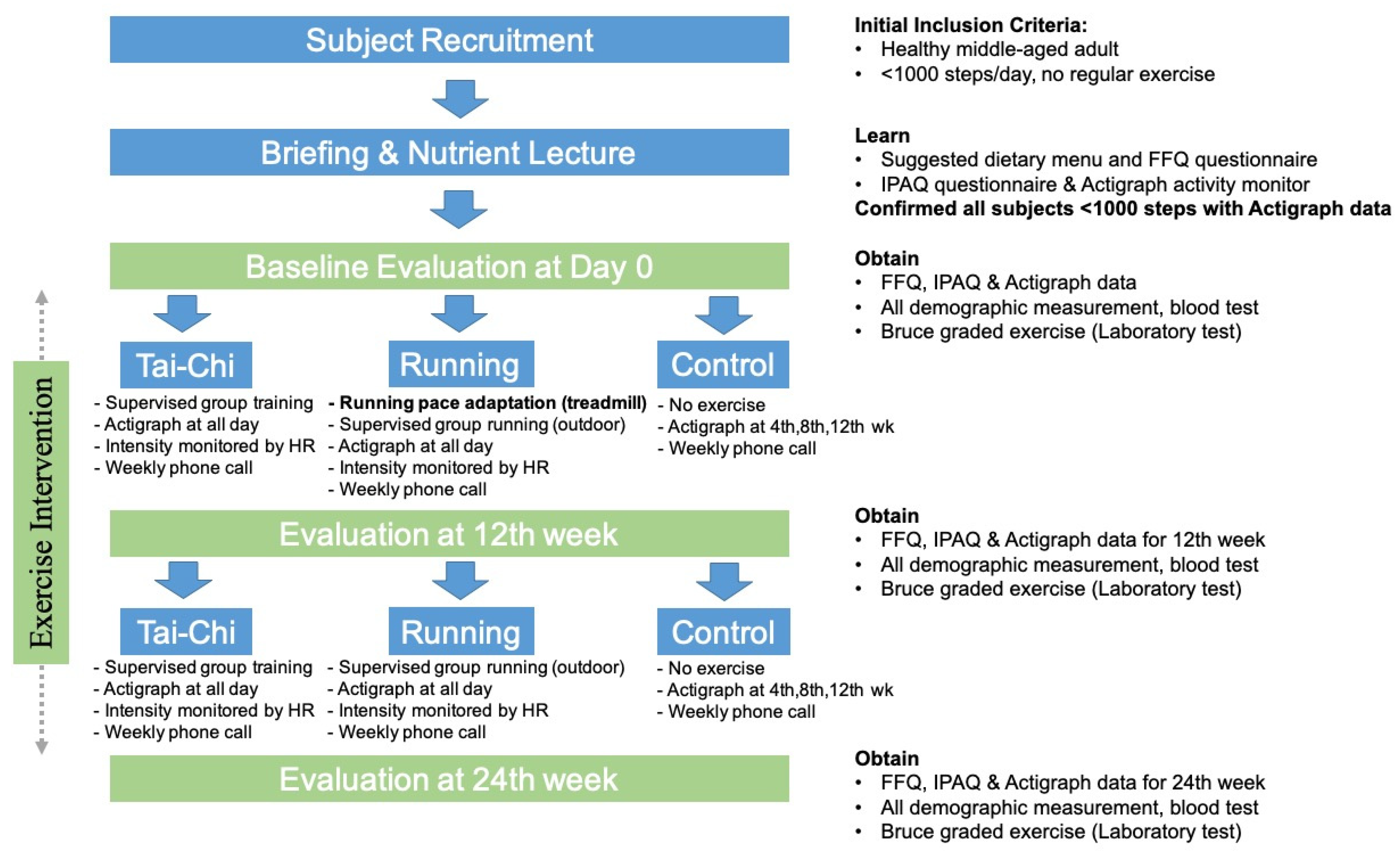
2. Materials and Methods
2.1. Participants
2.2. Exercise Intervention
2.3. Evaluation Tasks
2.4. Data Analysis
3. Results
3.1. Physical Activity and Nutrient Uptakes
3.2. Demographic Characteristics
3.3. Blood Pressure
3.4. Blood Parameters
3.5. Cardiorespiratory Fitness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barlow, C.E.; LaMonte, M.J.; Fitzgerald, S.J.; Kampert, J.B.; Perrin, J.L.; Blair, S.N. Cardiorespiratory fitness is an independent predictor of hypertension incidence among initially normotensive healthy women. Am. J. Epidemiol. 2006, 163, 142–150. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Craig, C.L.; Gauvin, L. Adiposity, physical fitness and incident diabetes: The physical activity longitudinal study. Diabetologia 2007, 50, 538–544. [Google Scholar] [CrossRef] [Green Version]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [Green Version]
- Oja, P. Dose response between total volume of physical activity and helth and fitness. Med. Sci. Sports Exerc. 2001, 33 (Suppl. S6), S428–S437. [Google Scholar] [CrossRef] [Green Version]
- Midgley, A.W.; McNaughton, L.R.; Wilkinson, M. Is there an optimal training intensity for enhancing the maximal oxygen uptake of distance runners? Empirical research findings, current opinions, physiological rationale and practical recommendations. Sports Med. 2006, 36, 117–132. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Hickson, R.C.; Rosenkoetter, M.A. Reduced training frequencies and maintenance of increased aerobic power. Med. Sci. Sports Exerc. 1981, 13, 13–16. [Google Scholar] [CrossRef]
- Lan, C.; Chen, S.Y.; Lai, J.S.; Wong, A.M. Tai Chi Chuan in medicine and health promotion. Evid. Based Complementary Altern. Med. 2013, 2013, 298768. [Google Scholar] [CrossRef]
- Hui, S.S.-C.; Xie, Y.J.; Woo, J.; Kwok, T.C.-Y. Practicing Tai Chi had lower energy metabolism than walking but similar healthbenefits in terms of aerobic fitness, resting energy expenditure, body composition and self-perceived physical health. Complementary Ther. Med. 2016, 27, 43–50. [Google Scholar] [CrossRef]
- Kang, J.W.; Lee, M.S.; Posadzki, P.; Ernst, E. Tai chi for the treatment of osteoarthritis: A systematic review and meta-analysis. BMJ Open 2011, 1, e000035. [Google Scholar] [CrossRef]
