
Effect of Coronary Artery Disease on COVID-19—Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis

 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
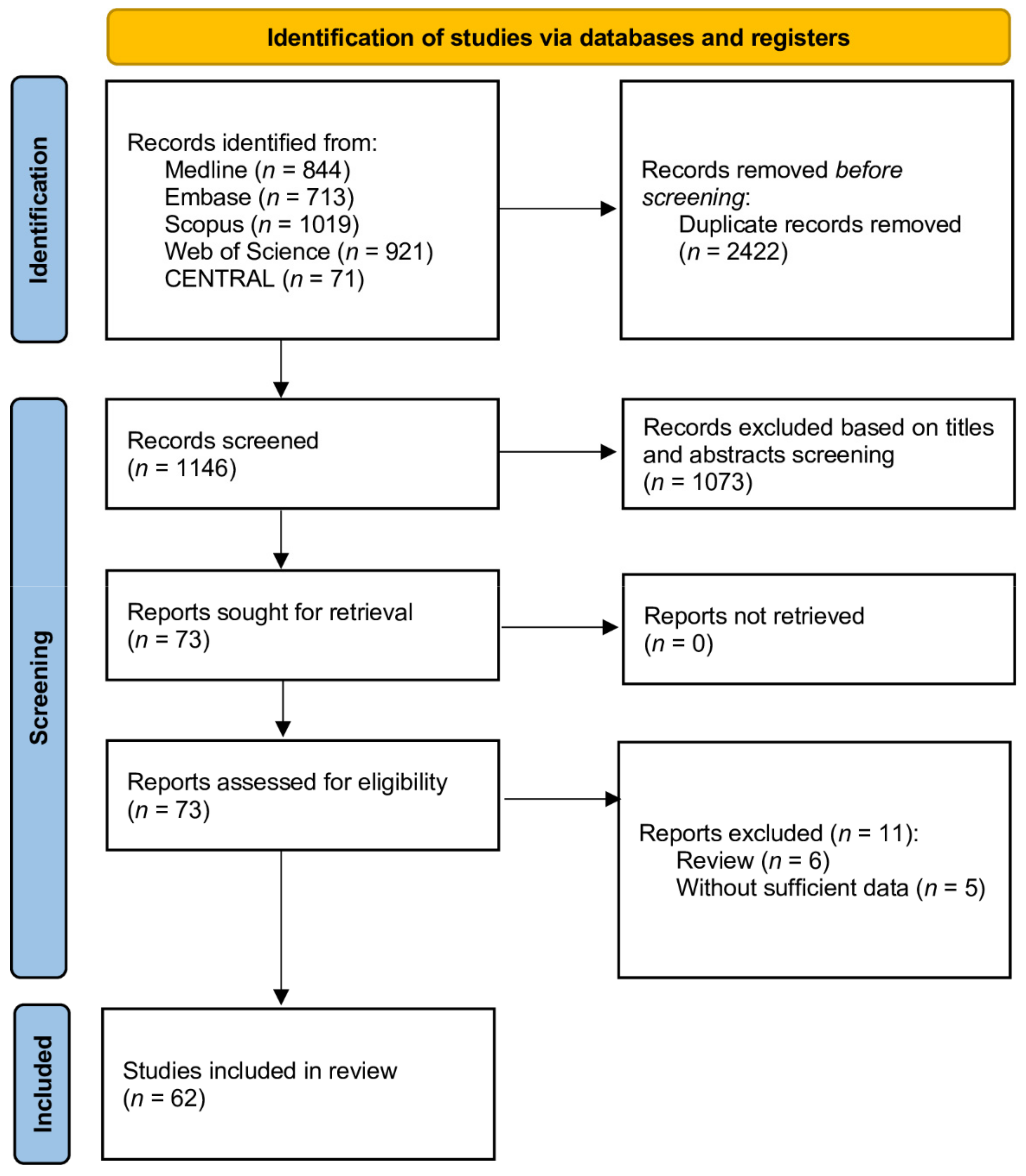
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
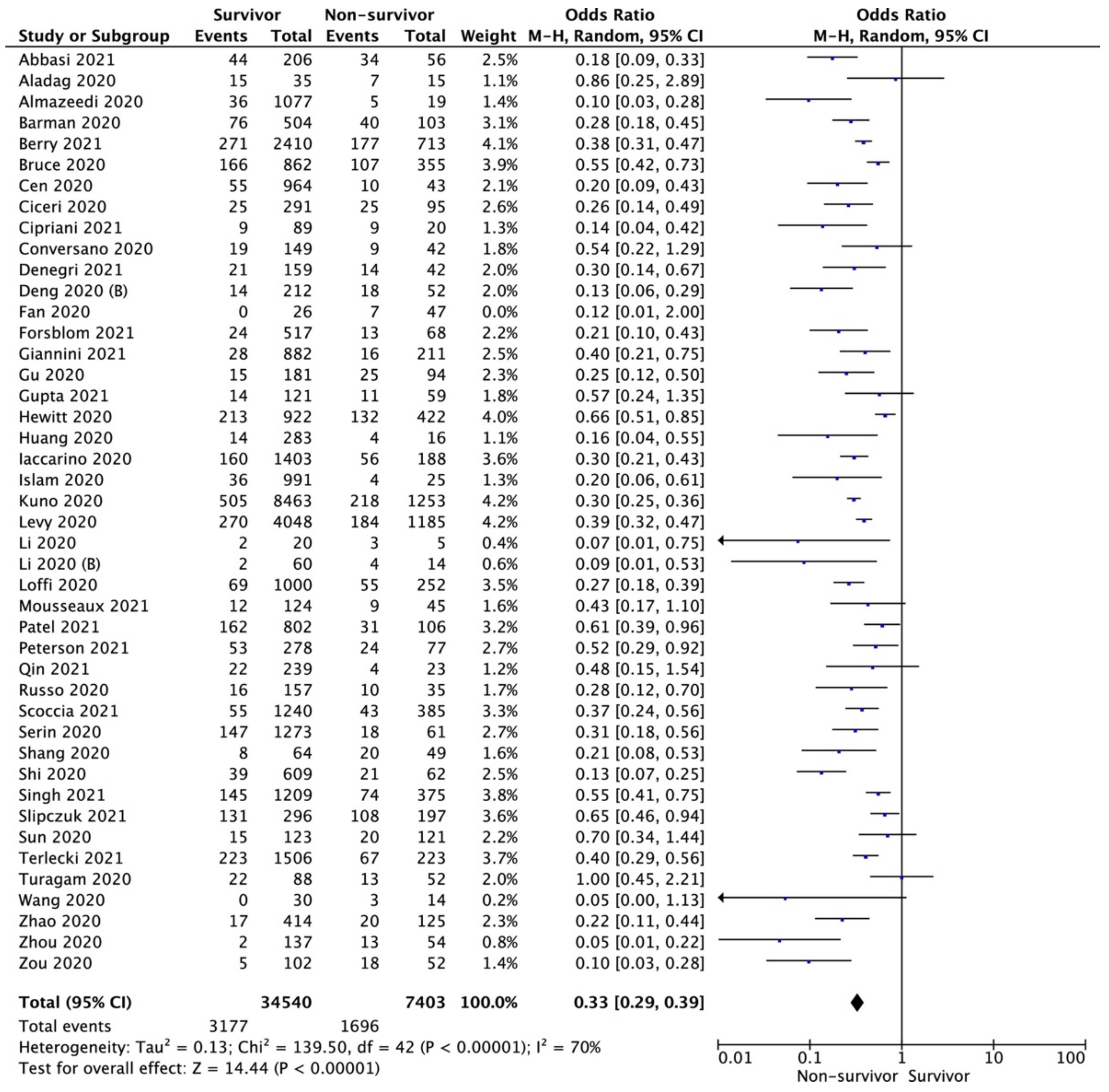
