
An Accurate Multiple Sclerosis Detection Model Based on Exemplar Multiple Parameters Local Phase Quantization: ExMPLPQ

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
- A prospective brain MRI dataset was collected to train and test the proposed ExMPLPQ model. The dataset has been made publicly available.
- The handcrafted ExMPLPQ model attained over 97% classification accuracy on the study dataset. In addition, our results for MS detection were demonstrably superior to 19 state-of-the-art pretrained methods, which included transfer learning and deep learning models.
2. Materials and Methods
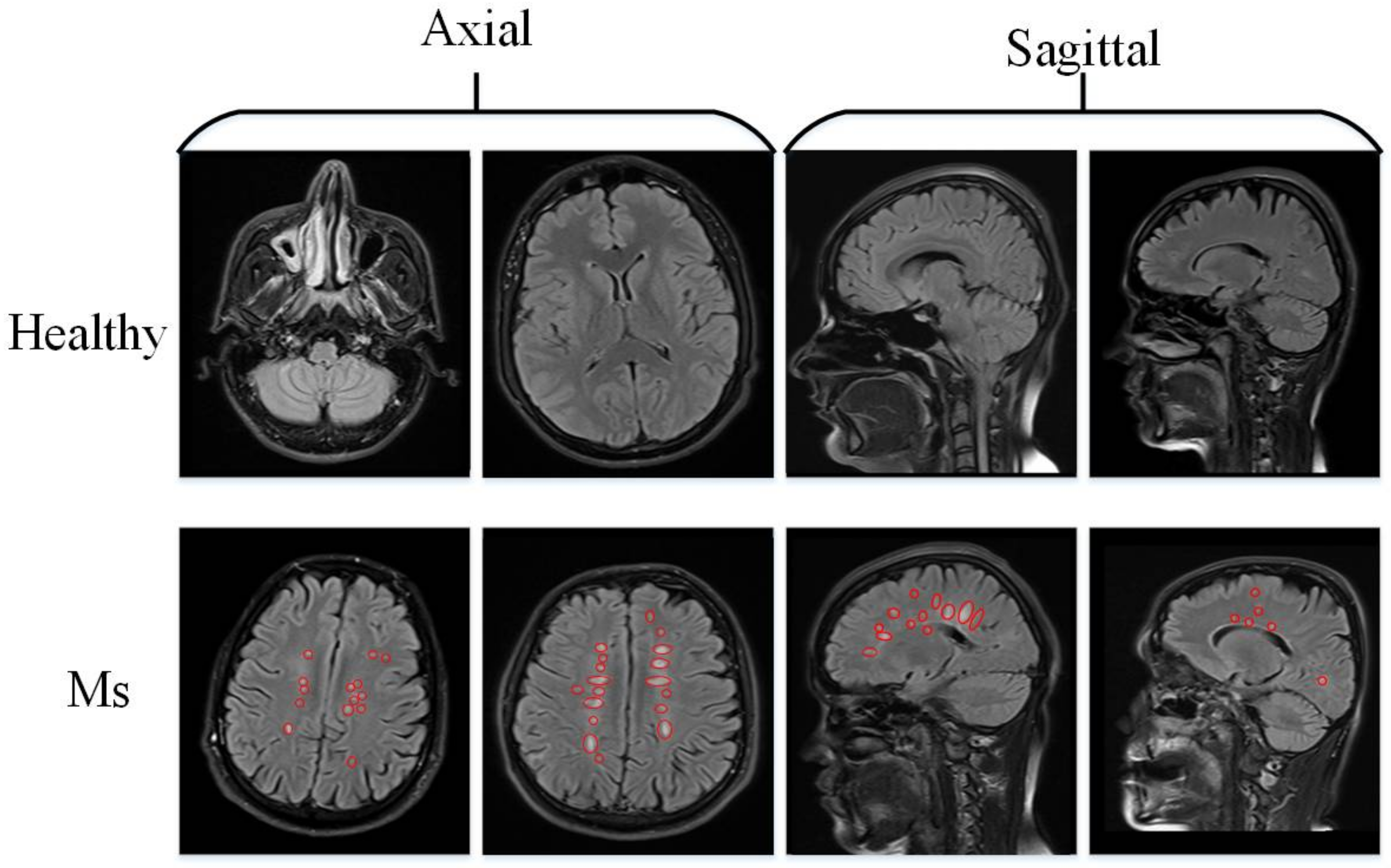
2.1. Materials
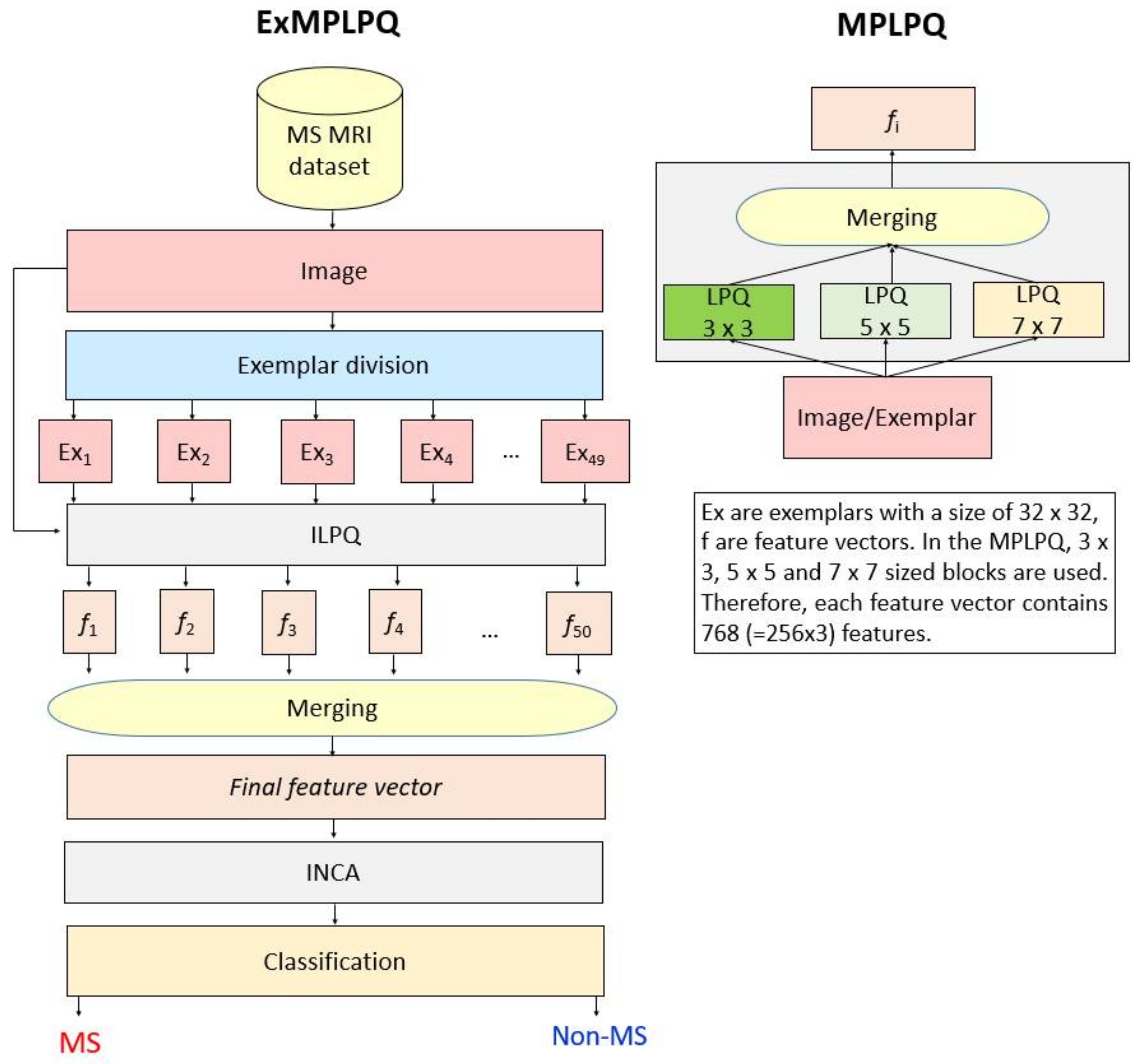
2.2. Transfer Learning-Based Feature Engineering Model
| Algorithm 1. Detailed flow of the ExMPLPQ technique |
| Input: The used MS dataset with 3.427 MRIs. |
| Output: Results. |
| 00: Load MS dataset |
| 01: for k = 1 to 3427 do |
| 02: I = MS(k); Image reading from MS dataset |
| 03: Reshape image into 224 × 224 sized image |
| 04: X(k,1:768) = [lpq(I,3) lpq(I,5) lpq(I,7)] |
| 05: for i = 1 to 224 step by 32 do |
| 06: for j = 1 to 224 step by 32 do |
| 07: exm = res(i:i+31,j:j+31,1) |
| 08: X(k, counter * 768+1:(counter+1) * 768) = [lpq(exm,3) lpq(exm,5) lpq(exm,7)] |
| 09: end for j |
| 10: end for i |
| 11: Extract the 50th feature vector using the resized images. |
| 12: Merge the generated feature vectors to create the final feature vector. |
| 13: end for k |
| 14: Apply INCA to generated features. |
| 15: Forward the selected features to kNN classifiers. |
| 16: Obtain predict values |
3. Performance Analysis
4. Results
5. Discussion
- A new brain MRI dataset comprising three study data subsets was prospectively acquired to train and test the model. This dataset has been made publicly available.