- Lan, C.; Chen, S.Y.; Wong, M.K.; Lai, J.S. Tai Chi chuan exercise for patients with cardiovascular disease. Evid. Based Complementary Altern. Med. 2013, 2013, 983208. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Stock, R.; Galver, J.; Maddalozzo, G.; Batya, S.S. Tai Chi and postural stability in patients with Parkinson’s disease. N. Eng. J. Med. 2012, 366, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Yeh, G.Y.; Wang, C.; Wayne, P.M.; Phillips, R.S. The effect of tai chi exercise on blood pressure: A systematic review. Prev. Cardiol. 2008, 11, 82–89. [Google Scholar] [CrossRef]
- Hong, Y.L.; Li, J.X.; Robinson, P.D. Balance control, flexibility, and cardiorespiratory fitness among older Tai Chi practitioners. Br. J. Sport Med. 2000, 34, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Ma, X.; Wang, L.; Zhang, C.; Song, Q.; Gu, H.; Mao, D. Effects of Tai Chi Chuan and Brisk Walking Exercise on Balance Ability in Elderly Women: A Randomized Controlled Trial. Mot. Control 2019, 23, 100–114. [Google Scholar] [CrossRef]
- Lan, C.; Lai, J.S.; Chen, S.Y.; Wong, M.K. 12-month Tai Chi training in the elderly: Its effect on health fitness. Med. Sci. Sport Exer. 1998, 30, 345–351. [Google Scholar] [CrossRef]
- Taylor-Piliae, R.E.; Froelicher, E.S. Effectiveness of Tai Chi exercise in improving aerobic capacity: A meta-analysis. J. Cardiovasc. Nurs. 2004, 19, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.S.; Lan, C.; Wong, M.K.; Teng, S.H. Two-Year trends in cardorespiratory function among older Tai Chi chuan practitioner and sedentary subjects. J. Am. Geriatr. Soc. 1995, 43, 1222–1227. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Lippincott Williams & Wilmins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Willett, W.C.; Hu, F.B. The food frequency questionnaire. Cancer Epidemiol. Biomark. Prev. 2007, 16, 182–183. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Wang, G.; He, M.; Pan, X.; Wang, Z. China Food Composition (Book 1), 6th ed.; Beijing Medical University Press: Beijing, China, 2018. [Google Scholar]
- Fielding, R.A.; Frontera, W.R.; Hughes, V.A.; Fisher, E.C.; Evans, W.J. The reproducibility of the Bruce protocol exercise test for the determination of aerobic capacity in older women. Med. Sci. Sports Exerc. 1997, 29, 1109–1113. [Google Scholar] [CrossRef]
- Xu, D.Q.; Li, J.X.; Hong, Y. Effects of long term Tai Chi practice and jogging exercise on muscle strength and endurance in older people. Br. J. Sports Med. 2006, 40, 50–54. [Google Scholar] [CrossRef] [Green Version]
