

Biomechanical Effect of Hybrid Dynamic Stabilization Implant on the Segmental Motion and Intradiscal Pressure in Human Lumbar Spine
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimen Preparation
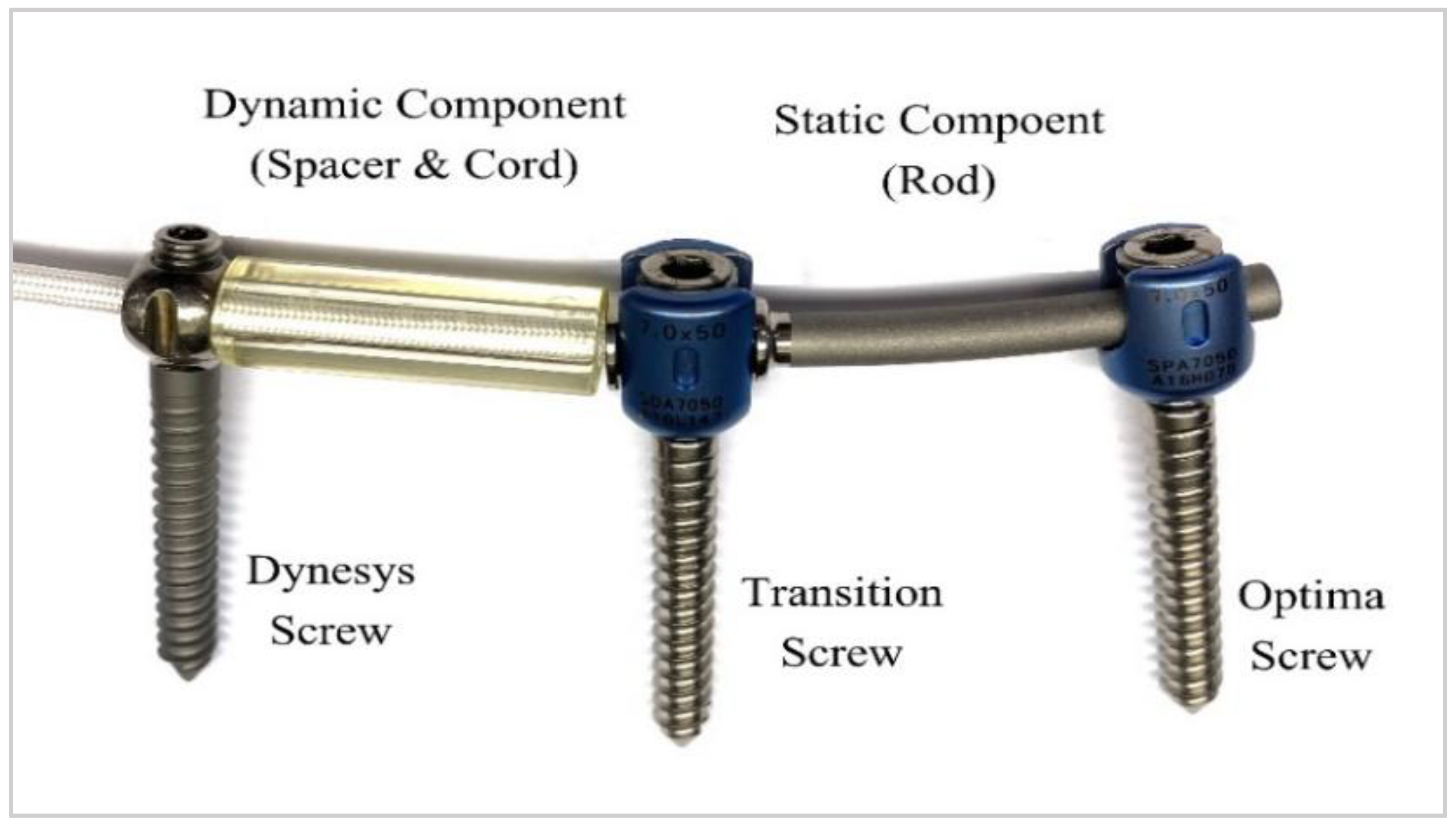
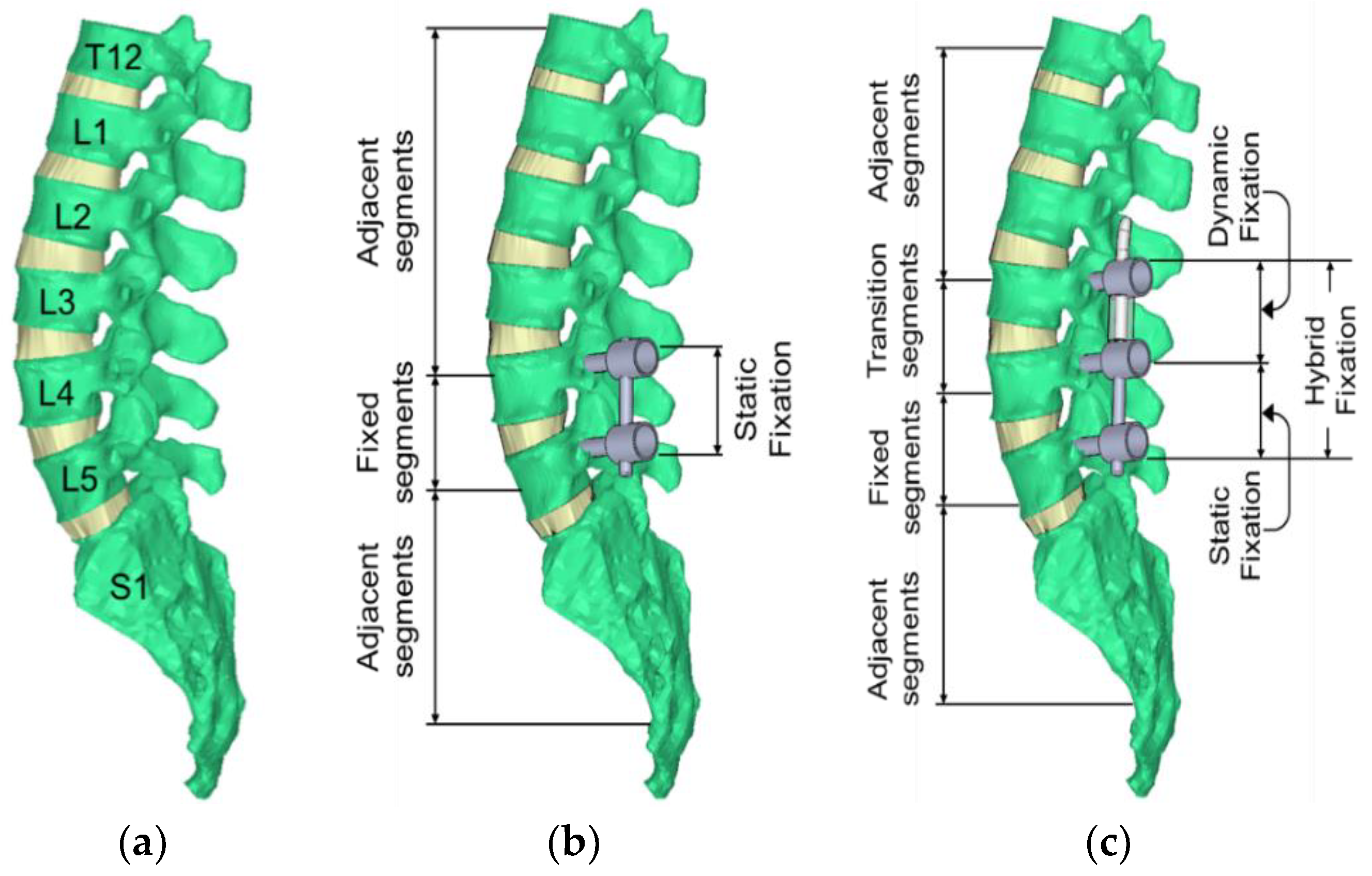
2.2. Description of Hybrid Dynamic Stabilization System and Surgical Treatment
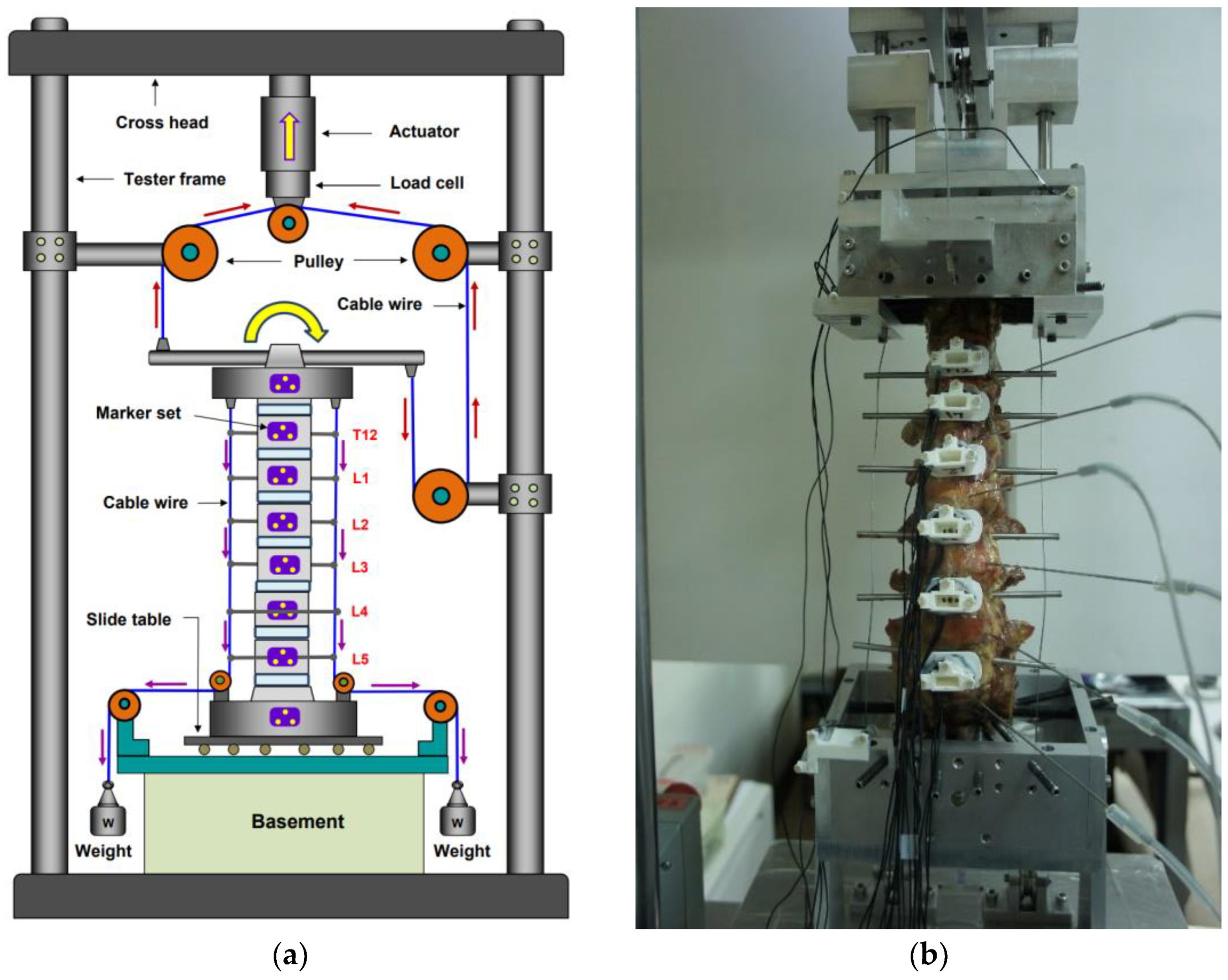
2.3. Biomechanical Test
2.4. Data and Statistical Analysis
3. Results
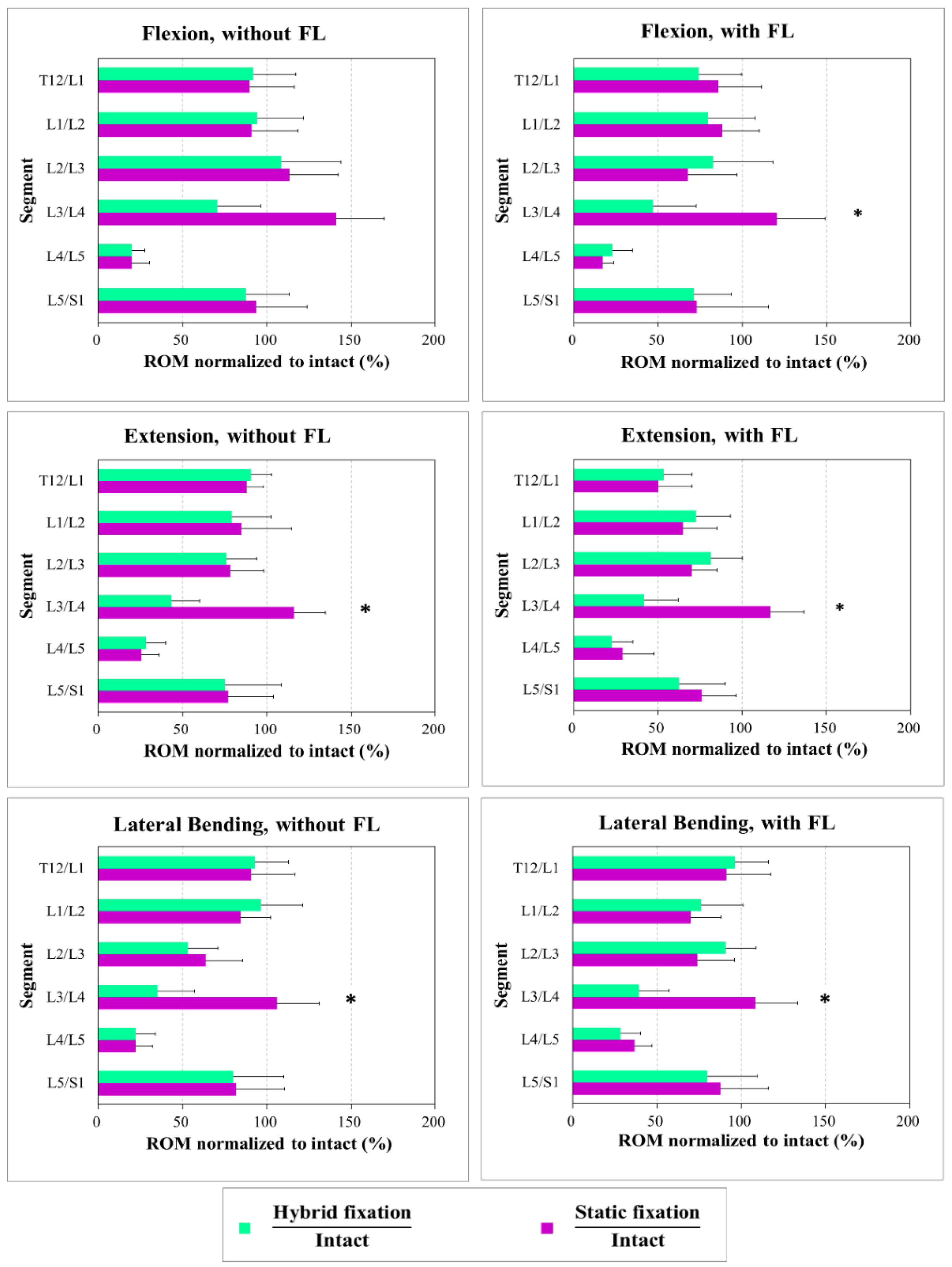
3.1. Range of Motion (ROM)
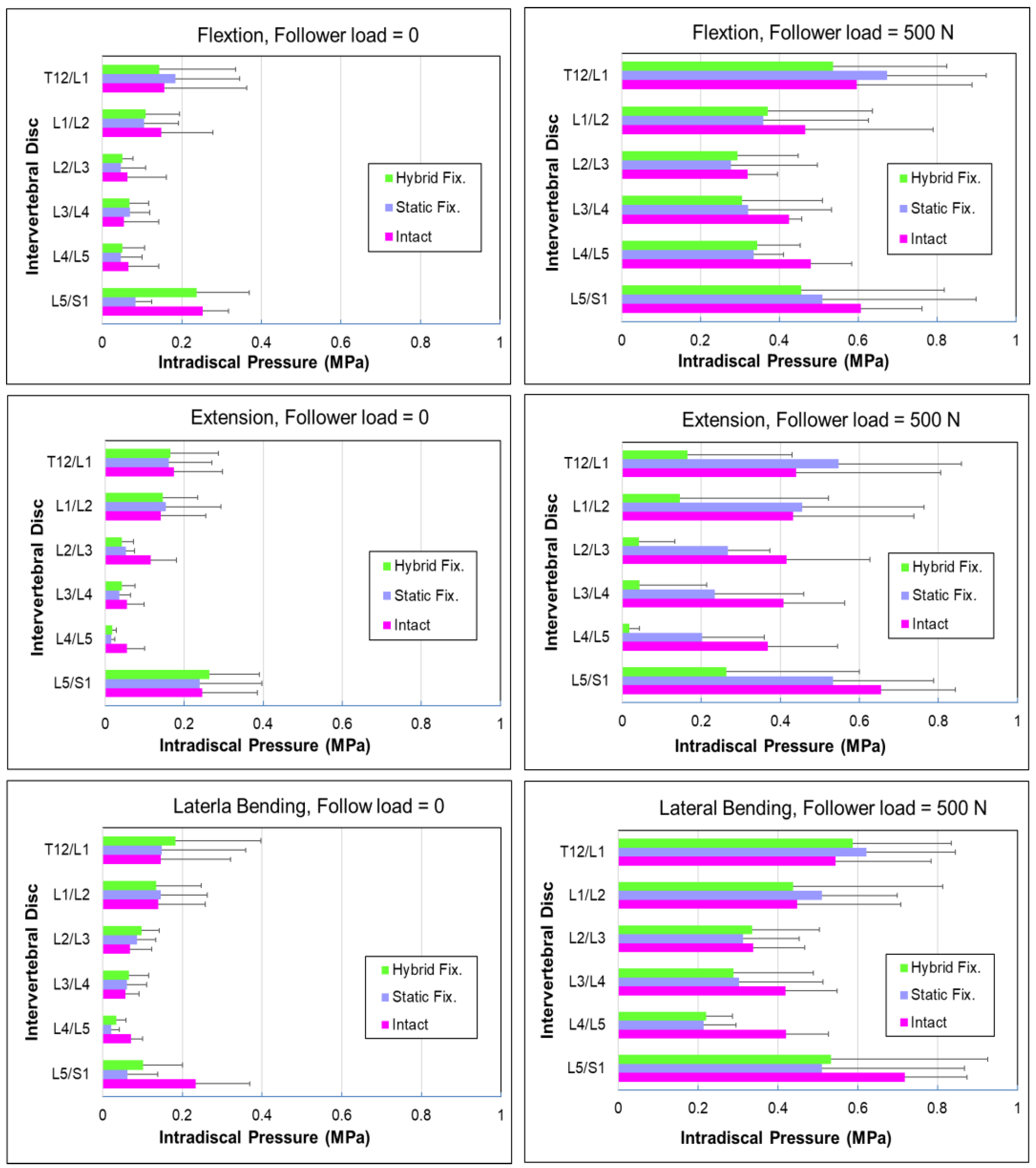
3.2. Intradiscal Pressure (IDP)
4. Discussion
4.1. Bone Quality and Loosening of Fixations
4.2. Range of Motion at the Implanted and Adjacent Levels
4.3. Effects of Follower Load on the Intradiscal Pressure (IDP)
4.4. Effects of Stiffness and Cord Tension of DTO
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghasemi, A.A. Adjacent segment degeneration after posterior lumbar fusion: An analysis of possible risk factors. Clin. Neurol. Neurosurg. 2016, 143, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Eck, J.C.; Humphreys, S.C.; Hodges, S.D. Adjacent-segment degeneration after lumbar fusion: A review of clinical, biomechanical, and radiologic studies. Am. J. Orthop. 1999, 28, 336–340. [Google Scholar] [PubMed]
- Ghiselli, G.; Wang, J.C.; Bhatia, N.N.; Hsu, W.K.; Dawson, E.G. Adjacent segment degeneration in the lumbar spine. J. Bone Jt. Surg. Am. 2004, 86, 1497–1503. [Google Scholar] [CrossRef] [PubMed]
- Hilibrand, A.S.; Robbins, M. Adjacent segment degeneration and adjacent segment disease: The consequences of spinal fusion? Spine 2004, 4, 190–194. [Google Scholar] [CrossRef]
- Lee, C.K. Accelerated degeneration of the segment adjacent to a lumbar fusion. Spine 1988, 13, 375–377. [Google Scholar] [CrossRef] [PubMed]
- Panjabi, M.M.; Henderson, G.; Abjornson, C.; Yue, J. Multidirectional testing of one- and two-level ProDisc-L versus simulated fusions. Spine 2007, 32, 1311–1319. [Google Scholar] [CrossRef]
- Huang, R.C.; Girardi, F.P.; Lim, M.R.; Cammisa, F.P., Jr. Advantages and disadvantages of nonfusion technology in spine surgery. Orthop. Clin. North Am. 2005, 36, 263–269. [Google Scholar] [CrossRef]