- By design, the ExMPLPQ model exploited the advantages of both exemplar and multiple parameters for feature extraction.
- The best features were automatically selected for each of the three binary classification problems using INCA.
- ExMPLPQ attained over 97% accuracies for all study data subsets.
- ExMPLPQ attained better classification performance compared with 19-pre-trained CNNs. Of note, more than a million parameters were required to be assigned/optimized using the deep learning models, which increased their time complexity considerably.
- The ExMPLPQ algorithm has a low time complexity of approximately .
- The base architecture of ExMPLPQ is parametric and is amenable to modification and optimization to create new models using variable patch sizes and updating of feature extractors, feature selectors, and classifiers.
- The dataset was new, which precluded direct comparison with extant methods in the literature. Nevertheless, the common dataset was used to test the ExMPLPQ model and 19 comparator deep learning techniques, which demonstrated superior results for our model.
- Only MS patients admitted to one hospital during one year (2021) were included in the study.
- Patients with less than 9 MS lesions on brain MRIs were excluded from the study.
- Patients with poor MRI image quality and motion artifacts were excluded from the study.
- Patients under 18 years of age were excluded from the study.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garg, N.; Smith, T.W. An update on immunopathogenesis, diagnosis, and treatment of multiple sclerosis. Brain Behav. 2015, 5, e00362. [Google Scholar] [CrossRef] [PubMed]
- Mult Scler, J. Multiple sclerosis under the spotlight. Lancet Neurol. 2021, 20, 497. [Google Scholar]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Nicholas, R.S.; Heaven, M.L.; Middleton, R.M.; Chevli, M.; Pulikottil-Jacob, R.; Jones, K.H.; Ford, D.V. Personal and societal costs of multiple sclerosis in the UK: A population-based MS Registry study. Mult. Scler. J. Exp. Transl. Clin. 2020, 6, 2055217320901727. [Google Scholar] [CrossRef]
- Dahham, J.; Rizk, R.; Kremer, I.; Evers, S.M.; Hiligsmann, M. Economic burden of multiple sclerosis in low-and middle-income countries: A systematic review. Pharmacoeconomics 2021, 39, 789–807. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and treatment of multiple sclerosis: A review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Vargas, D.L.; Tyor, W.R. Update on disease-modifying therapies for multiple sclerosis. J. Investig. Med. 2017, 65, 883–891. [Google Scholar] [CrossRef]
- Noyes, K.; Bajorska, A.; Chappel, A.; Schwid, S.; Mehta, L.; Weinstock-Guttman, B.; Holloway, R.; Dick, A. Cost-effectiveness of disease-modifying therapy for multiple sclerosis: A population-based study. Neurology 2011, 77, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Rovira, À.; León, A. MR in the diagnosis and monitoring of multiple sclerosis: An overview. Eur. J. Radiol. 2008, 67, 409–414. [Google Scholar] [CrossRef]