- Gyllensten, A.L.; Hui-Chan, C.W.; Tsang, W.W. Stability limits, single-leg jump, and body awareness in older Tai Chi practitioners. Arch. Phys. Med. Rehabil. 2010, 91, 215–220. [Google Scholar] [CrossRef]
- Park, M.; Song, R. Effects of Tai Chi on fall risk factors: A meta-analysis. J. Korean Acad. Nurs. 2013, 43, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.Y.K.; Chong, Y.L.; Li, N.Y.; Li, M.C.; Na Lin, L.; Wong, L.Y.; Wong, B.K.; Yip, W.P.; Hon, C.H.; Chung, P.K.; et al. Feasibility and effectiveness of a Chen-style Tai Chi programme for stress reduction in junior secondary school students. Stress Health 2013, 29, 117–124. [Google Scholar] [CrossRef]
- Tsai, J.-C.; Liu, J.-C.; Kao, C.-C.; Tomlinson, B.; Kao, P.-F.; Chen, J.-W.; Chan, P. Beneficial effects on blood pressure and lipid profile of programmed exercise training in subjects with white coat hypertension. Am. J. Hypertens. 2002, 15, 571–576. [Google Scholar] [CrossRef] [Green Version]
- Mossavar-Rahmani, Y.; Hua, S.; Qi, Q.; Strizich, G.; Sotres-Alvarez, D.; Talavera, G.A.; Evenson, K.R.; Gellman, M.D.; Stoutenberg, M.; Castañeda, S.F.; et al. Are sedentary behavior and physical activity independently associated with cardiometabolic benefits? The Hispanic community of health study. BMC Public Health 2020, 20, 1400. [Google Scholar] [CrossRef]
- Thomas, G.N.; Hong, A.W.L.; Tomlinson, B.; Lau, E.; Lam, C.W.K.; Sanderson, J.E.; Woo, J. Effects of Tai Chi and resistance training on cardiovascular risk factors in elderly Chinese subjects: A 12-month longitudinal, randomized, controlled intervention study. Clin. Endocrinol. 2005, 63, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Ingul, C.B.; Tjonna, A.E.; Stolen, T.O.; Stoylen, A.; Wisloff, U. Impaired cardiac function among obese adolescents: Effect of aerobic interval training. Arch. Pediatr. Adolesc. Med. 2010, 164, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, J.F.; Hansen, P.R.; Andersen, T.R.; Andersen, L.J.; Hornstrup, T.; Krustrup, P.; Bangsbo, J. Cardiovascular adaptations to 4 and 12 months of football or strength training in 65- to 75-year-old untrained men. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. S1), 86–97. [Google Scholar] [CrossRef] [Green Version]
- Pitsavos, C.; Chrysohoou, C.; Koutroumbi, M.; Aggeli, C.; Kourlaba, G.; Panagiotakos, D.; Michaelides, A.; Stefanadis, C. The impact of moderate aerobic physical training on left ventricular mass, exercise capacity and blood pressure response during treadmill testing in borderline and mildly hypertensive males. Hell. J. Cardiol. 2011, 52, 6–14. [Google Scholar]