- Ha, K.-Y.; Seo, J.-Y.; Kwon, S.-E.; Son, I.-N.; Kim, K.-W.; Kim, Y.-H. Posterior dynamic stabilization in the treatment of degenerative lumbar stenosis: Validity of its rationale. J. Neurosurg. Spine 2013, 18, 24–31. [Google Scholar] [CrossRef]
- Hayes, M.A.; Tompkins, S.F.; Herndon, W.A.; Gruel, C.R.; Kopta, J.A.; Howard, T.C. Clinical and Radiological Evaluation of Lumbosacral Motion below Fusion Levels in Idiopathic Scoliosis. Spine 1988, 13, 1161–1167. [Google Scholar] [CrossRef]
- Chen, C.-S.; Cheng, C.-K.; Liu, C.-L. A Biomechanical Comparison of Posterolateral Fusion and Posterior Fusion in the Lumbar Spine. J. Spinal Disord. Tech. 2002, 15, 53–63. [Google Scholar] [CrossRef]
- Kim, Y.; Goel, V.K.; Weinstein, J.N.; Lim, T.-H. Effect of Disc Degeneration at One Level on the Adjacent Level in Axial Mode. Spine 1991, 16, 331–335. [Google Scholar] [CrossRef]
- Grevitt, M.P.; Gardner, A.D.H.; Spilsbury, J.; Shackleford, I.M.; Baskerville, R.; Pursell, L.M.; Hassaan, A.; Mulholland, R.C. The Graf stabilisation system: Early results in 50 patients. Eur. Spine J. 1995, 4, 169–175; discussion 135. [Google Scholar] [CrossRef] [PubMed]
- Freudiger, S.; Dubois, G.; Lorrain, M. Dynamic neutralisation of the lumbar spine confirmed on a new lumbar spine simulator in vitro. Arch. Orthop. Trauma Surg. 1999, 119, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Stoll, T.M.; Dubois, G.; Schwarzenbach, O. The dynamic neutralization system for the spine: A multi-center study of a novel non-fusion system. Eur. Spine J. 2002, 11 (Suppl. S2), S170–S178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondrashov, D.G.; Hannibal, M.; Hsu, K.Y.; Zucherman, J.F. Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: A 4-year follow-up study. J. Spinal Disord. Tech. 2006, 19, 323–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, M.; Karadimas, E.; Nicol, M.; Smith, F.W.; Wardlaw, D. Effects of X-Stop Device on Sagittal Lumbar Spine Kinematics in Spinal Stenosis. J. Spinal Disord. Tech. 2006, 19, 328–333. [Google Scholar] [CrossRef] [Green Version]