- De Stefano, N.; Matthews, P.M.; Antel, J.P.; Preul, M.; Francis, G.; Arnold, D.L. Chemical pathology of acute demyelinating lesions and its correlation with disability. Ann. Neurol. 1995, 38, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Filippi, M.; Preziosa, P.; Banwell, B.L.; Barkhof, F.; Ciccarelli, O.; De Stefano, N.; Geurts, J.J.; Paul, F.; Reich, D.S.; Toosy, A.T. Assessment of lesions on magnetic resonance imaging in multiple sclerosis: Practical guidelines. Brain 2019, 142, 1858–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sati, P.; George, I.C.; Shea, C.D.; Gaitán, M.I.; Reich, D.S. FLAIR*: A combined MR contrast technique for visualizing white matter lesions and parenchymal veins. Radiology 2012, 265, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Rolak, L.A.; Fleming, J.O. The differential diagnosis of multiple sclerosis. Neurologist 2007, 13, 57–72. [Google Scholar] [CrossRef] [PubMed]
- Mader, I.; Rauer, S.; Gall, P.; Klose, U. 1H MR spectroscopy of inflammation, infection and ischemia of the brain. Eur. J. Radiol. 2008, 67, 250–257. [Google Scholar] [CrossRef]
- Morgen, K.; McFarland, H.F.; Pillemer, S.R. Central nervous system disease in primary Sjögren’s syndrome: The role of magnetic resonance imaging. Semin. Arthritis Rheum. 2004, 34, 623–630. [Google Scholar] [CrossRef]
- Shoeibi, A.; Khodatars, M.; Jafari, M.; Moridian, P.; Rezaei, M.; Alizadehsani, R.; Khozeimeh, F.; Gorriz, J.M.; Heras, J.; Panahiazar, M.; et al. Applications of deep learning techniques for automated multiple sclerosis detection using magnetic resonance imaging: A review. Comput. Biol. Med. 2021, 136, 104697. [Google Scholar] [CrossRef]
- Ranschaert, E.R.; Morozov, S.; Algra, P.R. Artificial Intelligence in Medical Imaging: Opportunities, Applications and Risks; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Schwab, P.; Karlen, W. A deep learning approach to diagnosing multiple sclerosis from smartphone data. IEEE J. Biomed. Health Inform. 2020, 25, 1284–1291. [Google Scholar] [CrossRef]
- Tousignant, A.; Lemaître, P.; Precup, D.; Arnold, D.L.; Arbel, T. Prediction of disease progression in multiple sclerosis patients using deep learning analysis of MRI data. In Proceedings of the International Conference on Medical Imaging with Deep Learning, Lübeck, Germany, 7–9 July 2021; pp. 483–492. [Google Scholar]
- Storelli, L.; Azzimonti, M.; Gueye, M.; Vizzino, C.; Preziosa, P.; Tedeschi, G.; De Stefano, N.; Pantano, P.; Filippi, M.; Rocca, M.A. A Deep Learning Approach to Predicting Disease Progression in Multiple Sclerosis Using Magnetic Resonance Imaging. Investig. Radiol. 2022. [Google Scholar] [CrossRef]
- Alijamaat, A.; NikravanShalmani, A.; Bayat, P. Multiple sclerosis identification in brain MRI images using wavelet convolutional neural networks. Int. J. Imaging Syst. Technol. 2021, 31, 778–785. [Google Scholar] [CrossRef]
- De Oliveira, M.; Piacenti-Silva, M.; Rocha, F.C.G.d.; Santos, J.M.; Cardoso, J.d.S.; Lisboa-Filho, P.N. Lesion Volume Quantification Using Two Convolutional Neural Networks in MRIs of Multiple Sclerosis Patients. Diagnostics 2022, 12, 230. [Google Scholar] [CrossRef] [PubMed]