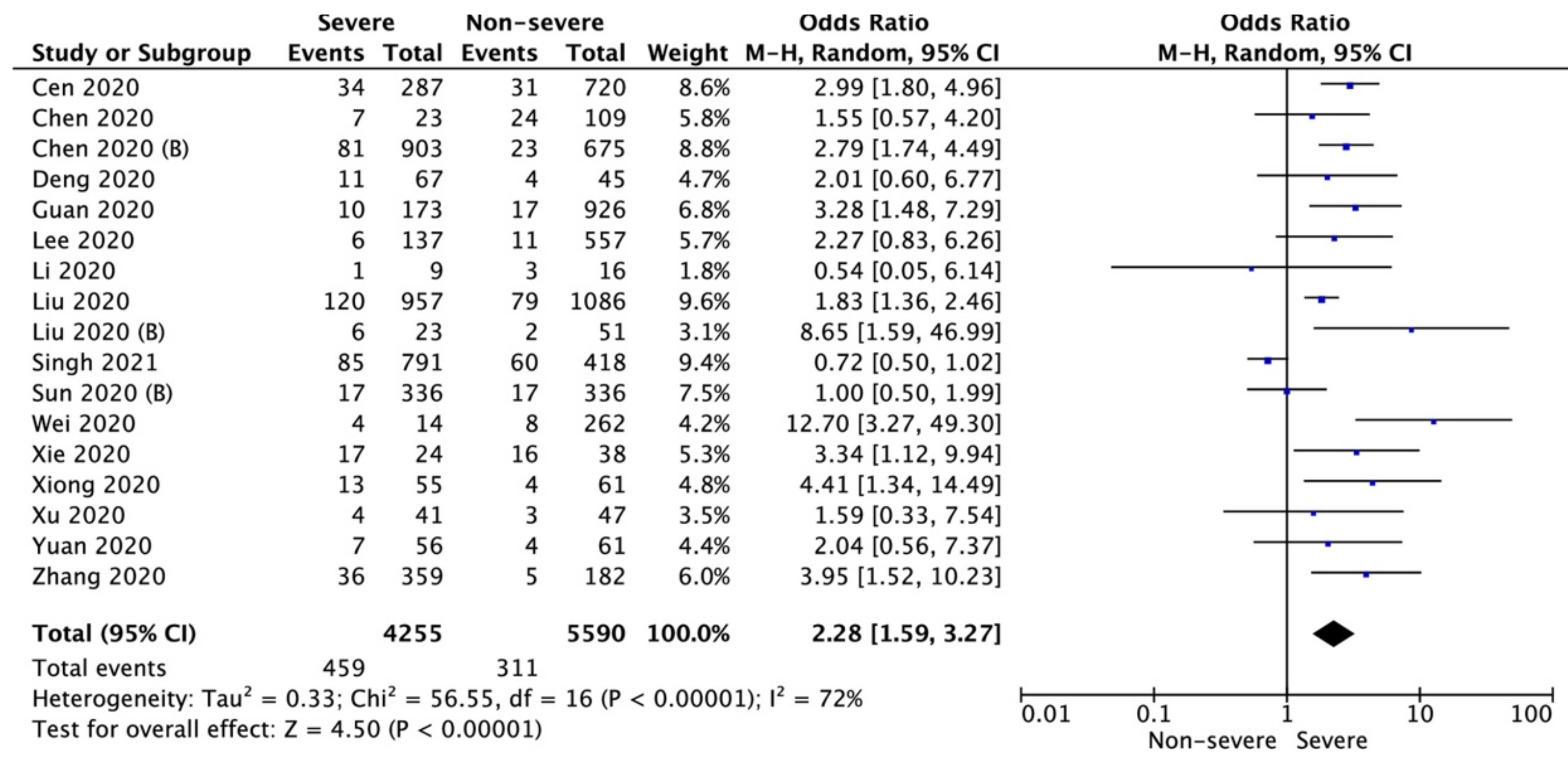
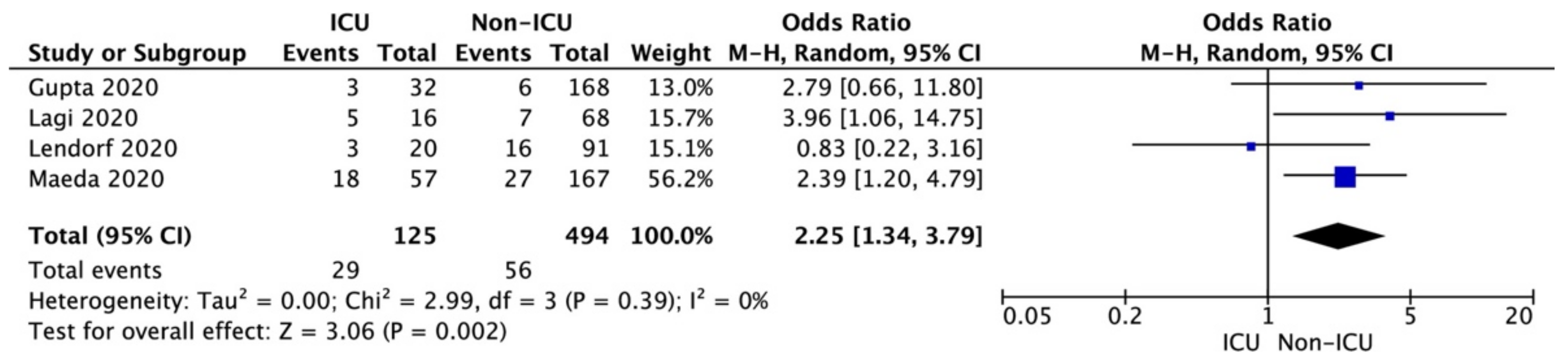
3.2. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dzieciatkowski, T.; Szarpak, L.; Filipiak, K.J.; Jaguszewski, M.; Ladny, J.R.; Smereka, J. COVID-19 challenge for modern medicine. Cardiol. J. 2020, 27, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Dabrowski, M.; Steliga, A.; Dabrowska, A.; Smereka, J.; Szarpak, L. Use simulation to improve the effectiveness of PPE in COVID-19. Disaster Emerg. Med. J. 2020, 5, 171–173. [Google Scholar] [CrossRef]
- COVID-19 MAP. Available online: https://coronavirus.jhu.edu/map.html (accessed on 17 November 2021).
