1. Introduction
The restoration of autonomous and functional ambulation is a major priority. A gait study can identify variations and movements impairments that can help to make therapeutic decisions and to estimate the recovery status. Clinical gait analysis may also help to distinguish between disease entities and to determine the risk of disease or injury [
1,
2,
3,
4]. Base clinical gait evaluations are primarily observational or gait speed-based and they are ideal for measuring, tracking and evaluating a wide range of population functions and general health [
5]. However, base clinical gait evaluations do not have the precision or the richness of the data of instrumented methods which are necessary for comprehensive gait analysis on the kinematic and spatiotemporal aspects of the gait cycle [
3,
4]. However, instrumental gait analysis calls for expensive instruments, which in clinical settings are not always available.
Precise, non-intrusive and cost-efficient clinical gait analysis devices have many diagnosis, tracking, treatment and recovery uses [
3,
6]. Such uses include early detection and evaluation, assessing drug efficacy in the home or even improving care directly. A number of methods for gait analysis have been suggested in the state of art. Marker systems typically use infrared (IR) cameras and markers to be placed on the subject’s body. These systems are reliable, but also very expensive and unsustainable. In addition, before each capture session, passive or active markers have to be placed on the body correctly.
The use of wearable sensors has been proposed in recent studies [
7]. These systems are suitable for ambulatory measurements at home since they are small, easy, mobile and cheaper. Wearable sensors need to be positioned correctly and safely. In addition, the weight, noise and signal drift must be taken into account. Each sensor is normally limited to measuring very few gait properties and thus, a number of sensors are needed to obtain a complete analysis. In addition, these sensors entail adjustments to the subject’s daily routine. Furthermore, they often need maintenance in the form of batteries, data upload and sanitation. To avoid these inadequacies, in the context of gait analysis, individuals can be identified using single or multiple video cameras [
8,
9].
Three-dimensional (3D) depth sensing may provide useful healthcare data such as location, posture and movement of patients [
10]. In addition, it can collect 3D body physics measurements [
10]. This ability to produce quantitative data helps meet the clinician’s need to make decisions based on accurate measures and promote cost-effective custom medical practice [
11]. A well-known 3D depth sensor is Microsoft Kinect (Microsoft Co., Redmond, WA, USA), named Kinect v2 in its latest version. Kinect is an input system designed for XBox video game console computer gaming. The sensor allows a user to communicate in virtual reality through body motion, hand movements and speech commands. The sensor uses color camera, infrared (IR) emitter and IR sensor to create a three-dimensional (3D) image containing a cloud with a location and surface of more than 200,000 points representing the object as coordinates x, y and z. Kinect can be used to promote a healthy life by tracking patterns of activity, by collecting health data, or by detecting early warning sings in elderly or poor health people [
12]. In addition, Kinect applications are used for disease control and monitoring as well as to determine patient attitude and motion [
10,
11,
13,
14,
15], and to design rehabilitation exercises and therapy devices [
16,
17,
18,
19].