- Murphy, M.H.; Nevill, A.M.; Murtagh, E.M.; Holder, R.L. The effect of walking on fitness, fatness and resting blood pressure: A meta-analysis of randomised, controlled trials. Prev. Med. 2007, 44, 377–385. [Google Scholar] [CrossRef]
- Rodrigues, A.C.T.; Costa, J.D.M.; Alves, G.B.; da Silva, D.F.; Picard, M.H.; Andrade, J.L.; Mathias, W.; Negrão, C.E. Left ventricular function after exercise training in young men. Am. J. Cardiol. 2006, 97, 1089–1092. [Google Scholar] [CrossRef]
- Melling, C.; Grisé, K.; Hasilo, C.; Fier, B.; Milne, K.; Karmazyn, M.; Noble, E. A model of poorly controlled type 1 Diabetes Mellitus and its treatment with aerobic exercise training. Diabetes Metab. 2013, 39, 226–235. [Google Scholar] [CrossRef]
- Yeh, G.Y.; Wood, M.J.; Wayne, P.M.; Quilty, M.T.; Stevenson, L.W.; Davis, R.B.; Phillips, R.S.; Forman, D.E. Tai chi in patients with heart failure with preserved ejection fraction. Congest. Heart Fail. 2013, 19, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Dalleck, L.C.; Allen, B.A.; Hanson, B.A.; Borresen, E.C.; Erickson, M.E.; De Lap, S.L. Dose-response relationship between moderate-intensity exercise duration and coronary heart disease risk factors in postmenopausal women. J. Women Health 2009, 18, 105–113. [Google Scholar] [CrossRef]
- Kline, C.E.; Sui, X.; Hall, M.H.; Youngstedt, S.D.; Blair, S.N.; Earnest, C.; Church, T.S. Dose-response effects of exercise training on the subjective sleep quality of postmenopausal women: Exploratory analyses of a randomised controlled trial. BMJ Open 2012, 2, e001044. [Google Scholar] [CrossRef]
- Brien, S.E.; Janssen, I.; Katzmarzyk, P.T. Cardiorespiratory fitness and metabolic syndrome: US National Health and Nutrition Examination Survey 1999–2002. Appl. Physiol. Nutr. Metab. 2007, 32, 143–147. [Google Scholar] [CrossRef]
- Ou, Y.-C.; Chuang, H.-H.; Li, W.-C.; Tzeng, I.-S.; Chen, J.-Y. Gender difference in the association between lower muscle and metabolic syndrome independent of insulin resistance in a middle-aged and elderly Taiwanese population. Arch. Gerontol. Geriatr. 2017, 72, 12–18. [Google Scholar] [CrossRef]


{kind=link}
| Tai Chi (n = 10) | Running (n = 14) | Control (n = 12) | |
|---|---|---|---|
| Age (year) | 57.1 ± 3.8 | 56.8 ± 6.5 | 53.1 ± 4.9 |
| Height (cm) | 165.9 ± 4.5 | 166.9 ± 7.1 | 162.7 ± 5.0 |
| Body mass (kg) | 65.2 ± 5.1 | 66.7 ± 8.6 | 61.3 ± 7.6 |
| Lean mass (kg) | 50.9 ± 3.9 | 52.0 ± 6.8 | 47.9 ± 5.9 |