- Erbulut, D.U.; Zafarparandeh, I.; Ozer, A.F.; Goel, V.K. Biomechanics of Posterior Dynamic Stabilization Systems. Adv. Orthop. 2013, 2013, 451956. [Google Scholar] [CrossRef] [Green Version]
- Christie, S.D.; Song, J.K.; Fessler, R.G. Dynamic Interspinous Process Technology. Spine 2005, 30, S73–S78. [Google Scholar] [CrossRef]
- Boody, B.S.; Smucker, J.D.; Sasso, W.; Miller, J.W.; Snowden, R.; Sasso, R.C. Evaluation of DIAM Spinal Stabilization System for lower lumbar disc degenerative disease: A randomized, prospective, single-site study. J. Orthop. 2020, 21, 171–177. [Google Scholar] [CrossRef]
- Barrey, C.Y.; Ponnappan, R.K.; Song, J.; Vaccaro, A.R. Biomechanical evaluation of pedicle screw-based dynamic stabilization devices for the lumbar spine: A systematic review. SAS J. 2008, 2, 159–170. [Google Scholar] [CrossRef]
- Weinhoffer, S.L.; Guyer, R.D.; Herbert, M.; Griffith, S.L. Intradiscal pressure measurements above an instrumented fusion. A cadaveric study. Spine 1995, 20, 526–531. [Google Scholar] [CrossRef]
- Dubois, G.; Prere, J.; Schwarzenbach, O.; Stoll, T.M. Dynamic Neutralization: Treatment of Mobile Vertebral Instability. Spinal Restabilization Procedures; Elsevier: Amsterdam, The Netherlands, 2002; pp. 345–354. [Google Scholar]
- Prud’homme, M.; Barrios, C.; Rouch, P.; Charles, Y.P.; Steib, J.P.; Skalli, W. Clinical outcomes and complications after pedicle-anchored dynamic or hybrid lumbar spine stabilization: A Systematic literature review. J. Spinal Disord. Tech. 2015, 28, 439–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayyazi, A.H.; Ordway, N.R.; Park, S.A.; Fredrickson, B.E.; Yonemura, K.; Yuan, H.A. Radiostereometric analysis of postoperative motion after application of dryness dynamic posterior stabilization system for treatment of degenerative spondylolisthesis. J. Spinal Disord. Tech. 2010, 23, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Maserati, M.B.; Tormenti, M.J.; Panczykowski, D.M.; Bonfield, C.M.; Gerszten, P.C. The use of a hybrid dynamic stabilization and fusion system in the lumbar spine: Preliminary