In previous works, we applied a supervised approach to the learning process to determine gait parameters automatically and precisely using a simulated 3D skeleton [
20]. It helped to go beyond normal stage parameters. The proposed method was compared with one commercial vision system used in protocols for clinical trials. The findings showed that the method is equivalent to the commercial system. Currently, the gait analysis system described in [
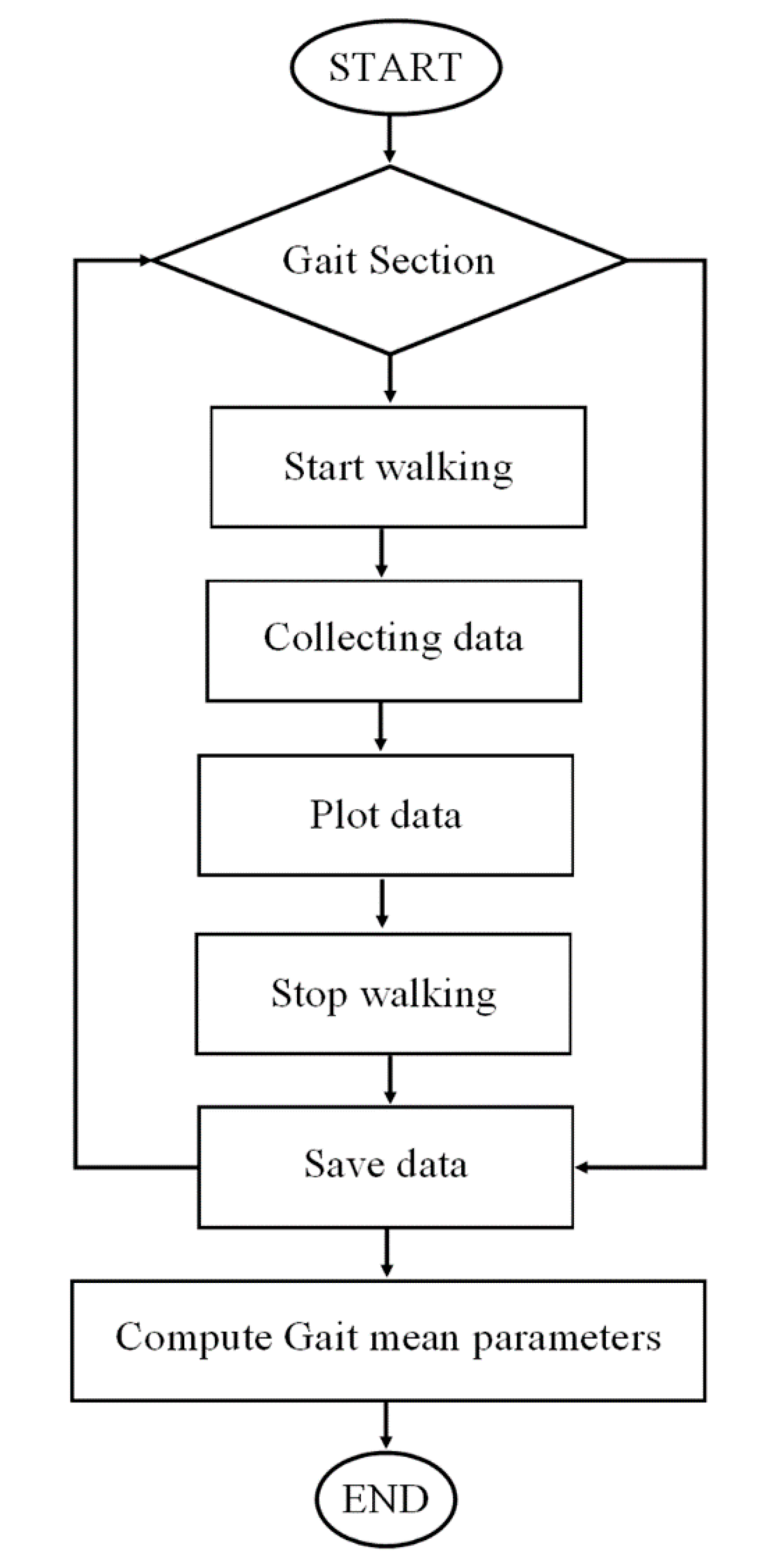
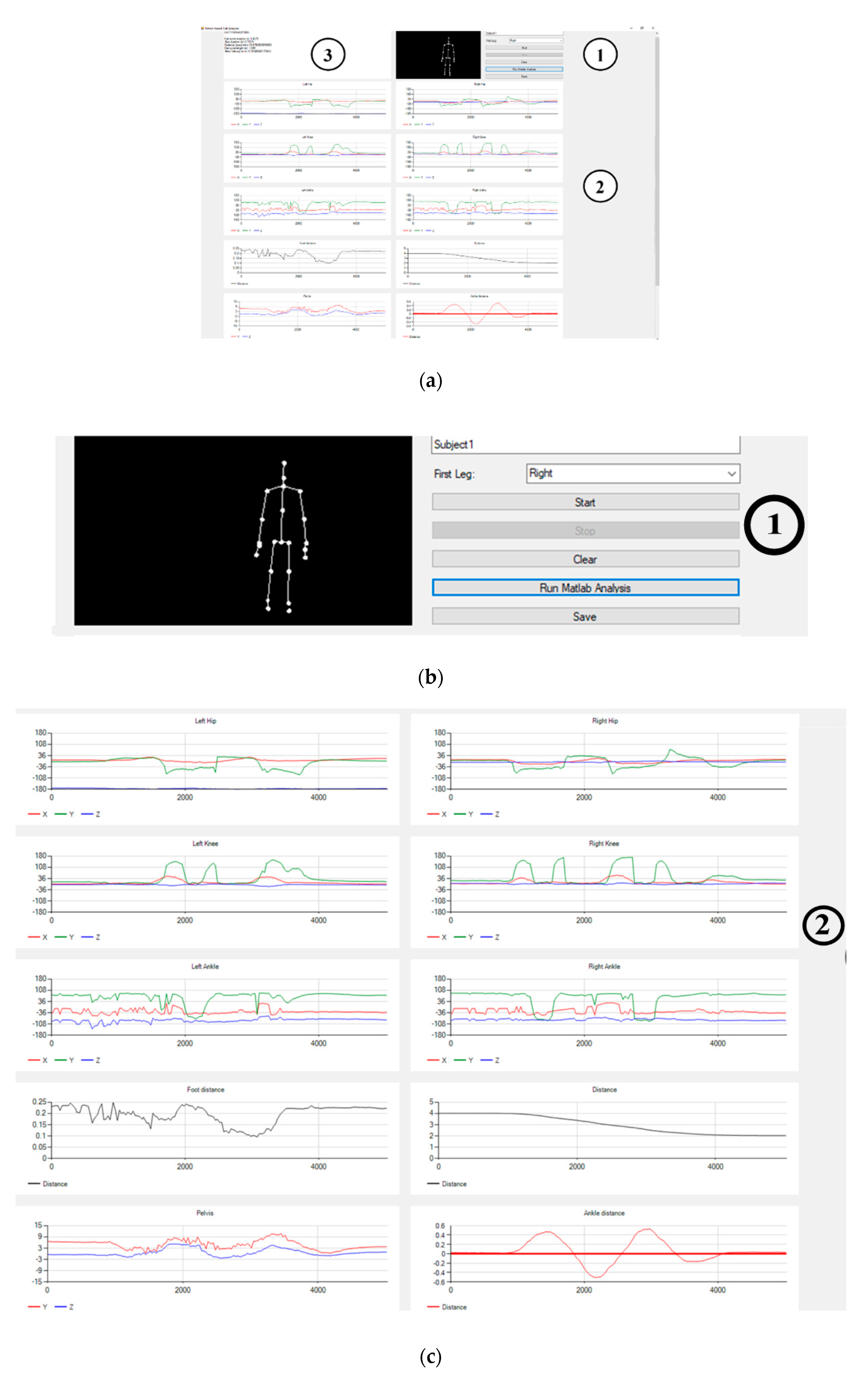
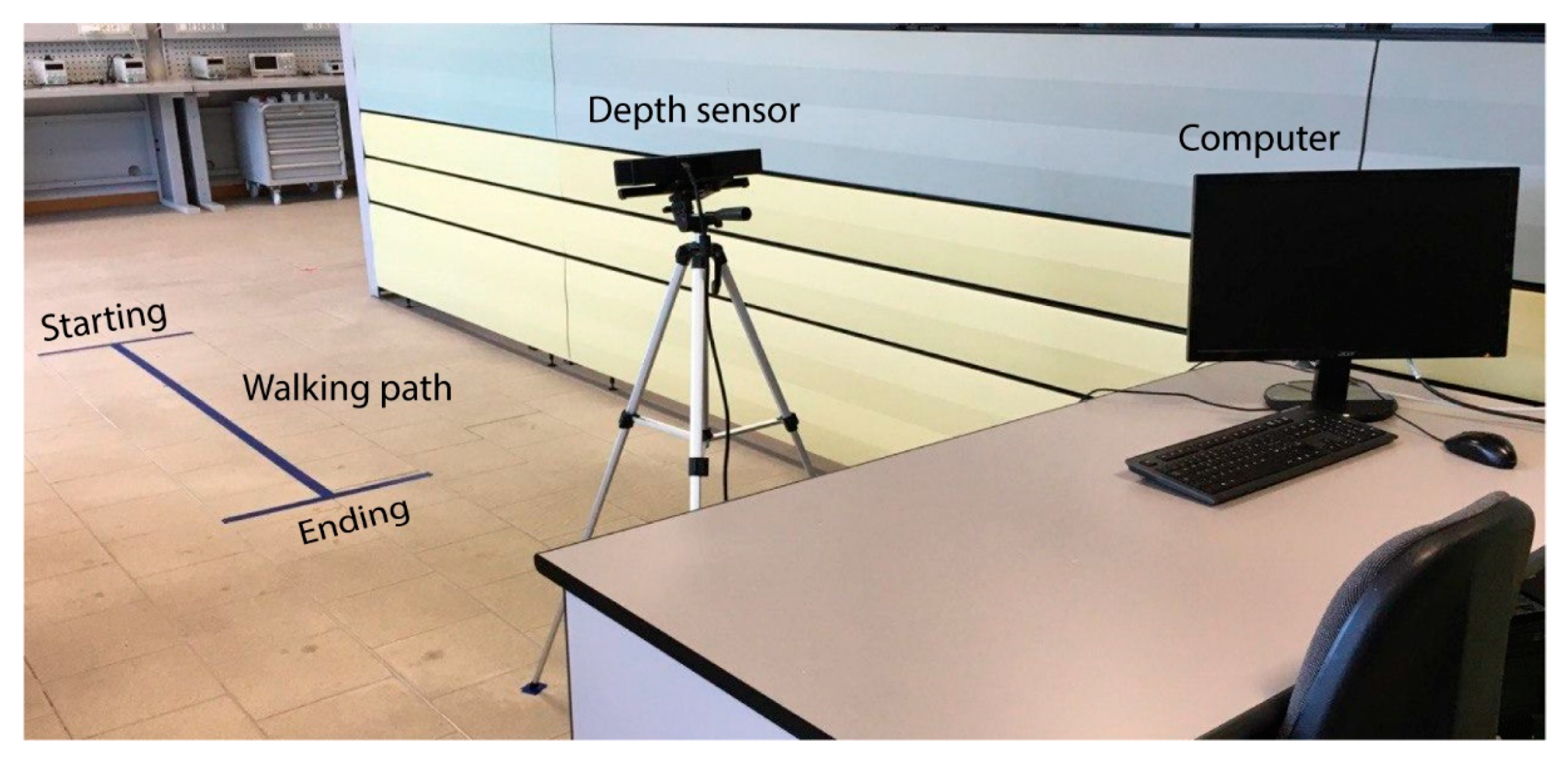
20] is an end-product ready for end-users (noncommercial yet) that has been named SANE (eaSy gAit aNalysis systEm). SANE system is a low-cost, non-intrusive solution which can accurately measure a wide range of gait parameters via a depth sensor and a connected software working together. One of the main advantages of SANE is that the parameter calculation is carried out automatically, that is, it is not necessary to manually indicate where each gait cycle begins and ends since SANE detects it automatically using the distance between ankles. SANE uses a Microsoft Kinect v2 sensor (Microsoft Co., Redmond, WA, USA) as the depth sensor.