- Kirtipal, N.; Bharadwaj, S.; Kang, S.G. From SARS to SARS-CoV-2, insights on structure, pathogenicity and immunity aspects of pandemic human coronaviruses. Infect. Genet. Evol. 2020, 85, 104502. [Google Scholar] [CrossRef]
- Hosseini, E.S.; Kashani, N.R.; Nikzad, H.; Azadbakht, J.; Bafrani, H.H.; Kashani, H.H. The novel coronavirus Disease-2019 (COVID-19): Mechanism of action, detection and recent therapeutic strategies. Virology 2020, 551, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Szarpak, L.; Borkowska, M.; Peacock, F.W.; Rafique, Z.; Gasecka, A.; Smereka, J.; Pytkowska, K.; Jachowicz, M.; Iskrzycki, L.; Gilis-Malinowska, N.; et al. Characteristics and outcomes of in-hospital cardiac arrest in COVID-19. A systematic review and meta-analysis. Cardiol. J. 2021, 28, 503–508. [Google Scholar] [CrossRef]
- Gasecka, A.; Pruc, M.; Kukula, K.; Gilis-Malinowska, N.; Filipiak, K.J.; Jaguszewski, M.J.; Szarpak, L. Post-COVID-19 heart syndrome. Cardiol. J. 2021, 28, 353–354. [Google Scholar] [CrossRef] [PubMed]
- Huff, H.V.; Singh, A. Asymptomatic Transmission during the Coronavirus Disease 2019 Pandemic and Implications for Public Health Strategies. Clin. Infect. Dis. 2020, 71, 2752–2756. [Google Scholar] [CrossRef] [PubMed]
- Forsblom, E.; Silén, S.; Kortela, E.; Ahava, M.; Kreivi, H.R.; Holmberg, V.; Järvinen, A.; Hästbacka, J.; Kivivuori, S.M.; Meretoja, A. Male predominance in disease severity and mortality in a low Covid-19 epidemic and low case-fatality area—A population-based registry study. Infect. Dis. 2021, 53, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Szarpak, L.; Pruc, M.; Filipiak, K.J.; Popieluch, J.; Bielski, A.; Jaguszewski, M.J.; Gilis-Malinowska, N.; Chirico, F.; Rafique, Z.; Peacock, F.W. Myocarditis: A complication of COVID-19 and LONG-COVID-19 syndrome as a serious threat in modern cardiology. Cardiol. J. 2021, 29. [Google Scholar] [CrossRef]
- Lipton, R.B.; Schwedt, T.J.; Friedman, B.W. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Theroux, P. Pathophysiology of Coronary Artery Disease. Circulation 2005, 111, 3481–3488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Borkowska, M.J.; Jaguszewski, M.J.; Koda, M.; Gasecka, A.; Szarpak, A.; Gilis-Malinowska, N.; Safiejko, K.; Szarpak, L.; Filipiak, K.J.; Smereka, J. Impact of Coronavirus Disease 2019 on Out-of-Hospital Cardiac Arrest Survival Rate: A Systematic Review with Meta-Analysis. J. Clin. Med. 2021, 10, 1209. [Google Scholar] [CrossRef]
- Szarpak, L.; Jaguszewski, M.J.; Pruc, M.; Rafique, Z. Myocardial injury: A future challenge for long-COVID-19 complications. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 618. [Google Scholar] [CrossRef]
- Scoccia, A.; Gallone, G.; Cereda, A.; Palmisano, A.; Vignale, D.; Leone, R.; Nicoletti, V.; Gnasso, C.; Monello, A.; Khokhar, A.; et al. Impact of clinical and subclinical coronary artery disease as assessed by coronary artery calcium in COVID-19. Atherosclerosis 2021, 328, 136–143. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 12 December 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection is Suspected: Interim Guidance, 28 January 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Bielski, K.; Makowska, K.; Makowski, A.; Kopiec, T.; Gasecka, A.; Malecka, M.; Pruc, M.; Rafique, Z.; Peacock, F.W.; Denegri, A.; et al. Impact of COVID-19 on in-hospital cardiac arrest outcomes: An updated meta-analysis. Cardiol. J. 2021, 28, 816–824. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Syn. Meth. 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wichmann, D.; Sperhake, J.-P.; Lutgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy findings and venous thromboembolism in patients with COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Nägele, M.P.; Haubner, B.; Tanner, F.C.; Ruschitzka, F.; Flammer, A.J. Endothelial dysfunction in COVID-19: Current findings and therapeutic implications. Atherosclerosis 2020, 314, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef]