experience. Neurosurg. Focus 2010, 28, E2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaeren, S.; Broger, I.; Jeanneret, B. Minimum four-year follow-up of spinal stenosis with degenerative spondylolisthesis treated with decompression and dynamic stabilization. Spine 2008, 33, E636–E642. [Google Scholar] [CrossRef] [Green Version]
- Grob, D.; Benini, A.; Junge, A.; Mannion, A.F. Clinical experience with the Dynesys semi-rigid fixation system for the lumbar spine: Surgical and patient-oriented outcome in 50 cases after an average of 2 years. Spine 2005, 30, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Fay, L.Y.; Wu, J.C.; Tsai, T.Y.; Wu, C.L.; Huang, W.C.; Cheng, H. Dynamic stabilization for degenerative spondylolisthesis: Evaluation of radiographic and clinical outcomes. Clin. Neurol. Neurosurg. 2013, 115, 535–541. [Google Scholar] [CrossRef]
- Samo, K.; Fokter, S.K.; Strahovnik, A. Dynamic versus rigid stabilization for the treatment of disc degeneration in the lumbar spine. Evid. Based Spine Care J. 2011, 2, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.; Delamarter, R.; Maxwell, J.; Welch, W.; Wingate, J.; Sherman, J. Preliminary 3-year results from a prospective, randomized, controlled IDE study of the Dynesys dynamic stabilization system. Spine J. 2009, 9, 86S. [Google Scholar] [CrossRef]
- Yang, M.; Li, C.; Chen, Z.; Bai, Y.; Li, M. Short-term outcome of posterior dynamic stabilization system in degenerative lumbar diseases. Indian J. Orthop. 2014, 48, 574–581. [Google Scholar] [CrossRef]
- Mageswaran, P.; Techy, F.; Colbrunn, R.W.; Bonner, T.F.; McLain, R.F. Hybrid dynamic stabilization: A biomechanical assessment of adjacent and supra adjacent levels of the lumbar spine- Laboratory investigation. J. Neurosurg. Spine 2012, 17, 232–242. [Google Scholar] [CrossRef]