Inter-method reliability assesses the agreement between measures of different methods or instruments. Therefore, a new method or instrument can be compared with existing methods calculating the inter-method reliability [
21]. Recent studies have addressed the inter-method reliability of Kinect-based systems for gait analysis and promising results have been found for spatiotemporal parameters with respect to other existing methods/systems, as demonstrated in the detailed review about validity of the Kinect for gait assessment in [
1]. For example, authors in [
22] found a good to excellent agreement between the measures of spatiotemporal gait parameters (gait speed, cadence, step length, stride length, step width, step time and stride time) of a Kinect V2-based system, compared with a 60 Hz Optotrak System 3D motion analysis (Northern Digital Inc., Waterloo, ON, Canada) and a standardized clinical method namely 10 m walking test (10 MWT). As well, the authors in [
10] found excellent agreement between the spatiotemporal measures namely gait speed, step length and stride length of a Kinect-based system compared with a 120 Hz VICON 3D motion analysis (VICON, UK). Other comparable results are described in detail in the focused review about the validity of Kinect for gait assessment in [
1], when the inter-method reliability is addressed for Kinect-based systems, generally at the same time the intra-rater reliability is assessed [
10,
23]. However, few studies include test-retest reliability, the intra-rater reliability and inter-rater reliability of Kinect-based systems when it is used for assessing spatiotemporal parameters of the human gait [
24,
25,
26]; particularly, inter-rater reliability is almost never addressed. However, the three—test-retest, inter-rater and intra-rater reliability—are important to assess the agreement between measures of an instrument. The test-retest reliability allows to assess the agreement between measures obtained by one evaluator that tests a same group of subjects at different times (when giving the same task to the same subjects two or more times). The inter-rater reliability allows to assess the agreement between the measures obtained by two different evaluators that test the same group of subjects (when giving the same observations to two or more evaluator). Intra-rater reliability allows to assess the agreement between repeated measures obtained by one evaluator that tests a same group of subjects (when giving repeatedly the same observations to one evaluator) [
27,
28,
29,
30,
31,
32]. The training of the evaluator and the standardization of the task influence the inter-rater and intra-rater reliability. On the other hand, a highly dependent on the situation or on the subject’s condition influences the test-retest reliability [
27]. This study aims to assess the test-retest, inter-rater and intra-rater reliability of SANE for spatiotemporal parameter of the gait. The estimation of test-retest, inter-rater and intra-rater reliability of SANE were carried out in order to verify through the agreement between measures that SANE is a feasible markerless system for assessing spatiotemporal gait parameters.
4. Discussion
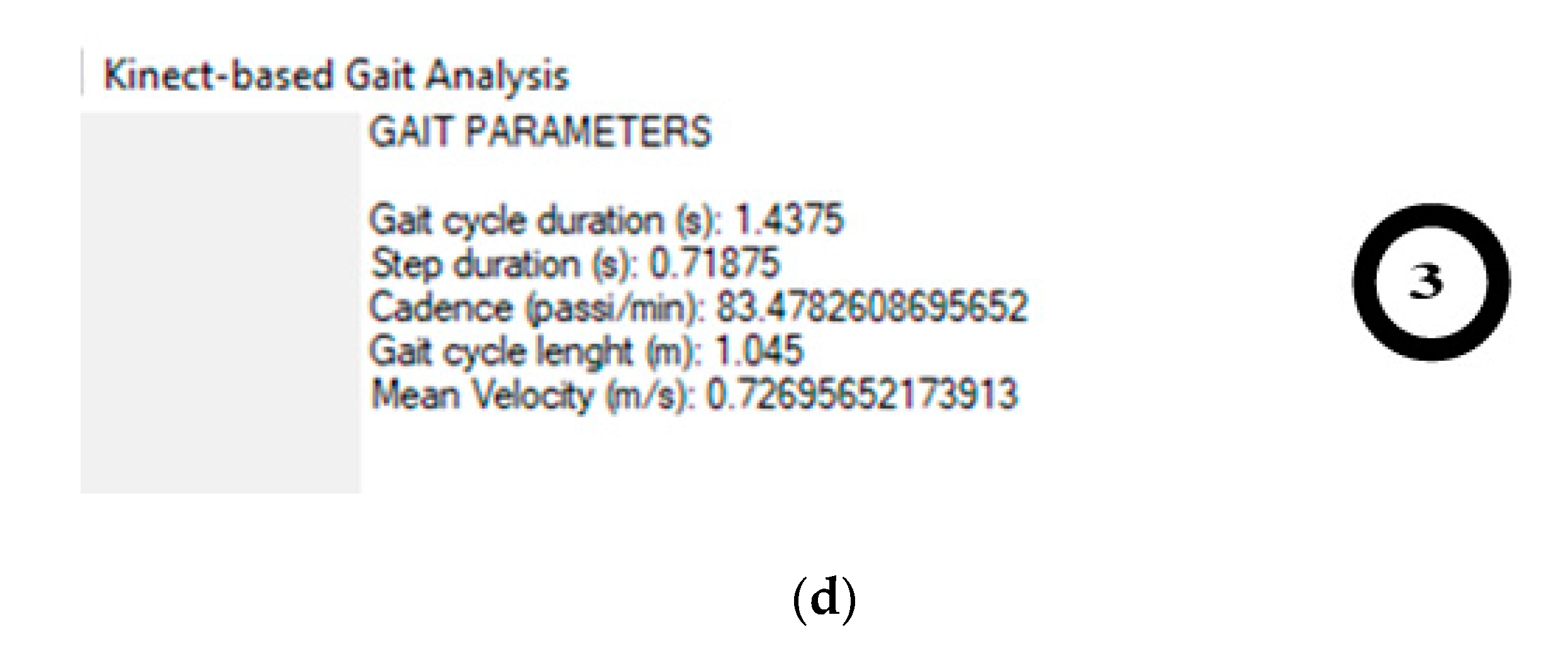