- Fan, H.; Zhang, L.; Huang, B.; Zhu, M.; Zhou, Y.; Zhang, H.; Tao, X.; Cheng, S.; Yu, W.; Zhu, L.; et al. Cardiac injuries in patients with coronavirus disease 2019: Not to be ignored. Int. J. Infect. Dis. 2020, 96, 294–297. [Google Scholar] [CrossRef]
- Banerjee, A.; Pasea, L.; Harris, S.; Gonzalez-Izquierdo, A.; Torralbo, A.; Shallcross, L.; Noursadeghi, M.; Pillay, D.; Sebire, N.; Holmes, C.; et al. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: A population-based cohort study. Lancet 2020, 395, 1715–1725. [Google Scholar] [CrossRef]
- Cen, Y.; Chen, X.; Shen, Y.; Zhang, X.H.; Lei, Y.; Xu, C.; Jiang, W.R.; Xu, H.T.; Chen, Y.; Zhu, J.; et al. Risk factors for disease progression in patients with mild to moderate coronavirus disease 2019—A multi-centre observational study. Clin. Microbiol. Infect. 2020, 26, 1242–1247. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, J.; Li, C.; Hu, Z.; Zhang, M.; Tu, P.; Liu, L.; Zong, W. The characteristics and death risk factors of 132 COVID-19 pneumonia patients with comorbidities: A retrospective single center analysis in Wuhan, China. medRxiv 2020. [Google Scholar] [CrossRef]
- Kuno, T.; Takahashi, M.; Obata, R.; Maeda, T. Cardiovascular comorbidities, cardiac injury, and prognosis of COVID-19 in New York City. Am. Heart J. 2020, 226, 24–25. [Google Scholar] [CrossRef]
- Russo, V.; Di Maio, M.; Attena, E.; Silverio, A.; Scudiero, F.; Celentani, D.; Lodigiani, C.; Di Micco, P. Clinical impact of pre-admission antithrombotic therapy in hospitalized patients with COVID-19: A multicenter observational study. Pharmacol. Res. 2020, 159, 104965. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, G.; Grassi, G.; Borghi, C.; Ferri, C.; Salvetti, M.; Volpe, M.; SARS-RAS Investigators. Age and Multimorbidity Predict Death Among COVID-19 Patients: Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension 2020, 76, 366–372. [Google Scholar] [CrossRef]
- Denegri, A.; Pezzuto, G.; D’Arienzo, M.; Morelli, M.; Savorani, F.; Cappello, C.G.; Luciani, A.; Boriani, G. Clinical and electrocardiographic characteristics at admission of COVID-19/SARS-CoV2 pneumonia infection. Intern. Emerg. Med. 2021, 16, 1451–1456. [Google Scholar] [CrossRef]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020, 5, e444–e451. [Google Scholar] [CrossRef]
- Krittanawong, C.; Kumar, A.; Hahn, J.; Wang, Z.; Zhang, H.J.; Sun, T.; Bozkurt, B.; Ballantyne, C.M.; Virani, S.S.; Halperin, J.L.; et al. Cardiovascular risk and complications associated with COVID-19. Am. J. Cardiovasc. Dis. 2020, 10, 479–489. [Google Scholar]
- Planek, M.I.C.; Ruge, M.; Du Fay de Lavallaz, J.M.; Kyung, S.B.; Gomez, J.M.D.; Suboc, T.M.; Williams, K.A.; Volgman, A.S.; Simmons, J.A.; Rao, A.K. Cardiovascular findings on chest computed tomography associated with COVID-19 adverse clinical outcomes. Am. Heart J. Plus. 2021, 11, 100052. [Google Scholar] [CrossRef]
- Mousseaux, E.; Fayol, A.; Danchin, N.; Soulat, G.; Charpentier, E.; Livrozet, M.; Carves, J.B.; Tea, V.; Salem, F.B.; Chamandi, C.; et al. Association between coronary artery calcifications and 6-month mortality in hospitalized patients with COVID-19. Diagn. Interv. Imaging 2021, 102, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. People Who Are at Higher Risk for Severe Illness. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/underlying-evidence-table.html (accessed on 1 December 2020).