| BMI (kg/m2) | 23.7 ± 2.0 | 23.8 ± 1.9 | 23.1 ± 2.3 |
| Average number of step/day (step) | 763.7 ± 102.5 | 766.7 ± 144.5 | 829.7 ± 121.5 |
| Self-reported physical activity (MET-min/week) * | 1347.1 ± 339.0 | 1537.6 ± 288.1 | 1354.1 ± 307.3 |
| Time (wk) | Tai-Chi (T) | Running (R) | Control (C) | T vs. C p Value | R vs. C p Value | T vs. R p Value | Group * Time p Value | |
|---|---|---|---|---|---|---|---|---|
| Average number of steps/day (Step) | 0 | 763.7 ± 102.5 | 766.7 ± 144.5 | 829.7 ± 121.5 | 0.695 | 0.643 | 1.000 | <0.001 |
| 12 | 1734.6 ± 102.4 ** | 1671.5 ± 107.6 ** | 707.6 ± 153.6 | <0.001 | <0.001 | 0.537 | ||
| 24 | 1563.7 ± 102.5 ** | 1566.7 ± 144.5 ** | 774.8 ± 127.9 | <0.001 | <0.001 | 1.000 | ||
| Self-reported physical activity (MET-min/week) | 0 | 1347.1 ± 339.0 | 1537.6 ± 288.1 | 1354.1 ± 307.3 | 0.161 | 1.000 | 0.055 | <0.001. |
| 12 | 1340.6 ± 339.0 | 1539.9 ± 288.2 | 1558.6 ± 307.8 ** | 0.328 | 1.000 | 0.388 | ||
| 24 | 1342.9 ± 339.0 | 1542.1 ± 288.2 | 1560.8 ± 307.8 ** | 0.341 | 0.998 | 0.372 | ||
| Reported dietary intake (kcal) | 0 | 2703.0 ± 1.6 | 2702.6.6 ± 1.5 | 2702.7 ± 1.5 | 0.968 | 0.993 | 0.890 | <0.001 |
| 12 | 2729.9 ± 3.2 * | 2716.7 ± 13.8 ** | 2702.9 ± 1.5 | <0.001 | 0.007 | 0.011 | ||
| 24 | 2762.5 ± 21.7 ** † | 2768.6 ± 5.8 ** †† | 2703.0 ± 1.5 | <0.001 | <0.001 | 0.773 | ||
| Carbohydrate intake (g/day) | 0 | 354.4 ± 5.3 | 357.4 ± 4.7 | 353.6 ± 5.3 | 0.973 | 0.174 | 0.410 | 0.013 |
| 12 | 368.2 ± 4.3 ** | 367.6 ± 4.2 ** | 354.4 ± 8.7 | <0.001 | 0.001 | 0.981 | ||
| 24 | 361.2 ± 4.9 † | 364.1 ± 4.2 * | 355.6 ± 8.2 | 0.163 | 0.015 | 0.381 | ||
| Fat intake (g/day) | 0 | 94.0 ± 1.4 | 94.8 ± 1.3 | 93.8 ± 1.4 | 0.973 | 0.174 | 0.410 | 0.007 |
| 12 | 97.6 ± 1.2 ** | 97.5 ± 1.1 ** | 94.0 ± 2.3 | 0.001 | 0.001 | 0.981 | ||
| 24 | 96.1 ± 1.3 * | 96.8 ± 1.1 * | 94.9 ± 1.3 | 0.120 | 0.002 | 0.382 | ||
| Protein intake (g/day) | 0 | 89.9 ± 1.4 | 90.7 ± 1.3 | 89.7 ± 1.4 | 0.973 | 0.174 | 0.410 | 0.007 |
| 12 | 91.6 ± 1.2 * | 91.5 ± 1.1 | 89.9 ± 2.3 | 0.106 | 0.138 | 0.981 | ||
| 24 | 91.1 ± 1.3 | 91.8 ± 1.1 | 90.2 ± 1.4 | 0.374 | 0.011 | 0.382 |
| Time (wk) | Tai-Chi (T) | Running (R) | Control (C) | T vs. C p Value | R vs. C p Value | T vs. R p Value | Group * Time p Value | |
|---|---|---|---|---|---|---|---|---|
| Resting heart rate (b/min) | 0 | 72.9 ± 10.87 | 69.0 ± 6.5 | 68.1 ± 6.4 | 0.146 | 0.679 | 0.068 | 0.057 |
| 12 | 67.0 ± 7.4 | 66.2 ± 5.7 | 69.6 ± 7.1 | 0.109 | 0.175 | 0.570 | ||