This study aimed to assess the test-retest, inter-rater and intra-rater reliability of SANE for estimating gait parameters: cycle duration, step duration, cadence, cycle length and mean velocity. The test-retest, inter-rater and intra-rater reliability were excellent for gait mean velocity. The intra-rater reliability was excellent for gait cycle duration, step duration, cadence and mean velocity, and modest for gait cycle length. The test-retest was excellent for gait cadence and mean velocity, and modest for gait cycle duration, step duration and cycle length. The gait mean velocity showed an excellent inter-rater reliability, and the other valued parameter presented a modest inter-rater reliability. No parameters presented a poor correlation. Summarizing for all parameters, test-retest reliability ranged from 0.62 to 0.81, inter-rater reliability ranged from 0.70 to 0.95 and intra-rater ranged from 0.74 to 0.92.
Since inter-rater and intra-rater reliability were close with small differences for all parameters, the training of the evaluators and the standardization of the task indicate to have a small effect on the reliability of SANE. On the other hand, test-retest reliability was lower than intra-rater and inter-rater reliability showing that the subject behavior has a greater effect on the reliability of SANE than the evaluator performance and the standardization of the task. Although it was suggested to the subjects to carry out a walk as natural as possible, it is evident that it is difficult to perform an identical walk seven days later.
The authors found that reliability studies for spatiotemporal parameters of the gait using the depth sensors Kinect usually focus on inter-method reliability comparing their measurements with the measurements of other existing systems and few of them are related with test-retest, inter-rater and intra-rater reliability of the system itself. Therefore, the results found in the study are difficult to compare with other depth sensor-based systems in terms of test-retest, inter-rater and intra-rater reliability. In [
24,
33] inter-day reliability (test-retest) was calculated for depth sensor-based system (Kinect v2). In [
33], a one-day interval was used to perform a second session to test gait parameters of 10 children with cerebral palsy. However, the parameters evaluated are different from those evaluated in this study thus the reliability results cannot be compared. In [
24], inter-day reliability (test-retest) of spatiotemporal and kinematic variables of the gait were estimated for a depth sensor-based system (Kinect v2) using seven-day interval (with injury-free/young subjects); reliability of spatiotemporal ranged from 0.55 and 0.87 (with comfortable pace) except for ground contact time (s) that had an ICC of 0.03. Test-retest reliability of SANE is within the reliability range found in [
24], since the ICCs for SANE measurements ranged from 0.62 to 0.81. Therefore, it can be said that SANE has an acceptable behavior in terms of reliability when used in different days (seven-day interval). However, strategies could be tested to help the subjects have additional references during a walk test, apart from the signs on the floor, with the aim of reducing the influence of subject behavior in the test-retest measurements. For example, music background or sound references could help set a similar pace from session to session.