- Sengupta, D.K.; Herkowitz, H.N. Pedicle screw-based posterior dynamic stabilization: Literature review. Adv. Orthop. 2012, 2012, 424268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fay, L.Y.; Chang, C.C.; Chang, H.K.; Tu, T.H.; Tsai, T.Y.; Wu, C.L.; Huang, W.C.; Wu, J.C.; Cheng, H. A Hybrid Dynamic Stabilization and Fusion System in Multilevel Lumbar Spondylosis. Neurospine 2018, 15, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Dubois, G. Dynamic stabilization with the Dynesys® system and the dynamic transition option DTO™ implant: Philosophy—Concept—Surgical technique. Interact. Surg. 2008, 3, 239–244. [Google Scholar] [CrossRef]
- Kashkoush, A.; Agarwal, N.; Paschel, E.; Goldschmidt, E.; Gerszten, P.C. Evaluation of a Hybrid Dynamic Stabilization and Fusion System in the Lumbar Spine: A 10-Year Experience. Cureus 2016, 8, 637. [Google Scholar] [CrossRef] [Green Version]
- Herren, C.; Sobottke, R.; Pishnamaz, M.; Scheyerer, M.J.; Bredow, J.; Westermann, L.; Berger, E.M.; Oikonomidis, S.; Eysel, P.; Siewe, J. The use of the DTO™ hybrid dynamic device: A clinical outcome- and radiological-based prospective clinical trial. BMC Musculoskelet. Disord. 2018, 19, 199. [Google Scholar] [CrossRef]
- Bothmann, M.; Kast, E.; Boldt, G.J.; Oberle, J. Dynesys fixation for lumbar spine degeneration. Neurosurg. Rev. 2008, 31, 189–196. [Google Scholar] [CrossRef]
- Patwardhan, A.G.; Havey, R.M.; Meade, K.P.; Lee, B.; Dunlap, B. A follower load increases the load-carrying capacity of the lumbar spine in compression. Spine 1999, 24, 1003–1009. [Google Scholar] [CrossRef]
- Yeager, M.S.; Cook, D.J.; Cheng, B.C. In Vitro Comparison of Dynesys, PEEK, and Titanium Constructs in the Lumbar Spine. Adv. Orthop. 2015, 2015, 895931. [Google Scholar] [CrossRef] [Green Version]
- Brandon, S.; Andres, F.C.; Daniel, J.C.; Matthew, S.Y.; James, B.B.; Benjamin, W.; Boyle, C.C. Comparison of Intervertebral ROM in Multi-Level Cadaveric Lumbar Spines Using Distinct Pure Moment Loading Approaches. Int. J. Spine Surg. 2015, 9, 32. [Google Scholar]
- White, A.A.; Panjabi, M.M. Clinical biomechanics of the Spine; J.B. Lippincott Company: Philadelphia, PA, USA, 1978. [Google Scholar]