- Narayana, P.A.; Coronado, I.; Sujit, S.J.; Wolinsky, J.S.; Lublin, F.D.; Gabr, R.E. Deep learning for predicting enhancing lesions in multiple sclerosis from noncontrast MRI. Radiology 2020, 294, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Barquero, G.; La Rosa, F.; Kebiri, H.; Lu, P.-J.; Rahmanzadeh, R.; Weigel, M.; Fartaria, M.J.; Kober, T.; Théaudin, M.; Du Pasquier, R. RimNet: A deep 3D multimodal MRI architecture for paramagnetic rim lesion assessment in multiple sclerosis. NeuroImage Clin. 2020, 28, 102412. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; George, A.; Wu, A.T.; Niu, X.; Lin, J.; Adusumilli, G.; Naismith, R.T.; Cross, A.H.; Sun, P.; Song, S.K. Deep learning with diffusion basis spectrum imaging for classification of multiple sclerosis lesions. Ann. Clin. Transl. Neurol. 2020, 7, 695–706. [Google Scholar] [CrossRef] [Green Version]
- Vogelsanger, C.; Federau, C. Latent space analysis of vae and intro-vae applied to 3-dimensional mr brain volumes of multiple sclerosis, leukoencephalopathy, and healthy patients. arXiv 2021, arXiv:2101.06772. [Google Scholar]
- Shrwan, R.; Gupta, A. Classification of Pituitary Tumor and Multiple Sclerosis Brain Lesions through Convolutional Neural Networks. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1049, 012014. [Google Scholar] [CrossRef]
- Afzal, H.R.; Luo, S.; Ramadan, S.; Lechner-Scott, J.; Amin, M.R.; Li, J.; Afzal, M.K. Automatic and robust segmentation of multiple sclerosis lesions with convolutional neural networks. Comput. Mater. Contin. 2021, 66, 977–991. [Google Scholar] [CrossRef]
- Afzal, H.R.; Luo, S.; Ramadan, S.; Lechner-Scott, J.; Li, J. Automatic prediction of the conversion of clinically isolated syndrome to multiple sclerosis using deep learning. In Proceedings of the 2018 the 2nd International Conference on Video and Image Processing, Hong Kong, China, 29–31 December 2018; pp. 231–235. [Google Scholar]
- Rahtu, E.; Heikkilä, J.; Ojansivu, V.; Ahonen, T. Local phase quantization for blur-insensitive image analysis. Image Vis. Comput. 2012, 30, 501–512. [Google Scholar] [CrossRef]
- Peterson, L.E. K-nearest neighbor. Scholarpedia 2009, 4, 1883. [Google Scholar] [CrossRef]
- Goldberger, J.; Hinton, G.E.; Roweis, S.; Salakhutdinov, R.R. Neighbourhood components analysis. Adv. Neural Inf. Process. Syst. 2004, 17, 513–520. [Google Scholar]
- Xu, Y.; Zhu, Q.; Fan, Z.; Qiu, M.; Chen, Y.; Liu, H. Coarse to fine K nearest neighbor classifier. Pattern Recognit. Lett. 2013, 34, 980–986. [Google Scholar] [CrossRef]
- Powers, D.M. Evaluation: From precision, recall and F-measure to ROC, informedness, markedness and correlation. arXiv 2020, arXiv:2010.16061. [Google Scholar]
- Warrens, M.J. On the equivalence of Cohen’s kappa and the Hubert-Arabie adjusted Rand index. J. Classif. 2008, 25, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Bengio, Y.; Goodfellow, I.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2017; Volume 1. [Google Scholar]