| 24 | 66.2 ± 8.0 ** | 65.3 ± 5.8 ** | 72.2 ± 8.4 | 0.014 | 0.018 | 0.528 | ||
| Body mass (kg) | 0 | 65.2 ± 5.1 | 66.7 ± 8.6 | 61.3 ± 7.6 | 0.710 | 0.232 | 1.000 | <0.001 |
| 12 | 65.7 ± 5.2 | 67.2 ± 8.7 | 61.8 ± 7.7 | 0.714 | 0.235 | 1.000 | ||
| 24 | 64.8 ± 5.1 | 66.3 ± 8.6 | 61.9 ± 7.6 | 1.000 | 0.443 | 1.000 | ||
| Lean mass (kg) | 0 | 50.9 ± 3.9 | 52.0 ± 6.7 | 47.9 ± 5.9 | 0.709 | 0.234 | 1.000 | <0.001 |
| 12 | 53.9 ± 4.2 | 55.1 ± 7.1 | 48.5 ± 6.0 | 0.143 | 0.028 | 1.000 | ||
| 24 | 56.4 ± 7.1 | 51.3 ± 8.1 | 43.4 ± 5.4 | <0.001 | <0.001 | 1.000 | ||
| Systolic blood pressure (SBP, mmHg) | 0 | 124.7 ± 3.2 | 126.1 ± 8.5 | 126.8 ± 11.1 | 0.643 | 0.851 | 0.750 | 0.703 |
| 12 | 119.7 ± 5.6 | 124.6 ± 12.8 | 126.8 ± 10.6 | 0.217 | 0.639 | 0.376 | ||
| 24 | 116.8 ± 6.1 | 121.8 ± 8.8 | 125.3 ± 11.5 | 0.095 | 0.388 | 0.307 | ||
| Diastolic blood pressure (DBP, mmHg) | 0 | 77.7 ± 6.9 | 78.2 ± 5.8 | 79.6 ± 5.9 | 0.544 | 0.597 | 0.852 | 0.006 |
| 12 | 72.0 ± 8.0 | 72.9 ± 7.6 | 83.5 ± 8.6 | 0.010 | 0.004 | 0.818 | ||
| 24 | 70.2 ± 7.7 ** | 70.2 ± 5.6 ** † | 83.6 ± 7.9 | 0.001 | <0.001 | 0.985 | ||
| Total cholesterol (TC, mmol/L) | 0 | 4.33 ± 0.54 | 4.35 ± 0.64 | 4.40 ± 0.56 | 0.787 | 0.842 | 0.929 | 0.073 |
| 12 | 4.24 ± 0.48 | 4.11 ± 0.60 | 4.37 ± 0.61 | 0.591 | 0.246 | 0.579 | ||
| 24 | 4.04 ± 0.58 | 4.00 ± 0.62 | 4.46 ± 0.59 | 0.115 | 0.058 | 0847 | ||
| Triglycerides (TG, mmol/L) | 0 | 1.49 ± 0.19 | 1.51 ± 0.21 | 1.49 ± 0.33 | 0.976 | 0.884 | 0.865 | <0.001 |
| 12 | 1.36 ± 0.22 | 1.24 ± 0.23 ** | 1.53 ± 0.32 | 0.141 | 0.008 | 0.276 | ||
| 24 | 1.37 ± 0.22 | 1.18 ± 0.22 ** † | 1.56 ± 0.32 | 0.103 | 0.001 | 0.074 | ||
| High-density lipoprotein cholesterol (HDL-C, mmol/L) | 0 | 1.36 ± 0.33 | 1.34 ± 0.29 | 1.34 ± 0.23 | 0.897 | 0.940 | 0.838 | 0.694 |
| 12 | 1.41 ± 0.26 | 1.42 ± 0.24 | 1.35 ± 0.22 | 0.574 | 0.444 | 0.882 | ||
| 24 | 1.49 ± 0.26† | 1.46 ± 0.27 | 1.38 ± 0.24 | 0.329 | 0.444 | 0.775 | ||
| Low-density lipoprotein cholesterol (LDL-C, mmol/L) | 0 | 2.63 ± 0.54 | 2.63 ± 0.52 | 2.68 ± 0.50 | 0.801 | 0.790 | 0.992 | 0.012 |
| 12 | 2.46 ± 0.51 | 2.25 ± 0.48 ** | 3.10 ± 0.96 * | 0.046 | 0.005 | 0.491 | ||
| 24 | 2.41 ± 0.50 | 2.18 ± 0.44 ** †† | 3.12 ± 0.97 * | 0.028 | 0.002 | 0.443 | ||
| Fasting blood glucose (FBG, mmol/L) | 0 | 5.37 ± 0.21 | 5.38 ± 0.21 | 5.38 ± 0.25 | 0.881 | 0.942 | 0.933 | 0.088 |
| 12 | 5.40 ± 0.12 | 5.30 ± 0.20 | 5.37 ± 0.27 | 0.773 | 0.410 | 0.286 | ||
| 24 | 5.19 ± 0.16 | 5.16 ± 0.22 | 5.32 ± 0.25 | 0.197 | 0.089 | 0.753 |