- Ko, C.C.; Tsai, H.W.; Huang, W.C.; Wu, J.C.; Chen, Y.C.; Shih, Y.H.; Chen, H.C.; Wu, C.L.; Cheng, H. Screw loosening in the Dynesys stabilization system: Radiographic evidence and effect on outcomes. Neurosurg. Focus 2010, 28, E10. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.C.; Huang, W.C.; Tsai, H.W.; Ko, C.C.; Wu, C.L.; Tu, T.H.; Cheng, H. Pedicle screw loosening in dynamic stabilization: Incidence, risk, and outcome in 126 patients. Neurosurg. Focus 2011, 31, E9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.H.; Chang, P.Y.; Tu, T.H.; Fay, L.Y.; Chang, H.K.; Wu, J.C.; Huang, W.C.; Cheng, H. The Effect of Lumbar Lordosis on Screw Loosening in Dynesys Dynamic Stabilization: Four-Year Follow-Up with Computed Tomography. Biomed. Res. Int. 2015, 2015, 152435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmoelz, W.; Huber, J.F.; Nydegger, T.; Claes, L.; Wilke, H.J. Influence of a dynamic stabilization system on load bearing of a bridged disc: An in vitro study of intradiscal pressure. Eur. Spine J. 2006, 15, 1276–1285. [Google Scholar] [CrossRef]
- Panjabi, M.M.; Oxland, T.R.; Yamamoto, T.; Crisco, J.J. Mechanical behavior of the human lumbar and lumbosacral spine as shown by three-dimensional load-displacement curves lumbosacral behavior spine of the human curves. J. Bone Jt. Surg. Am. 1994, 76, 413–424. [Google Scholar] [CrossRef]
- Park, P.; Garton, H.J.; Gala, V.C.; Hoff, J.T.; McGillicuddy, J.E. Adjacent segment disease after lumbar or lumbosacral fusion: Review of the literature. Spine 2004, 29, 1938–1944. [Google Scholar] [CrossRef]
- Aota, Y.; Kumano, K.; Hirabayashi, S. Post fusion instability at the adjacent segments after rigid pedicle screw fixation for degenerative lumbar spinal disorders. J. Spinal Disord. 1955, 8, 464–473. [Google Scholar]
- Etebar, S.; Cahill, D.W. Risk factors for adjacent-segment failure following lumbar fixation with rigid instrumentation for degenerative instability. J. Neurosurg. 1999, 90, 163–169. [Google Scholar] [CrossRef]
- Rahm, M.D.; Hall, B.B. Adjacent-segment degeneration after lumbar fusion with instrumentation: A retrospective study. J. Spinal Disord. 1996, 9, 392–400. [Google Scholar] [CrossRef]