- Faust, O.; Hagiwara, Y.; Hong, T.J.; Lih, O.S.; Acharya, U.R. Deep learning for healthcare applications based on physiological signals: A review. Comput. Methods Programs Biomed. 2018, 161, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kora, P.; Ooi, C.P.; Faust, O.; Raghavendra, U.; Gudigar, A.; Chan, W.Y.; Meenakshi, K.; Swaraja, K.; Plawiak, P.; Acharya, U.R. Transfer learning techniques for medical image analysis: A review. Biocybern. Biomed. Eng. 2021, 42, 79–107. [Google Scholar] [CrossRef]
- Barbedo, J.G.A. Impact of dataset size and variety on the effectiveness of deep learning and transfer learning for plant disease classification. Comput. Electron. Agric. 2018, 153, 46–53. [Google Scholar] [CrossRef]
- Cao, C.; Liu, F.; Tan, H.; Song, D.; Shu, W.; Li, W.; Zhou, Y.; Bo, X.; Xie, Z. Deep learning and its applications in biomedicine. Genom. Proteom. Bioinform. 2018, 16, 17–32. [Google Scholar] [CrossRef]
- Key, S.; Baygin, M.; Demir, S.; Dogan, S.; Tuncer, T. Meniscal Tear and ACL Injury Detection Model Based on AlexNet and Iterative ReliefF. J. Digit. Imaging 2022, 35, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Demir, F.; Taşcı, B. An Effective and Robust Approach Based on R-CNN+ LSTM Model and NCAR Feature Selection for Ophthalmological Disease Detection from Fundus Images. J. Pers. Med. 2021, 11, 1276. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Redmon, J.; Farhadi, A. YOLO9000: Better, faster, stronger. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 6517–6525. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning transferable architectures for scalable image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 8697–8710. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–10 February 2017; pp. 4278–4284. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 84–90. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, X.; Lin, M.; Sun, J. Shufflenet: An extremely efficient convolutional neural network for mobile devices. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 6848–6856. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18-23 June 2018; pp. 4510–4520. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50× fewer parameters and <0.5 MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 9–15 June 2019; pp. 6105–6114. [Google Scholar]
- Wang, S.-H.; Tang, C.; Sun, J.; Yang, J.; Huang, C.; Phillips, P.; Zhang, Y.-D. Multiple sclerosis identification by 14-layer convolutional neural network with batch normalization, dropout, and stochastic pooling. Front. Neurosci. 2018, 12, 818. [Google Scholar] [CrossRef]
- Plati, D.; Tripoliti, E.; Zelilidou, S.; Vlachos, K.; Konitsiotis, S.; Fotiadis, D.I. Multiple Sclerosis Severity Estimation and Progression Prediction Based on Machine Learning Techniques. In Proceedings of the 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society, Glasgow, Scotland, UK, 11–15 July 2022. [Google Scholar]