In [
25], inter and intra-rater reliability, standard error of measurement and minimal detectable change of gait parameters were calculated for a depth sensor-based system (Kinect v2). In [
25], the intra-rater reliability for spatiotemporal parameters ranged approximability from 0.77 to 0.98 and the inter-rater reliability from 0.64 to 0.98. The sessions for the intra-rater reliability were carried out within 24 h. The intra-rater reliability of SANE ranged from 0.74 to 0.92 being comparable to the intra-rater reliability values found in [
25]. In addition, the inter-rater reliability of SANE ranged from 0.70 to 0.95 being within the range of inter-rater reliability found in [
25]. Therefore, it can be considered that SANE has an acceptable behavior in terms of reliability when it is used during repeated measurements by a same evaluator and when it is used by different evaluators. The authors in [
25] consider that their results about inter and intra-rater reliability are supported by the preliminary studies in [
24,
26]. However, in [
24] (reference already addressed in the previous paragraph) the results can be better compared with the test-rest reliability type since the reliability in [
24] was estimated using seven days interval between sessions. In [
26], inter-trail reliability (which can be considered intra-rater reliability) for a depth sensor-based system (Kinect v2) ranged from 0.73 to 0.96 for spatiotemporal parameters. Therefore, intra-rater reliability of SANE and the Kinect based system in [
25] are within the range of the results found in [
26]. In [
39], inter and intra-rater reliability were assessed for a depth sensor-based system (Kinect) for subject standing height, vertical jump height and broad jump length, finding that the reliability is comparable to clinically accepted manual measurements. However, in [
39], spatiotemporal parameter of the gait was not addressed.
Test-retest reliability (from 0.62 to 0.81), inter-rater reliability (from 0.70 to 0.95) and intra-rater reliability (from 0.74 to 0.92) of SANE are comparable with those of the one of the most popular gait analysis systems VICON (three-dimensional motion analysis system): in [
40], test-retest reliability and inter-tester reliability of VICON 140™ ranged from 0.97 to 0.99 for the sagittal plane, from 0.76 to 0.98 for the frontal plane and from 0.73 to 0.90 for the transverse plane; in [
41], inter-session (between two sessions with a two-day interval) was >0.82 and the intra-session (between five trials) was ≥0.78 for VICON system. Furthermore, the test-retest reliability for spatiotemporal parameters of the three-dimensional motion analysis system (3DMA) (not Kinect) used in [
24] ranged from 0.63 to 0.85 except for ground contact time(s) that had an ICC of 0.21. Therefore, test-retest reliability of SANE is comparable with 3DMA. On the other hand, it is important to mention that the authors in [
25] found that the inter-rater and intra-rater reliability obtained by their Kinect v2-based system are comparable to the clinical tools 10MWT (10 Meter Walk Test, used to assess walking speed) and DGI (Dynamic Gait Index, to assess gait, balance and fall risk). As well as the authors in [
26] demonstrated that their Kinect v2-based system showed a high inter-method reliability for spatiotemporal parameters when it is compared with the system GAITRite mat. In addition, it is important to mention that SANE showed an excellent inter-method reliability when it was compared with the measures of VICON cameras system in a previous study in [
20].
The SEM% for reliability tests for gait cadence, cycle length and mean velocity were acceptable (<5.0%). Although SEM% of test-retest and inter-rater reliability for gait cycle duration and step duration were ≤5.9% (close to accepted values), SEM% values of SANE are comparable to the results for spatiotemporal variables in [
24] where SEM% using Kinect v2 was <16.8% and using 3DMA system <15.2%. SDC% for all reliability tests were from acceptable to excellent (<16.4%). SDC% values of SANE are comparable to the results in [
25] for spatiotemporal variables using Kinect v2 where SDC% was <23.9%, except for Double support time and Step asymmetry.








{kind=link}
{kind=link}
{kind=link}
{kind=link}