- Kumar, M.N.; Jacquot, F.; Hall, H. Long-term follow-up of functional outcomes and radiographic changes at adjacent levels following lumbar spine fusion for degenerative disc disease. Eur. Spine J. 2001, 10, 309–313. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Lee, J.; Song, H. The impact of adjacent segment degeneration on the clinical outcome after lumbar spinal fusion. Spine 2008, 33, 503–507. [Google Scholar] [CrossRef]
- Schlegel, J.D.; Smith, J.A.; Schleusener, R.L. Lumbar motion segment pathology adjacent to thoracolumbar, lumbar, and lumbosacral fusions. Spine 1996, 21, 970–981. [Google Scholar] [CrossRef]
- Schmoelz, W.; Huber, J.F.; Nydegger, T.; Dipl-Ing; Claes, L.; Wilke, H.J. Dynamic stabilization of the lumbar spine and its effects on adjacent segments: An in vitro experiment. J. Spinal Disord. Tech. 2003, 16, 418–423. [Google Scholar] [CrossRef]
- Vaga, S.; Brayda-Bruno, M.; Perona, F.; Fornari, M.; Raimondi, M.T.; Petruzzi, M.; Grava, G.; Costa, F.; Caiani, E.G.; Lamartina, C. Molecular MR imaging for the evaluation of the effect of dynamic stabilization on lumbar intervertebral discs. Eur. Spine J. 2009, 18, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Broberg, K.B. Slow deformation of intervertebral discs. J. Biomech. 1993, 26, 501–512. [Google Scholar] [CrossRef]
- McGill, S.M.; Brown, S. Creep response of the lumbar spine to prolonged full flexion. Biomech 1992, 7, 43–46. [Google Scholar] [CrossRef]
- Thornton, G.M.; Oliynyk, A.; Frank, C.B.; Shrive, N.G. Ligament creep cannot be predicted from stress relaxation at low stress: A biomechanical study of the rabbit medial collateral ligament. J. Orthop. Res. 1997, 15, 652–656. [Google Scholar] [CrossRef]
- Frank, C.B.; Hart, D.A.; Shrive, N.G. Molecular biology and biomechanics of normal and healing ligaments—A review. Osteoarthr. Cartil. 1999, 7, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Jahng, T.A.; Kim, Y.E.; Moon, K.Y. Comparison of the biomechanical effect of pedicle-based dynamic stabilization: A study using finite element analysis. Spine J. 2013, 13, 85–94. [Google Scholar] [CrossRef]
- Atiq, D.; Viral, J.; Rasesh, D.; Brandon, B.; Aditya, I.; Aditya, M.; Mark, M.; Saif, K. Could Junctional Problems at the End of a Long Construct be Addressed by Providing a Graduated Reduction in Stiffness? A Biomechanical Investigation. Spine. 2012, 37, 16–22. [Google Scholar]