- Eitel, F.; Soehler, E.; Bellmann-Strobl, J.; Brandt, A.U.; Ruprecht, K.; Giess, R.M.; Kuchling, J.; Asseyer, S.; Weygandt, M.; Haynes, J.-D. Uncovering convolutional neural network decisions for diagnosing multiple sclerosis on conventional MRI using layer-wise relevance propagation. NeuroImage Clin. 2019, 24, 102003. [Google Scholar] [CrossRef]
- Calimeri, F.; Marzullo, A.; Stamile, C.; Terracina, G. Graph based neural networks for automatic classification of multiple sclerosis clinical courses. In Proceedings of the ESANN, Bruges, Belgium, 25–27 April 2018. [Google Scholar]
- Marzullo, A.; Kocevar, G.; Stamile, C.; Durand-Dubief, F.; Terracina, G.; Calimeri, F.; Sappey-Marinier, D. Classification of multiple sclerosis clinical profiles via graph convolutional neural networks. Front. Neurosci. 2019, 13, 594. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Male, n | Female, n | Total, n | Age, Years | Number of MRI Images, n | |
|---|---|---|---|---|---|
| MS-Axial | 21 | 51 | 72 | 28.4 ± 5.66 | 650 |
| MS-Sagittal | 21 | 51 | 72 | 28.4 ± 5.66 | 761 |
| Healthy-Axial | 27 * | 30 * | 57 * | 29.5 ± 8.32 | 1002 |
| Healthy-Sagittal | 29 * | 20 * | 49 * | 27.4 ± 6.48 | 1014 |
| Step | Parameter |
|---|---|
| Exemplar division | 32 × 32 sized patches have been used. To generate features from local areas. |
| LPQ | This step was used to extract textural features with variable parameters (we have used 3, 5, and 7 parameters). Therefore, this feature extractor is named MPLPQ. The prime purpose of this feature extractor is to use the effectiveness of the LPQ by using variable parameters. |
| Feature concatenation | The proposed model extracts 768 features from each patch and raw image. In our architecture, 50 (=49 + 1) feature vectors have been created, and each feature vector has 768 features. Therefore, the created feature vector has 38,400 (=768 × 50) features. |
| INCA | Loop range: from 100 to 1000 Loss vector: kNN |
| Classification using kNN | k: 1 Distance: Spearman Voting: None |
| Data Subset | Accuracy | Sensitivity | Specificity | Precision | F-Score | MCC |
|---|---|---|---|---|---|---|
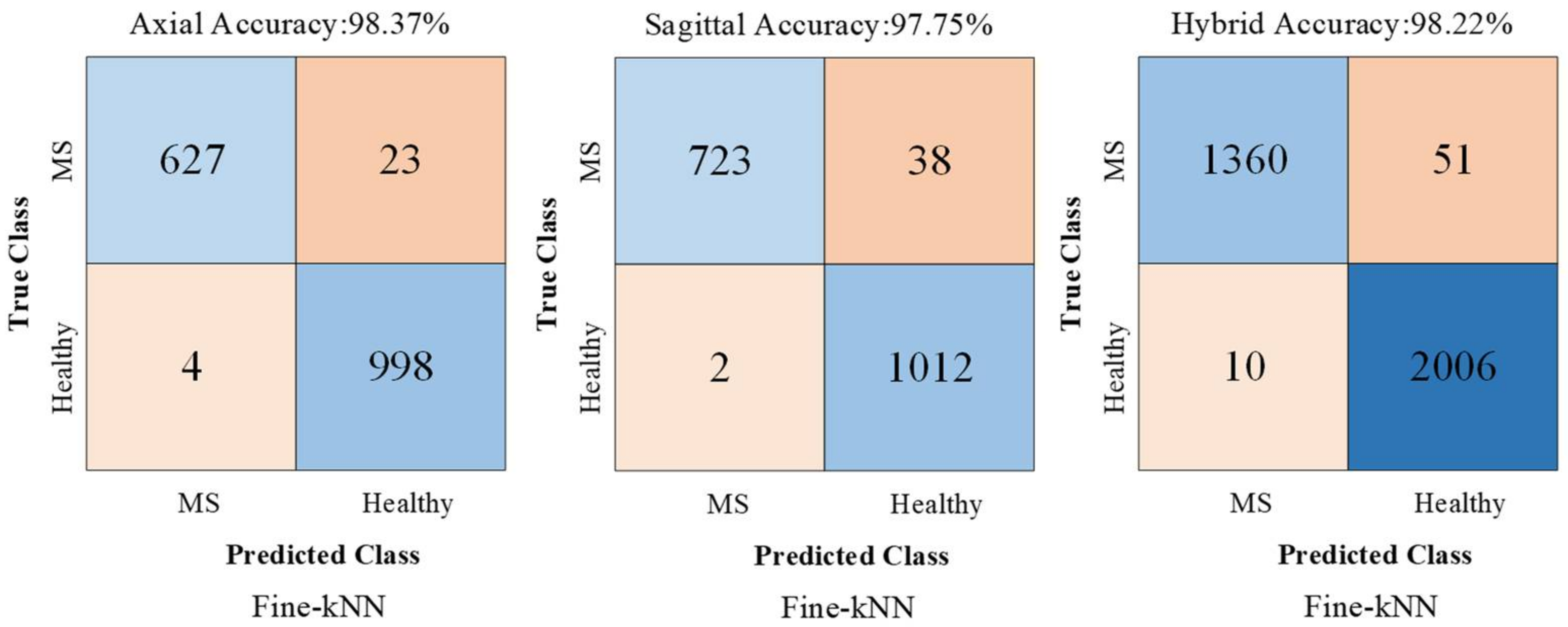
| Axial | 98.37 | 96.46 | 99.60 | 99.37 | 97.89 | 96.59 |
| Sagittal | 97.75 | 95.01 | 99.80 | 99.72 | 97.31 | 95.46 |
| Hybrid | 98.22 | 96.39 | 99.50 | 99.27 | 97.81 | 96.34 |
| Data Subset | Accuracy | Sensitivity | Specificity | Precision | F-Score | MCC |
|---|---|---|---|---|---|---|
| Axial | 98.35 ± 0.02 | 96.45 ± 0.03 | 99.59 ± 0.01 | 99.36 ± 0.02 | 97.88 ± 0.02 | 96.58 ± 0.04 |
| Sagittal | 97.74 ± 0.019 | 95.00 ± 0.044 | 99.79 ± 0.054 | 99.71 ± 0.075 | 97.30 ± 0.024 | 95.45 ± 0.03 |
| Hybrid | 98.20 ± 0.06 | 96.38 ± 0.06 | 99.49 ± 0.06 | 99.26 ± 0.04 | 97.80 ± 0.05 | 96.32 ± 0.012 |
| Number | Pre-Trained Model | Axial Accuracy | Sagittal Accuracy | Hybrid Accuracy |
|---|---|---|---|---|
| 1 | GoogleNet [44] | 84.49 ± 0.53 | 82.02 ± 0.58 | 85.62 ± 0.35 |
| 2 | DarkNet53 [45] | 87.79 ± 0.47 | 86.49 ± 0.63 | 88.02 ± 0.32 |
| 3 | Inceptionv3 [46] | 89.06 ± 0.48 | 82.47 ± 0.62 | 88.19 ± 0.33 |
| 4 | NasnetLarge [47] | 86.20 ± 0.41 | 81.63 ± 0.52 | 88.22 ± 0.30 |
| 5 | NasnetMobile [47] | 87.48 ± 0.34 | 82.41 ± 0.56 | 88.56 ± 0.30 |