- Chen, Y.; Ke, Y.; Liu, X.; Wang, Z.; Jia, R.; Liu, W.; Yang, C.; Jia, L.; Wang, Y.; Han, L.; et al. Clinical features and antibody response of patients from a COVID-19 treatment hospital in Wuhan, China. J. Med. Virol. 2021, 93, 2782–2789. [Google Scholar] [CrossRef]
- Angeli, F.; Marazzato, J.; Verdecchia, P.; Balestrino, A.; Bruschi, C.; Ceriana, P.; Chiovato, L.; Dalla Vecchia, L.A.; De Ponti, R.; Fanfulla, F.; et al. Joint effect of heart failure and coronary artery disease on the risk of death during hospitalization for COVID-19. Eur. J. Intern. Med. 2021, 89, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Hessami, A.; Shamshirian, A.; Heydari, K.; Pourali, F.; Alizadeh-Navaei, R.; Moosazadeh, M.; Abrotan, S.; Shojaie, L.; Sedighi, S.; Shamshirian, D.; et al. Cardiovascular diseases burden in COVID-19: Systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 46, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Conversano, A.; Melillo, F.; Napolano, A.; Fominskiy, E.; Spessot, M.; Ciceri, F.; Agricola, E. Renin-Angiotensin-Aldosterone System Inhibitors and Outcome in Patients with SARS-CoV-2 Pneumonia: A Case Series Study. Hypertension 2020, 76, e10–e12. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Offringa-Hup, A.K.; Logtenberg, S.J.J.; Van der Linden, P.D.; Janssen, W.M.T.; Klein, H.; Waanders, F.; Simsek, S.; de Jager, C.P.C.; Smits, P.; et al. Discontinuation of Antihypertensive Medications on the Outcome of Hospitalized Patients With Severe Acute Respiratory Syndrome-Coronavirus 2. Hypertension 2021, 78, 165–173. [Google Scholar] [CrossRef] [PubMed]
- McAlister, F.A.; Wang, T.; Wang, X.; Chu, A.; Goodman, S.G.; van Diepen, S.; Jackevicius, C.A.; Kaul, P.; Udell, J.; Ko, D.T.; et al. Statins and SARS-CoV-2 Infection: Results of a Population-Based Prospective Cohort Study of 469,749 Adults from 2 Canadian Provinces. J. Am. Heart Assoc. 2021, 10, e022330. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szarpak, L.; Mierzejewska, M.; Jurek, J.; Kochanowska, A.; Gasecka, A.; Truszewski, Z.; Pruc, M.; Blek, N.; Rafique, Z.; Filipiak, K.J.; et al. Effect of Coronary Artery Disease on COVID-19—Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis. Biology 2022, 11, 221. https://doi.org/10.3390/biology11020221
Szarpak L, Mierzejewska M, Jurek J, Kochanowska A, Gasecka A, Truszewski Z, Pruc M, Blek N, Rafique Z, Filipiak KJ, et al. Effect of Coronary Artery Disease on COVID-19—Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis. Biology. 2022; 11(2):221. https://doi.org/10.3390/biology11020221
Chicago/Turabian StyleSzarpak, Lukasz, Malgorzata Mierzejewska, Jonasz Jurek, Anna Kochanowska, Aleksandra Gasecka, Zenon Truszewski, Michal Pruc, Natasza Blek, Zubaid Rafique, Krzysztof J. Filipiak, and et al. 2022. "Effect of Coronary Artery Disease on COVID-19—Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis" Biology 11, no. 2: 221. https://doi.org/10.3390/biology11020221