- Niosi, C.A.; Zhu, Q.A.; Wilson, D.C.; Keynan, O.; Wilson, D.R.; Oxland, T.R. Biomechanical characterization of the three-dimensional kinematic behaviour of the Dynesys dynamic stabilization system: An in vitro study. Eur. Spine J. 2006, 15, 913–922. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discal Level | Intact Without Implanted ∆IDP (MPa) | Fusion L4/5 (Static) ∆IDP (MPa) | Hybrid L3/4 (Dynamic) + L4/5 (Static) ∆IDP (MPa) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Flexion | Extension | Lateral Bending | Flexion | Extension | Lateral Bending | Flexion | Extension | Lateral Bending | |
| T12/L1 | 0.440 | 0.266 | 0.399 | 0.490 | 0.385 | 0.474 | 0.393 | 0.383 | 0.405 |
| L1/2 | 0.318 | 0.291 | 0.309 | 0.253 | 0.301 | 0.365 | 0.262 | 0.287 | 0.304 |
| L2/3 | 0.256 | 0.301 | 0.270 | 0.230 | 0.266 | 0.226 | 0.243 | 0.232 | 0.237 |
| L3/4 | 0.371 | 0.352 | 0.361 | 0.251 | 0.292 | 0.302 | 0.088 | 0.069 | 0.070 |
| L4/5 | 0.405 | 0.383 | 0.370 | 0.087 | 0.076 | 0.091 | 0.093 | 0.080 | 0.085 |
| L5/S1 | 0.394 | 0.409 | 0.429 | 0.425 | 0.333 | 0.448 | 0.219 | 0.299 | 0.432 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, C.-K.; Tsai, Y.-J.; Yen, C.-Y.; Li, Y.-C.; Hsiao, H.-Y.; Tu, Y.-K. Biomechanical Effect of Hybrid Dynamic Stabilization Implant on the Segmental Motion and Intradiscal Pressure in Human Lumbar Spine. Bioengineering 2023, 10, 31. https://doi.org/10.3390/bioengineering10010031
Hsiao C-K, Tsai Y-J, Yen C-Y, Li Y-C, Hsiao H-Y, Tu Y-K. Biomechanical Effect of Hybrid Dynamic Stabilization Implant on the Segmental Motion and Intradiscal Pressure in Human Lumbar Spine. Bioengineering. 2023; 10(1):31. https://doi.org/10.3390/bioengineering10010031
Chicago/Turabian StyleHsiao, Chih-Kun, Yi-Jung Tsai, Cheng-Yo Yen, Yi-Chen Li, Hao-Yuan Hsiao, and Yuan-Kun Tu. 2023. "Biomechanical Effect of Hybrid Dynamic Stabilization Implant on the Segmental Motion and Intradiscal Pressure in Human Lumbar Spine" Bioengineering 10, no. 1: 31. https://doi.org/10.3390/bioengineering10010031