| 6 | VGG19 [48] | 87.80 ± 0.60 | 83.03 ± 0.56 | 88.58 ± 0.37 |
| 7 | VGG16 [48] | 88.54 ± 0.45 | 84.78 ± 0.54 | 88.79 ± 0.31 |
| 8 | Resnet101 [49] | 88.76 ± 0.47 | 85.86 ± 0.51 | 88.90 ± 0.32 |
| 9 | Inceptionresnetv2 [50] | 90.10 ± 0.38 | 84.18 ± 0.55 | 89.42 ± 0.27 |
| 10 | AlexNet [51] | 87.38 ± 0.57 | 84.57 ± 0.51 | 89.77 ± 0.34 |
| 11 | ShuffleNet [52] | 90.25 ± 0.54 | 86.25 ± 0.54 | 90.12 ± 0.35 |
| 12 | Resnet50 [49] | 90.81 ± 0.51 | 88.33 ± 0.46 | 90.15 ± 0.35 |
| 13 | Xception [53] | 91.35 ± 0.44 | 86.15 ± 0.51 | 90.24 ± 0.28 |
| 14 | Resnet18 [49] | 91.50 ± 0.42 | 85.77 ± 0.48 | 90.45 ± 0.32 |
| 15 | Darknet19 [45] | 89.90 ± 0.51 | 85.61 ± 0.54 | 90.57 ± 0.31 |
| 16 | MobileVnet2 [54] | 91.08 ± 0.46 | 85.70 ± 0.50 | 91.15 ± 0.31 |
| 17 | DenseNet201 [55] | 91.88 ± 0.53 | 87.75 ± 0.50 | 91.81 ± 0.30 |
| 18 | SqueezeNet [56] | 90.76 ± 0.53 | 86.42 ± 0.49 | 91.89 ± 0.32 |
| 19 | Efficient b0 [57] | 93.69 ± 0.45 | 90.26 ± 0.39 | 93.22 ± 0.28 |
| Study | Method | Dataset | Subjects | Results, % |
|---|---|---|---|---|
| Plati et al. [59] | Typographic error-based feature extraction, oversampling based feature selection and classification | 78 records, 51 with EDSS 0–3.5, 18 with EDSS 4.0–5.0, 10 with EDSS 5.5–10.0 | 30 MS | Accuracy 94.87, *TP rate for low class 90.40, *TP rate for medium-class 94.20, *TP rate for high class 100.00 |
| Wang et al. [58] | CNN with 14 layers | eHealth Lab and clinic | 38 MS, 26 healthy | Accuracy 98.77, Sensitivity 98.77, Specificity 98.76 |
| Eitel et al. [60] | CNN pretrained on Alzheimer’s neuroimaging initiative dataset | Clinic | 76 MS, 71 healthy | Accuracy 87.04, AUC 96.08 |
| Calimeri et al. [61] | Graph neural network | Clinic | 90 MS | Specificity 82, F1-Score 80 |
| Marzullo [62] | Graph CNN | Clinic | 90 MS | Specificity 92, F1-Score 92 |
| Our model | ExMPLPQ | Clinic | 72 MS, 59 healthy | Axial: Accuracy 98.37, Sensitivity 96.46, Specificity 99.60 Sagittal: Accuracy 97.75, Sensitivity 95.01. Specificity 99.80 Hybrid: Accuracy 98.22, Sensitivity 96.39, Specificity 99.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macin, G.; Tasci, B.; Tasci, I.; Faust, O.; Barua, P.D.; Dogan, S.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. An Accurate Multiple Sclerosis Detection Model Based on Exemplar Multiple Parameters Local Phase Quantization: ExMPLPQ. Appl. Sci. 2022, 12, 4920. https://doi.org/10.3390/app12104920
Macin G, Tasci B, Tasci I, Faust O, Barua PD, Dogan S, Tuncer T, Tan R-S, Acharya UR. An Accurate Multiple Sclerosis Detection Model Based on Exemplar Multiple Parameters Local Phase Quantization: ExMPLPQ. Applied Sciences. 2022; 12(10):4920. https://doi.org/10.3390/app12104920
Chicago/Turabian StyleMacin, Gulay, Burak Tasci, Irem Tasci, Oliver Faust, Prabal Datta Barua, Sengul Dogan, Turker Tuncer, Ru-San Tan, and U. Rajendra Acharya. 2022. "An Accurate Multiple Sclerosis Detection Model Based on Exemplar Multiple Parameters Local Phase Quantization: ExMPLPQ" Applied Sciences 12, no. 10: 4920. https://doi.org/10.3390/app12104920