| Time (wk) | Tai-Chi (T) | Running (R) | Control (C) | T vs. C p Value | R vs. C p Value | T vs. R p Value | Group * Time p Value | |
|---|---|---|---|---|---|---|---|---|
| Maximal MET achieved in Bruce test (MET-min/week) | 0 | 9.2 ± 1.0 | 9.6 ± 1.0 | 9.2 ± 0.9 | 1.000 | 0.925 | 1.000 | <0.001 |
| 12 | 10.9 ± 0.8 | 11.0 ± 1.0 | 9.1 ± 1.0 | <0.001 | <0.001 | 1.000 | ||
| 24 | 11.7 ± 0.9 | 12.8 ± 0.8 | 9.4 ± 1.0 | <0.001 | <0.001 | 0.019 | ||
| Rating of Perceived Exertion at 50–60% VO2max (RPE) | 0 | 12.5 ± 0.5 | 12.3 ± 0.5 | 12.3 ± 0.5 | 0.830 | 0.992 | 0.669 | <0.001 |
| 12 | 9.5 ± 0.5 * | 9.6 ± 0.5 * | 12.3 ± 0.5 | <0.001 | <0.001 | 0.876 | ||
| 24 | 9.4 ± 0.5 * | 9.3 ± 0.5 ** | 12.3 ± 0.5 | <0.001 | <0.001 | 0.924 | ||
| Maximal oxygen uptake (VO2max, mL/kg/min) | 0 | 32.6 ± 3.5 | 33.4 ± 3.3 | 31.1 ± 3.4 | 0.305 | 0.089 | 0.305 | <0.001 |
| 12 | 38.0 ± 3.2 ** | 38.6 ± 3.3 ** | 30.6 ± 2.2 | <0.001 | <0.001 | 0.603 | ||
| 24 | 40.2 ± 2.1 ** †† | 44.6 ± 2.8** †† | 31.4 ± 2.2 | <0.001 | <0.001 | <0.001 | ||
| Maximal aerobic speed (Vmax, km/h) | 0 | 5.7 ± 0.5 | 5.9 ± 0.8 | 5.9 ± 0.8 | 0.601 | 0.919 | 0.524 | <0.001 |
| 12 | 6.5 ± 0.5 ** | 7.2 ± 0.6 ** | 6.1 ± 0.9 | 0.208 | <0.001 | 0.019 | ||
| 24 | 7.1 ± 1.1 ** | 7.9 ± 1.0 ** † | 6.1 ± 0.9 | 0.020 | <0.001 | 0.085 | ||
| Peak heart rate (HRpeak, b/min) | 0 | 166.8 ± 9.9 | 166.8 ± 15.2 | 164.9 ± 13.6 | 0.745 | 0.725 | 0.998 | 0.440 |
| 12 | 176.7 ± 14.7 | 172.7 ± 12.2 | 168.8 ± 12.6 | 0.164 | 0.445 | 0.465 | ||
| 24 | 181.6 ± 11.4 ** | 176.3 ± 6.8 ** | 167.2 ± 13.5 | 0.003 | 0.038 | 0.239 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Guo, X.; Liu, L.; Xie, M.; Lam, W.-K. Effects of Tai-Chi and Running Exercises on Cardiorespiratory Fitness and Biomarkers in Sedentary Middle-Aged Males: A 24-Week Supervised Training Study. Biology 2022, 11, 375. https://doi.org/10.3390/biology11030375
Wang Y, Guo X, Liu L, Xie M, Lam W-K. Effects of Tai-Chi and Running Exercises on Cardiorespiratory Fitness and Biomarkers in Sedentary Middle-Aged Males: A 24-Week Supervised Training Study. Biology. 2022; 11(3):375. https://doi.org/10.3390/biology11030375
Chicago/Turabian StyleWang, Yi, Xian Guo, Liangchao Liu, Minhao Xie, and Wing-Kai Lam. 2022. "Effects of Tai-Chi and Running Exercises on Cardiorespiratory Fitness and Biomarkers in Sedentary Middle-Aged Males: A 24-Week Supervised Training Study" Biology 11, no. 3: 375. https://doi.org/10.3390/biology11030375